1
Endodontic anatomy and pulp considerations
For the success of endodontic therapy, it is essential to have the knowledge of normal and
usual configuration of the pulp cavity and its variations. Before initiating the endodontic
therapy, thorough knowledge of pulp anatomy is required. In addition to general morphology,
variations in canal system must be kept in mind while performing the root canal therapy.
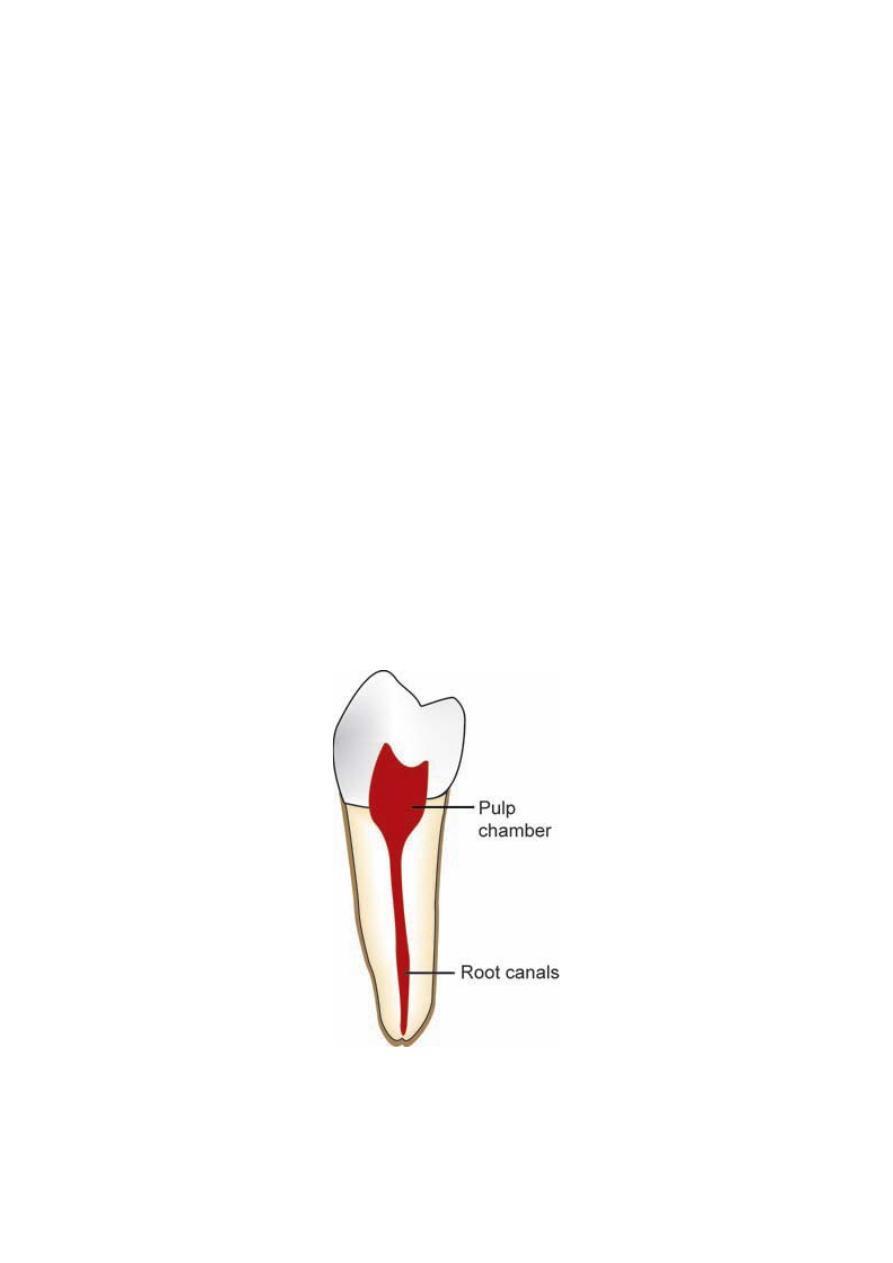
Pulp cavity: The pulp cavity lies within the tooth and is enclosed by dentin all around,
except at the apical foramen. It is divided into two parts; coronal (pulp chamber) and
radicular (root canal).
Pulp Chamber
• Coronal portion, i.e. pulp chamber (Fig.1) reflects the external form of crown.
• It occupies the coronal portion of pulp cavity. It acquires shape according to shape and size
of crown of the tooth, age of person, and irritation (which induces reparative dentine
formation), if any.
• The roof of pulp chamber consists of dentin covering the pulp chamber occlusally or
incisally.
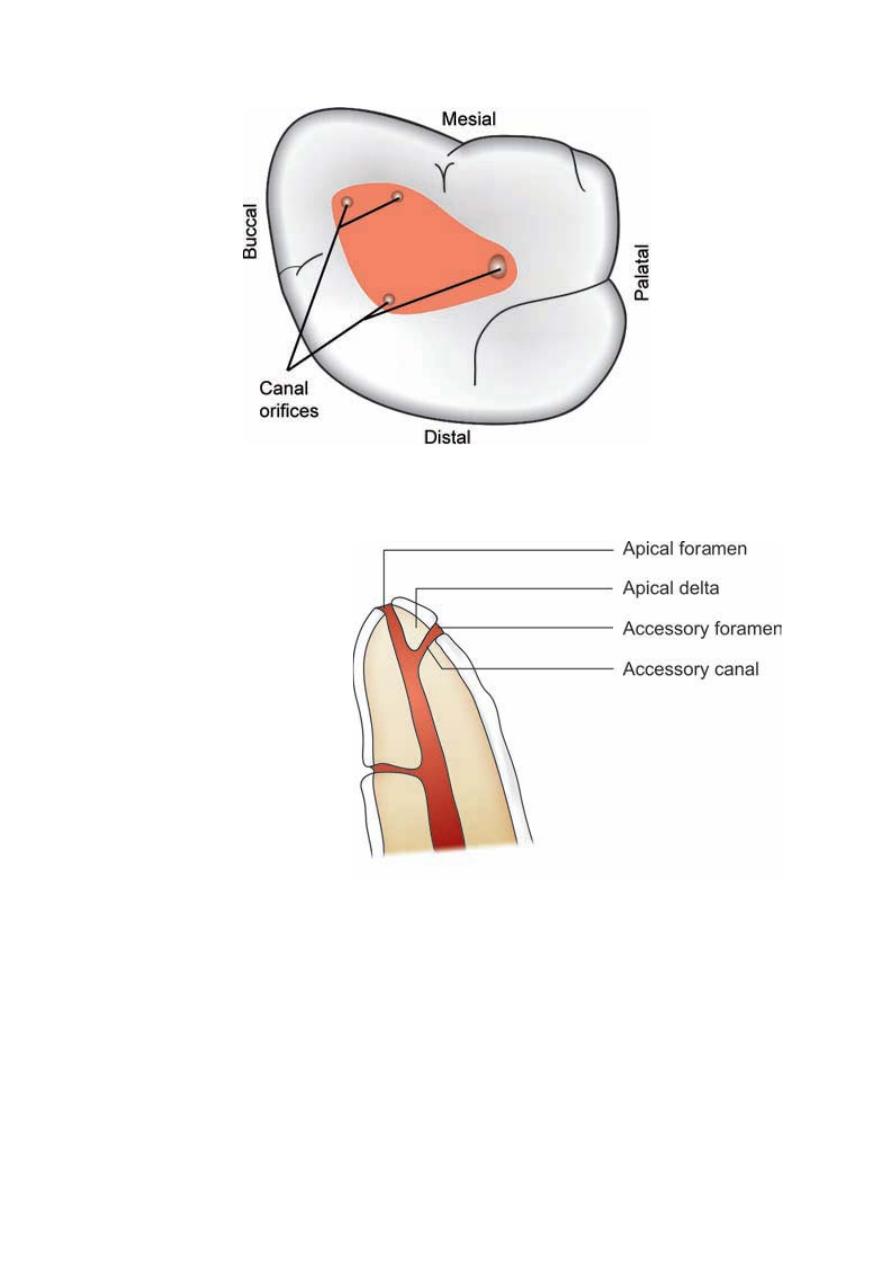
• The floor of pulp chamber merges into the root canal at the orifices. Thus, canal orifices are
the openings in the floor of pulp chamber leading into the root canals (Fig.2).
Root Canal: The root canal extends from canal orifice to the apical foramen.
Apical Foramen: It is the apical opening of the root canal through which blood vessels enter
the canal (Fig.3).
Fig. 1 Pulp cavity showing pulp chamber and root canals
.ﺩ
ﻋﻼء ﺍﺩﺭﻳﺱ
2
Fig. 2 Canal orifices
Fig. 3
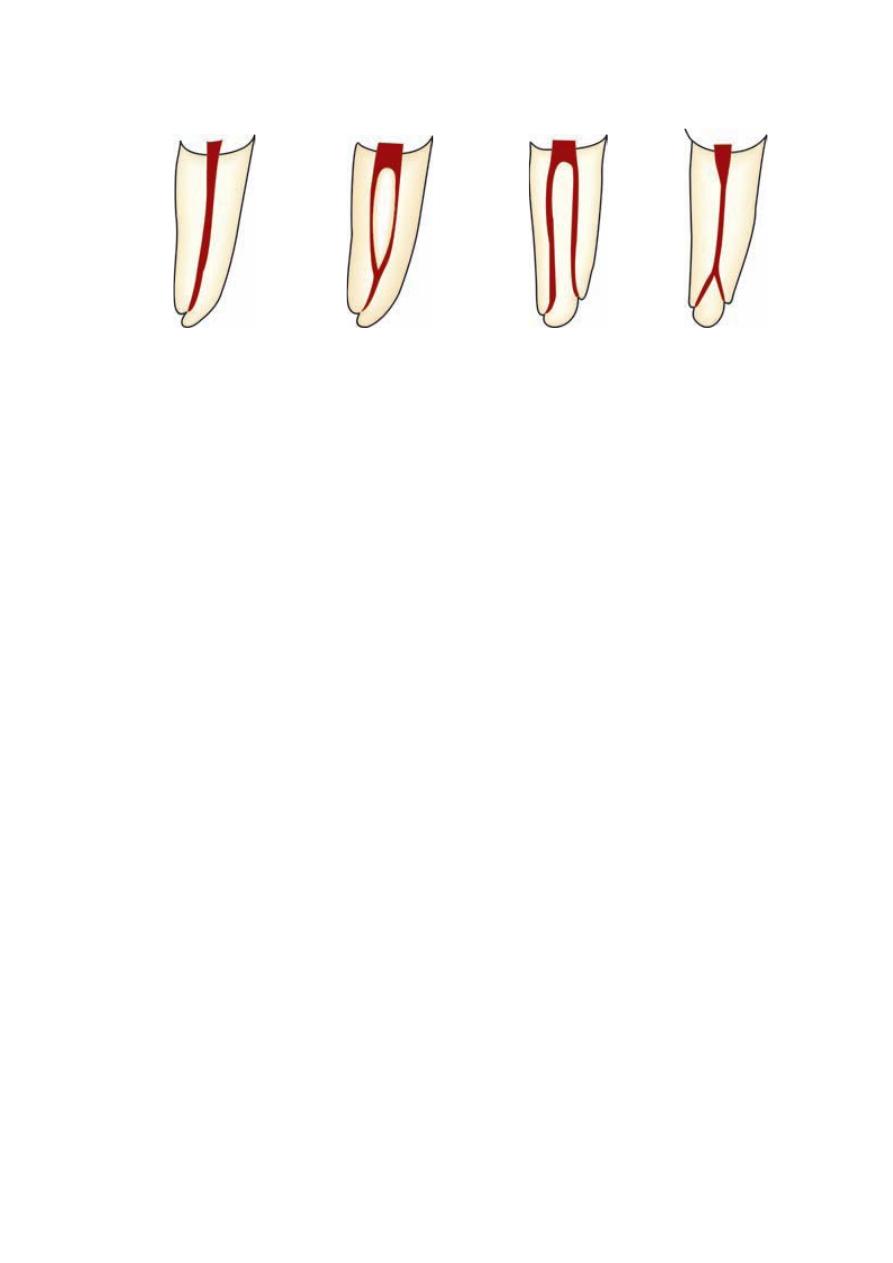
Canal configurations
In most cases, number of root canals corresponds with number of roots but a root may have
more than one canal. Despite of many combinations of canals which are present in the roots
of the teeth, four categories of root canal system can be described. These are as follows
(Fig.4):
Type I: Single canal from pulp chamber to apex.
Type II: Two separate canals leaving the chamber but exiting as one canal.
Type III: Two separate canals leaving the chamber and exiting as two separate foramina.
Type IV: One canal leaving the chamber but dividing into two separate canals and exiting in
two separate foramina.
3
Fig. 4 Type I Type II Type III Type IV
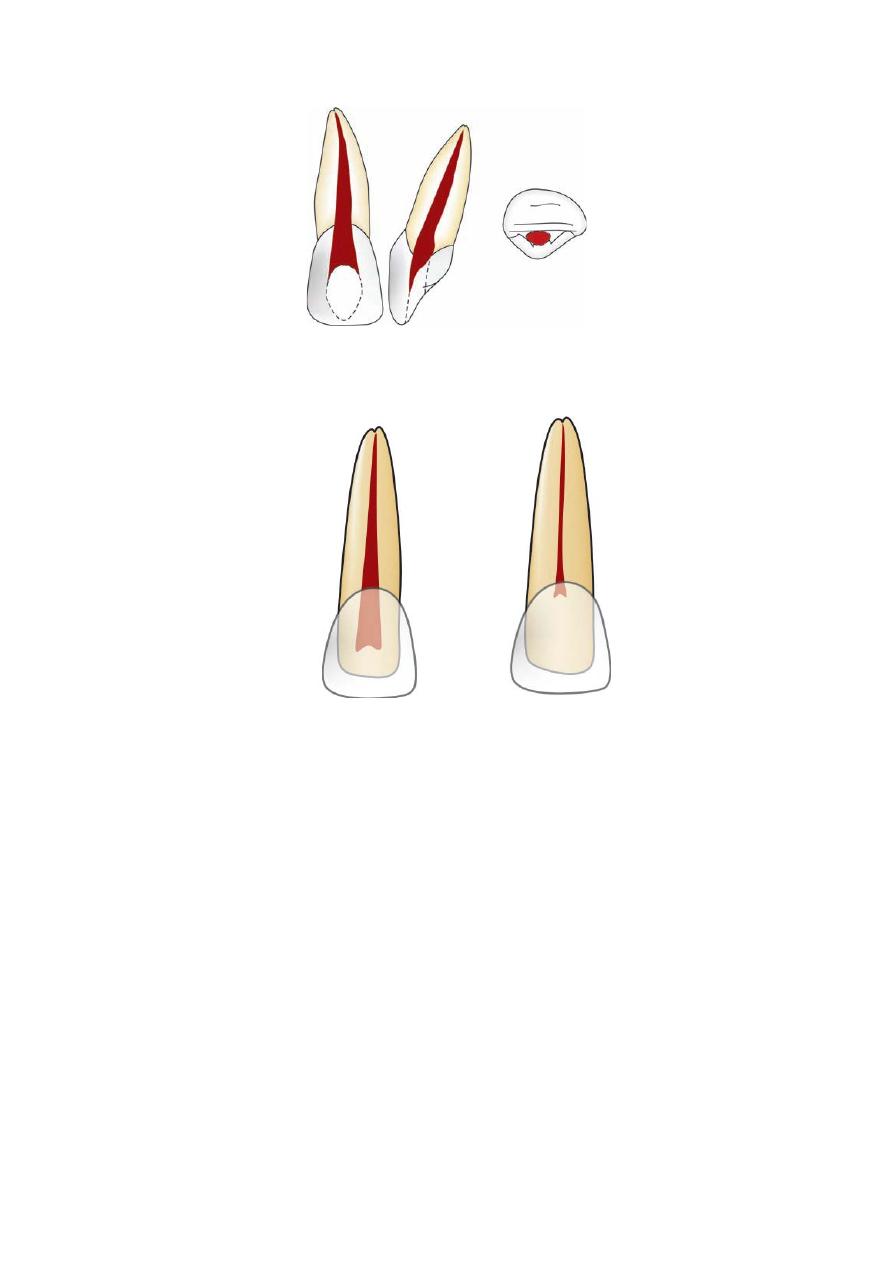
Individual tooth anatomy
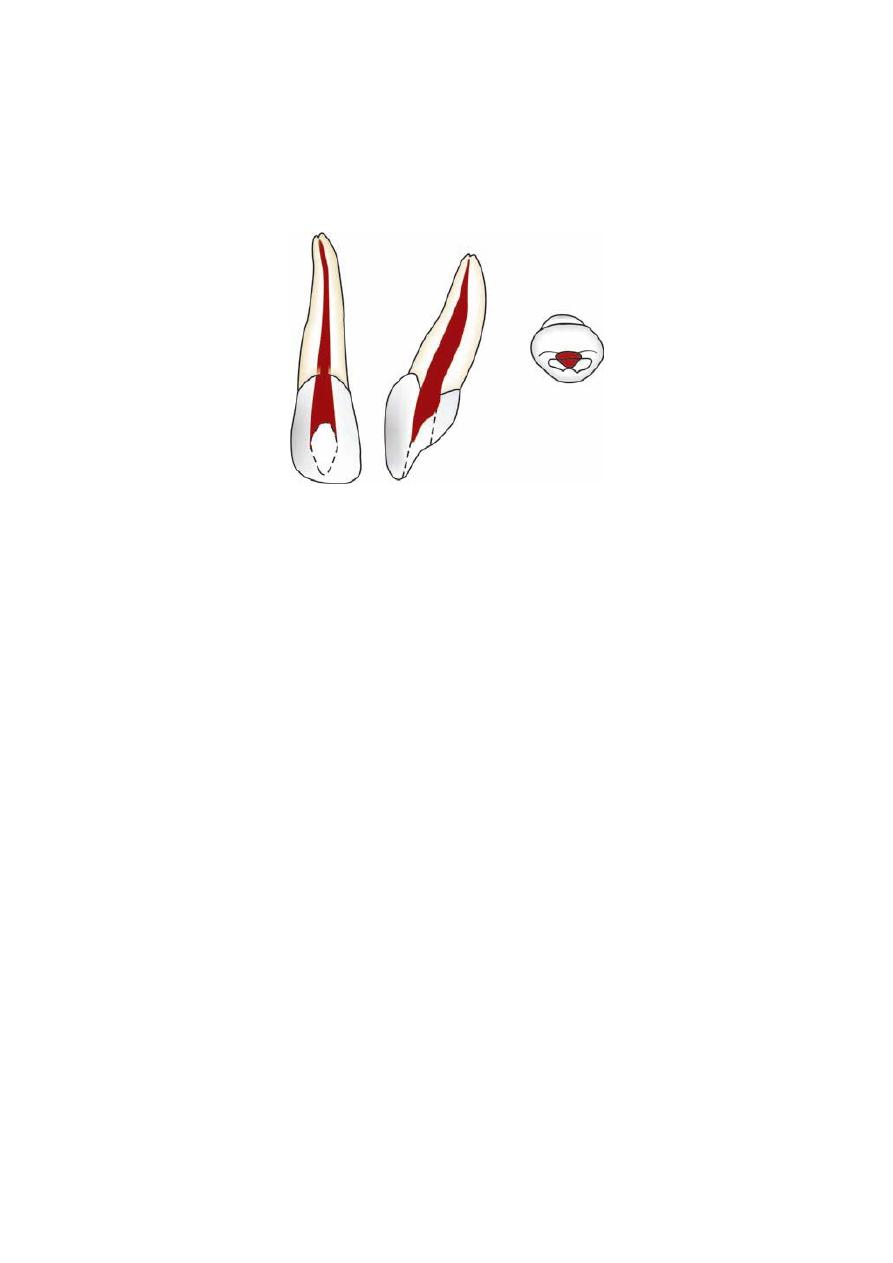
Maxillary Central Incisor (Figs 5 and 6)
Average Tooth Length: The average length of the maxillary central incisor is 22.5 mm.
Pulp Chamber
• It is located in the center of the crown, with equal distance from the dentinal walls.
• Mesiodistally, pulp chamber follows outline of the crown and it is ovoid in shape.
• Buccopalatally the pulp chamber is narrow as it transforms into the root canal with a
constriction just apical to the cervix.
• In young patient, central incisor has three pulp horns that correspond to enamel mamelons
on the incisal edge.
Root Canal
• Central incisor has one root with one root canal.
• Coronally, the root canal is wider buccopalatally.
• Coronally or cervically, the canal shape is ovoid in crosssection but in apical region, the
canal is round.
• The root canal differs greatly in outline in mesiodistal and labiopalatal view.
– Mesidistal view shows a fine straight canal.
– In labiopalatal view the canal is very much wider and often shows a constriction just apical
to the cervix.
• Usually lateral canals are found in apical third.
• Most of the time, the root of central incisor is found to be straight.
Clinical Considerations
• A pulp horn can be exposed following a relatively small fracture of an incisal corner in the
young patient.
• Placing the access cavity too far palatally makes straight line access difficult.
• Lateral canals are usually found in apical third.
• Most of canals are straight, but 15 to 20 percent of roots show labial or palatal curve. The
labial or palatal curve cannot be seen on routine radiograph, unless it is taken at different
horizontal angulations.
• Labial perforation is most commonly seen during access cavity preparation.
4
Fig. 4 Root canal anatomy of maxillary central incisor
(A) (B)
Fig. 5 (A) Root canal anatomy of young patient; (B) In older patient, pulp cavity decreases in size
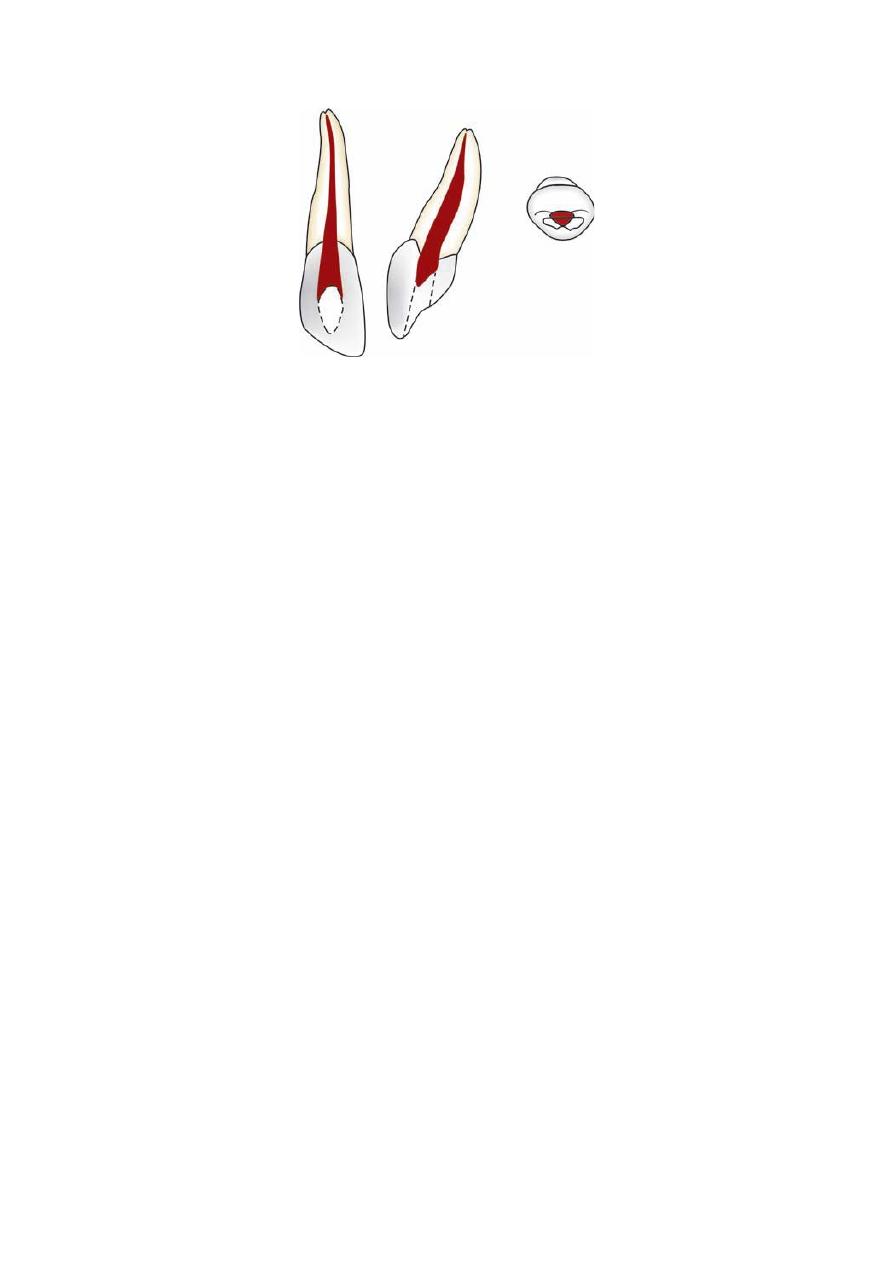
Maxillary Lateral Incisor (Fig.6)
Average Length: The average length of maxillary lateral incisor is 21 mm.
Pulp Chamber
The shape of pulp chamber of maxillary lateral incisor is similar to that of maxillary central
incisor but there are few differences.
• The incisal outline of the pulp chamber tends to be more rounded.
• Lateral incisor has two pulp horns, corresponding to the development mammelons.
Root Canal
• Root canal has finer diameter than that of central incisor though shape is similar to that.
• Labiopalatally, the canal is wider and usually shows constriction just apical to the cervix.
• Canal is ovoid labiopalatally in cervical third, ovoid in middle third and round in apical
third.
• Apical region of the canal is usually curved in a palatal direction.
Clinical Considerations
• Cervical constriction need to be removed during coronal preparation to produce a smooth
progression from pulp chamber to root canal.
• Since palatal curvature of apical region is rarely seen radiographically, during cleaning and
shaping ledge formation may occur at this curve. This may result in root canal filling short of
apex and other problems.
5
• Apical curvature can also complicate surgical procedures like root end cavity preparation
and root resection.
• Lateral canals are more common than maxillary central incisors.
• Most of the roots have distal curvature (> 50%).
• Labial perforation is most common error during access cavity preparation.
Fig. 6 Root canal anatomy of maxillary lateral incisor
Maxillary Canine (Fig. 7)
Average Tooth Length: Longest tooth: It is the longest tooth with an average length of 26.5
mm.
Pulp Chamber
• Labiopalatally, the pulp chamber is almost triangular shape with apex pointed incisally.
• Mesiodistally it is narrow, sometimes resembling a flame. Sometimes at cervix, there can be
constrictions.
• In cross-section it is ovoid in shape with larger diameter labiopalatally.
• Usually one pulp horn is present corresponding to one cusp.
Root Canal
• Normally there is single root canal which is wider labiopalatally than in mesiodistal aspect.
• Cross-section at cervical and middle third show its oval shape, at apex it becomes circular.
• Canal is usually straight but may show a distal apical curvature.
Clinical Considerations
• Cervical constriction needs to be shaped during coronal flaring to produce uniformly
tapered preparation.
• When long, sclerosed canal is being prepared, care must be taken to avoid blockage of the
root canal.
• Surgical access sometimes becomes difficult because of long length of the tooth.
• Almost 30 percent of roots show distal curve in the root.
• Lateral canals are present in apical third.
• Abscess of maxillary canine perforates the labial cortical plate below insertion of levator
muscles of the upper lip and drains into the buccal vestibule.
• If perforation occurs above the insertion of levator muscles of lip, drainage of abscess
occurs into the canine space, resulting in cellulitis.
6
Fig. 7 Maxillary canine
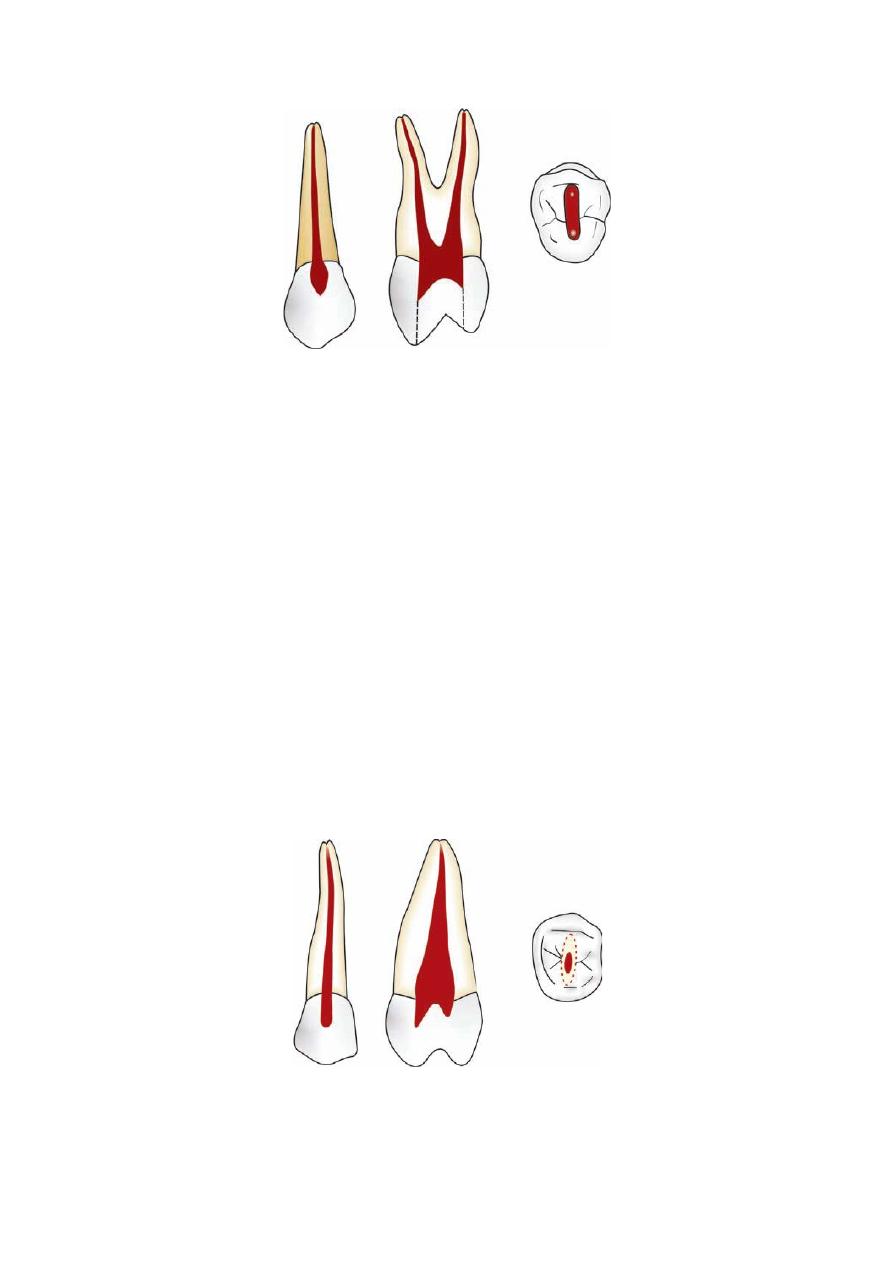
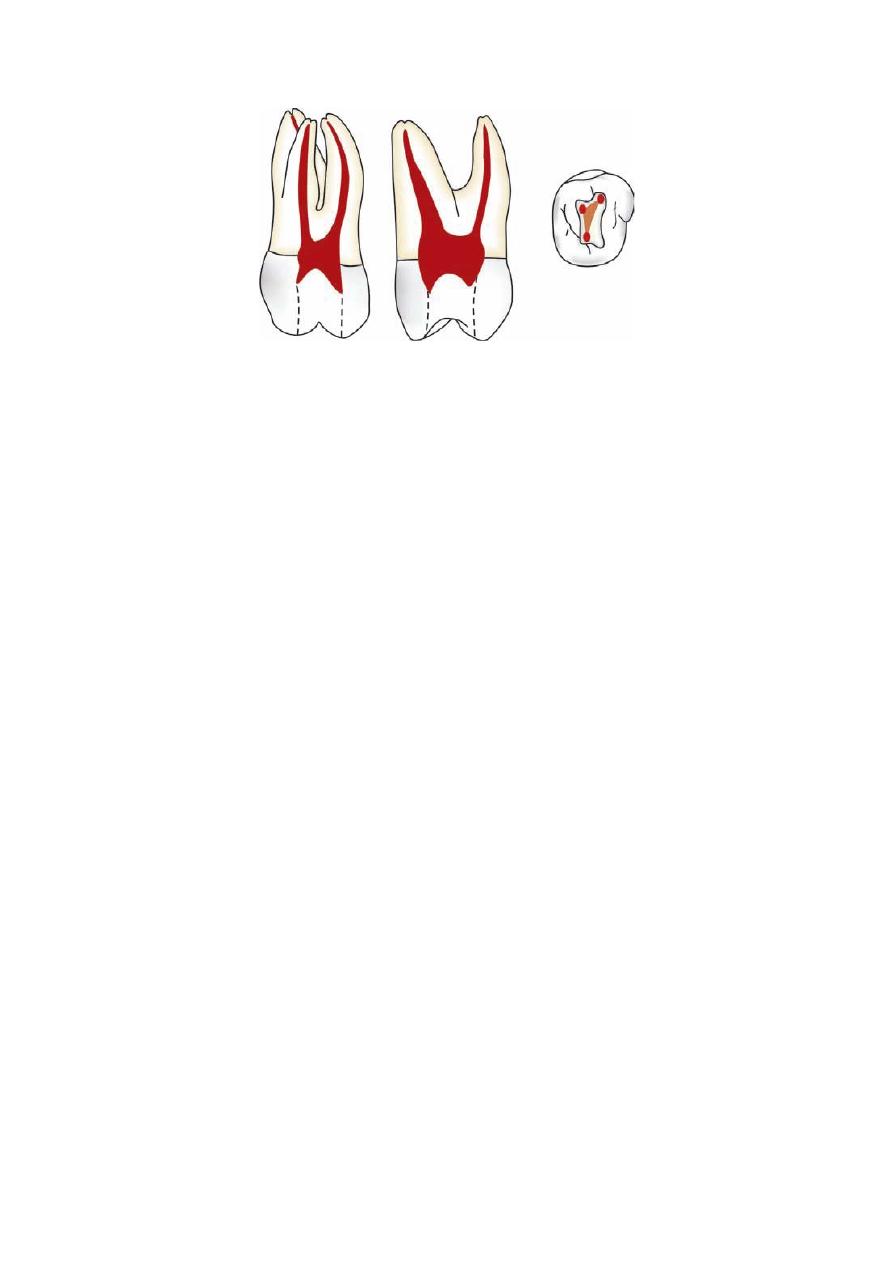
Maxillary First Premolar (Fig. 8)
Average Tooth Length: This tooth has generally two roots with two canals and average
length of 21 mm.
Pulp Chamber
• Pulp chamber is wider buccopalatally with two pulp horns, corresponding to buccal and
palatal cusps.
• Palatal canal is usually larger than buccal canal.
• The alveolar socket of maxillary first premolar is separated from maxillary sinus by a thin
layer of bone.
• Buccal surface of premolar lies close to buccal cortical plate. It may result in dehiscence or
fenestrations of that plate.
• Roof of pulp chamber is coronal to the cervical line
• Floor is convex generally with two canal orifices.
Root Canal
• Maxillary first premolar has two roots in most (> 60%) of the cases but cases with single
root or three roots have also been reported.
• Buccal canal is directly under the buccal cusp and palatal canal is directly under the palatal
cusp
• Cross-section of root canals shows ovoid shape in cervical third with larger dimensions
buccopalatally. At middle and apical third, canals show circular shape in cross-section
• The root canals are usually straight and divergent.
Clinical Considerations
• To locate both the canals properly, a good quality of radiograph should be taken from an
angle so as to avoid superimposition of canals.
• Avoid over flaring of the coronal part of the buccal root to avoid perforation of palatal
groove present on it.
• Surgical procedures on first premolar should be given more consideration since palatal root
may be difficult to reach.
• In maxillary first premolar, failure to observe the distal-axial inclination of the tooth may
lead to perforation.
• Palatal canal is usually larger than buccal canal.
• The alveolar socket of maxillary first premolar is separated from maxillary sinus by a thin
layer of bone.
• Buccal surface of premolar lies close to buccal cortical plate. It may result in dehiscence or
fenestrations of that plate.
7
Fig. 8 Maxillary first premolar
Maxillary Second Premolar (Fig.9)
Average length of maxillary second premolar is 21.5 mm.
Pulp Chamber
• Maxillary second premolar usually has one root with a single canal, but shape of canal
system is variable.
• Pulp chamber is wider buccopalatally and narrower mesiodistally.
• In cross-section, pulp chamber has narrow and ovoid shape.
Root Canal
• In more than 60 percent of cases single root with single canal is found. There may be a
single canal along entire length of the root.
• If there are two canals, they may be separated or distinct along the entire length of the root
or they may merge to form a single canal as they approach apically.
• Canal is wider buccopalatally forming a ribbon like shape.
• At cervix, cross-section shows ovoid and narrow shape, at middle third it is ovoid which
becomes circular in apical third.
Clinical Considerations
• Narrow ribbon like canal is often difficult to clean and obturate effectively
• If one canal is present, orifice is indistinct, but if two canals are present, two orifices are
seen.
• Care should be taken to explore, clean and obturate the second canal of maxillary second
premolar (40% of the cases).
Fig. 9 Maxillary second premolar

8
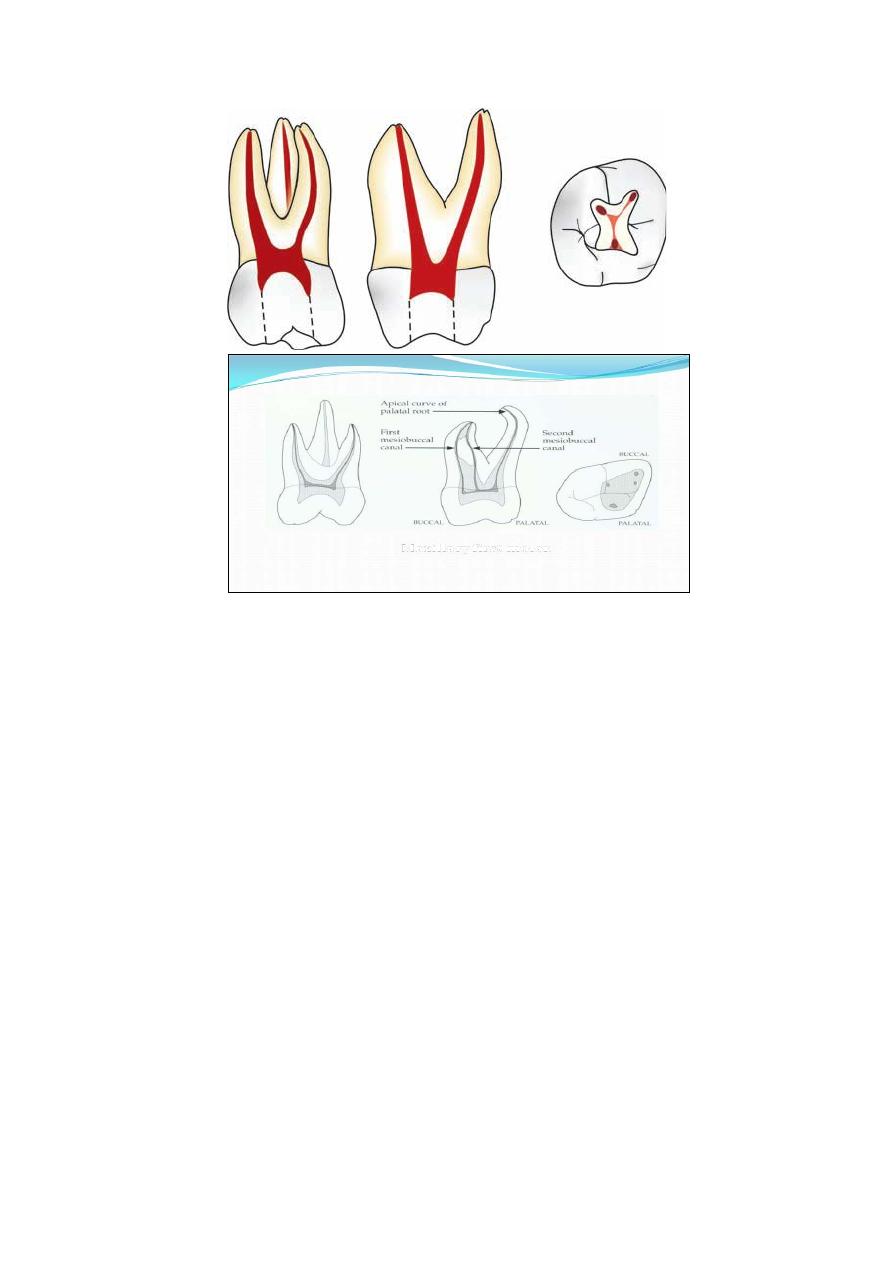
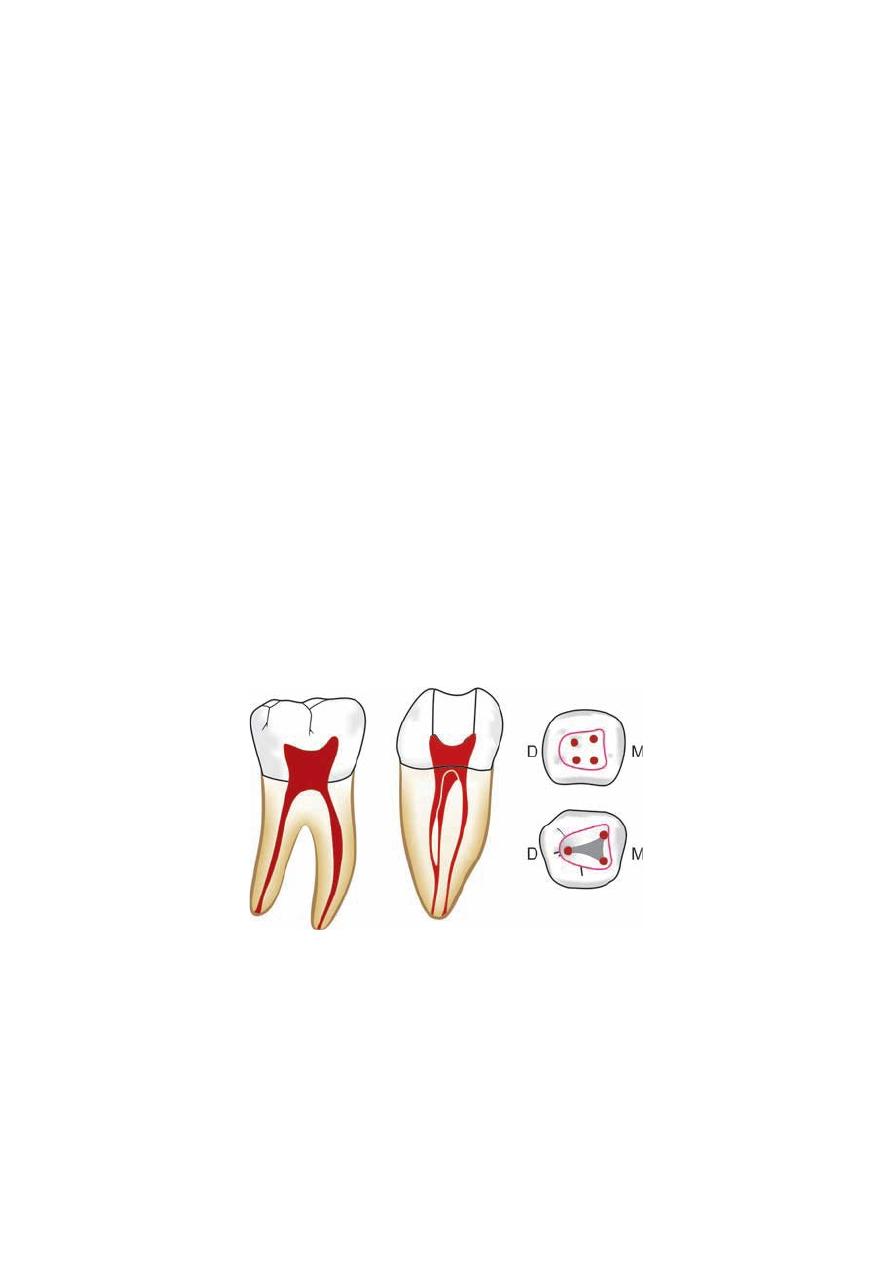
Maxillary First Molar (Fig. 10)
Average Tooth Length: The average tooth length of this tooth is 21 mm.
Pulp Chamber
• Largest pulp chamber: Maxillary first molar has the largest pulp chamber with four pulp
horns: mesiobuccal, mesiopalatal, distobuccal and distopalatal.
• Bulk of pulp chamber lies mesial to the oblique ridge across the surface of the tooth.
• The four pulp horns are arranged in such a fashion that gives pulp chamber rhomboidal
shape in the crosssection. The four walls forming roof converge towards the floor, where
palatal wall almost disappears making a triangular form in cross-section.
• Orifices of root canals are located in the three angles of the floor; palatal orifice is largest
and easiest to locate and appears funnel like in the floor of pulp chamber.
• Distobuccal canal orifice is located more palatally than mesiobuccal canal orifice
• More than 80 percent of maxillary first molars have shown the presence of two canals in
mesiobuccal root. MB2 is located 2 to 3 mm palatal to the MB1 canal, on an imaginary line
connecting MB1 and palatal canal.
Root Canal
• Maxillary first molar has generally three roots with three or four canals.
• Two canals in mesiobuccal root are closely interconnected and sometimes merge into one
canal.
• Mesiobuccal canal is the narrowest of the three canals, flattened in mesiodistal direction at
cervix but becomes round as it reaches apically.
• Distobuccal canal is narrow, tapering canal, sometimes flattened in mesiodistal direction but
generally it is round in cross-section.
• The palatal root canal has largest diameter which has rounded triangular cross-section
coronally and becomes round apically.
• Palatal canal can curve buccally in the apical one-third.
• Lateral canals are found in 40 percent of the molars at apical third and at trifurcation area.
Clinical Considerations
• Buccal curvature of palatal canal (56% of cases) may not be visible on radiographs, leading
to procedural errors.
• MB2 should be approached from distopalatal angle since the initial canal curvature is
mesial.
• Sometimes isthmus is present between mesiobuccal canals, it should be cleaned properly for
the success of treatment.
• Because of close proximity to sinus and buccal bony plate, any defect in bony prominences
may result in only periodontal ligament and mucoperiosteal lining of the sinus between roots
and the sinus. This can result in sinusitis because of pulpal disease or soreness in maxillary
teeth because of sinusitis.
• Mesiobuccal canals show curvature sometimes which is not visible radiographically.
• Since pulp chamber lies mesial to oblique ridge, pulp cavity is prepared usually mesial to
oblique ridge.
• Caries, previous restorative procedures, attrition, etc. can lead to formation of secondary
dentin causing alteration in pulp cavity. Therefore careful study of preoperative radio graphs
is mandatory to avoid any procedural errors.
• Perforation of palatal root is commonly caused by assuming canal to be straight.
9
Fig. 10 Maxillary first molar
Maxillary Second Molar (Fig. 11)
Average Tooth Length: The average tooth length of this tooth is 20 mm.
Pulp Chamber
• It is similar to maxillary first molar except that it is narrower Mesiodistally.
• Roof of pulp chamber is more rhomboidal in cross-section and floor is an obtuse triangle
• Mesiobuccal and distobuccal canal orifices lie very close to each other, sometimes all the
three canal orifices lie in a straight line.
Root Canal
• Similar to first molar except that in maxillary second molar roots tend to be less divergent
and may be fused
• Fewer lateral canals are present in roots and furcation area than in first molar.
Clinical Considerations
• Similar to maxillary first molar.
• Maxillary second molar lies closer to the maxillary sinus than first molar.
10
Fig. 11 Maxillary second molar
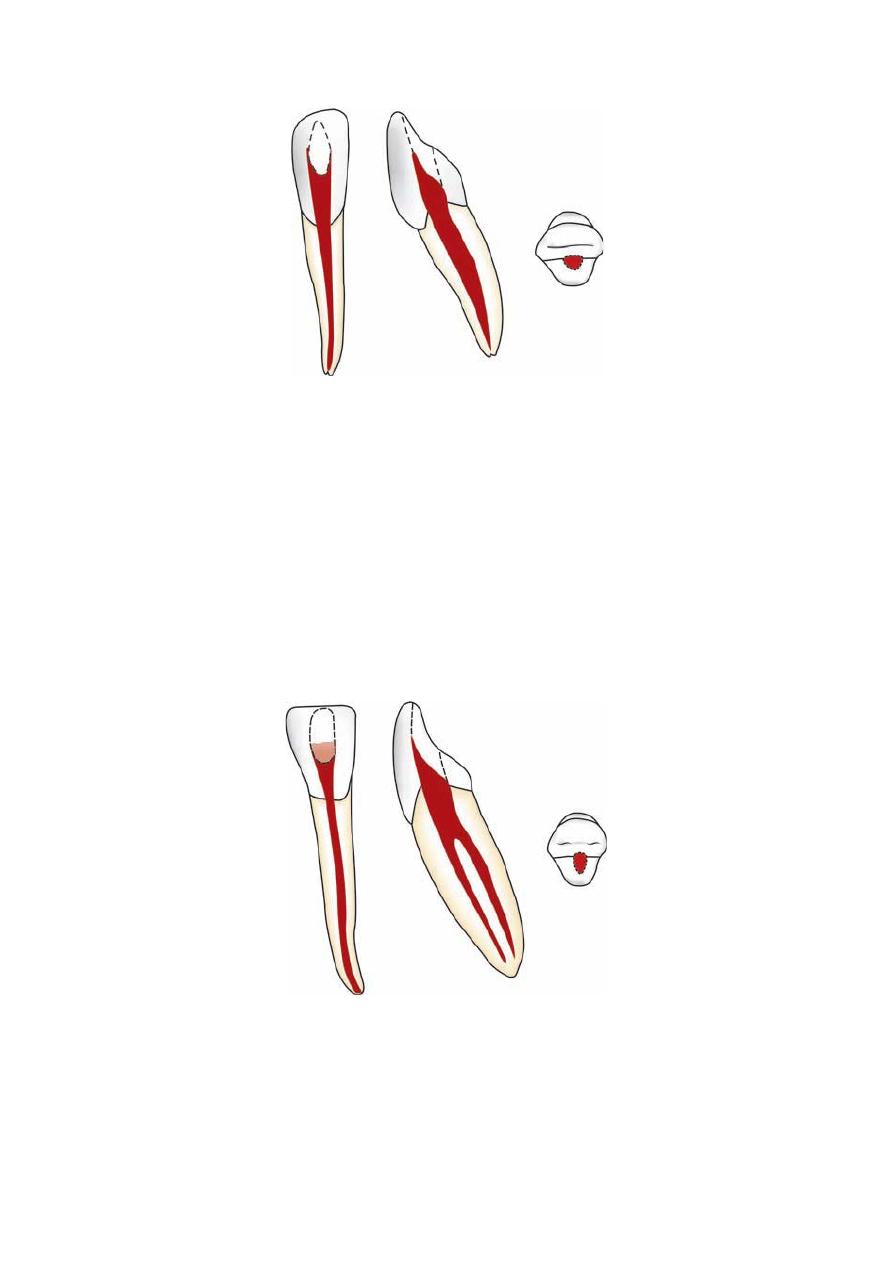
Mandibular Central Incisor (Fig. 12)
Average Tooth Length: Average length of this tooth is 21 mm.
Pulp Chamber
Smallest tooth in the arch: Mandibular central incisor is the smallest tooth in the arch.
• Pulp chamber is similar to maxillary central incisor being wider labiolingually and pointed
incisally with three pulp horns.
• Cross-section of pulp chamber shows its ovoid shape.
Root Canal
• Various root canal formations have been seen in mandibular incisors. There can be a single
canal from orifice to apex or a single canal by bifurcate into two canals or sometimes two
separate canals are also found. Incidence of two canals can be as high as 41 percent.
• Cross-section of root canals show wider dimension in labiolingual direction making it ovoid
shape whereas round in the apical third.
• Since canal is flat and narrow mesiodistally and wide buccopalatally, ribbon shaped
configuration is formed.
Clinical Considerations
• If root canals are overprepared, because of presence of groove along the length of root and
narrow canals, weakening of the tooth structure or chances of strip perforations are increased.
• It is common to miss presence of two canals on preoperative radiograph if they are
superimposed
• Second canal is usually found lingual to the main canal.
• Since apex of mandibular central incisor is inclined lingually, the surgical access may
become difficult to achieve.
11
Fig. 12 Mandibular central incisor
Mandibular Lateral Incisor (Fig. 13)
Average Tooth Length: Average length of mandibular lateral incisor is 21 mm.
Pulp Chamber
The configuration of pulp chamber is similar to that of mandibular central incisor except that
it has larger dimensions.
Root Canal
• It is almost similar to that of mandibular central incisor.
• Usually the root is straight or curved distally or labially, but distal curve is sharper than that
of mandibular central incisors.
Clinical Considerations
They are similar to central incisor.
Fig. 13 Mandibular lateral incisor
12
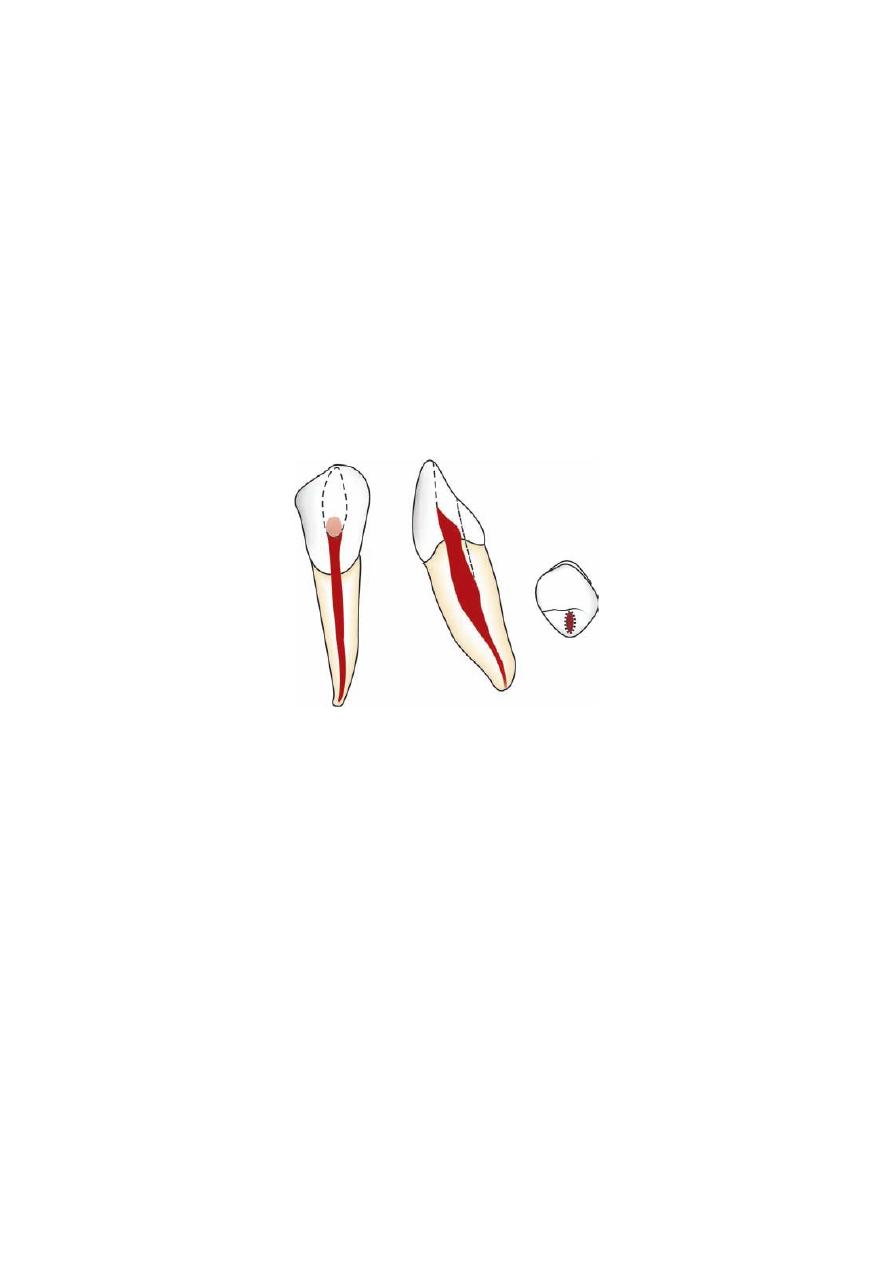
Mandibular Canine (Fig. 14)
• Average tooth length: Average length of the tooth is 22.5 mm
Pulp Chamber
• On viewing labiolingually, the pulp chamber tapers to a point in the incisal third of the
crown.
• In cervical third of tooth, it is wider in dimensions and ovoid in cross-section.
• Pulp chamber appears narrower mesiodistally.
• Cervical constriction is present.
Root Canal
• Mandibular canine usually has one root and one canal but can occasionally have two (14%
cases)
• Coronally, the root canal is oval in cross-section, becomes round in the apical region.
• Lateral canals are present in 30 percent of the cases.
Clinical Consideration
In older patients, where there is deposition of secondary dentine, it becomes necessary to
incorporate the incisal edge into the access cavity for straight line access.
Fig. 14 Mandibular canine
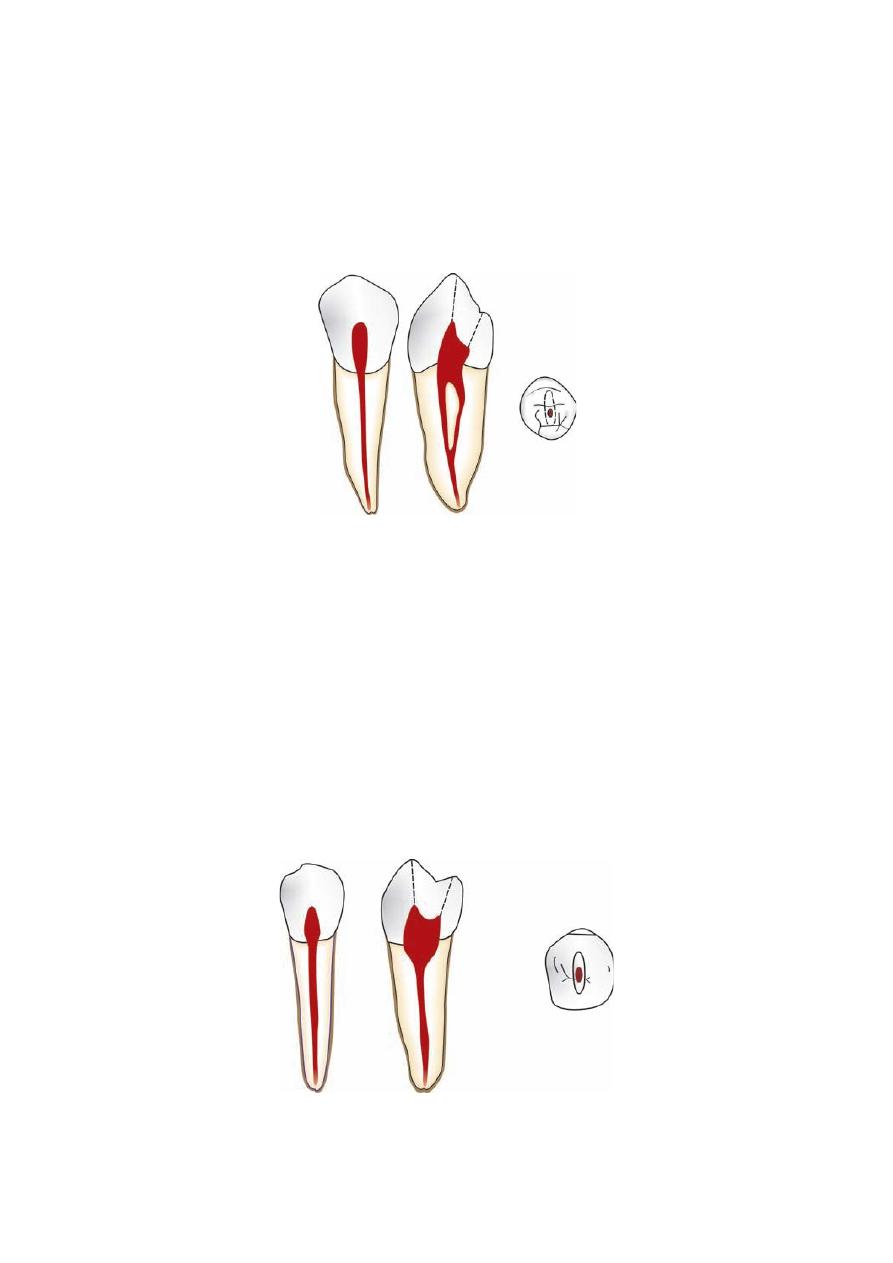
Mandibular First Premolar (Fig. 15)
Average Tooth Length: Average length of the tooth is 21.5 mm.
Pulp Chamber
• Mesiodistally, the pulp chamber is narrow.
• Pulp chamber has two pulp horns, the buccal horn being more prominent
• Buccolingually, the pulp chamber is wide and ovoid in cross-section.
Root Canal
• Mandibular first premolar has one root and one canal. Sometimes presence of second canal
can be seen.
• Mesiodistally, the canal is narrower.
• Buccolingually, root canal cross-sections tend to be oval but in apical area it becomes
round.
• Lateral canals are present in 44 percent of the cases.
Clinical Considerations
• The access cavity in mandibular first premolar extends on to the cusp tip, in order to gain
straight line access.
• Surgical access to the apex of the mandibular first premolar is often complicated by the
proximity of the mental nerve.
13
• Because of close proximity of root apex to mental canal and foramen, one may mimic its
radiographic appearance to periapical pathology.
• The lingual canal when present, is difficult to instrument. Access can usually be gained by
running a fine instrument down the lingual wall of the main buccal canal until the orifice is
located.
• Apical perforation should be avoided by taking care of buccal curvature of the canal at the
apex.
Fig. 15 Mandibular first premolar
Mandibular Second Premolar (Fig. 16)
Average Tooth Length: The average length of this tooth is 22.5 mm.
Pulp Chamber
• It is similar to that of mandibular first premolar except that lingual pulp horn is more
prominent.
• Cross-section of pulp chamber shows oval shape with greater dimensions buccolingually.
Root Canal
• Usually has one root and one canal but in 11 percent of the cases, a second canal can be
seen.
• Buccolingually, it is wider than that of mandibular first premolar.
• Root canal cross-sections tend to be oval coronally and round apically.
Clinical Consideration
They are similar to mandibular first premolar.
Fig. 16 Mandibular second premolar
14
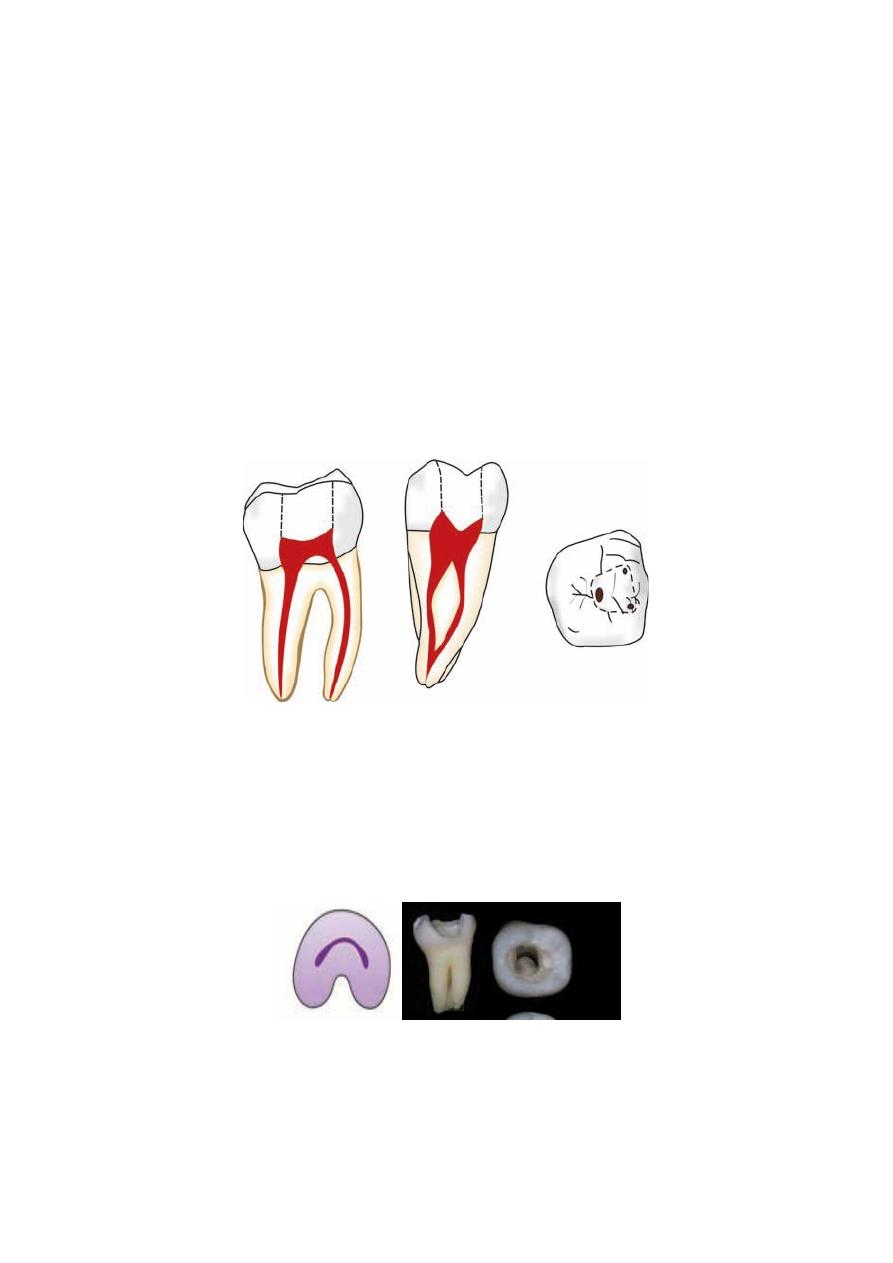
Mandibular First Molar (Fig. 17)
Average Tooth Length: The average length of this tooth is 21 mm.
Pulp Chamber
• It is quadrilateral in cross-section at the level of the pulp floor being is wider mesially than
distally.
• The roof of the pulp chamber is rectangular in shape with straight mesial wall and rounded
distal wall.
• There may be presence of four or five pulp horns.
• Mesiobuccal orifice is present under the mesiobuccal cusp.
• The mesiolingual orifice is located in a depression formed by mesial and the lingual walls.
Usually a connecting groove is present between mesiobuccal and mesiolingual orifices.
• Distal orifice is the widest of all three canals. It is oval in shape with greater diameter in
buccolingual direction.
Root Canal
Mandibular first molar has two roots with three canals. But teeth with three roots and four or
five canals have also been reported.
• Mesial root has two canals: mesiobuccal and mesiolingual with two foramina (> 41%
cases), or single foramen (30%) and in different pattern.
• Mesiobuccal canal is usually curved.
• Distal root generally has one canal (> 70% cases), but two canals are also seen in some
cases.
• A single distal canal is ribbon shaped and has larger diameter buccolingually. But when two
canals are present in distal root, they tend to be round in the cross-section.
Clinical Considerations
• Over-enlargement of mesial canals should be avoided to prevent procedural errors.
• To avoid superimposition of the mesial canals, radio graph should be taken at an angle.
Fig. 17 Mandibular first molar
15
Mandibular Second Molar (Fig. 18)
Average Tooth Length: The average length of this tooth is 20 mm.
Pulp Chamber
• It is similar to that of mandibular first molar except that it is smaller in size.
• Root canal orifices are smaller and lie closer.
Root Canal
• Usually mandibular second molar has two roots with three canals but variations are also
seen.
• C-shaped canals are also seen, i.e. mesial and distal canals become fused into a fine canal.
Clinical Considerations
• C-shaped canals make the endodontic procedures difficult so care should be taken while
treating them.
• There may be only one mesial canal. The mesial and distal canals may lie in midline of the
tooth.
• Perforation can occur at mesio-cervical region if one fails to recognize the mesially tipped
molar.
Fig. 18 Mandibular second molar
C-shaped canals (Fig 19)
• These are named C-shaped because of their morphology.
• Pulp chamber in C-shaped molar is single ribbon shaped with 180° arc or more.
• This type of canal is usually found in mandibular molars.
Fig. 19 C-shaped canal