
Back Pain
Examination, assessment, red flags,
20
20
-2019
Babylon collage of medicine

What factors are associated with
development of low back pain?
Work that requires heavy lifting; bending and twisting; or whole-body
vibration, such as truck driving
Physical inactivity
Obesity
Arthritis or osteoporosis
Pregnancy
Age >30 years
Bad posture
Stress or depression
Smoking

•
Factors associated with development of low back pain include obesity, physical inactivity,
occupational factors, and depression and other psychological conditions (see the Box:
Factors Associated With Low Back Pain or Disability Claims for Low Back Pain). Such
strategies as maintaining normal body weight, exercising, and avoiding activities that can
injure the back may decrease risk for low back pain, but direct evidence of the value of
such interventions is not available.
•
Clinicians should remember that back pain (the symptom), a health care visit for back
pain, and work loss or disability due to back pain do not necessarily reflect the same
underlying construct. Symptom severity does not correlate well with health care seeking
or functional outcome.
•
Factors Associated With Low Back Pain or Disability Claims for Low Back Pain
•
Work that requires heavy lifting; bending and twisting; or whole-body vibration, such as
truck driving
•
Physical inactivity
•
Obesity
•
Arthritis or osteoporosis
•
Pregnancy
•
Age >30 years
•
Bad posture
•
Stress or depression
•
Smoking

What serious underlying systemic conditions should clinicians
consider?
•
Compression fracture
– Associated with older age, white race, trauma, prolonged
corticosteroid use
Nonskin cancer
Hx cancer: strongest risk factor for cancer-related back pain
Also: unexplained weight loss, no relief with bed rest, pain
lasting >1 month, increased age
Ankylosing spondylitis
≥4 of following: morning stiffness, decreased discomfort
with exercise, onset of back pain before age 40, slow
symptom onset, pain persisting >3 months
Osteomyelitis
History of IV drug use, recent infection, fever

• Underlying systemic disease that causes back pain is rare but must be
considered. Prevalence is 4% for compression fracture, less than 1% for nonskin
cancer, 0.3% for ankylosing spondylitis, and 0.01% for infection (9). A history of
cancer is the strongest risk factor for cancer-related back pain; other factors,
such as unexplained weight loss, no relief with bed rest, pain lasting more than
1 month, and increased age are also risk factors but only increase risk slightly.
Osteomyelitis should be considered if there is a history of intravenous drug use,
recent infection, or fever. Increased age, white race, trauma, or prolonged
corticosteroid use are associated with compression fractures. Patients with at
least 4 of the following characteristics require further evaluation for ankylosing
spondylitis: morning stiffness, decreased discomfort with exercise, onset of
back pain before age 40 years, slow symptom onset, and pain persisting for
more than 3 months. However, because of the low prevalence of ankylosing
spondylitis, the positive predictive value of these characteristics is still low. The
absence of any of these worrisome features is highly sensitive but not specific
for excluding patients with systemic illness. The presence of these features may
indicate a need for further evaluation .

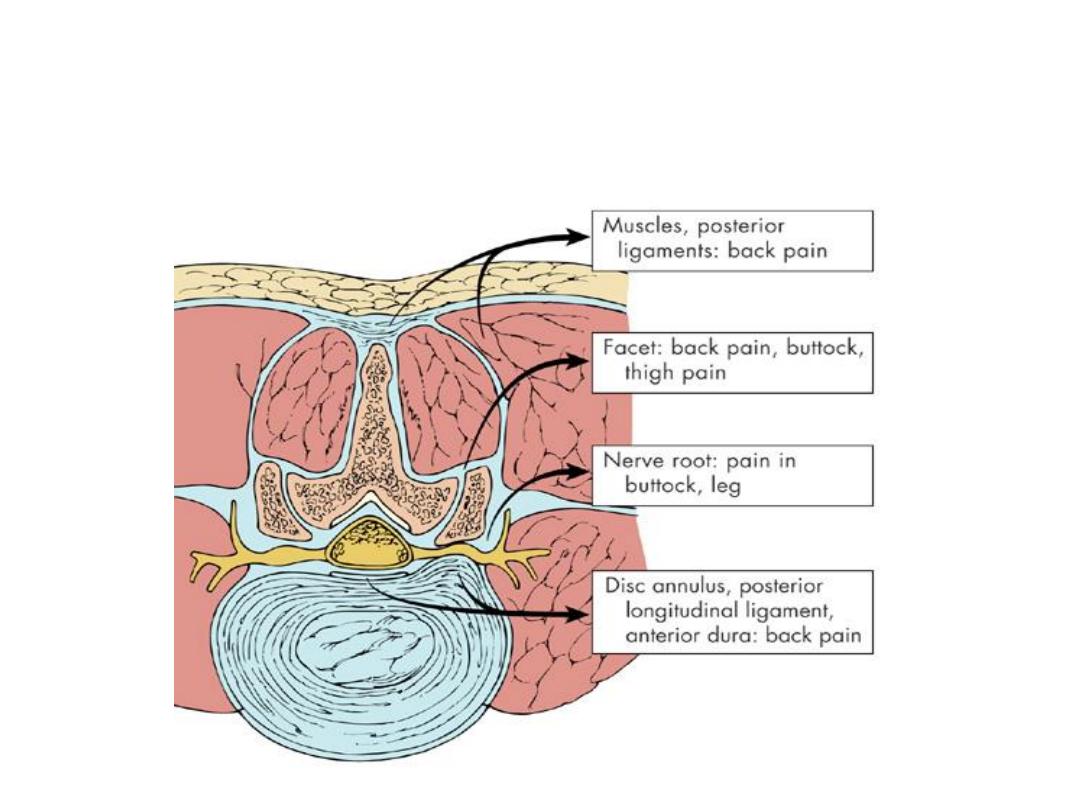
Causes of back pain 1
Mechanical - Muscles and ligaments
Local tenderness, muscle spasm, loss of lumbar
lordosis, percussion tenderness over spinous
process
NO MOTOR/SENSORY/REFLEXIC LOSS
Causes of back pain 1
What factors should lead clinicians to suspect nerve root
involvement?
Consider if patient presents with back & leg pain
The more distal the pain radiation, the more specific the
symptom for nerve root involvement
Pain that radiates from the back through the buttocks to
the legs (sciatica) is common
Severe or progressive motor deficits warrant urgent
evaluation (regardless of origin)
Symptoms of vascular claudication (not stenosis): leg pain
with exertion, rather than with changes in
position

• When patients present with back and leg pain, nerve root
involvement must be considered. Nerve root involvement can
cause neurologic compromise at the level of the nerve root
(common causes include lumbar disk herniation in patients
younger than 50 years and spinal stenosis in older patients) or the
upper motor neuron (causes include tumor or central disk
herniation). Nerve root involvement of the cauda equina, or the
area below the termination of the spinal cord, requires immediate
imaging and surgical evaluation to prevent permanent neurologic
damage. Signs and symptoms of the cauda equina syndrome
include bowel or bladder dysfunction and saddle anesthesia. When
upper motor neurons are involved due to compression of the
spinal cord above the conus medullaris, urgent specialist
consultation is also required (9). Signs and symptoms that suggest
upper motor neuron involvement include weakness, decreased
motor control, altered muscle tone, and spasticity or clonus.
Presence of severe or progressive motor deficits generally warrants
urgent evaluation, regardless of the origin.

• Patients with leg pain that is worse than back pain, a positive straight leg–raising
test result, and unilateral neurologic symptoms in the foot are very likely to have
nerve root compression as the source, most frequently from a herniated disk.
The most common sites for lumbar disk herniation are at L4–5 or L5–S1. Pain
that radiates from the back through the buttocks to the legs (sciatica) is
common, and the more distal the pain radiation, the more specific the symptom
is for nerve root involvement. Other common symptoms of disk herniation
include weakness of the ankle and great toe dorsiflexors, loss of ankle reflex,
and sensory loss in the feet. Causes of leg pain that may coexist with low back
pain but are not due to nerve root compression include the piriformis syndrome,
iliotibial band syndrome, trochanteric bursiti, and hip osteoarthritis.
• Spinal stenosis can also result in bilateral nerve root compression. Symptoms of
vascular claudication can be difficult to distinguish from spinal stenosis but are
characterized by leg pain that occurs with exertion rather than with changes in
position. Clinicians should consider vascular disease in patients with risk factors
for cardiovascular disease before attributing symptoms to spinal stenosis.

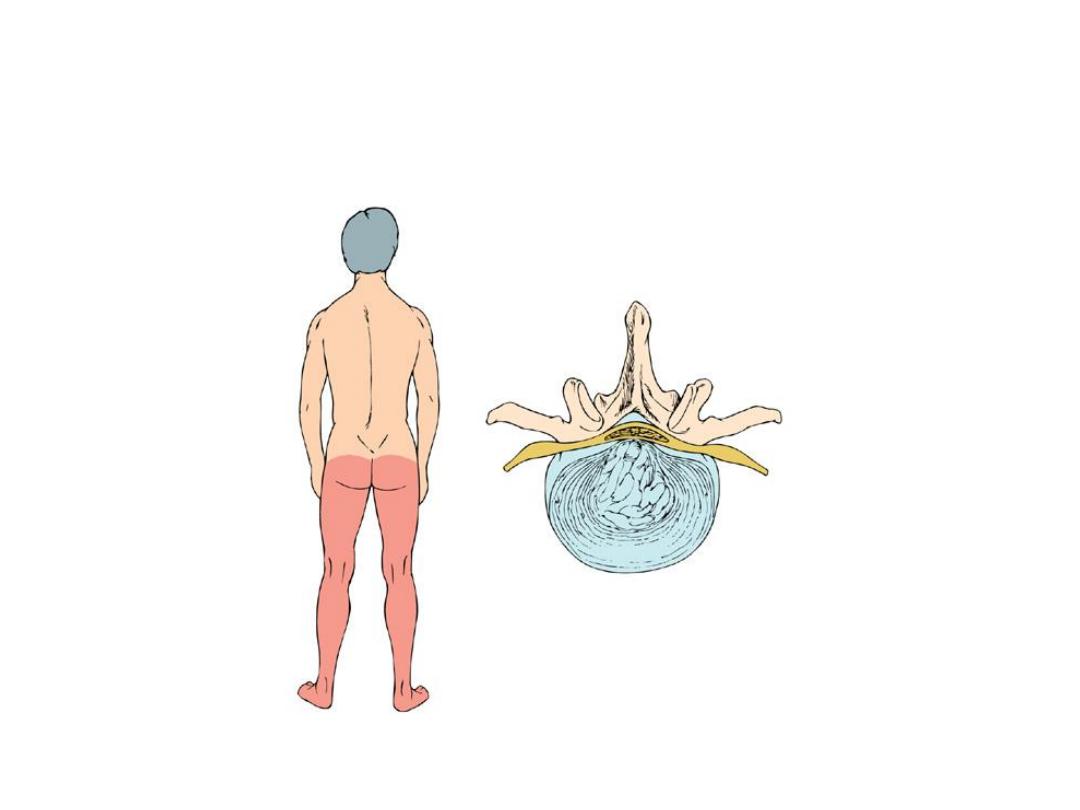
Causes of low back pain 2
• Radicular low back pain
– Herniated intervertebral disc commonest cause
but can be foraminal stenosis sec. OA / tumours /
infection (rare)
– TOP TIP not all pain referred down leg is sciatica
(facet joint disease / hip / SIJ / piriformis
syndrome etc.)

Structures that cause nerve root compression
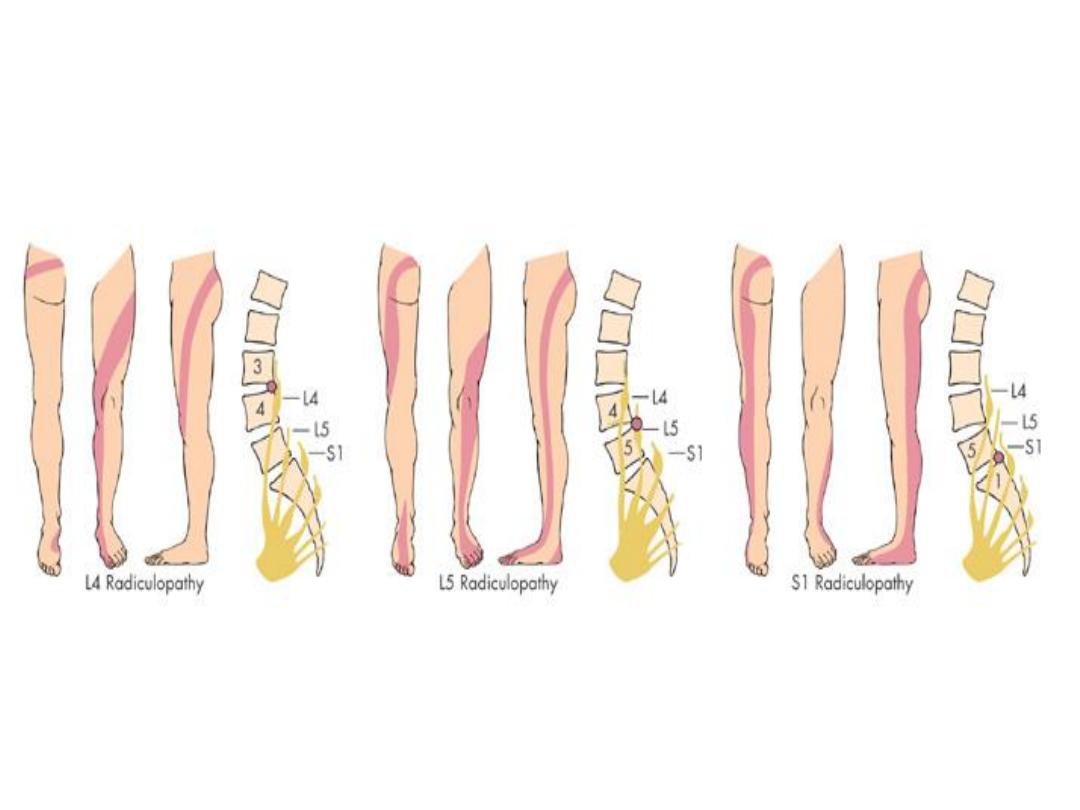
L4/L5/S1 Radiculopathy
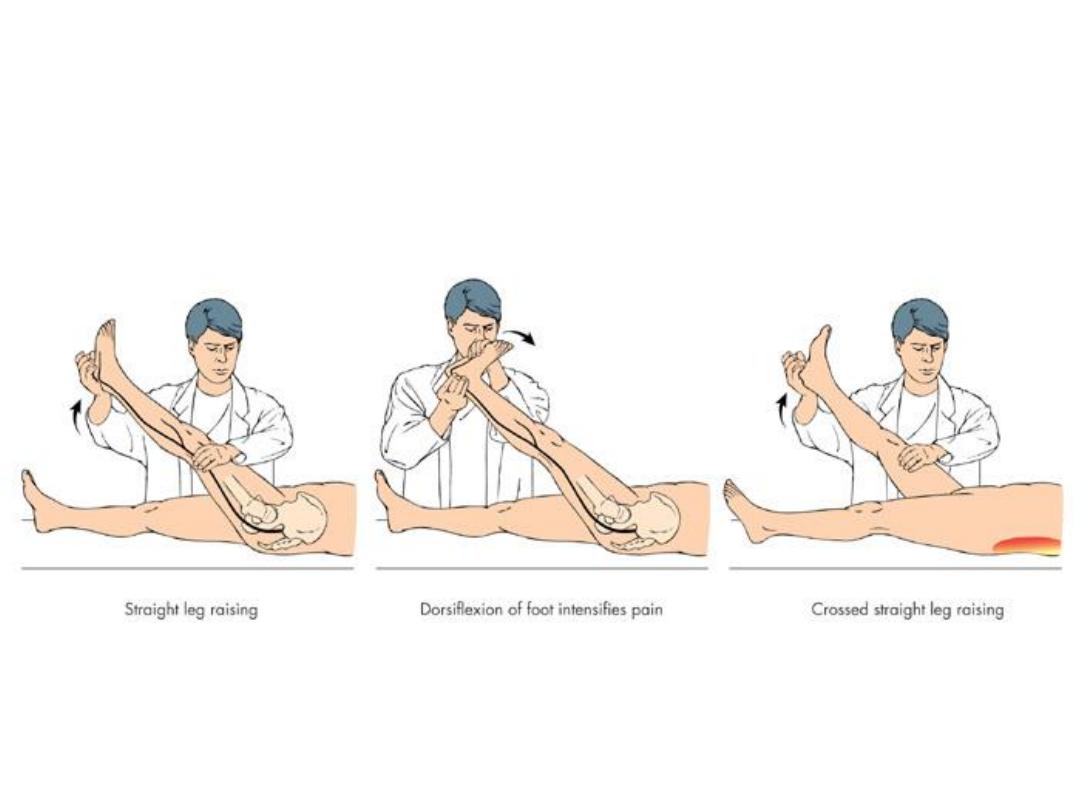
Straight Leg Raising
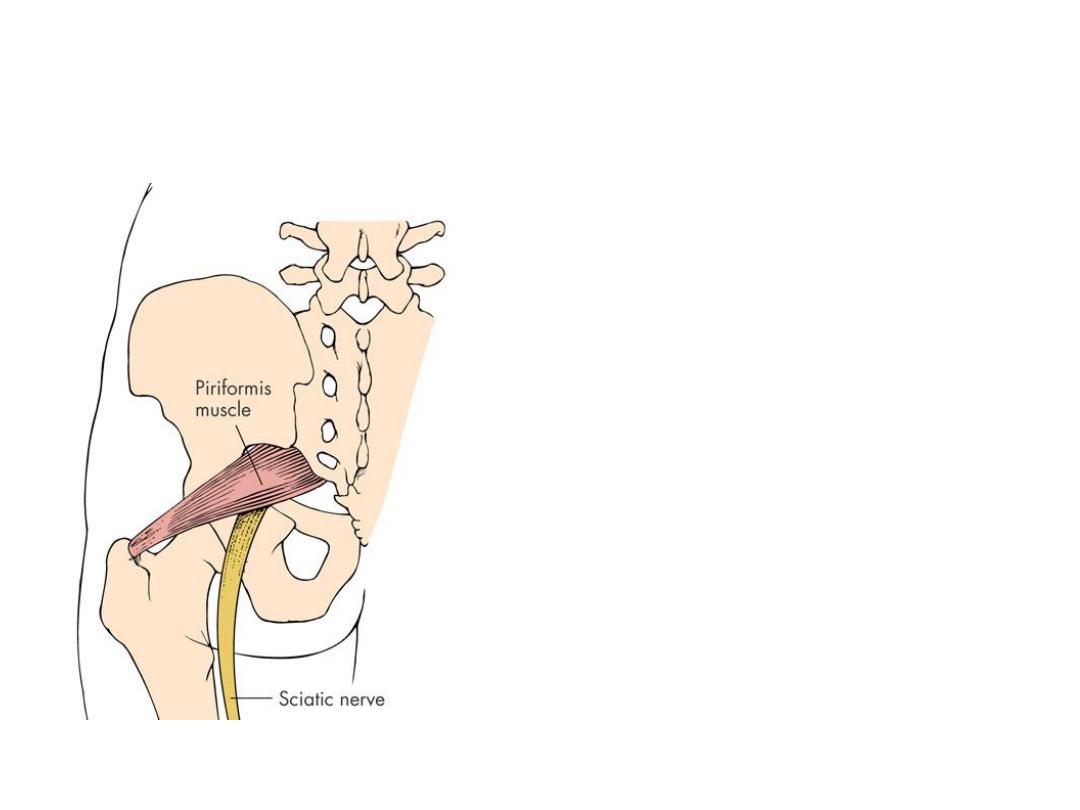
Piriformis syndrome
Pain from piriformis
muscle
– irritation of
sciatic nerve passing
deep or through it
Pain on resisted abduction /
external rotation of leg

Causes of low back pain 3
• Lumbar Spinal Stenosis
– Subtle presentation.
– Bilateral radicular signs should alert to possibility.
– Pain on walking- worse on flat –(eases if hunched
over – shopping trolley sign!)
– Can be mistaken for Claudication.
– Admit if progressive / or else CT scan.
Cauda Equina syndrome
(spinal canal compression)
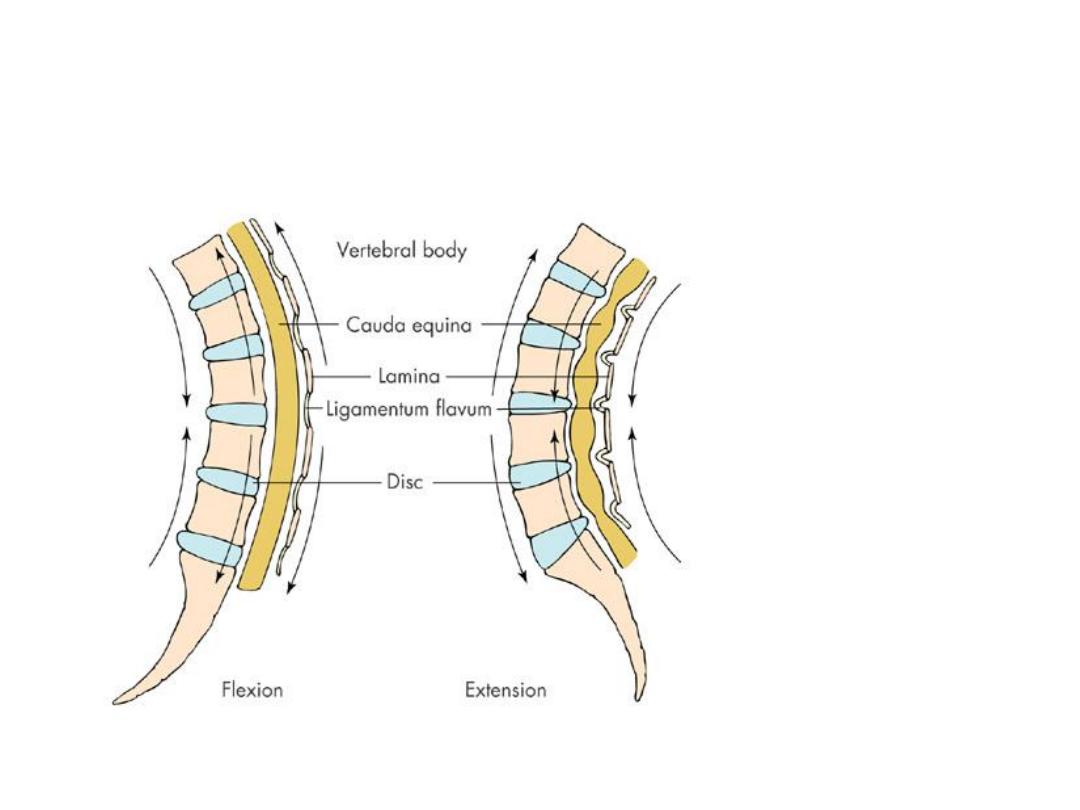
Spinal Stenosis

When should clinicians consider imaging?
• If history or physical suggests specific underlying cause
– Neurologic deficits are severe or progressive
– Serious underlying conditions are suspected
• If patients are candidates for surgery Persistent low
back pain
– Signs or symptoms of radiculopathy or spinal stenosis
– Use MRI (preferred
)
or CT

• Radiographic examinations are usually of limited use in patients
with low back pain unless the history or physical examination
suggests a specific underlying cause. Radiographic findings
correlate poorly with low back symptoms. Spinal imaging studies in
asymptomatic individuals commonly reveal anatomical findings,
such as bulging or herniated disks, spinal stenosis, annular tears,
and disk degeneration, which may not be clinically relevant and can
reduce the specificity of imaging tests. Thus, the demonstration of
an anatomical abnormality should not automatically lead the
clinician to assume that it is the cause of the pain. Routine imaging
also increases costs and is associated with a greater likelihood of
invasive procedures, such as surgery, without improved patient
outcomes (17).

• A
guideline developed by the American College of Physicians and the American
Pain Society in 2007 recommends that clinicians not routinely obtain imaging or
other diagnostic tests in patients with nonspecific low back pain, that they
perform diagnostic imaging and testing in patients with low back pain when
severe or progressive neurologic deficits are present or when serious underlying
conditions are suspected, and that they evaluate patients with persistent low
back pain and signs or symptoms of radiculopathy or spinal stenosis with
magnetic resonance imaging (preferred) or computed tomography only if the
patients are potential candidates for surgery or epidural steroid injection (for
suspected radiculopathy). The guideline developers rated these
recommendations as strong and based on moderate-quality evidence (18). The
American College of Physicians subsequently published best-practice advice for
high-value, cost-conscious low back imaging, including indications for imaging
and use of magnetic resonance imaging, based on the presence and type of risk
factors found (Table 2) (17). The American College of Radiology has also
developed appropriateness criteria for radiographic procedures in the
evaluation of patients with low back pain (19).

• These criteria are meant to guide clinician decision making in the
context of each patient’s clinical circumstances.
• In summary, imaging is more useful as the pretest probability of
underlying serious disease requiring surgical or other intervention
increases. A negative plain film does not definitively exclude
cancer or infection in someone at high risk for these conditions.
For such persons, additional advanced imaging may be
appropriate.
• A systematic review of 6 RCTs found no difference between
immediate lumbar imaging and usual care without immediate
imaging for pain or function at short-term (up to 3 months) or
long-term (6–12 months) follow-up (20).
© Copyright Annals of Internal Medicine, 2014
Ann Int Med. 160 (6): ITC6-1.
Under what circumstances should
clinicians consider electromyography and
other laboratory tests?
Possible cancer but negative lumbar radiography
Check erythrocyte sedimentation rate: high elevation
associated with presence of cancer
Uncertainty about relationship of leg symptoms to
anatomical findings on advanced imaging
Assess with electromyography and nerve conduction tests
Possible myelopathy, radiculopathy, neuropathy, myopathy
Assess with electrophysiologic tests
Don’t test patients with duration of symptoms < 4 weeks
Radiculopathy or neuropathy: results might be unreliable in
limb muscles until > 3 to 4 wks limb symptoms
© Copyright Annals of Internal Medicine, 2014
Ann Int Med. 160 (6): ITC6-1.
Additional diagnostic and laboratory tests are not indicated in most
patients with low back pain. A highly elevated erythrocyte
sedimentation rate is associated with the presence of cancer and
might be considered in patients suspected of having cancer with
negative lumbar radiography (21). Clinicians may consider
electromyography and nerve conduction tests for patients in whom
there is diagnostic uncertainty about the relationship of leg
symptoms to anatomical findings on advanced imaging, although
evidence to define appropriate strategies for using such tests is not
available. Electrophysiologic tests can assess suspected
myelopathy, radiculopathy, neuropathy, and myopathy. With
radiculopathy or neuropathy, electromyography results might be
unreliable in limb muscles until a patient has significant limb
symptoms for more than 3
–4 weeks, so testing should not be done
in patients with a duration of symptoms less than 4 weeks.

Causes of low back pain 4
• Inflammatory – Ankylosing Spondylitis
– Difficult to diagnose if early stages but:
• Morning stiffness for > 30 minutes
• Pain that alternates from side to side of lumbar
spine
• Sternocostal pain
• Reduced chest expansion
– Schobers test
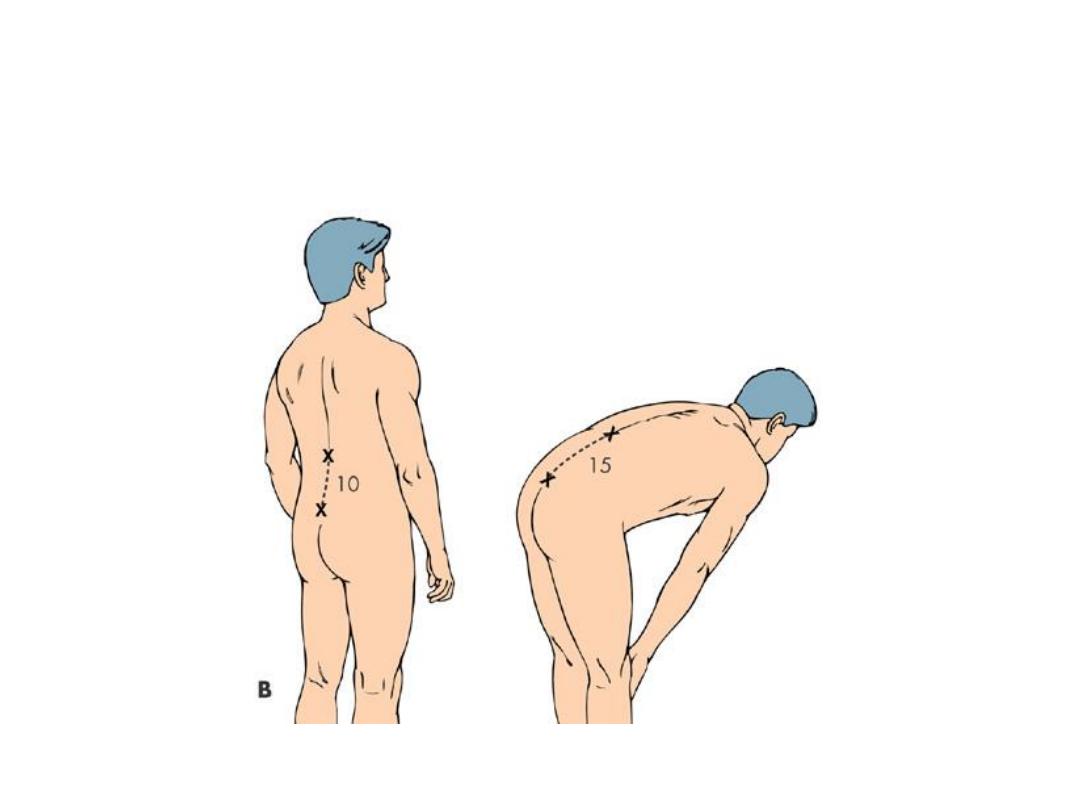
Schobers Test
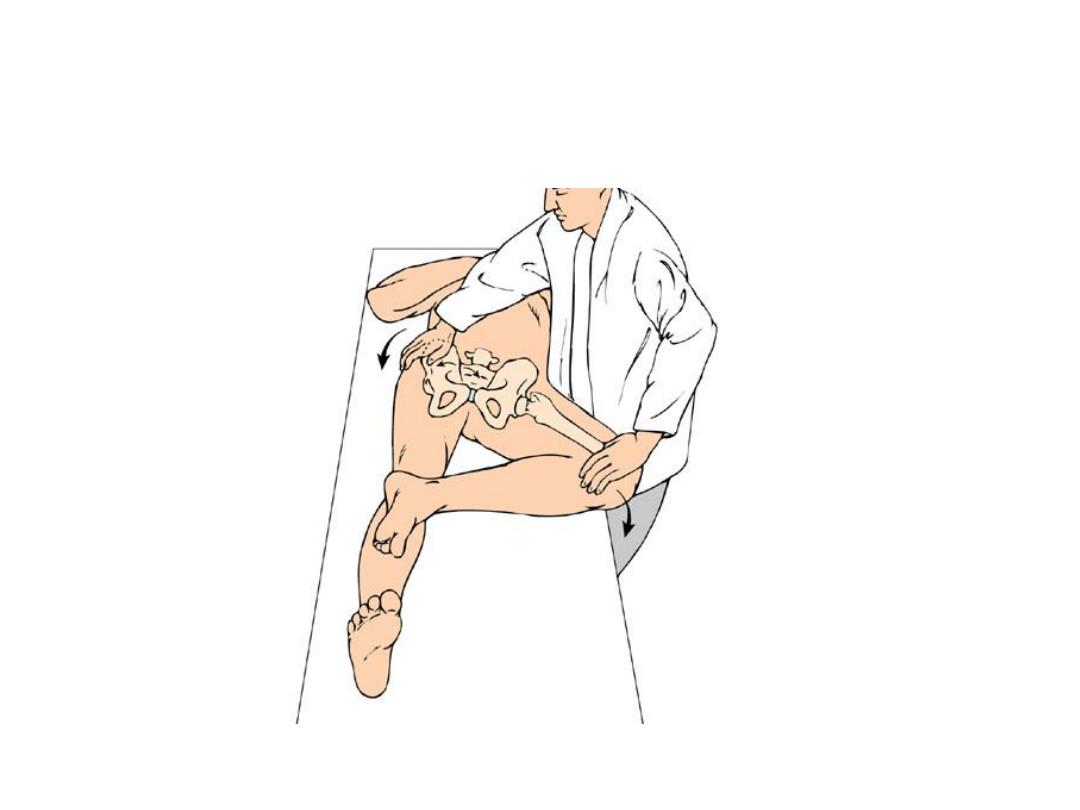
Fabere test
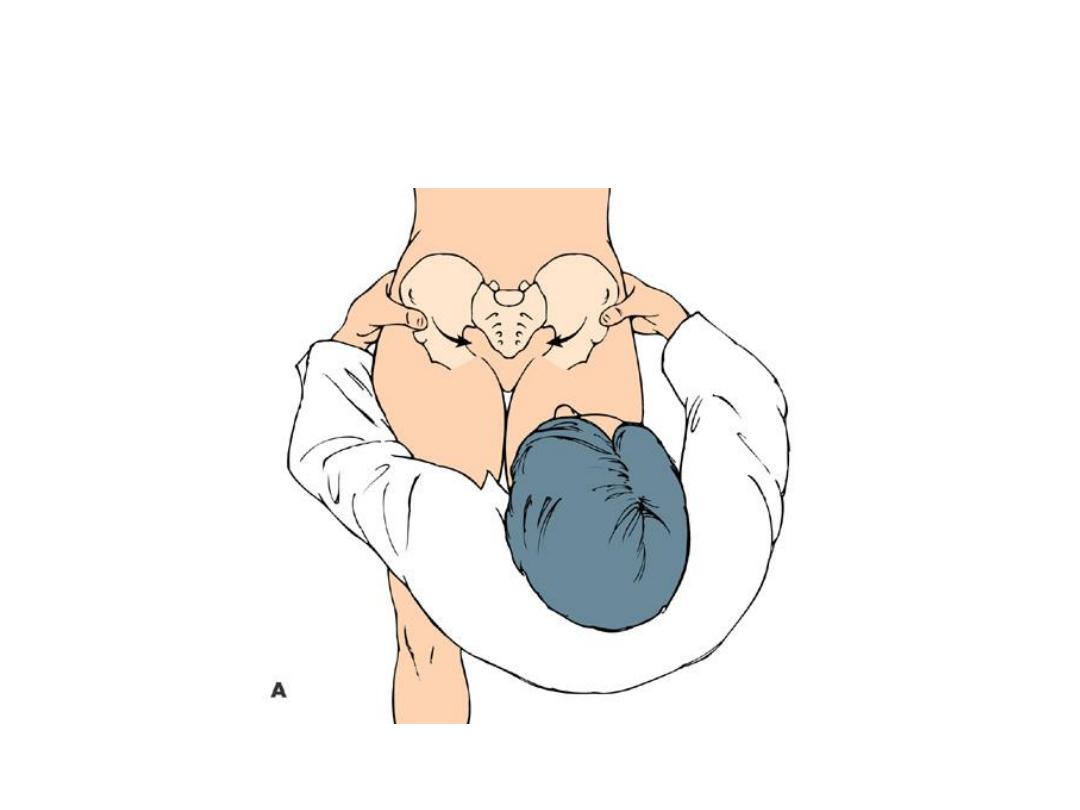
Pelvic Compression Test

Red Flags
• Weight loss, fever, night sweats
• History of malignancy
• Acute onset in the elderly
• Neurological disturbance Bilateral or alternating
symptoms
• Sphincter disturbance
• Immunosuppression
• Infection (current/recent)
• Claudication or signs of peripheral ischaemia
• Nocturnal pain

Yellow flags 1

Yellow Flags 2
Factors prolonging back pain
• Internal factors-Opioid dependency
• “External controller” patient-type; learned
helplessness; factitious disorder
• Mental health- depression or anxiety
• Interpersonal factors "Sick role“
• Stressors in relationships
• Environmental / societal factors- Disability payments /
Litigation / Malingering

Causes of back pain
• Structural
• Mechanical
Facet joint arthritis
Proplapsed
intervertebral disc
Spondylolysis / Spinal
stenosis
• Inflammatory
• SacroiliitisSpondyloarth
ropathies
• Infection
• Metabolic
• Osteoporotic vertebral
collapse
Paget's disease
Osteomalacia
• Neoplasm
Ca Prostate
Ca Breast
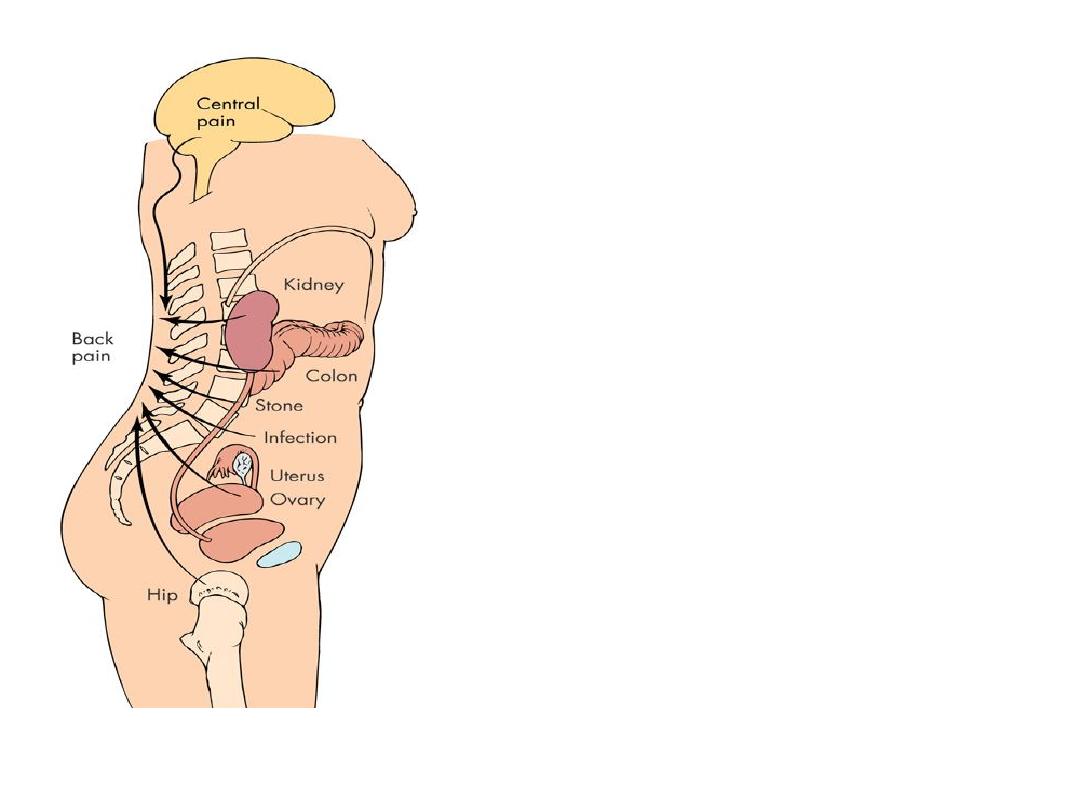
Referred pain
•Pleuritic pain
•Upper UTI / renal calculus
•Abdominal aortic aneurysm
•Uterine pathology (fibroids)
•Irritable bowel (SI pain)
•Hip pathology

Imaging modalities
• Xrays good first line Ix if red flags,
osteoporotic fracture
• Bone scan (also good initial Ix if Xray nad and
red flags) - mets, infection, pagets, PMR
• CT Scan bone tumours fractures and spinal
stenosis
• MRI spinal cord, nerve roots, discs,
haemorrhage
• Dexa Scan Bone density

TREATMENTS Simple Back Pain
(over 95% of cases)
Aim: to relieve symptoms and mobilise early.
Avoid Bed rest
Paracetamol (+nsaid if insufficient)
Avoid opiates if at all possible
No evidence that co-analgesics better than paracetamol alone.
Muscle relaxants (diazepam / methocarbamol) small additional
benefit.

No evidence for:
• Short wave diathermy
• TENS
• Spinal manipulation
• Traction
• Acupuncture
• Exercises
• Spinal cortisone injections
Occupational issues

Occupational issues
• More sick leave : Less chance of recovery
• 4-12 w - 40% chance of still being off at 1 year.
• Don’t need to be pain free to return to work
• MDT Rehabilitation programs: psychological
therapies; CBT; graduated return to work (light
duties)

Blocks to returning to work (blue flags!)
• perceived work load
• low pay
• management attitudes
• poor support
• loss of confidence
• depression

JD’s top tips for back pain.
• Patient who attends a second time with “simple”
back pain- get them to strip to their underwear!

Top tips
• True sciatica means that the leg pain is worse than
the back pain- start examination with them sitting
on the couch.

Top tips
• With radiculopathy re-examine regularly, carefully
note findings and refer early if weakness (foot drop
can be irreversible)

Top Tips
• Physios are very good at managing the
psychological aspects of chronic pain.

Top Tips
• Sending someone to casualty is pointless but can
have a very useful ‘placebo’ effect in showing the
patient how impressed you are with his or her pain.