
1
Acute Coronary Syndrome
(ACS):
Unstable Angina/ Non-ST
Elevation Myocardial Infarction
UA/NSTEMI

Objectives
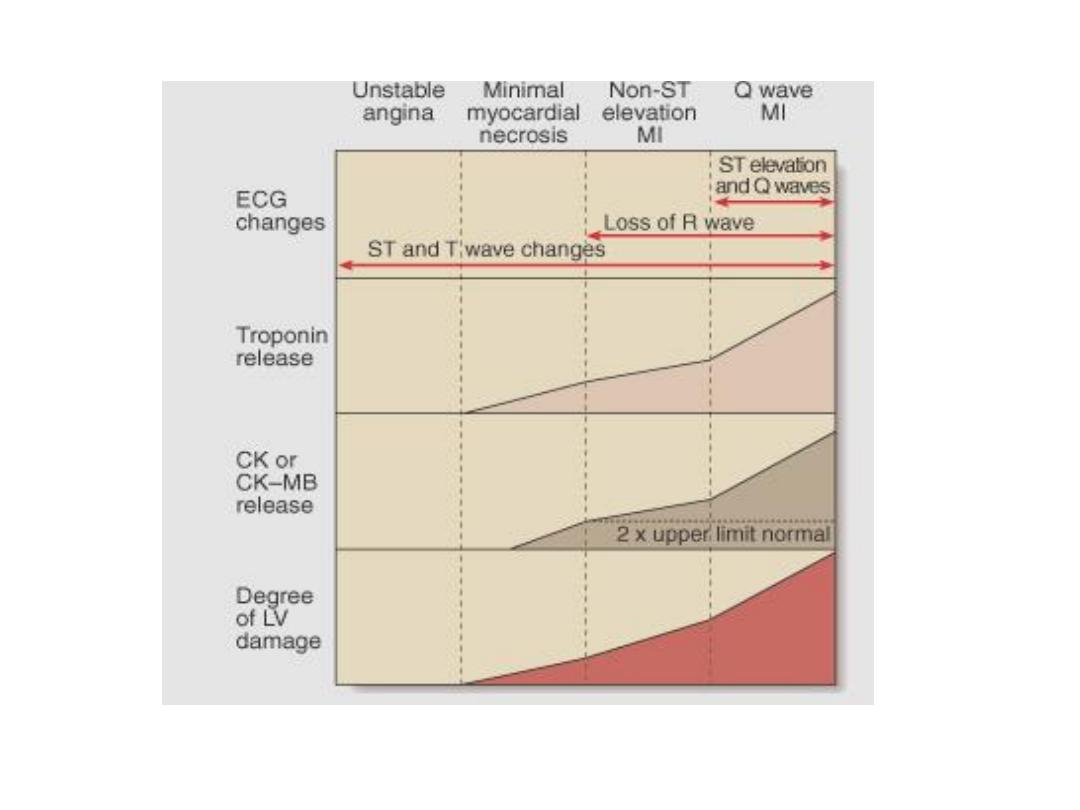
• ACS can present as unstable angina,
NSTEMI, and STEMI
• The above division is based on the
ECG and s.troponin
• The difference in clinical presentation
between STEMI and NSTEMI depends
on whether the obstruction is
complete or partial.
2

objectives
• Life-long medication is essential to
improve long term outcomes
3
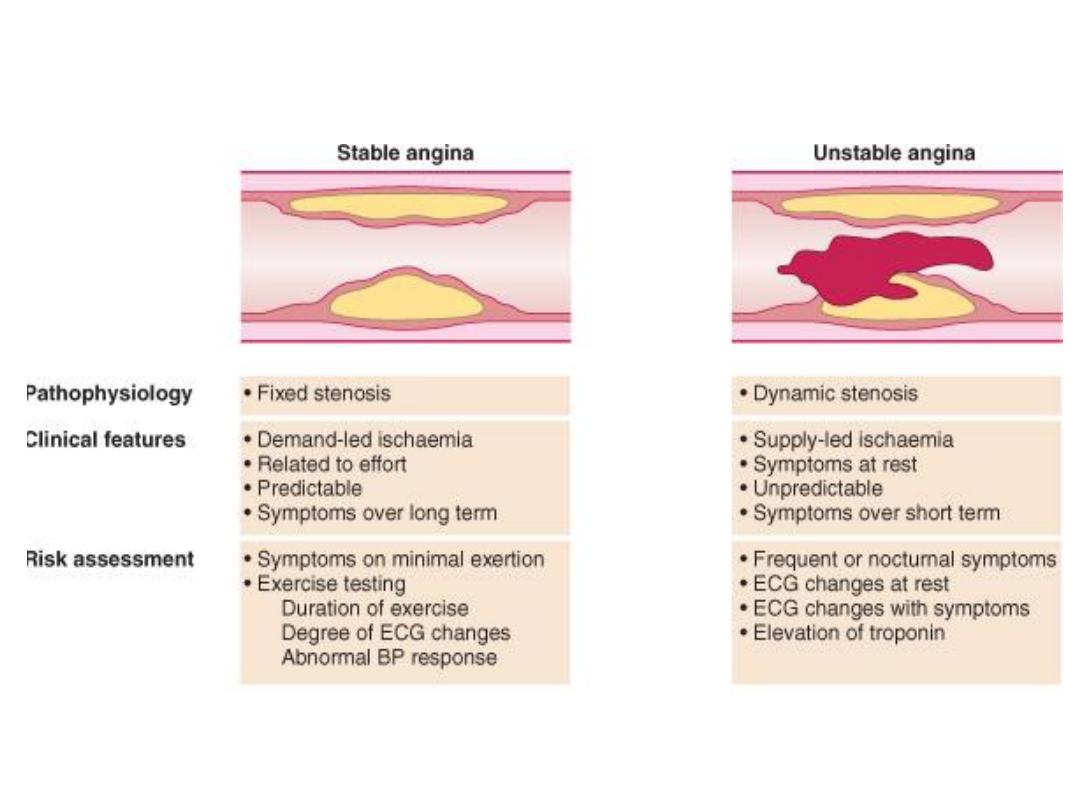
UA/NSTEMI
Definition:
unstable angina is ischemia
caused by dynamic
obstruction of a coronary
artery by vessel spasm or
plaque rupture and
superimposed thrombus
4

5
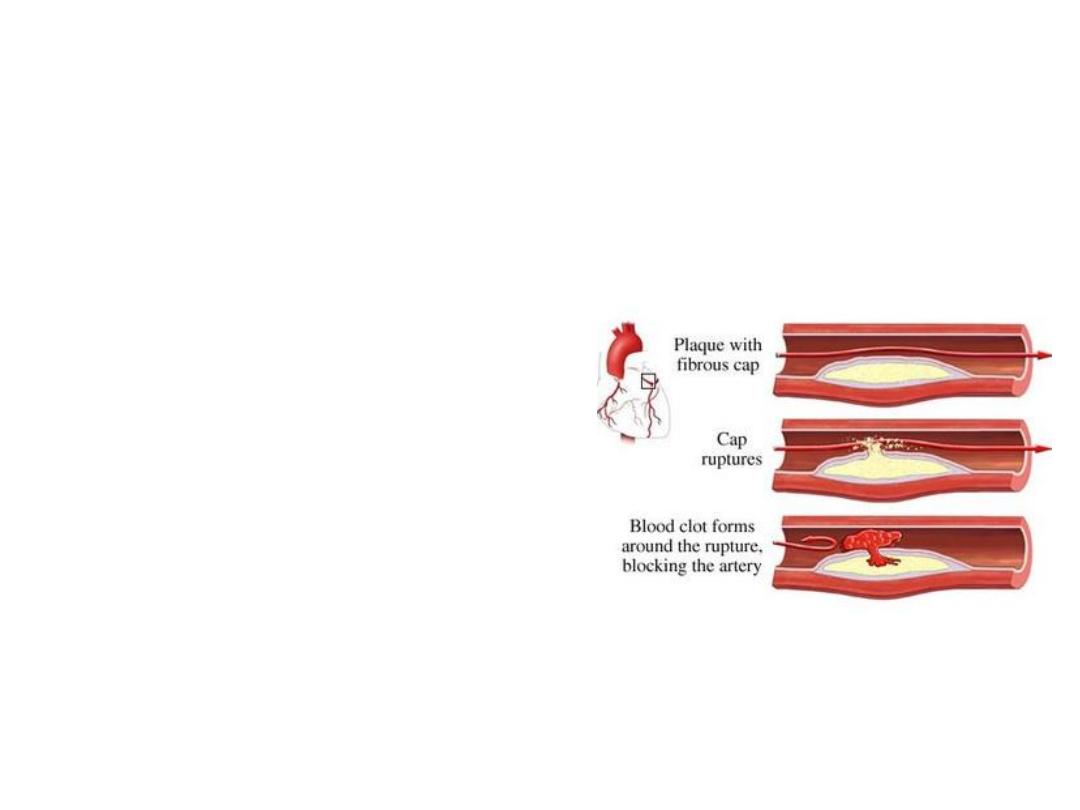
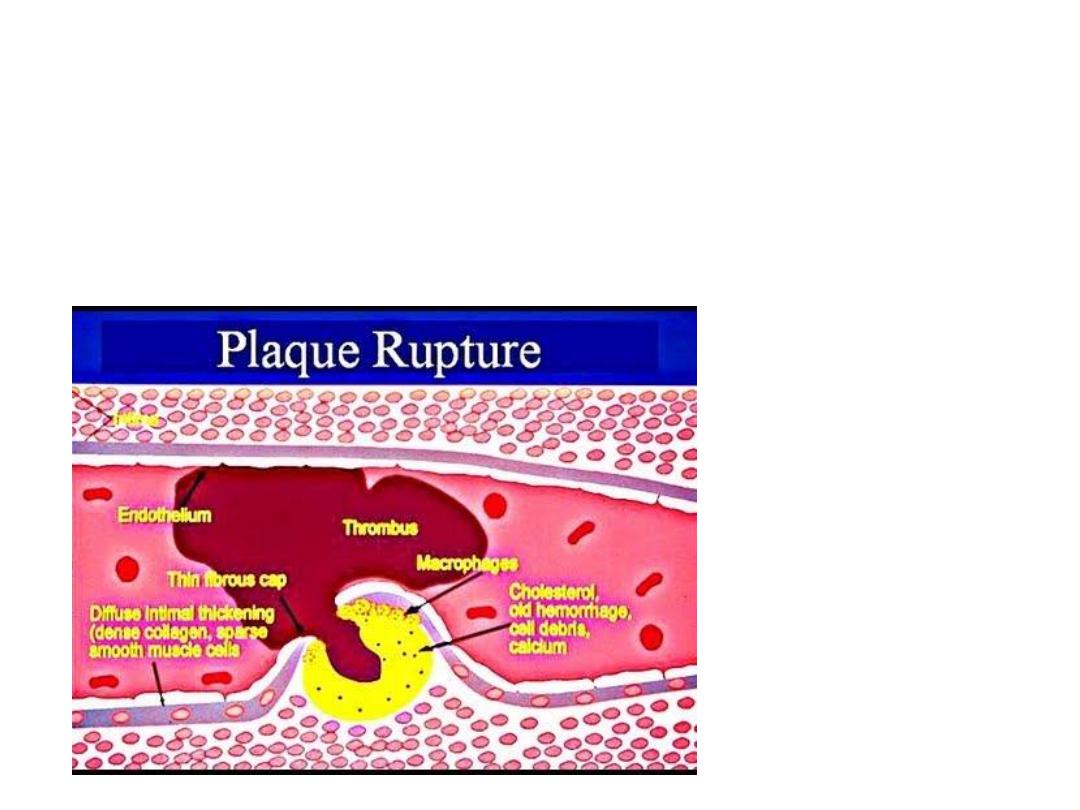
Pathophysiology
• Similar to that of acute myocardial
infarction (AMI)
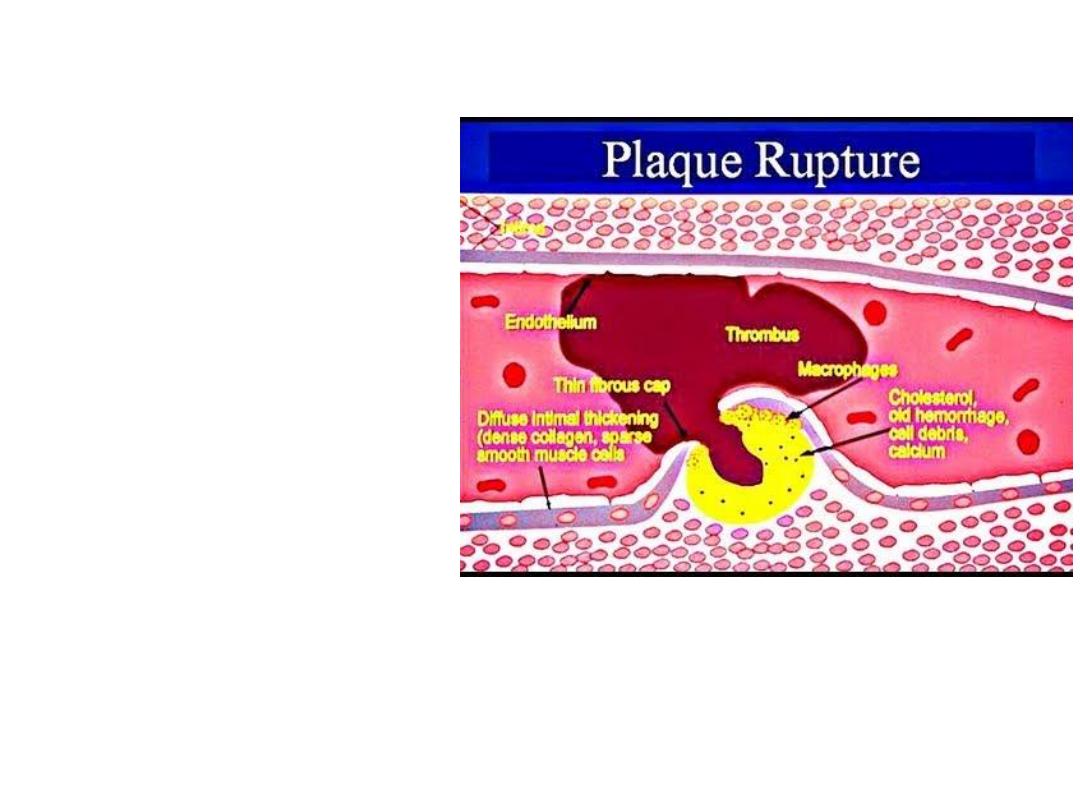
Pathophysiology
Thrombus
developing on top
of an ulcerated,
fissured, or
ruptured
atherosclerotic
plaque
6

Unlike AMI (STEMI), thrombus is usually
non-occlusive
NSTEMI
STEMI
7
8

9
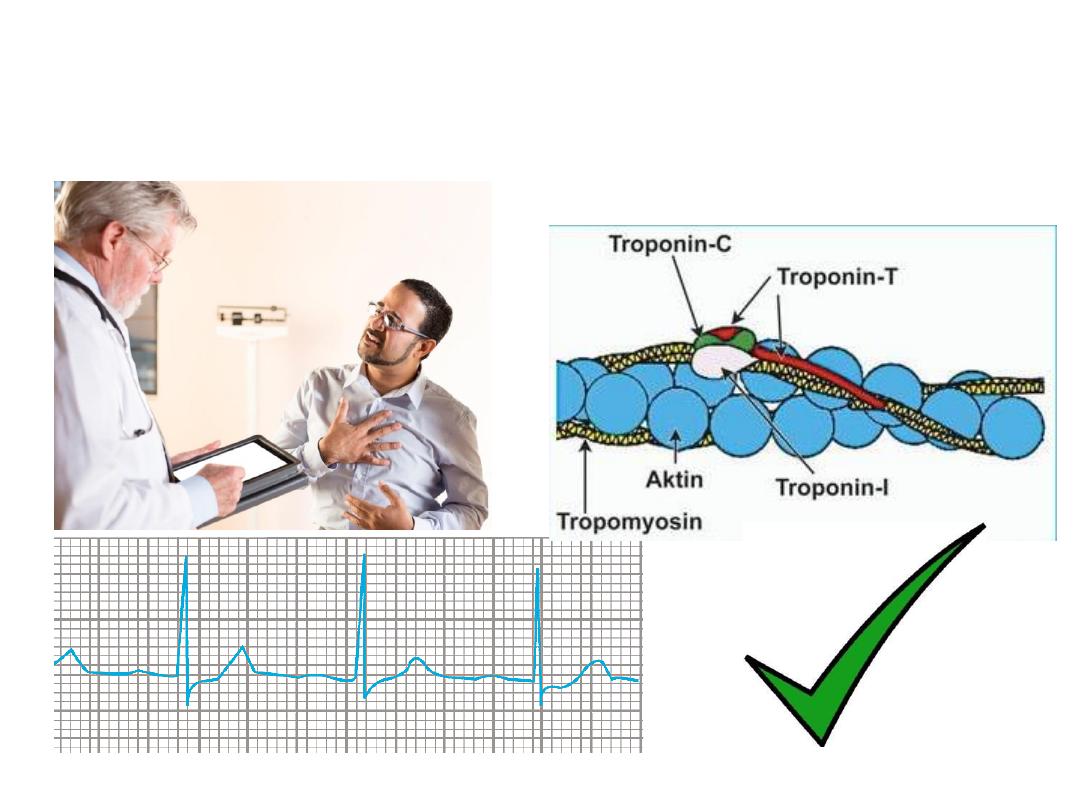
Pathophysiology
• In UA/NSTEMI, thrombus is mainly
composed of platelets
• In STEMI, the thrombus is composed
mainly of fibrin
• The condition is no longer an imbalance
between myocardial blood supply and
demand, since chest pain is present
• A at rest
10
11
Acute Coronary syndrome Vs
Stable Angina

Components of ACS: Clinical
Differentiation
• Unstable angina
• Non-ST segment myocardial infarction
(NSTEMI)
• ST-elevation MI (STEMI)
12
Unstable angina: pain at rest, NO
ECG changes, troponin normal
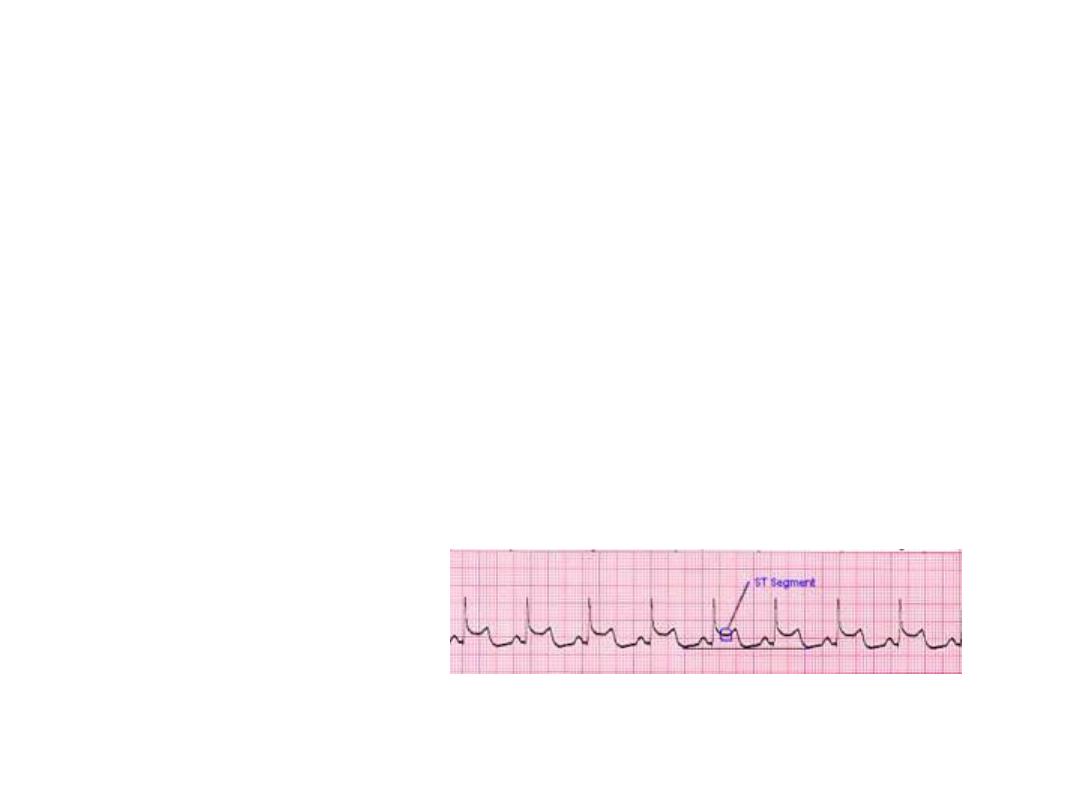
13
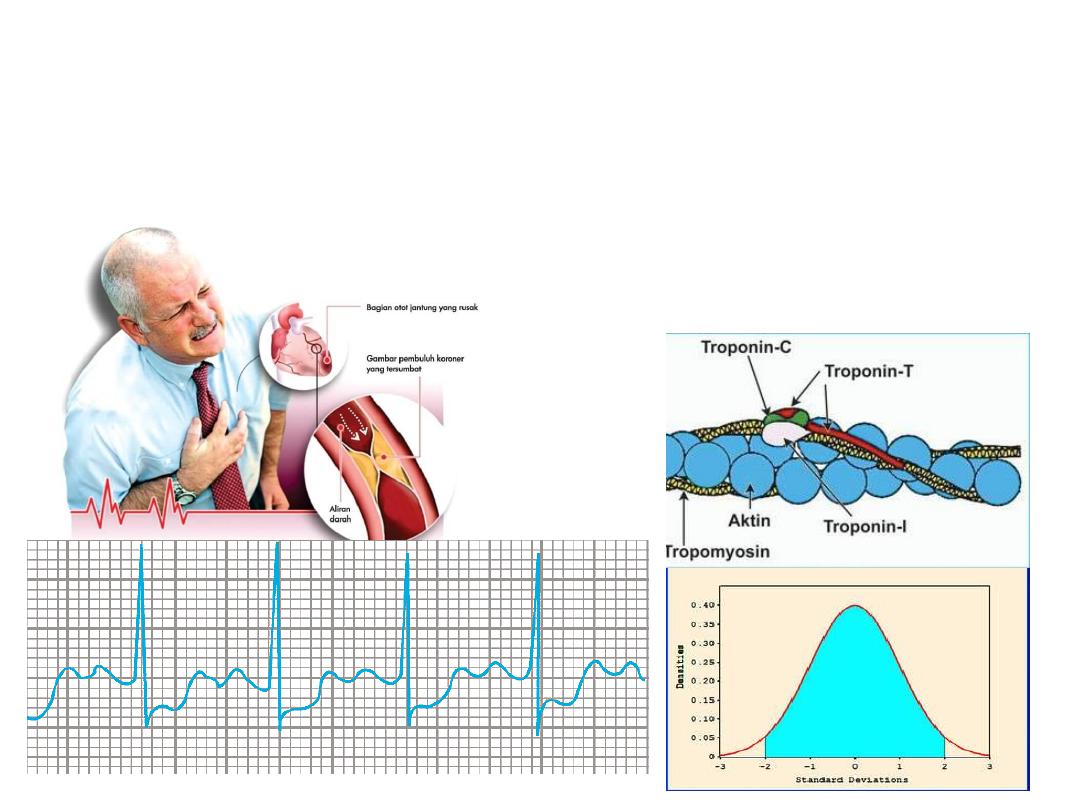
NSTEMI: chest pain, ECG normal
or shows ST-Depression, troponin
increased
14
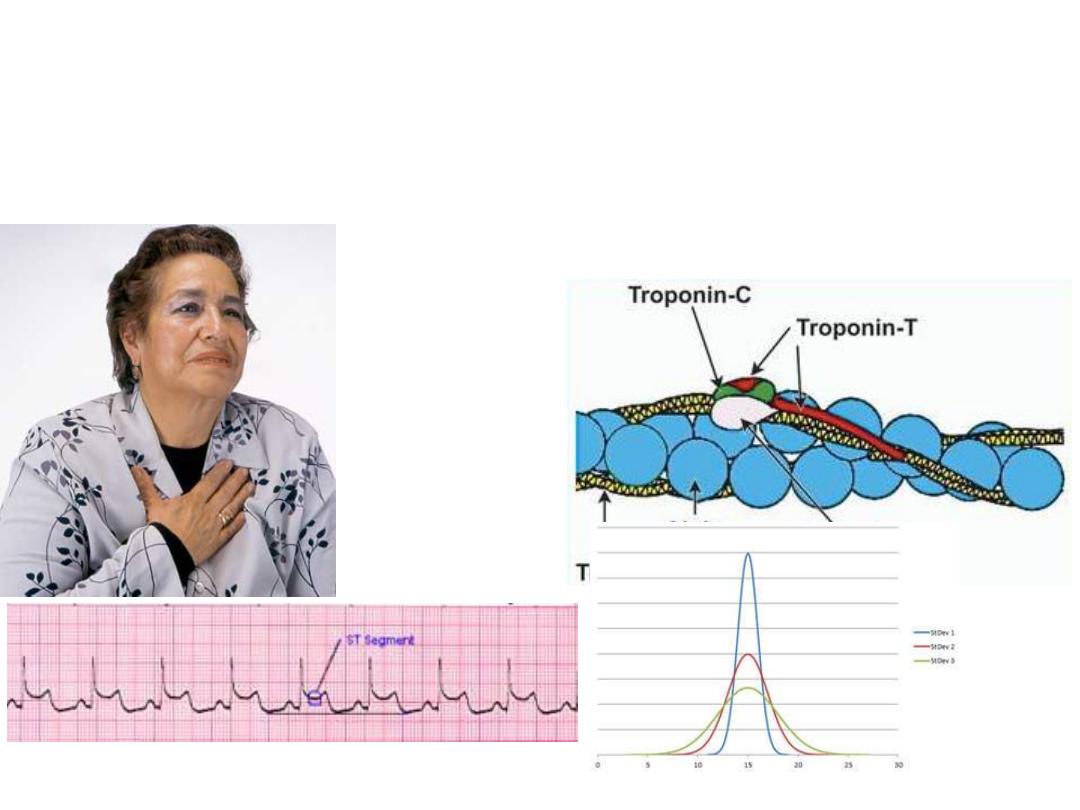
STEMI: chest pain, ECG shows ST
elevation, troponin high
15
16
NSTEMI
STEMI
17

18
Definition
• Prolonged angina (> 20 minutes)
• New onset (de novo) severe angina
(within 3 months)
• Recent destabilization of previously
stable angina: angina at rest
• Post MI angina

19
Clinical Features: Symptoms
• Anginal pain
– Rest pain
– Nocturnal angina
– Minimal exertion
• Sweating
• Nausea
• Abdominal pain
• Syncope

20
Clinical Features: Signs
Depend on the severity of the
condition and the state of LV function
• Can be unremarkable
• Severe anxiety
• Pallor
• Sweating
• S3 & S4 gallop
• Crepitations

21
UA/NSTEMI: Risk Stratification
Depends on
• Clinical
• ECG
• & Biochemical criteria

Clinical Criteria of Poor Px
• Old age
• Diabetes mellitus
22
Clinical Criteria of Poor Px
• Recurrent, prolonged chest pain at
rest
• Post MI angina
• Congestive heart failure
• Mitral regurgitation
23
24
ECG Criteria of Serious Disease
• Arrhythmias
• Widespread ST depression
• Transient ST elevation (< 30 min)
Biochemical Criteria for Px
Plasma troponin level:
• > 0.1 µg/l correlates
with serious disease
and poor prognosis
(extensive myocardial
damage)
• < 0.1 µg/l correlates
with low risk
25

26
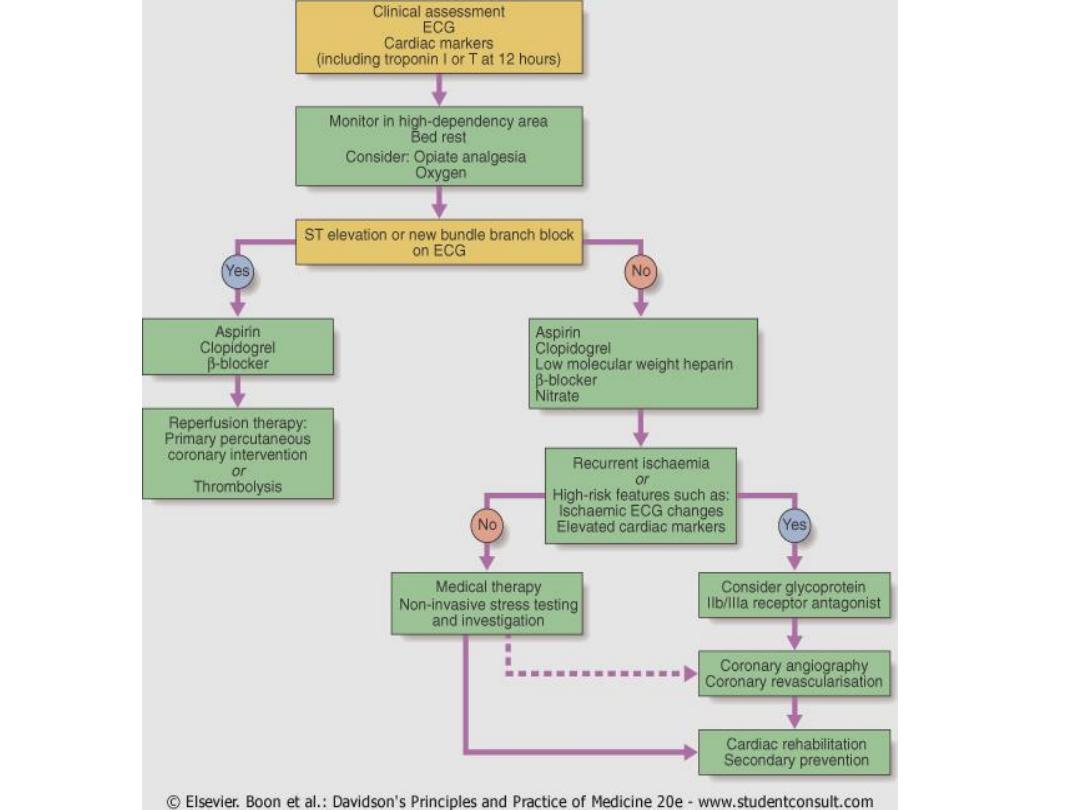
UA/NSTEMI: Management
• Urgent admission to hospital
• IV line
• Bed rest
• Oxygen if O2 saturation < 90%
• Detect and treat any precipitating
condition:
– Hypertension
– Tachycardia
– Anemia, thyrotoxicosis

27
UA/NSTEMI: Management
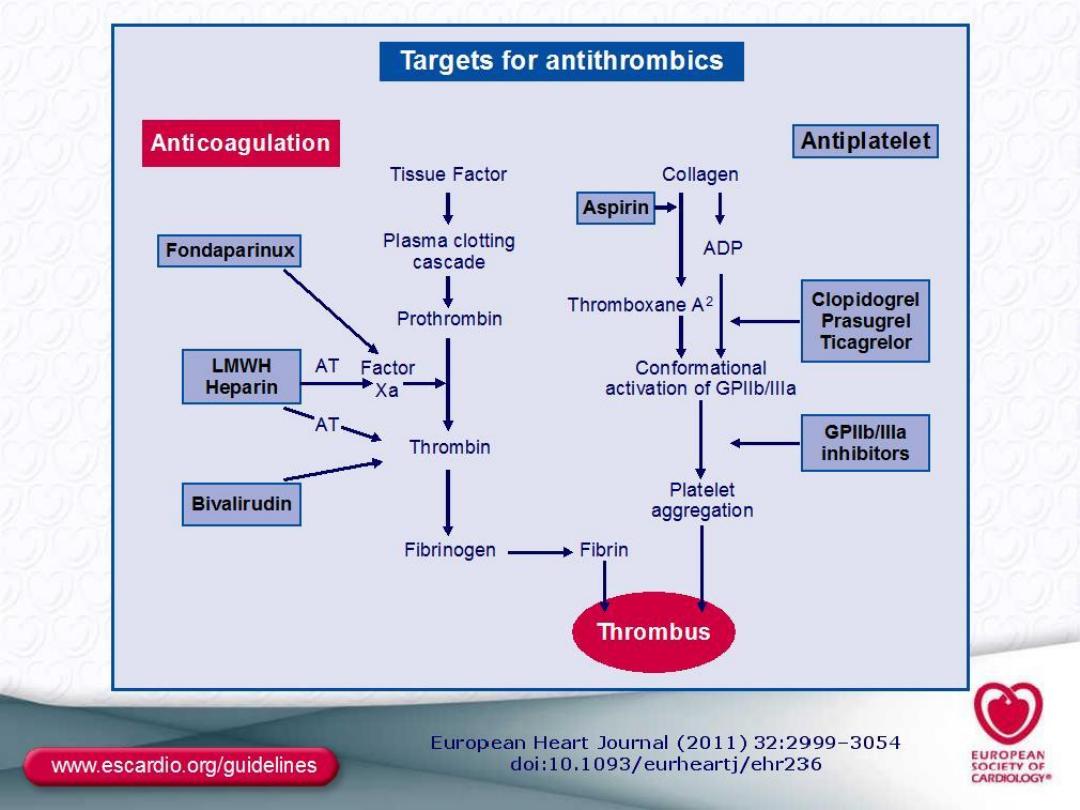
• Aspirin: 300 mg initially followed by
100 mg daily
• Clopidogrel
• Anticoagulation:
– Unfractionated heparin
– Low molecular weight heparin
– Bivaluridin


30
UA/NSTEMI: Management
• Oral beta blockers: especially if
tachycardia or hypertension without
signs of heart failure
• Nitrates: oral or intravenous,
according to severity.
– Used cautiously if BP< 90mmHg

UA/NSTEMI: Management
• ACE inhibitors
• Statins
31

32
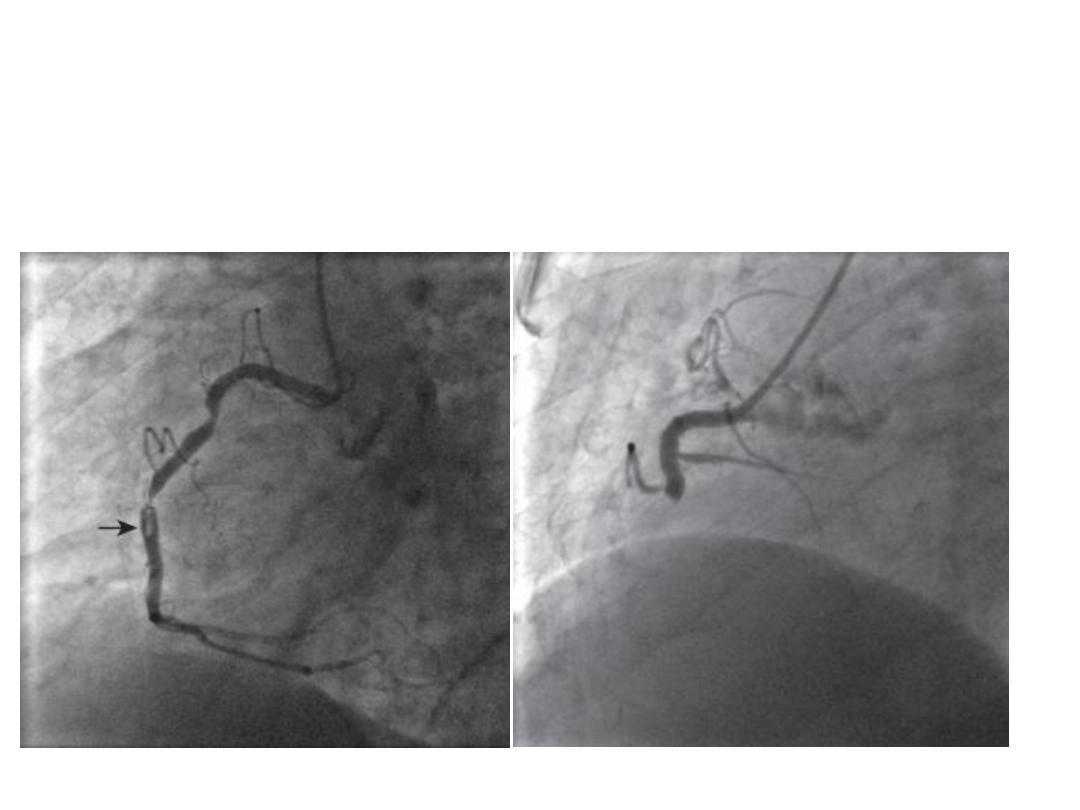
Management of the High Risk
Patient
• Early invasive strategy: PCI or CABG
• Done under cover of GP IIb-IIIa
antagonists: abciximab, tirofiban,
eptifibatide
• Thrombolytic therapy?
– Not useful (why?)
– May be harmful
33

Steps in Managements
• Optimized medical treatment
• If patient is still unstable:
invtervention
• If chest pain resolves: kept in
hospital for 3-5 days, then before
discharge ETT done at modified
workload
34

• If predischarge ETT positive;
intervention
• If predischarge ETT negative: patient
sent home on treatment, then ETT
repeated at full workload after 6
weeks
35

• If full workload ETT positive:
intervention
• If negative: medical therapy, with
regular check ups
36

Log Term Treatment
• LIFELONG treatment with:
• Aspirin
• Beta blockers
• Statin
• ACE inhibitor or ARB
• In addition to one-year treatment
with clopidogrel
37