Schizophrenia
Schizophrenia is a clinical syndrome of variable but profoundly disruptive psychopathology,
which involves thought, perception, emotion, movement, and behavior. The expression of
these symptoms varies across patients and over time, but the cumulative effect of the illness
is always severe and usually long lasting.
Emil Kraepelin: two major patterns of insanity: manic-depressive psychosis and dementia
praecox (or dementia of the young), and under the diagnostic category of dementia precox
the previously categories of insanity, such as hebephrenia, paranoia, and catatonia. In
differentiating dementia precox from manic-depressive disorder, Kraepelin emphasized what
he believed to be the characteristic poor long-term prognosis of dementia precox, as
compared to the relatively non deteriorating course of manic-depressive illness.
In 1911 Eugen Bleuler, recognizing that dementia was not a usual characteristic of dementia
precox, suggested the term schizophrenia (splitting of the mind) for the disorder. Bleuler
introduced the concept of primary and secondary schizophrenic symptoms; his four primary
symptoms (the four As) were:
1. Association loosening in the logical thoughts.
2. Affective blunting or incongruity.
3. Ambivalence: the co- existence of strongly conflicting feelings, attitudes and ideas leading
to inconsistent behavior.
4. Autism (withdrawal in thinking and behavior).
Schneider (1957) has defined diagnostic criteria for schizophrenia on the basis of clustering
and frequency of symptoms .He designated a group of the most common (so-called first
rank) symptoms which in the absence of organic mental diseases signify schizophrenia,
these include:
1- Auditory hallucinations taking the form of one of the following:
o
Thought Echo: Voices repeating the subject's thoughts out loud or anticipating
their thoughts.
o
Third person Hallucination: Two or more hallucinatory voices discussing the
subject or arguing about them in the third person.
o
Voices commenting on the subject's thoughts or behavior, often in the form of a
running commentary.
2- Thought Alienation:
A- Thought insertion: The sensation of alien thoughts being put into the subject's
mind by some external agency.
B- Thought withdrawal: of their own thoughts being taken away.
C- Thought broadcasting: the sensation that the subject's thinking is no longer
confined to their own mind, but is instead shared by, or accessible to, others.
3- Passivity Phenomena :The sensation of feelings, impulses, or acts being experienced
or carried out under external control, so that the subject feels as if they were being
hypnotized or had become a robot (passivity of affect, impulse, or volition)
4- Delusional perception (delusional misinterpretation of a normal perception). Refers to
the experience of interpreting a normal perception with a delusional meaning.
Limitations of Schneider’s approach:
1. These symptoms carry no prognostic value.
2. Their sensitivity is limited (around 20 % of schizophrenic patients never showed these
symptoms).
3. Their specificity is also limited (around 30 % of patients with these symptoms have mood
disorders; mania or depression).
EPIDEMIOLOGY
Schizophrenia is a leading public health problem that exacts enormous personal and
economic costs worldwide. Schizophrenia affects just under 1 percent of the world's
population (approximately 0.85 percent).
Worldwide, 2 million new cases appear each year. The lifetime risk of developing
schizophrenia is about 1%.
- Most common between 15 - 35 years. Paranoid type is later onset than other types.
There is no sex difference. Although males tend to have an earlier onset than females (23y
vs. 26y) and develop more severe illnesses.
More common in low social class this is generally attributed to the "social drift"
phenomenon.
Mortality; Suicide is the most common cause of premature death in schizophrenia (40 %).
The life time prevalence is about 5 %. Risk is probably highest in the year after first
presentation
ETIOLOGY
The etiological process or processes by which a causal agent creates the pathophysiology of
schizophrenia is not yet known.
All the evidence suggests multi factorial etiology for schizophrenia.
1. Genetic:Family, twin, and adoptive studies documented contribution of genetic factors to
the etiology of schizophrenia; however, it is not yet known which genes are involved.
- Incidence in families is higher than in general population.
- Monozygotic twin concordance rate is greater than dizygotic concordance rate (50 %, 15 %
respectively)
5 % Parents
10 % Siblings
14 % Child of one schizophrenic parent
46 % Child of two schizophrenic parents
2. Neurobiological
There are many Biochemical Theories identifies the relation between neurotransmitter and
schizophrenia.
A-Dopamine and Schizophrenia The hyperdopaminergic hypothesis of schizophrenia arose
from two sets of observations of drug action relating to the dopaminergic system. Drugs that
increase dopamine system activity, such as d-amphetamine, cocaine, levodopa (Larodopa),
and methylphenidate (Ritalin), can induce a paranoid psychosis that is similar to some
aspects of schizophrenia. In contrast, drugs that share the capacity to block postsynaptic
dopamine receptors reduce the symptoms of schizophrenia.
Increase in the dopamine or increase in the number or the sensitivity of the dopaminergic
receptors lead to schizophrenia.
B-Serotonin hypothesis: abnormal serotonin metabolism in some patients. Evidence
includes:
1. Hallucinogens like LSD (serotonin agonist) induce psychosis.
2. Serotonin antagonist, such as clozapine and Risperidone improves psychosis.
C. Glutamate is implicated in schizophrenia; N-methyl-d-aspartate (NMDA) antagonists
(e.g., memantine) are useful in treating some of the neurodegenerative symptoms in patients
with schizophrenia.
D. Disturbed balance between dopamine and serotonin as supported by the new generation
of antipsychotics (dopamine-serotonin antagonists).
3- Psychosocial and Environmental:
A. Life Events: Life stressors, particularly in the three months before onset, can induce
schizophrenia in those who are vulnerable.
B. Family Psychodynamic. Precipitation of schizophrenia can be due to:
1. Schizophrenogenic mother: over protective
2. Marital skew (submissive father and dominant mother)
3. Marital schism (contradicting parental messages).
4. Double – bind communication (a parent conveys two conflicting incompatible messages at
the time, one is overt and the other is covert).
C. High Expressed Emotions (EE) of the family which include critical comments and
emotional over-involvement.
Patients whose families have high expressed emotions have higher relapse rate than those
whose families have low expressed emotions.
Other markers of early influences, including gestational and birth complications, exposure to
influenza epidemics, Rhesus (Rh) incompatibility, starvation, and winter births ,Marital
Status(unmarried), Immigration ,Urbanization and Industrialization: The prevalence of
schizophrenia has been reported to be higher in urban environments than in rural areas., Life
Stressors ,Infections ,Finally, substance abuse has been identified as a risk factor for
developing schizophrenia.
Neuropathology and Neuroimaging :
- Cortical atrophy in 10 - 35 % - Enlargement of the lateral and third
ventricles in 10 - 50 %.
- Findings correlate more with negative features and with cognitive impairments.
- Abnormal frontal, parietal and temporal
lobe structure and metabolism.
Clinical features:
Prodromal signs: Quite, passive or irritable, few friends avoid social activity, day dreams,
somatic complaints, interest in the occult, religion or philosophy.
Positive symptoms: All types of hallucinations, delusions, bizarre behavior (Clothing,
appearance, Social, sexual behavior, Aggressive behavior, Repetitive/stereotyped behavior)
and Positive formal thought disorder (Derailment, Tangentiality, Incoherence, Illogicality,
Circumstantiality, Pressure of speech, Distractible speech, Clanging.
Negative symptoms: Loss of the normal level of motivation or drive, loss of awareness of
socially appropriate behavior, flattening of mood, and difficulty in abstract thinking.
*Affective flattening: Unchanging facial expression, Decreased spontaneous movements,
Poor eye contact, Affective non responsivity, inappropriate affect.
*Alogia: Poverty of speech, Poverty of content of speech.
*Avolition-apathy: Grooming and hygiene, Impersistence at work or school, Physical
anergia.
*Anhedonia-asociality: limitation in Recreational interests, activities, Sexual interest,
activity, Relationship with friends, peers.
*Attention: Social inattentiveness.
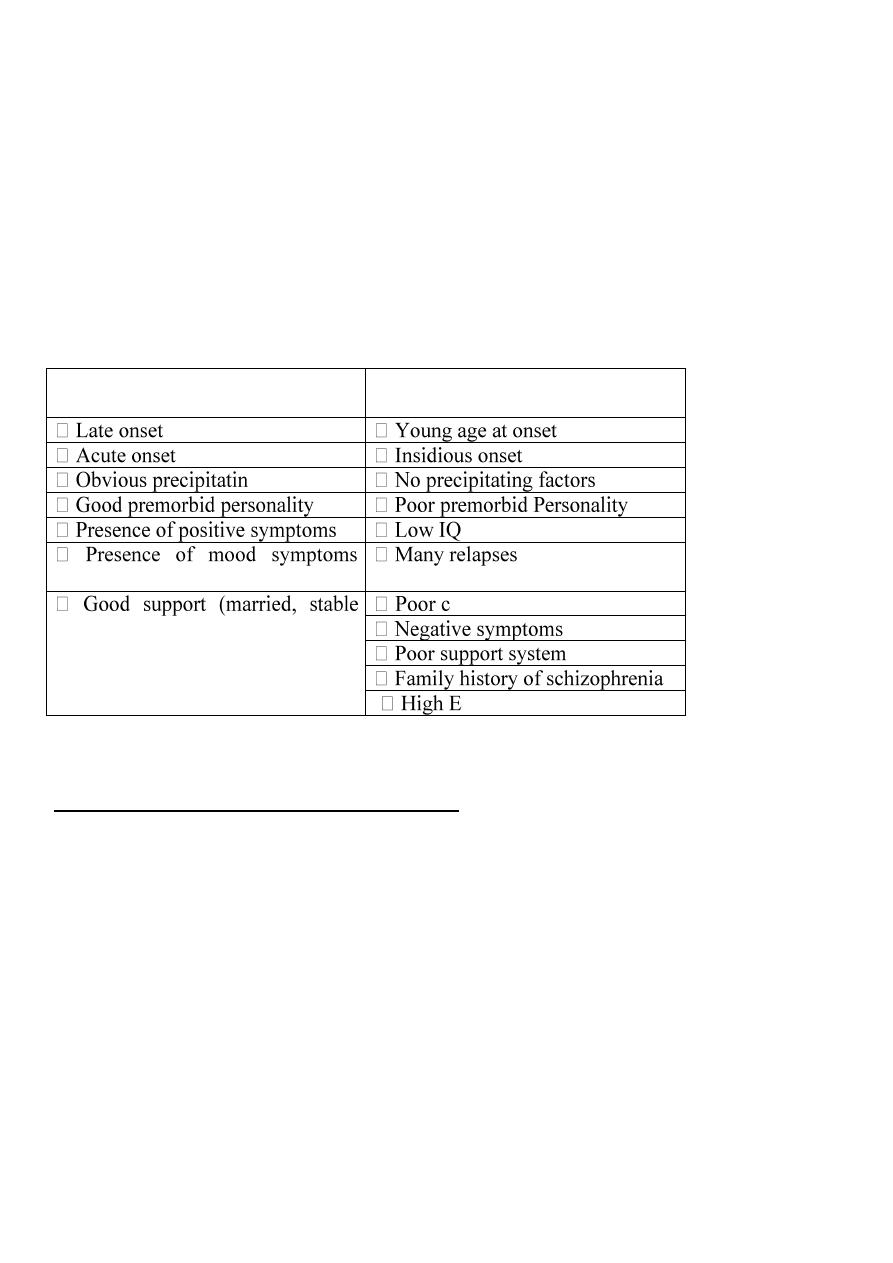
Good Prognostic Factors
Bad Prognostic Factors
g factors
(especially depression)
family)
ompliance
xpressed Emotion family
Diagnosis
DSM-V Diagnostic Criteria for Schizophrenia
A. Two (or more) of the following, each present for a significant portion of time during
a 1-month period (or less if successfully treated). At least one of these must be (1),
(2), or (3):
1. Delusions.
2. Hallucinations.
3. Disorganized speech (e.g., frequent derailment or incoherence).
4. Grossly disorganized or catatonic behavior.
5. Negative symptoms (i.e., diminished emotional expression or a volition).
B. For a significant portion of the time since the onset of the disturbance, level of
functioning in one or more major areas, such as work, interpersonal relations, or self-care,
is markedly below the level achieved prior to the onset (or when the onset is
in childhood or adolescence, there is failure to achieve expected level of interpersonal,
academic, or occupational functioning).
C. Continuous signs of the disturbance persist for at least 6 months. This 6-month period
must include at least 1 month of symptoms (or less if successfully treated) that
meet Criterion A (i.e., active-phase symptoms) and may include periods of prodromal
or residual symptoms. During these prodromal or residual periods, the signs
of the disturbance may be manifested by only negative symptoms or by two or
more symptoms listed in Criterion A present in an attenuated form (e.g., odd beliefs,
unusual perceptual experiences).
D. Schizoaffective disorder and depressive or bipolar disorder with psychotic features
have been ruled out because either 1) no major depressive or manic episodes
have occurred concurrently with the active-phase symptoms, or 2) if mood episodes
have occurred during active-phase symptoms, they have been present for
a minority of the total duration of the active and residual periods of the illness.
E. The disturbance is not attributable to the physiological effects of a substance (e.g.,
a drug of abuse, a medication) or another medical condition.
F. If there is a history of autism spectrum disorder or a communication disorder of
childhood onset, the additional diagnosis of schizophrenia is made only if prominent
delusions or hallucinations, in addition to the other required symptoms of
schizophrenia, are also present for at least 1 month (or less if successfully
treated).
The same criterions are used in the diagnosis of Brief psychotic disorder but negative
symptom is not included in criterion A and the duration is less than one month.
And used also in the diagnosis of schizophreniform disorder but the duration of symptom
is more than one month an less than six months.
===========================================================================
ICD-10 schizophrenia
1. At least one of the following:
Thought echo, insertion, withdrawal, or broadcasting.
Delusions of control, influence, or passivity; clearly referred to body or limb
movements or specific thoughts, actions, or sensations; and delusional perception.
Hallucinatory voices giving a running commentary on the patient's behavior or
discussing him/her between themselves, or other types of hallucinatory voices coming
from some part of the body.
Persistent delusions of other kinds that are culturally inappropriate or implausible,
(e.g. religious/political identity, superhuman powers and ability).
2. Or, at least two of the following:
Persistent hallucinations in any modality, when accompanied by fleeting or half-
formed delusions without clear affective content, persistent over-valued ideas, or
occurring every day for weeks or months on end.
Breaks of interpolations in the train of thought, resulting in incoherence or irrelevant
speech or neologisms.
Catatonic behavior such as excitement, posturing, or waxy flexibility, negativism,
mutism, and stupor.
Negative symptoms such as marked apathy, paucity of speech, and blunting or
incongruity of emotional responses.
A significant and consistent change in the overall quality of some aspects of personal
behavior, manifest as loss of interest, aimlessness, idleness, a self-absorbed attitude,
and social withdrawal.

3. Duration of 1 month.
Schizophrenia Subtypes
1-Paranoid Type:
A. Prominent paranoid delusion with frequent auditory hallucinations related to the
delusion.
B. Patient is usually potentially aggressive, angry or fearful, uncooperative and difficult
to deal with. No prominent disorganized behavior or mood.
C. The onset is usually late (compared to other subtypes of schizophrenia).
D. The prognosis is better than the other subtypes and deterioration in functioning is
usually much less.
2-Disorganized Type (Hebephrenic)
A. Disorganized behavior.
B. Marked incoherence and loosening of association.
C. Inappropriate affect.
D. Grimacing and bizarre mannerism are common.
3-Catatonic Type
A. Motoric immobility as evidenced by catalepsy (including waxy flexibility) or stupor
B. Excessive motor activity (that is apparently purposeless and not influenced by external
stimuli)
C. Extreme negativism (an apparently motiveless resistance to all instructions or
maintenance of a rigid posture against attempts to be moved) or Mutism
D. Peculiarities of voluntary movement as evidenced by posturing (voluntary assumption
of inappropriate or bizarre postures), stereotyped movements, prominent mannerisms,
or prominent grimacing
E. Echolalia or Echopraxia
4-Undifferentiated Type
A. The criteria are not met for the paranoid, disorganized, or catatonic type.
B. Prominent delusions and hallucinations.
C. Prominent disorganization behavior.
D. Incoherence.
5-Residual Type
A. Absence of prominent delusions, hallucinations, disorganized speech, and grossly
disorganized or catatonic behavior.
B. There is continuing evidence of the disturbance, as indicated by the presence of
negative symptoms or two or more symptoms listed in criterion A for schizophrenia,
present in an attenuated form (e.g., odd beliefs, unusual perceptual experiences).
MANAGEMENT: Multidisciplinary: Bio, Psycho, Social approach.
Hospitalization is usually indicated in the acute phase in order to:
A. Clarify diagnosis (rule out possible organic causes).
B. Control the disturbed behavior.
C. Protect the patient and / or others (risk of dangerousness or suicide)
D. Give electroconvulsive therapy (ECT) for Catatonic type, those with concomitant
depression and in resistant cases.
E. Antipsychotic medications
Psychosocial:
a. Family therapy education and explanation can significantly reduce relapse rate and
high EE family interaction can be diminished. Compliance may also be enhanced.
b. Rehabilitation :
-care).
-management skills (e.g. when to take medication).
Token economy: Useful for institutionalized chronic schizophrenics.
Positive and negative reinforcement are used to alter patient’s unacceptable behavior. It
should be part of a behavioral program.
Treatment
Antipsychotics:
Mechanism of action: Postsynaptic blockade of CNS dopamine receptors type 2 (D2) and
will act through three tracts:
Mesolimbic – Mesocortical tract Therapeutic antipsychotic effect.
Nigrostriatal tract- Extrapyramidal effects lead to Parkinson like features (side effect).
Tuberoinfundibular tract Excessive prolactin secretion.
Antipsychotics (Major Tranquilizers – Neuroleptics)
Phenothiazine:
- Aliphatic class e.g. Chlorpromazine (Largactil) (Low potency): Oral, IM, dose200–
600mg/day
-Piperidine class e.g. Thioridazine (Melleril).Low potency: Oral 200–600mg/day
Serious Side effects like retinitis pegmantosa and arrhythmia
-Piperazine class e.g. Trifluoperazine (Stelazine).High potency: Oral 5–30 up to60mg/day.
– Haloperidol (Serenace) high potency: Oral, IM, depot (5–
20mg, up to60mg/day oral).
(Clopixol)
– Sulpride (Dogmatil)
ylbutylpiperidine: Pimozide (Orap)
(Clozaril - Leponex)
(Risperdal)
DEPOT (SLOW RELEASE) ANTIPSYCHOTICS: These are esters of antipsychotic
drugs, usually in an oily medium, given as deep intramuscular injections to patients who
improve with drugs but cannot be relied on to take them regularly by mouth (i.e. poor
compliance
– Modecate): e.g. 25 – 100 mg / month.
– Fluanxol): e.g. 20 – 100 mg / month.
– 400 mg. / month.
– 600 mg. /month
-
- ½ the dose) to check patient’s tolerability.
Patients frequently experience the adverse effects of an antipsychotic agent before they
experience clinical improvement. Whereas a clinical response may be delayed for days or
weeks after drugs are started, adverse effects often begin almost immediately. For low-
potency drugs, these adverse effects are likely to include sedation, postural hypotension, and
anticholinergic effects, whereas high-potency drugs are likely to cause extrapyramidal side
effects.
The therapeutic effect of antipsychotics may take up to 6 weeks to appear.
A-High potency drugs:
B. Low potency drugs:
inent.
E.g. chlorpromazine, thioridazine.
Adverse Effects:
(1.) Extra-Pyramidal Side Effects (EPSE)
Acute dystonia:
icollis), ocular muscles (oculogric crisis)
muscles of the back (opisthotonus) and tongue protrusion.
– 10 mg IM or P.O.).
Parkinsonism:
stooped posture
Treated with anticholonergic drugs (e.g. procyclidine)
Akathisia (inability to keep still, associated with unpleasant feelings of inner tension)
Usually appears within days – weeks.
-blockers may help in the treatment, whereas anticholinergic have
no therapeutic effect.
Tardive Dyskinesia
– 20 % of patients on long-term antipsychotics, Chronic treatment with
an antipsychotic—usually for 6 months or more can result in neuroleptic-induced tardive
Dyskinesia
Chewing, sucking or choreo-athetoid movements of the facial and neck muscles
receptors resulting from prolonged dopamine
blockade
No specific treatment, the only agreed treatment is to discontinue the antipsychotic drug
when the patient’s state allows this.
-Treated by changing to atypical antipsychotic especially clozapine.
(2.) Antidrenergic:

(3.) Anticholonergic:
– angle glaucoma.
(4.) Others:
weight gain, galactorrhoea , amenorrhoea
Toxic Effect : Neuroleptic Malignant Syndrome ( NMS); Muscle rigidity , Fever , High CPK
B-Atypical or the new generation Anti psychotic: acting on positive symptom and more
potent in treating negative symptom than the traditional drugs, no or lower incidence of extra
pyramidal symptom and tardive dyskinesia, more effective in treating resistant schizophrenia
(about50% of resistant cases)
Olanzapine Oral 7.5–up to20 mg/day
Quetiapine Oral 150–750mg/day
Risperidone Oral 2–16 mg/day
Clozapine Oral 150–900
mg/day
Side effect; increase appetite, body weight .sedation.
Olanzapine and Risperidone might be related to development of Diabetes mellitus &
increase blood sugar in diabetic patient.
Clozapine was the first atypical antipsychotic drug. It is indicated for psychosis not
responding to traditional antipsychotics .
1. Neutropenia and agranulocytosis. Therefore, regular
blood test are required.
2. Seizure – dose dependent.
3. Sedation, weight gain, sialorrhoea, hypotension, constipation and tachycardia.
The patients should receive maintenance treatment for one year to decrease the chance of
relapse.
ELECTROCONVULSIVE THERAPY ( ECT )
History and Concept:
Patients with concomitant schizophrenia and epilepsy were found to improve in psychosis,
following repeated fits. It was therefore, thought that there is an antagonism between
schizophrenia and epilepsy.
In 1938 Cerletti administered an electrically – induced fit to a catatonic patient who then
showed reasonable improvement.
Later, anesthesia was introduced and convulsions were modified using muscle relaxing
agents.
Indications for ECT
1. Depression:
- depressive disorder with suicidal risk.
- depressive stupor or marked retardation.
- depressive disorder with delusions
- inability to take drugs :
- first trimester of pregnancy.
- in the elderly.
- in physical diseases e.g. renal failure.
2. Schizophrenia (catatonic, resistant to drugs…).
3. Post partum psychosis.
4. Schizoaffective disorder.
5. Mania and mixed affective states.
Precautions and Contraindications:
Recent research showed no absolute contraindications to ECT.
At one time raised intracranial pressure was considered as the only absolute
Contraindication to ECT. Remember that not all space occupying lesions produce raised
intracranial pressure.
Relative Contraindications:
references extend it to 2 years).
Psychiatric disorders that may show deterioration or no response
to ECT:
Mode of Action of ECT:
action is unknown.
the cerebral seizures (not
on the motor component) is thought to result from neurotransmitter changes probably
involving serotonin and noradrenaline transmission.
ECT Preparations:
and ECT consent by the patient or his
caretaker if the patient is minor or his judgment is impaired.
anaesthesia and ECT).
midnight).
-induced apnea, to facilitate seizure activity and
to reduce memory impairment.
muscle contraction may
lead to bone fracture).
mouth gag in patient’s mouth to prevent tongue or lip bites.
ECT Procedure:
Bilateral (most commonly used procedure)
d (frontotemporal position).
Unilateral:
– dominant side.
than bilateral.
– 3 times a week with a total of 6 – 12 sessions, according to
response and progress. Response begins usually after 2 – 4 sessions. If there is no response
after 8 sessions, it is unlikely that more sessions will produce a useful change.
In depressed patients antidepressants should be started towards the end of the course of ECT
to reduce the risk of relapse.
Side Effects of ECT: (ECT in general is a safe procedure)
amnesia).
– several months).
a during seizure.
Misconceptions about ECT
– 220 V) current.
-Electro convulsive therapy (ECT): Studies in patients with recent-onset schizophrenia
indicate that ECT is about as effective as antipsychotic medications and more effective than
psychotherapy. Supplementing antipsychotic medications with ECT is more effective than
antipsychotic medications alone. Use of ECT in chronic schizophrenia have been less
promising. ECT is effective in patients who respond poorly to antipsychotic medications.
Antipsychotic medications should be administered during and following ECT treatment.
ECT is used also to get rapid response especially in life threatening situation (catatonia,
suicidal, aggressiveness), poor response to treatment, poor compliance, large doses of anti
psychotic and we expect to lower the dose after ECT
Prognosis: When patients with acute schizophrenia receive an antipsychotic medication
approximately 60 percent improve to the extent that they will achieve a complete remission
or experience only mild symptoms; the remaining 40 percent of patients improve, but still
demonstrate variable levels of positive and negative symptoms that are resistant to the
medications.
DSM V Diagnostic Criteria for Schizoaffective Disorder
A. An uninterrupted period of illness during which there is a major mood episode (major
depressive or manic) concurrent with Criterion A of schizophrenia.
Note: The major depressive episode must include Criterion A1: Depressed mood.
B. Delusions or hallucinations for 2 or more weeks in the absence of a major mood
episode (depressive or manic) during the lifetime duration of the illness.
C. Symptoms that meet criteria for a major mood episode are present for the majority
of the total duration of the active and residual portions of the illness.
D. The disturbance is not attributable to the effects of a substance (e.g., a drug of
abuse, a medication) or another medical condition.
Treatment:
-Mood stabilizers: lithium, valproate (Depakote), and to a lesser extent carbamazepine
(Tegretol) in bipolar I disorder.
- Electroconvulsive therapy (ECT)
-Anti psychotics.
- Antidepressants.
DSM V Diagnostic Criteria for Delusional Disorder
The presence of one (or more) delusions with a duration of 1 month or longer.
B. Criterion A for schizophrenia has never been met.
Note: Hallucinations, if present, are not prominent and are related to the delusional
theme (e.g., the sensation of being infested with insects associated with delusions of
infestation).
C. Apart from the impact of the delusion(s) or its ramifications, functioning is not
markedly impaired, and behavior is not obviously bizarre or odd.
D. If manic or major depressive episodes have occurred, these have been brief relative
to the duration of the delusional periods.
E. The disturbance is not attributable to the physiological effects of a substance or
another medical condition and is not better explained by another mental disorder,
such as body dysmorphic disorder or obsessive-compulsive disorder.
Specify whether:
Erotomanic type: This subtype applies when the central theme of the delusion
is that another person is in love with the individual.
Grandiose type: This subtype applies when the central theme of the delusion is
the conviction of having some great (but unrecognized) talent or insight or having
made some important discovery.
Jealous type: This subtype applies when the central theme of the individual’s
delusion is that his or her spouse or lover is unfaithful.
Persecutory type: This subtype applies when the central theme of the delusion
involves the individual’s belief that he or she is being conspired against, cheated,
spied on, followed, poisoned or drugged, maliciously maligned, harassed, or obstructed
in the pursuit of long-term goals.
Somatic type: This subtype applies when the central theme of the delusion involves
bodily functions or sensations.
Mixed type: This subtype applies when no one delusional theme predominates.
Unspecified type: This subtype applies when the dominant delusional belief
cannot be clearly determined or is not described in the specific types (e.g., referential
delusions without a prominent persecutory or grandiose component).
Specify if:
With bizarre content: Delusions are deemed bizarre if they are clearly implausible,
not understandable, and not derived from ordinary life experiences (e.g.,

an individual’s belief that a stranger has removed his or her internal organs and
replaced them with someone else’s organs without leaving any wounds or
scars).
Shared Psychotic Disorder
(folie à deux)
This unusual condition has also been called folie a à deux and induced or shared psychotic
disorder. It develops in an individual in the context of a close relationship with another
person who has an established delusion that he or she also believes, and requires an absence
of psychotic disorder prior to the onset of the induced delusion; it is usually classified with
paranoid disorders.
Dr. Maytham Alyasiry