Digestion & Absorption
BIOMEDICAL IMPORTANCEBesides water, the diet must provide metabolic fuels (mainly carbohydrates and lipids), protein (for growth and turnover of tissue proteins), fiber (for roughage), minerals (elements with specific metabolic functions), and vitamins and essential fatty acids (organic compounds needed in small amounts for essential metabolic and physiologic functions).
The polysaccharides, triacylglycerols, and proteins that make up the bulk of the diet must be hydrolyzed to their constituent monosaccharides, fatty acids, and amino acids, respectively, before absorption and utilization. Minerals and vitamins must be released from the complex matrix of food before they can be absorbed and utilized.
Digestion of Carbohydrates:
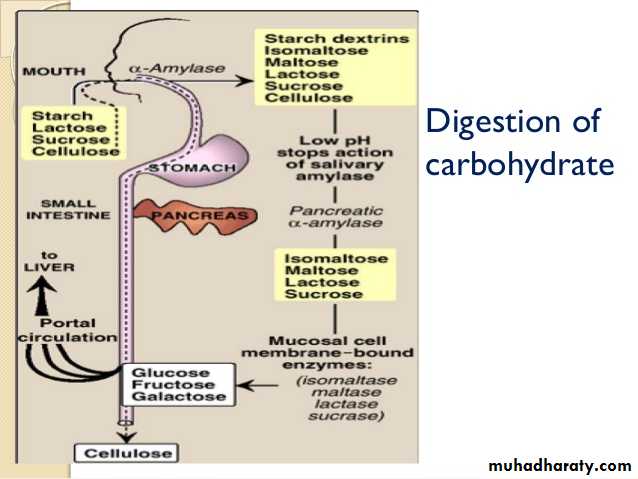
The principal sites of dietary carbohydrate digestion are the mouth and intestinal lumen.In the mouth: During mastication, salivary α-amylase acts briefly on dietary starch and glycogen in a random manner, hydrolyzing some α(1→4) bonds. Because branched amylopectin and glycogen also contain α(1→6) bonds, which α-amylase cannot hydrolyze, the digest resulting from its action contains a mixture of short, branched oligosaccharides or dextrins.
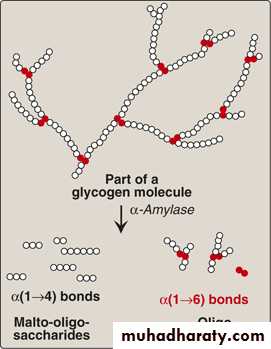
Degradation of dietary glycogen by salivary or pancreatic α-amylase
In the stomach: Carbohydrate digestion halts temporarily in the stomach, because the high acidity inactivates the salivary α-amylase.in the small intestine: When the acidic stomach contents reach the small intestine, they are neutralized by bicarbonate secreted by the pancreas, and pancreatic α-amylase continues the process of starch digestion. The final digestive processes occur at the mucosal lining of the upper jejunum, declining as they proceed down the small intestine, and include the action of several disaccharidases and oligosaccharidases.
For example, - isomaltase cleaves the α(1→6) bond in isomaltose .
maltase cleaves maltose, both producing glucose.
sucrase cleaves sucrose producing glucose and fructose.
lactase (β-galactosidase) cleaves lactose producing galactose and glucose. These enzymes are secreted through, and remain associated with, the luminal side of the brush border membranes of the intestinal mucosal cells.
Absorption of monosaccharides
The duodenum and upper jejunum absorb the bulk of the dietary sugars. Insulin is not required for the uptake of glucose by intestinal cells. However, different sugars have different mechanisms of absorption.galactose and glucose are transported into the mucosal cells by an active, energy-requiring process that requires a concurrent uptake of sodium ions; the transport protein is the sodium-dependent glucose cotransporter 1 (SGLT-1).
Fructose uptake requires a sodium-independent monosaccharide transporter (GLUT-5) for its absorption.
Abnormal degradation of disaccharides
Digestive enzyme deficiencies:Causes:
Hereditary deficiencies of disaccharidases.
Malnutrition.
drugs that injure the mucosa of the small intestine.
normal individuals with severe diarrhea lead to brush border enzymes are rapidly lost, causing a temporary, acquired enzyme deficiency. Thus, patients suffering or recovering from such a disorder cannot drink or eat significant amounts of dairy products or sucrose without exacerbating the diarrhea.
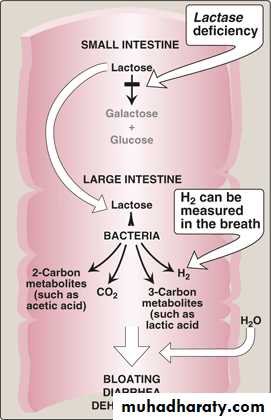
Lactose intolerance:
More than three quarters of the world's adults are lactose intolerant. This is particularly manifested in certain races. For example, up to ninety percent of adults of African or Asian descent are lactase-deficient and, therefore, are less able to metabolize lactose than individuals of Northern European origin.The mechanism: by which this age-dependent loss of the enzyme occurs is not clear, but it is determined genetically and represents a reduction in the amount of enzyme protein rather than a modified inactive enzyme.
Treatment:
for this disorder is to reduce consumption of milk while eating yogurts and cheeses, as well as green vegetables such as broccoli, to ensure adequate calcium intake; to use lactase-treated products; or to take lactase in pill form prior to eating.
Abnormal lactose metabolism
Isomaltase-sucrase deficiency: This enzyme deficiency results in an intolerance of ingested sucrose.Treatment : includes the withholding of dietary sucrose, and enzyme replacement therapy.
Diagnosis:
Identification of a specific enzyme deficiency can be obtained by performing oral tolerance tests with the individual disaccharides.Measurement of hydrogen gas in the breath is a reliable test for determining the amount of ingested carbohydrate not absorbed by the body, but which is metabolized instead by the intestinal flora.
DIGESTION & ABSORPTION OF LIPIDS:
The major lipids in the diet are triacylglycerols and, the remainder of the dietary lipids consists primarily of cholesterol, cholesteryl esters, phospholipids, and unesterified (“free”) fatty acids.In the stomach: The digestion of lipids begins in the stomach, catalyzed by an acid-stable lipase that originates from glands at the back of the tongue (lingual lipase). TAG molecules, particularly those containing fatty acids of short- or medium-chain length (less than 12 carbons, such as are found in milk fat), are the primary target of this enzyme. These same TAGs are also degraded by a separate gastric lipase, secreted by the gastric mucosa. Both enzymes are relatively acid-stable, with pH optimums of pH 4 to pH 6. These “acid lipases” play a particularly important role in lipid digestion in neonates, for whom milk fat is the primary source of calories.
In the small intestine: emulsification of dietary lipids occurs in the duodenum. Emulsification increases the surface area of the hydrophobic lipid droplets so that the digestive enzymes, which work at the interface of the droplet and the surrounding aqueous solution, can act effectively.
TAG degradation
pancreatic enzymes:pancreatic lipase :act on TAG molecules because they are too large to be taken up efficiently by the mucosal cells of the intestinal villi. which preferentially removes the fatty acids at carbons 1 and 3.
Colipase: also secreted by the pancreas, binds the lipase at a ratio of 1:1, and anchors it at the lipid-aqueous interface.
N.B: Orlistat, an antiobesity drug, inhibits gastric and pancreatic lipases, thereby decreasing fat absorption, resulting in loss of weight.
Cholesteryl ester degradation:
Most dietary cholesterol is present in the free (nonesterified) form, with 10–15% present in the esterified form. Cholesteryl esters are hydrolyzed by pancreatic cholesteryl ester hydrolase (cholesterol esterase), which produces cholesterol plus free fatty acids. Cholesteryl ester hydrolase activity is greatly increased in the presence of bile salts.
Phospholipid degradation:
Pancreatic juice is rich in the proenzyme of phospholipase A2 that, like procolipase, is activated by trypsin and, like cholesteryl ester hydrolase, requires bile salts for optimum activity. Phospholipase A2 removes one fatty acid from carbon 2 of a phospholipid, leaving a lysophospholipid. The remaining fatty acid at carbon 1 can be removed by lysophospholipase, leaving a glycerylphosphoryl base.Control of lipid digestion:
Cholecystokinin (CCK, formerly called pancreozymin): a small peptide hormone is produced by the Cells in the mucosa of the jejunum and lower duodenum in response to the presence of lipids and partially digested proteins entering these regions of the upper small intestine. CCK acts on the gallbladder (causing it to contract and release bile—a mixture of bile salts, phospholipids, and free cholesterol), and on the exocrine cells of the pancreas (causing them to release digestive enzymes). It also decreases gastric motility, resulting in a slower release of gastric contents into the small intestine.Secretin, in response to the low pH of the chyme entering the intestine. Secretin causes the pancreas and the liver to release a watery solution rich in bicarbonate that helps neutralize the pH of the intestinal contents, bringing them to the appropriate pH for digestive activity by pancreatic enzymes.
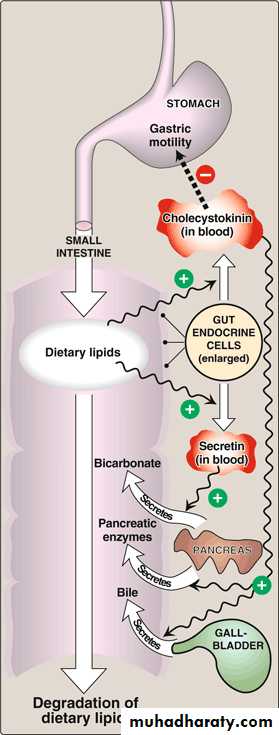
Hormonal control of lipid digestion in the small intestine.
Absorption of lipids by intestinal mucosal cells (enterocytes)Free fatty acids, free cholesterol, and 2-monoacylglycerol are the primary products of lipid digestion in the jejunum. These, plus bile salts and fat-soluble vitamins, form mixed micelles—disk-shaped clusters of amphipathic lipids that coalesce with their hydrophobic groups on the inside and their hydrophilic groups on the outside. Mixed micelles are, therefore, soluble in the aqueous environment of the intestinal lumen.
These particles approach the primary site of lipid absorption, the brush border membrane of the enterocytes (mucosal cell). This membrane is separated from the liquid contents of the intestinal lumen by an unstirred water layer that mixes poorly with the bulk fluid. The hydrophilic surface of the micelles facilitates the transport of the hydrophobic lipids through the unstirred water layer to the brush border membrane where they are absorbed.
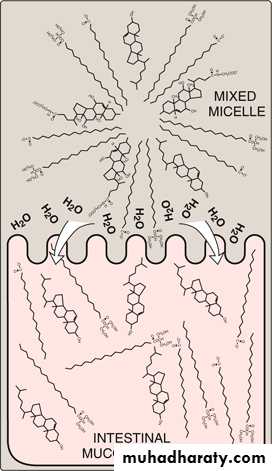
Absorption of lipids contained in a mixed micelle by an intestinal mucosal cell.
Resynthesis of TAG and cholesteryl estersThe mixture of lipids absorbed by the enterocytes migrates to the endoplasmic reticulum where biosynthesis of complex lipids takes place.
Lipid malabsorption
Lipid malabsorption, resulting in increased lipid (including the fat-soluble vitamins A, D, E, and K, and essential fatty acids) in the feces (that is, steatorrhea), can be caused by disturbances in lipid digestion and/or absorption . Such disturbances can result from several conditions, including CF (causing poor digestion) and shortened bowel (causing decreased absorption).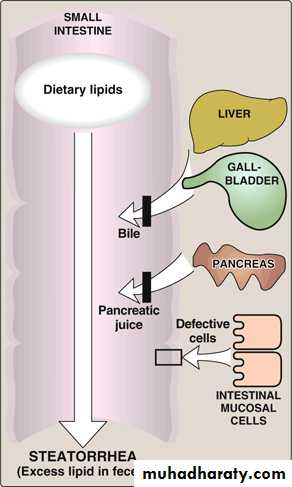
Possible causes of steatorrhea
Digestion of Dietary ProteinsMost of the nitrogen in the diet is consumed in the form of protein, Proteins are generally too large to be absorbed by the intestine. They must, therefore, be hydrolyzed to yield their constituent amino acids, which can be absorbed. Proteolytic enzymes responsible for degrading proteins are produced by three different organs: the stomach, the pancreas, and the small intestine .
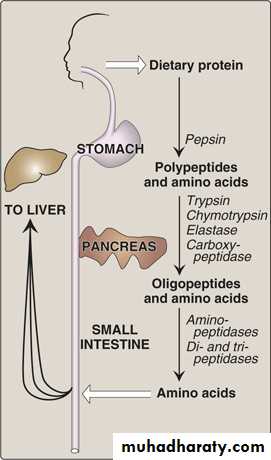
Digestion of dietary proteins by the proteolytic enzymes of the gastrointestinal tract.
Digestion of proteins by gastric secretion
The digestion of proteins begins in the stomach, which secretes gastric juice—a unique solution containing hydrochloric acid and the proenzyme, pepsinogen.Hydrochloric acid: Stomach acid is too dilute (pH 2–3) to hydrolyze proteins. The acid functions instead to kill some bacteria and to denature proteins, thus making them more susceptible to subsequent hydrolysis by proteases.
Pepsin: This acid-stable endopeptidase is secreted by the serous cells of the stomach as an inactive zymogen (or proenzyme), pepsinogen. Pepsinogen is activated to pepsin, either by HCl, or autocatalytically by other pepsin molecules that have already been activated. Pepsin releases peptides and a few free amino acids from dietary proteins.
Digestion of proteins by pancreatic enzymes
On entering the small intestine, large polypeptides produced in the stomach by the action of pepsin are further cleaved to oligopeptides and amino acids by a group of pancreatic proteases.
Release of zymogens: The release and activation of the pancreatic zymogens is mediated by the secretion of cholecystokinin and secretin, two polypeptide hormones of the digestive tract.
Enteropeptidase (formerly called enterokinase)— an enzyme synthesized by and present on the luminal surface of intestinal mucosal cells of the brush border membrane—converts the pancreatic zymogen trypsinogen to trypsin. Trypsin subsequently converts other trypsinogen molecules to trypsin by cleaving a limited number of specific peptide bonds in the zymogen. Enteropeptidase thus unleashes a cascade of proteolytic activity, because trypsin is the common activator of all the pancreatic zymogens.
Celiac disease (celiac sprue) is a disease of malabsorption resulting from immune-mediated damage to the small intestine in response to ingestion of gluten, a protein found in wheat and other grains.
Digestion of oligopeptides by enzymes of the small intestine
The luminal surface of the intestine contains aminopeptidase—an exopeptidase that repeatedly cleaves the N-terminal residue from oligopeptides to produce free amino acids and smaller peptides.Absorption of amino acids and dipeptides
Free amino acids are taken into the enterocytes up by a Na+-linked secondary transport system. Di- and tripeptides, however, are taken up by a H+-linked transport system. There, the peptides are hydrolyzed in the cytosol to amino acids before being released into the portal system. Thus, only free amino acids are found in the portal vein after a meal containing protein. These amino acids are either metabolized by the liver or released into the general circulation.DIGESTION & ABSORPTION OF VITAMINS & MINERALS
Vitamins and minerals are released from food during digestion—though this is not complete—and the availability of vitamins and minerals depends on the type of food and, especially for minerals, the presence of chelating compounds.
The fat-soluble vitamins are absorbed in the lipid micelles that result from fat digestion; water-soluble vitamins and most mineral salts are absorbed from the small intestine either by active transport or by carrier-mediated diffusion followed by binding to intracellular binding proteins to achieve concentration upon uptake.
Vitamin B12 absorption requires a specific transport protein, intrinsic factor; calcium absorption is dependent on vitamin D; zinc absorption probably requires a zinc-binding ligand secreted by the exocrine pancreas; and the absorption of iron is limited.
Calcium Absorption Is Dependent on Vitamin D
In addition to its role in regulating calcium homeostasis, vitamin D is required for the intestinal absorption of calcium. Synthesis of the intracellular calciumbinding protein, calbindin, required for calcium absorption, is induced by vitamin D, which also affects the permeability of the mucosal cells to calcium, an effect that is rapid and independent of protein synthesis. Phytic acid (inositol hexaphosphate) in cereals binds calcium in the intestinal lumen, preventing its absorption.
Other minerals, including zinc, are also chelated by phytate. This is mainly a problem among people who consume large amounts of unleavened whole wheat products; yeast contains an enzyme, phytase,
which dephosphorylates phytate, so rendering it inactive.
High concentrations of fatty acids in the intestinal lumen—as a result of impaired fat absorption—can also reduce calcium absorption by forming insoluble calcium salts; a high intake of oxalate can sometimes cause deficiency, since calcium oxalate is insoluble.
Iron Absorption
Although iron deficiency is a common problem, about10% of the population are genetically at risk of iron overload (hemochromatosis).Absorption of iron is strictly regulated. Inorganic iron is accumulated
in intestinal mucosal cells bound to an intracellular protein, ferritin. Once the ferritin in the cell is saturated with iron, no more can enter. Iron can only leave the mucosal cell if there is transferrin in plasma to bind to. Once transferrin is saturated with iron, any that has accumulated in the mucosal cells will be lost when the cells are shed. As a result of this mucosal barrier,only about 10% of dietary iron is normally absorbed and only 1–5% from many plant foods.
Inorganic iron is absorbed only in the Fe2+ (reduced) state, and for that reason the presence of reducing agents will enhance absorption. The most effective compound is vitamin C, and while intakes of 40–60 mg of vitamin C per day are more than adequate to meet requirements, an intake of 25–50 mg per meal will enhance iron absorption, especially when iron salts are used to treat iron deficiency anemia. Ethanol and fructose also enhance iron absorption. Heme iron from meat is absorbed separately and is considerably more available than inorganic iron. However, the absorption of both inorganic and heme iron is impaired by calcium—a glass of milk with a meal significantly reduces availability.