EXAMINATION OF THE
NEWBORN BABYThe objective of doing an examination of
the newborn baby is :-To do an early detection of any abnormality which may need urgent intervention and treatment shortly after birth, or to detect any other abnormalities which may need follow up or been able to be treated later on.
Also,the examination helps to:
-Identify any obvious major or minor malformations.
-To asses gestational age, nutrition and activity.
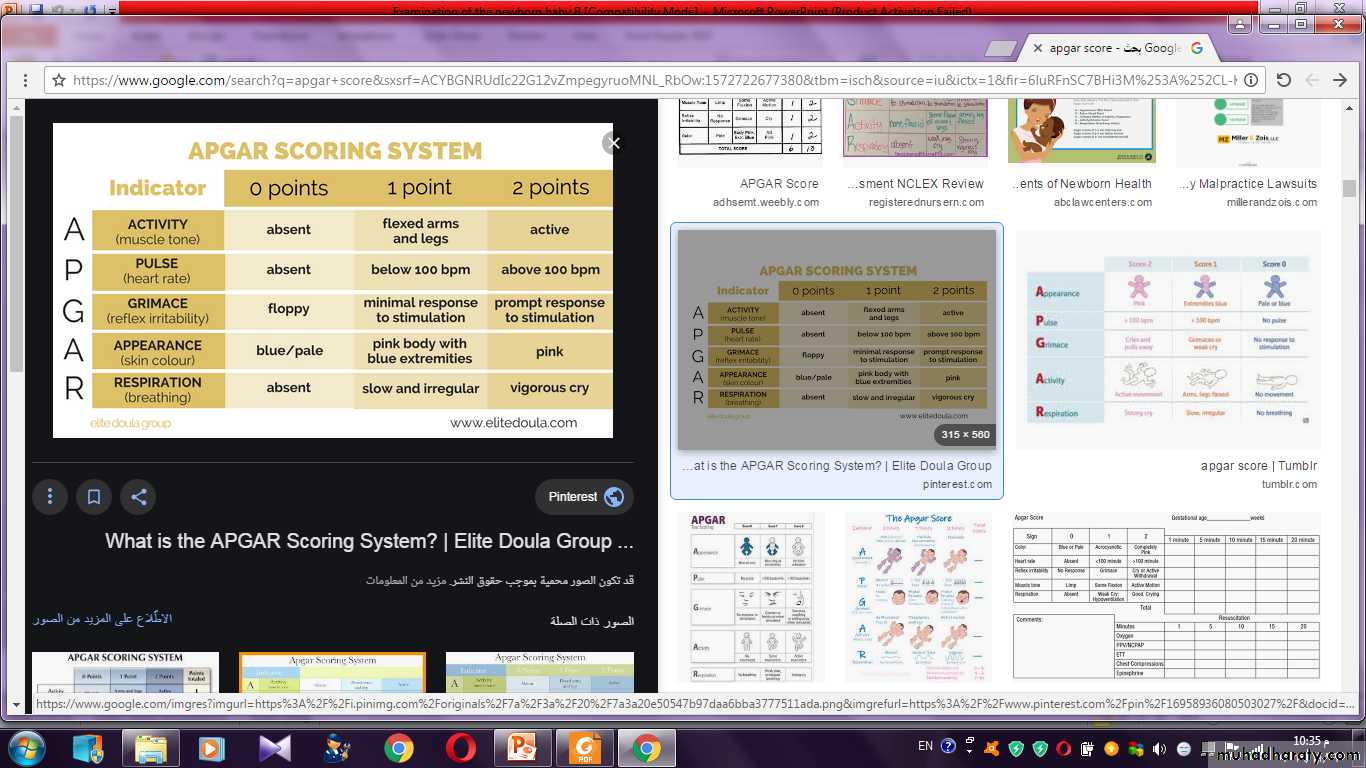
-To determine how well the baby handels the
transition from intra to extrauterine life, this can be
done by assessing what is called the APGAR scoring.
To have successful examination of the NBB, the baby
should be naked, warm , well illuminated, and stable.General examination:
First of all does the baby looks normal or abnormal, do the body proportions, head face and neck appears grossly normal?Are there any obvious deformities or unusual appearance?
Is the baby in distress or resting comfortably.
What is the color of the skin is it pink or it is pale, which may represent asphyxia, anemia, shock or edema.
If he is cyanosed, is it involving the hands and feet known as (acrocyanosis) especially when they are cold which is a normal phenomena due to vasomotor instability, or the cyanosis is central one due to cardiac, pulmonary or CNS disease.
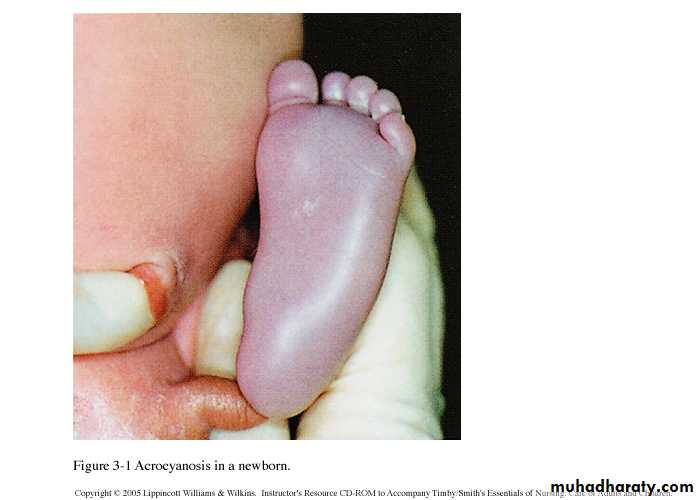
Acrocyanosis

cyanosis
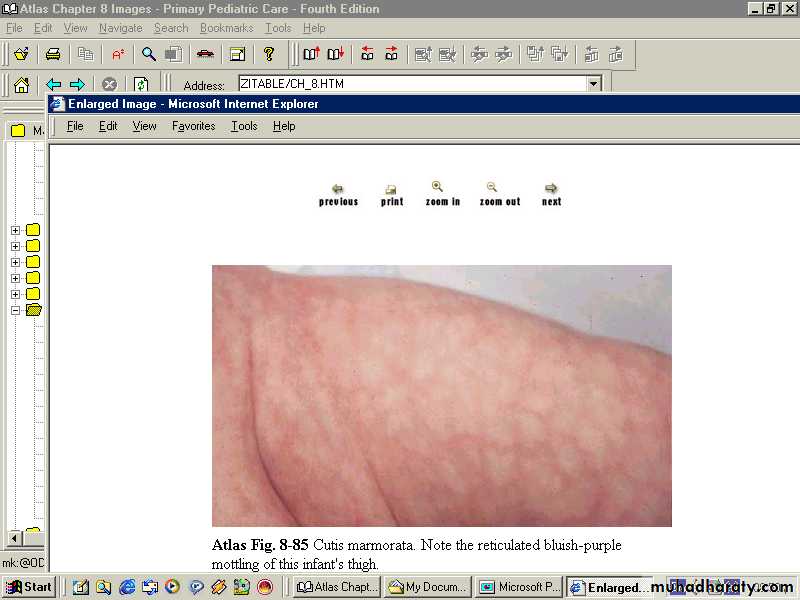
The extremities may be mottled with a net like pattern
if they are cool.Skin mottling usually indicate vasomotor instability, although it may signify sepsis or acidosis.
Another variation in skin color is the so called harlequin color change mostly seen in LBW infants where the baby’s skin is dark pink or reddish on the dependent half of the body while the upper half appears pale the two colors sharply demarcated along the midline (it is not pathological).
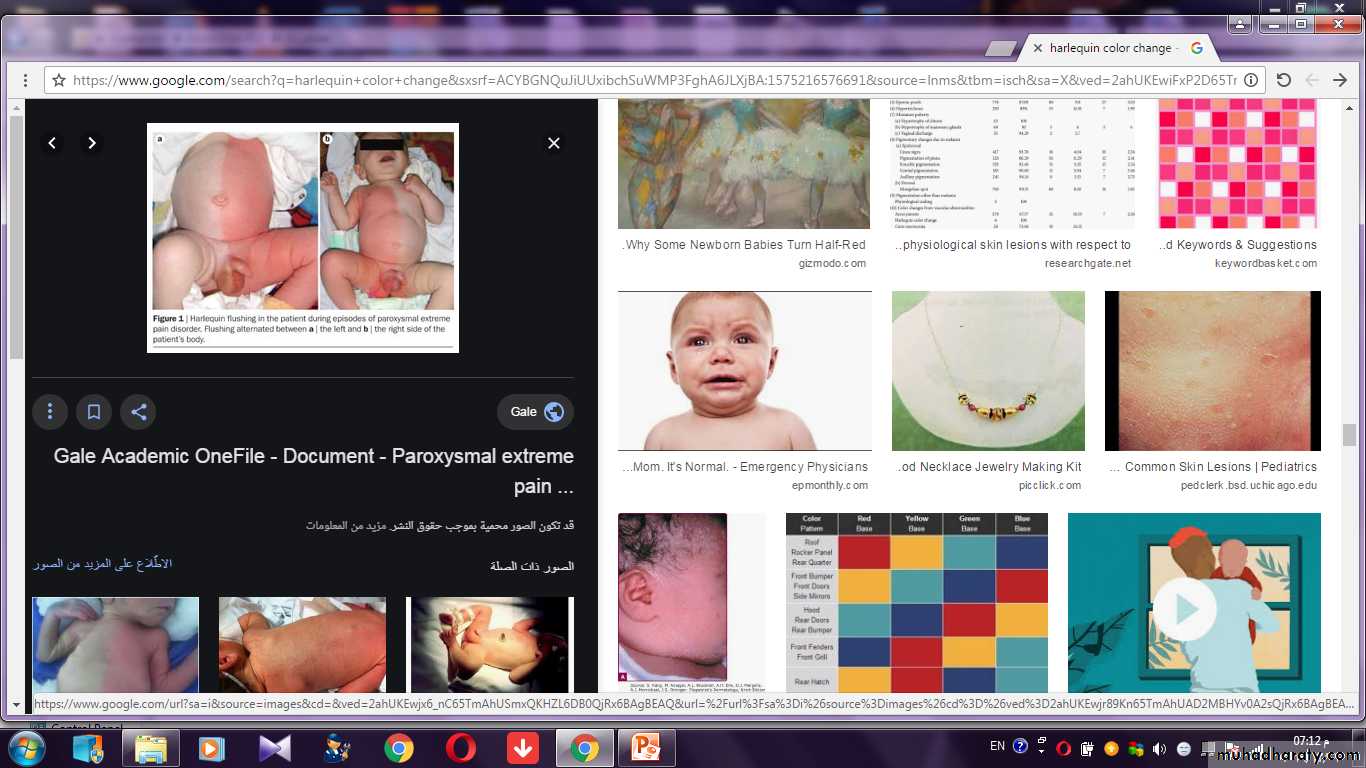
Harlequin colour change
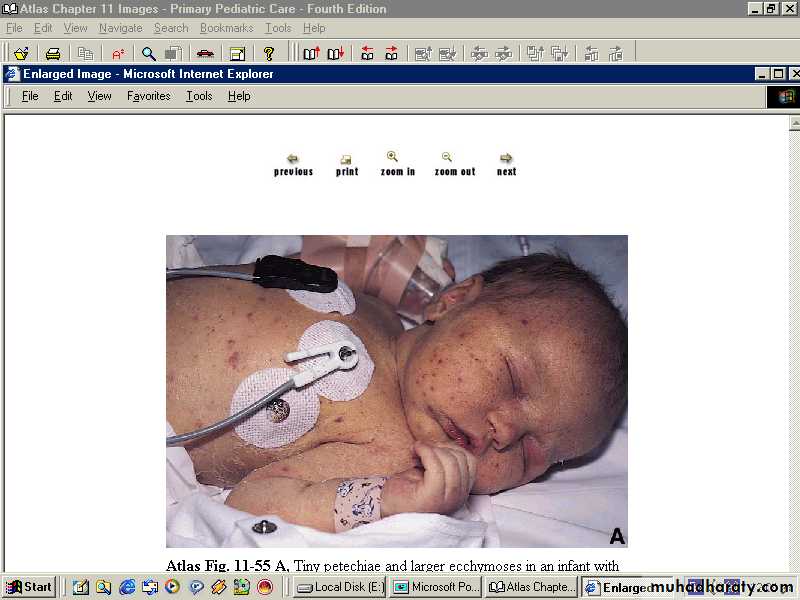
Look for petechiae which can be associated with increased
intravascular pressure during labor or due
to thrombocytopenia.
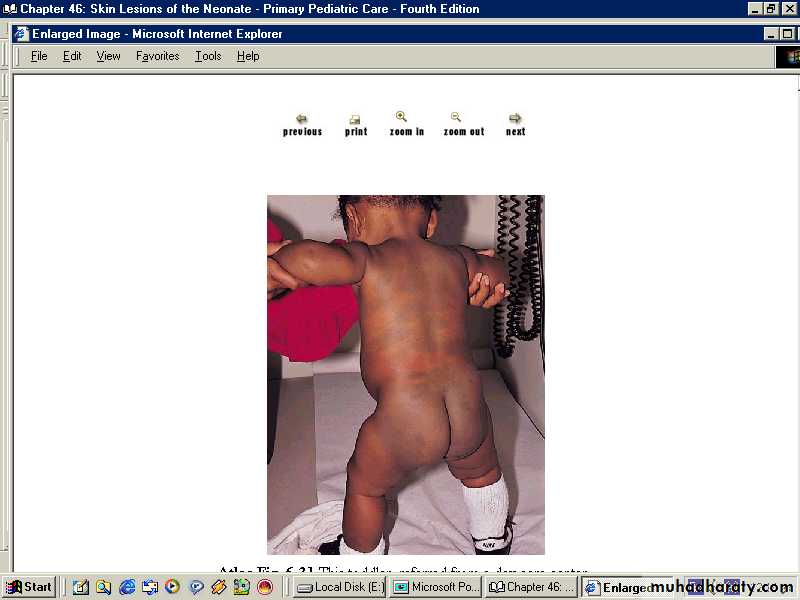
Mongolian blue spots:
Are blue well demarcated areas of pigmentation are seen overthe buttocks, back and sometimes other parts of the body,
they tends to disappear within the first year of life.
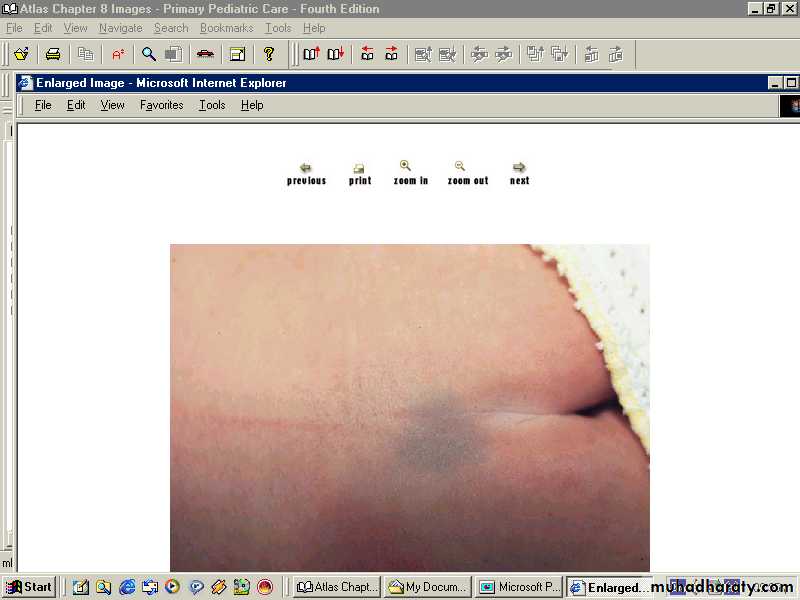
Mongolian spots
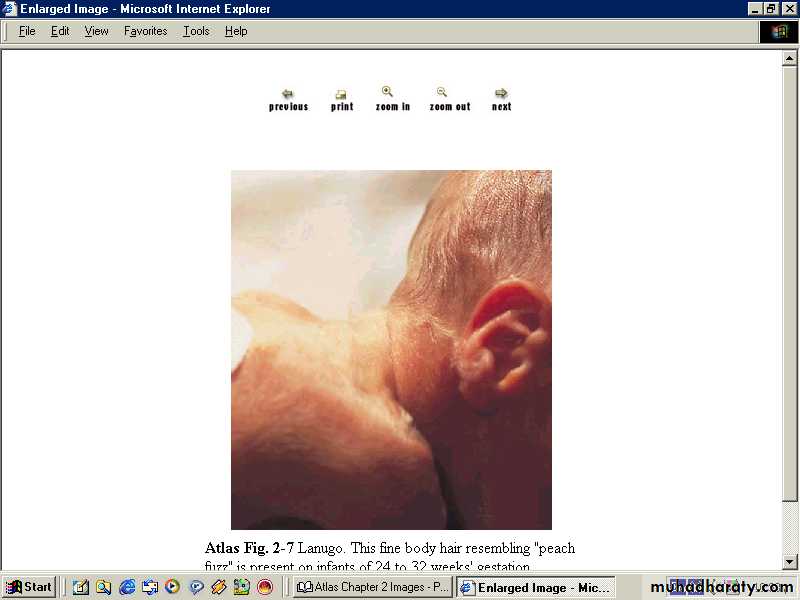
Fine soft immature hair lanugo hair frequently covers the scalp and may cover the face & shoulders in premature infants.
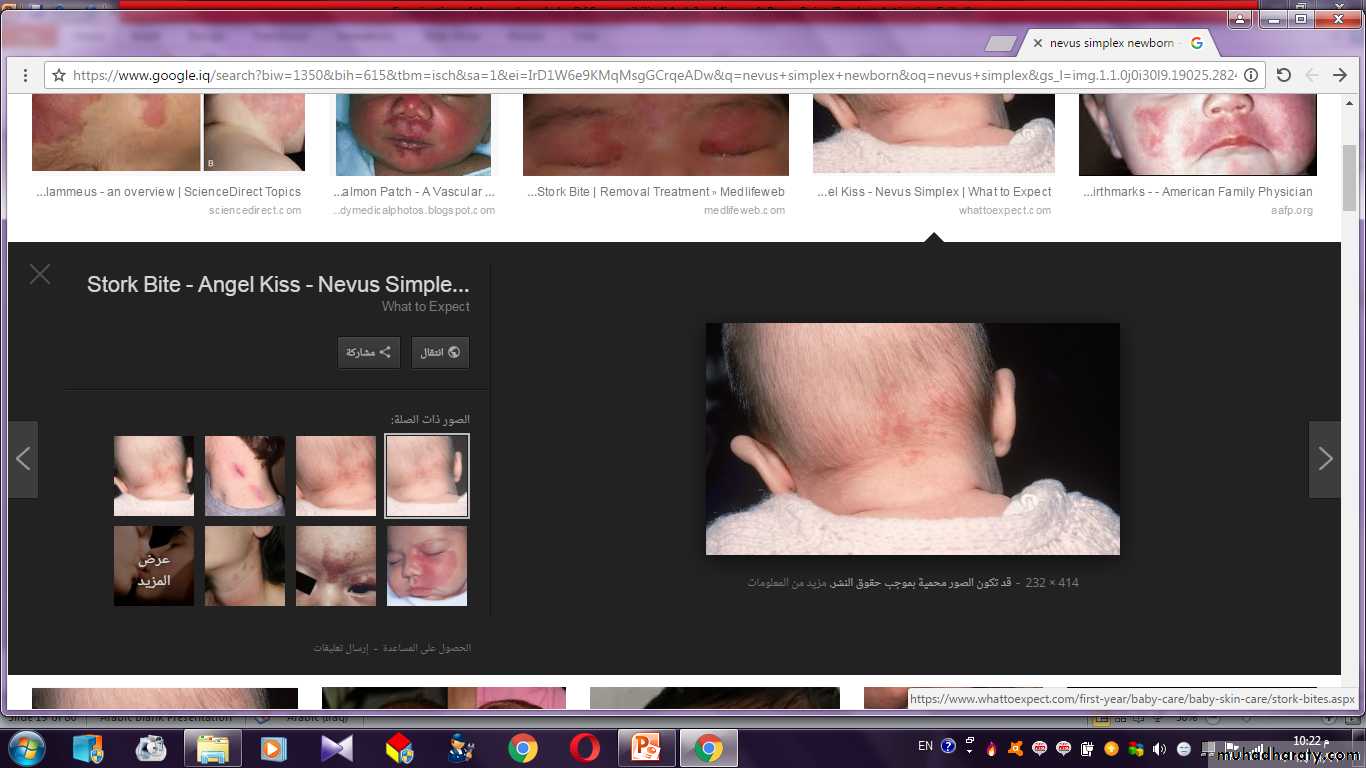
Salmon patch (nevus simplex):
are small pale pink ill defined flat vascular lesions that occurmostly on the glabella, eye lid upper lip & nuchal area in
30-40% of normal NBB, they may persist for several months
& become more visible with crying.
Nevus simplex
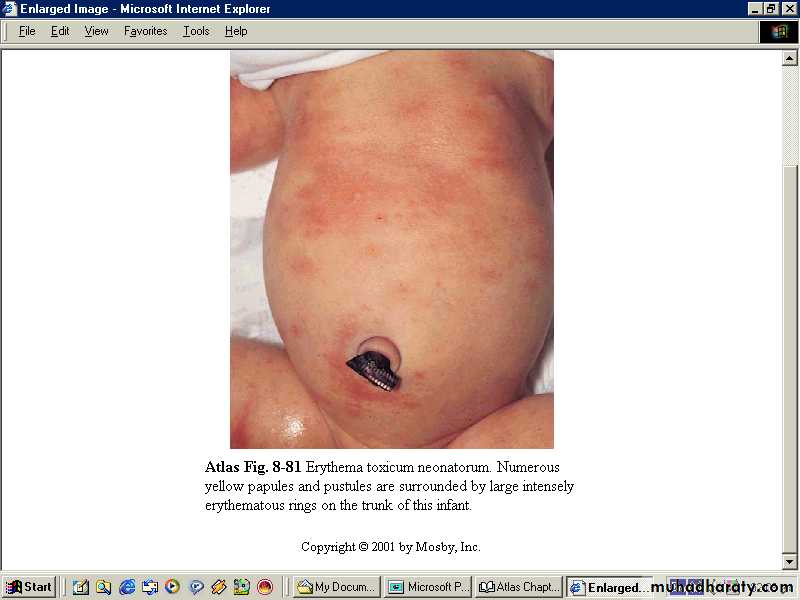
Erythema toxicum:benign self limited, the lesion are firm yellow white, 1-2 mm papule or pustules with a surrounding erythematous flare they may be sparse or numerous peak incidence is in the 2nd day of life and may last for 1 week.
Aspirate from the lesion show eosinophils infiltrate & absence of M.O. on a stained smear.
Pustular melanosis :
a benign lesion seen predominantly in black neonates, contains neutrophils and is present at birth as a vesiculopustular eruption around the chin, neck, back, extremities, and palms or soles; it lasts 2-3 days.
Pustular Melanosis
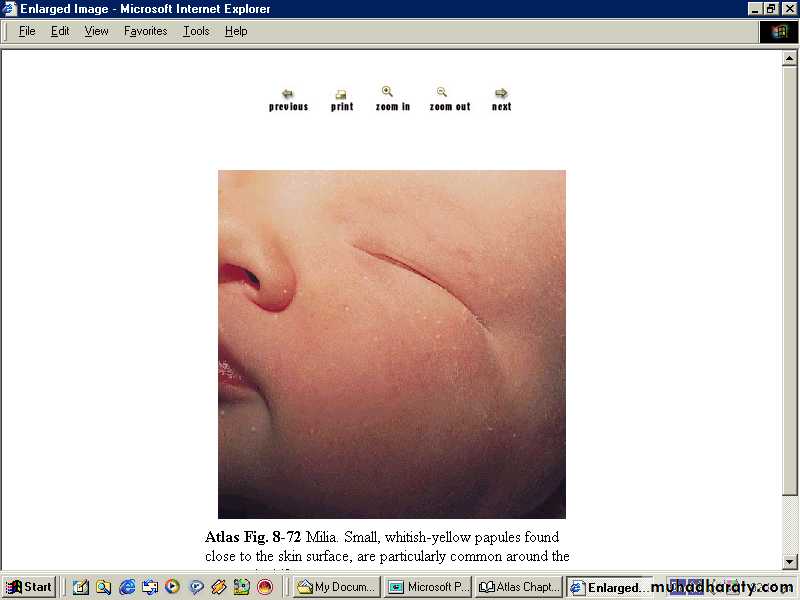
Milia:superficial epidermal inclusion cysts the lesion is firm papule
of 1-2 mm in diameter, pearly opalescent they are most
frequently scattered over the face, gingiva and on the midline
of the palate called Epistein pearl, it disappear spontaneously.
Miliaria:
Erythematous minute papulovesicular lesions may impact
a prickly sensation the lesions are usually located to sites of
occlusion or to flexural areas such as the neck, groin, and axilla.
It is due to retention of sweat in occluded sweat ducts.

Portwine stain (nevus flammeus):
Dilated dermal capillaries macular sharply demarcated pink to purple, vary in size, head and neck are most commonly involved, usually unilateral.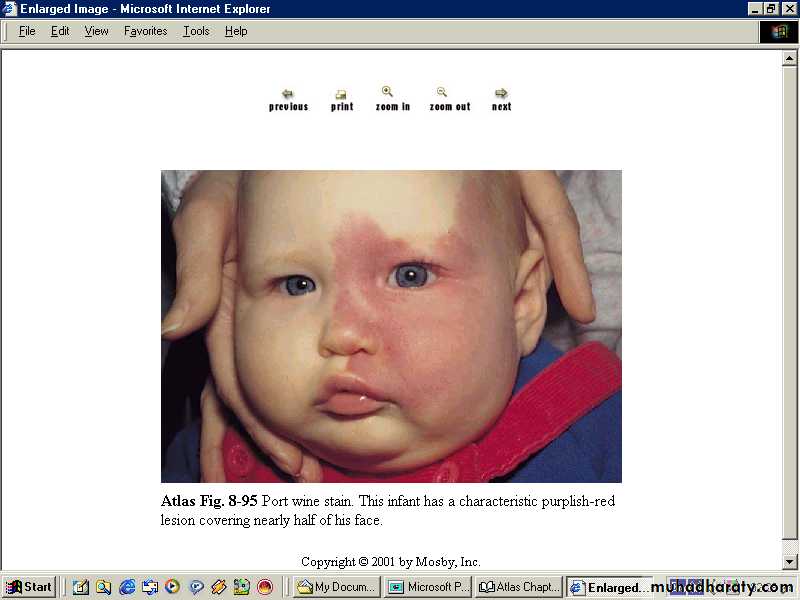
Strawbery nevus:
Bright red capillary hemangiomas protuberant, compressable, any part of the body can be affected.
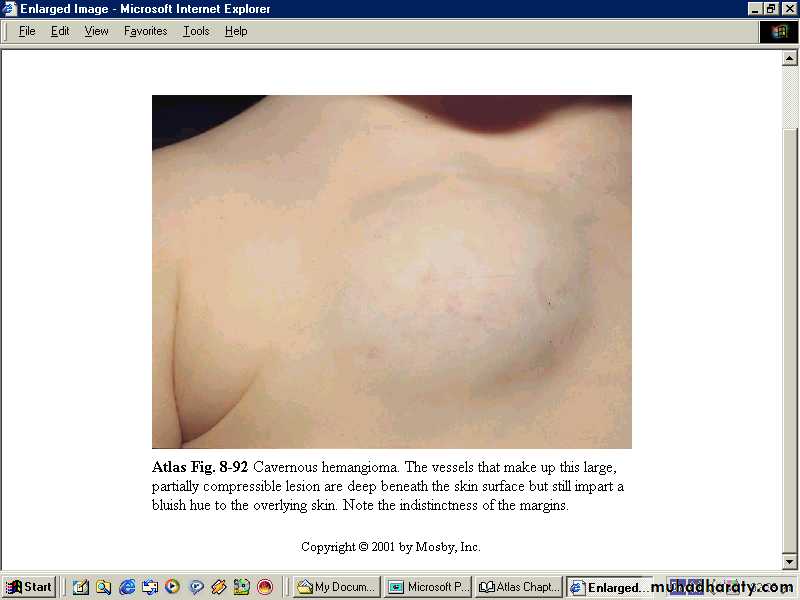
Cavernous hemangioma:
Ill defined & more diffuse, cystic, compressable, theoverlying skin color either normal or bluish.
Head:
The head circumference of all newborns should be plotted on a growth chart to identify an excessively small head (microcephaly) or excessively large head (megalencephaly).The head may be molded particularly if the baby is the 1st born. A rounded symmetrical head is seen if a baby is born by C-section or breach delivery, whereas babies born by vaginal vertex delivery usually has a head that is elongated occipitally with some overriding of the sutures & possibly a caput succedaneum or cephalhematoma.
Caput appears as a circular boggy area of edema with indistinct borders and often with overlying ecchymosis. It is a collection of subcutaneous oedema fluid caused by pressure during passage through the birth canal, present at birth, disappear within the 1st few days of life.

Caput succedaneum
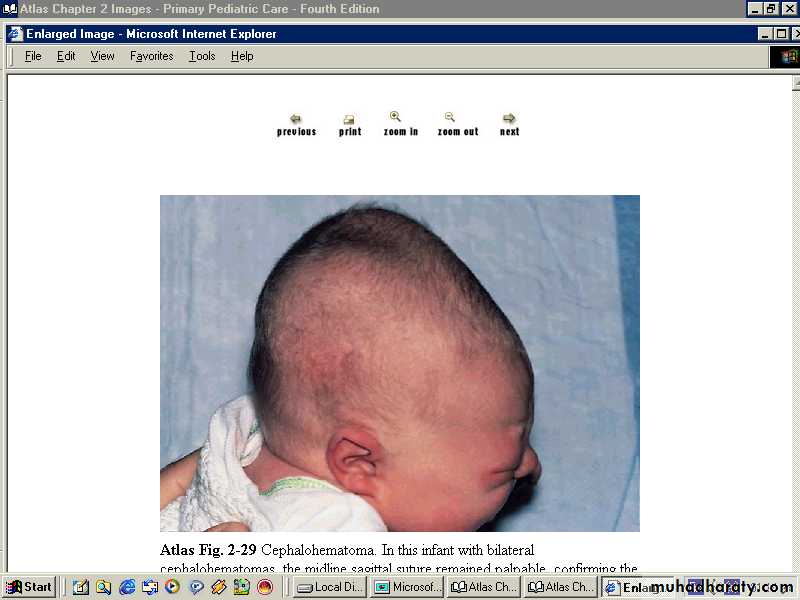
Cephalhematoma is a subperiosteal collection of blood
limited by the sutures of the skull it is soft to fluctuantstarts few hours after delivery and it lasts several weeks to
disappear.
The anterior fontanel should be flat or slightly sunken when the baby is held in the upright position & is quite, the size of the ant fontanel 1-3 cm in diameter,
post fontanel is either closed at birth or it is closed during the 1st 4 months of life.
Causes of large anterior fontanel:-
-Prematurity.-Hydrocephalus.
-Achondroplasia.
-Hypothyroidism.
-Intrauterine growth retardation.
-Osteogenesis imperfecta.
-Congenital rubella.
-Hypophosphatasia.
Trisomies (21,18,13).
Rickets (in older infants).
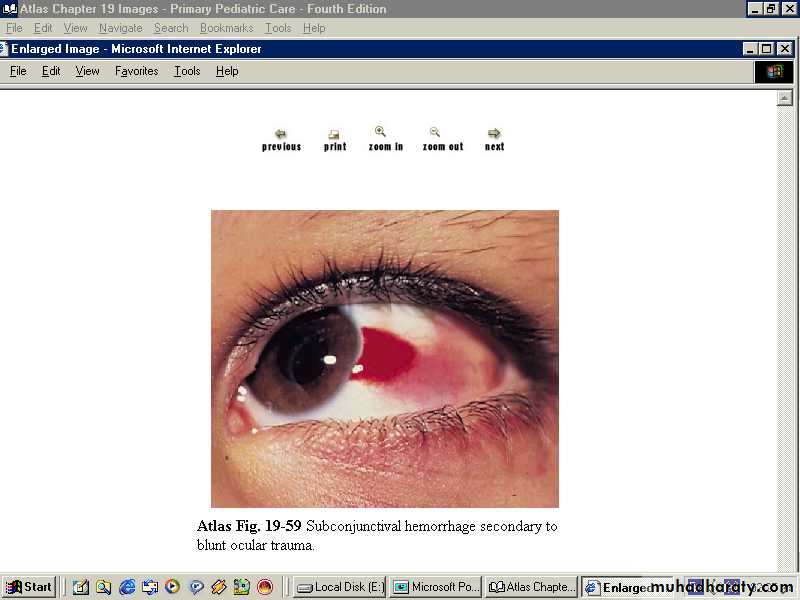
Eyes:
subconjunctival or retinal hemorrhage are not significant, occur during
difficult and assisted labor. They resolve within 2-4 weeks
Pupillary reflex should be present, the iris should be
inspected for colobomas or heterochromias:-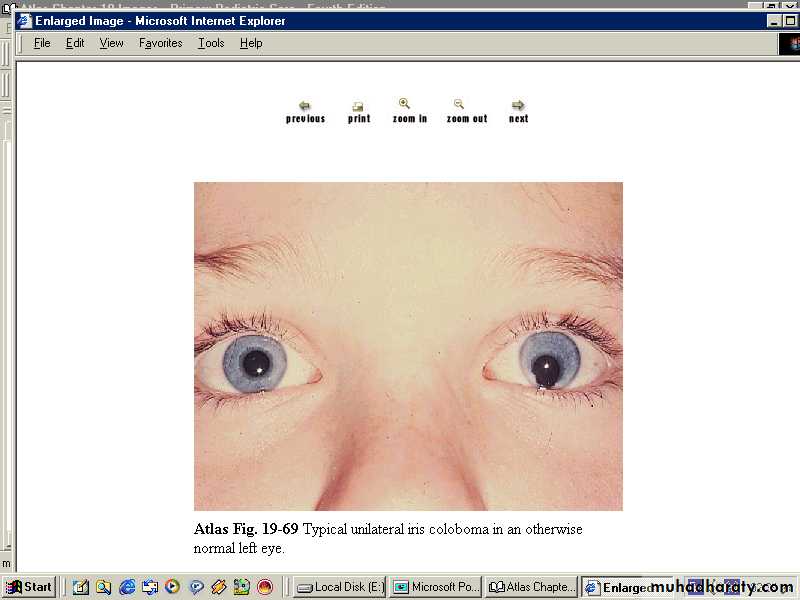
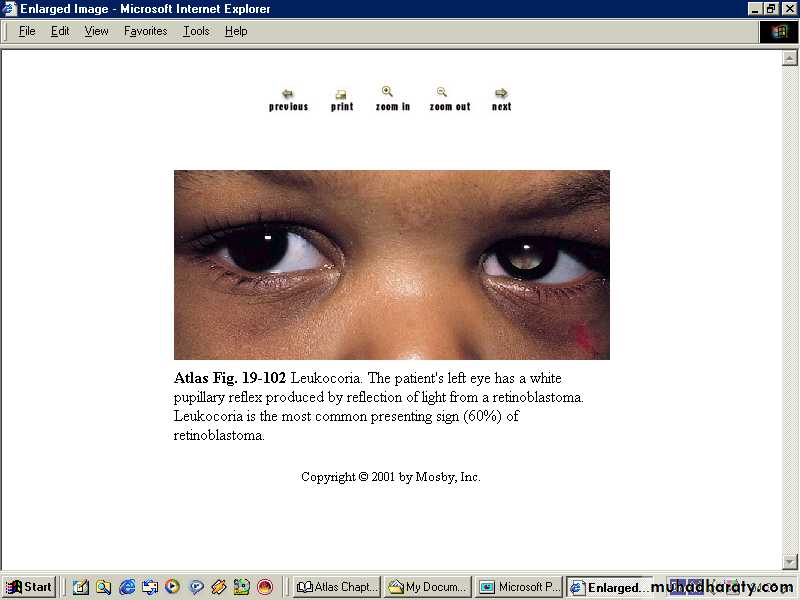
Presence of bilateral red reflex exclude cataract or
other intraoccular pathology.But white pupillary reflex (leukocorea) is seen in:-
cataract, tumor (retinoblastoma), chorioretinitis, retinopathyof prematurity, persistent hypeplastic primary viterious.
-A cornea of more than 1cm (megalocornea) with
photophobia and tearing suggest congenital glaucoma:-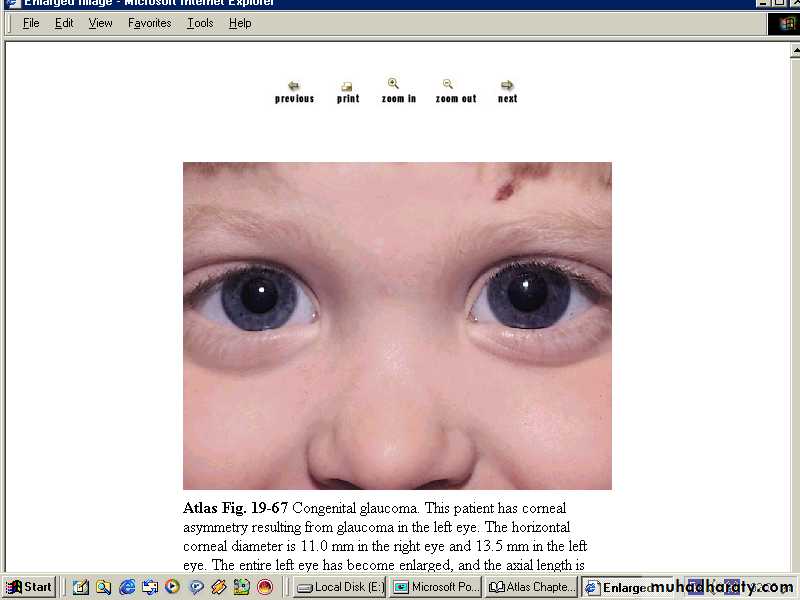
Mouth:
natal tooth in the lower incisor position may be seen, these teeth are usually shed before the eruption of thedeciduous teeth.
The hard & the soft palate should be inspected for a cleft palate. Epstein pearl may be seen on the hard palate.
Ankyloglossia (tongue tie) present when the frenulum of the
tongue is short.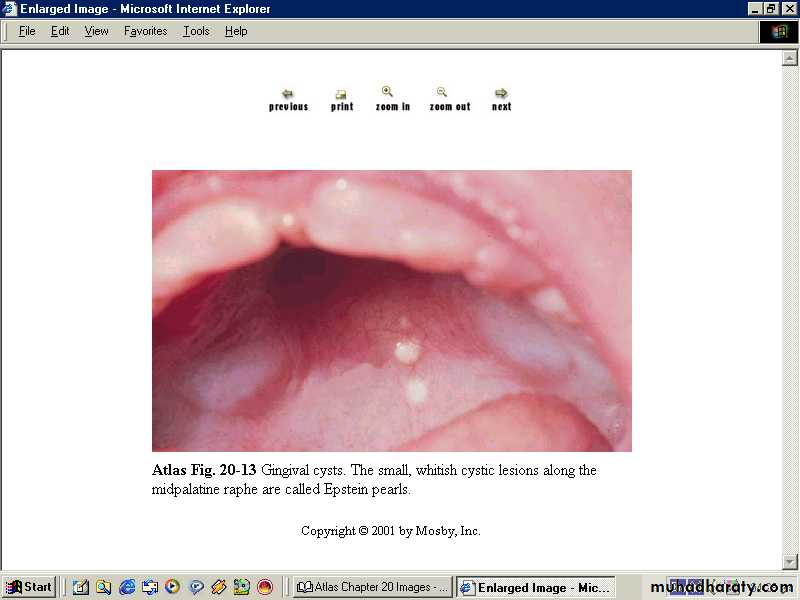
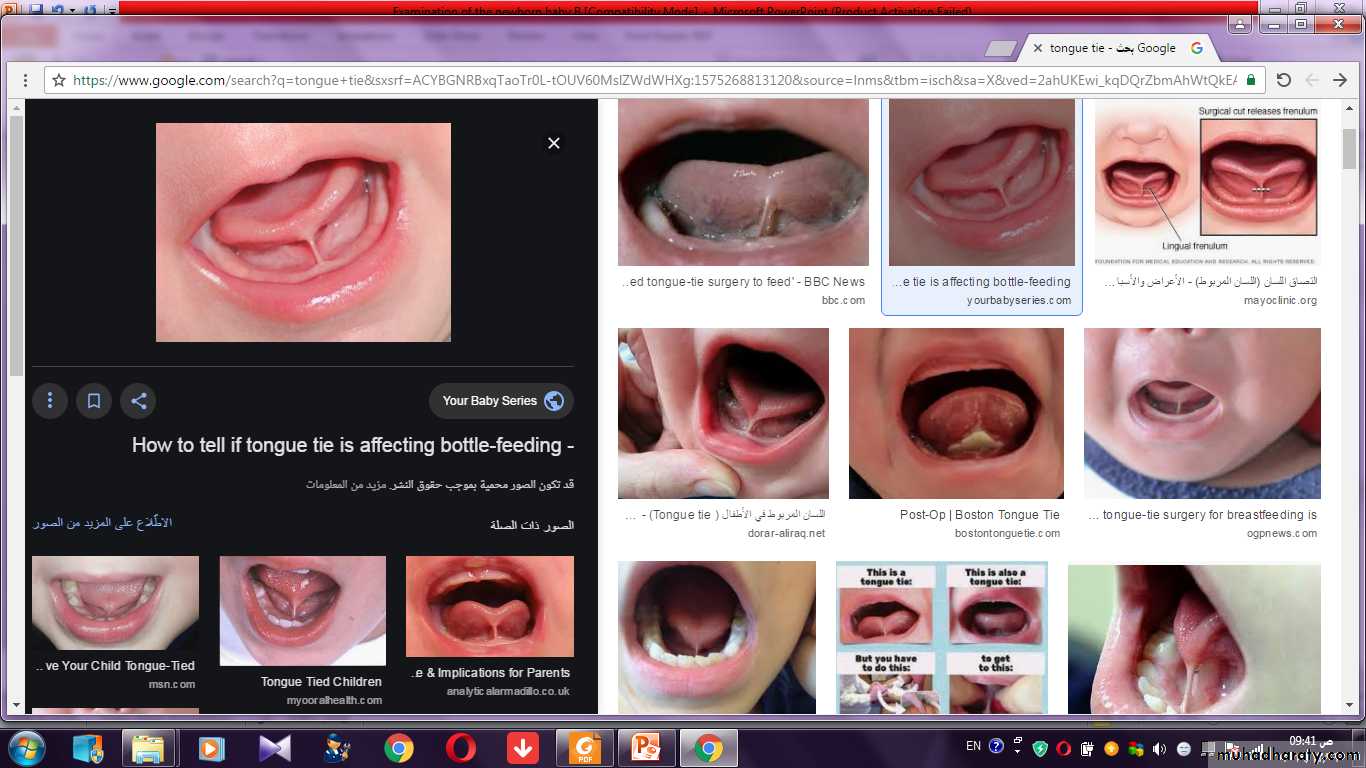
Ankyloglossia (tongue tie)
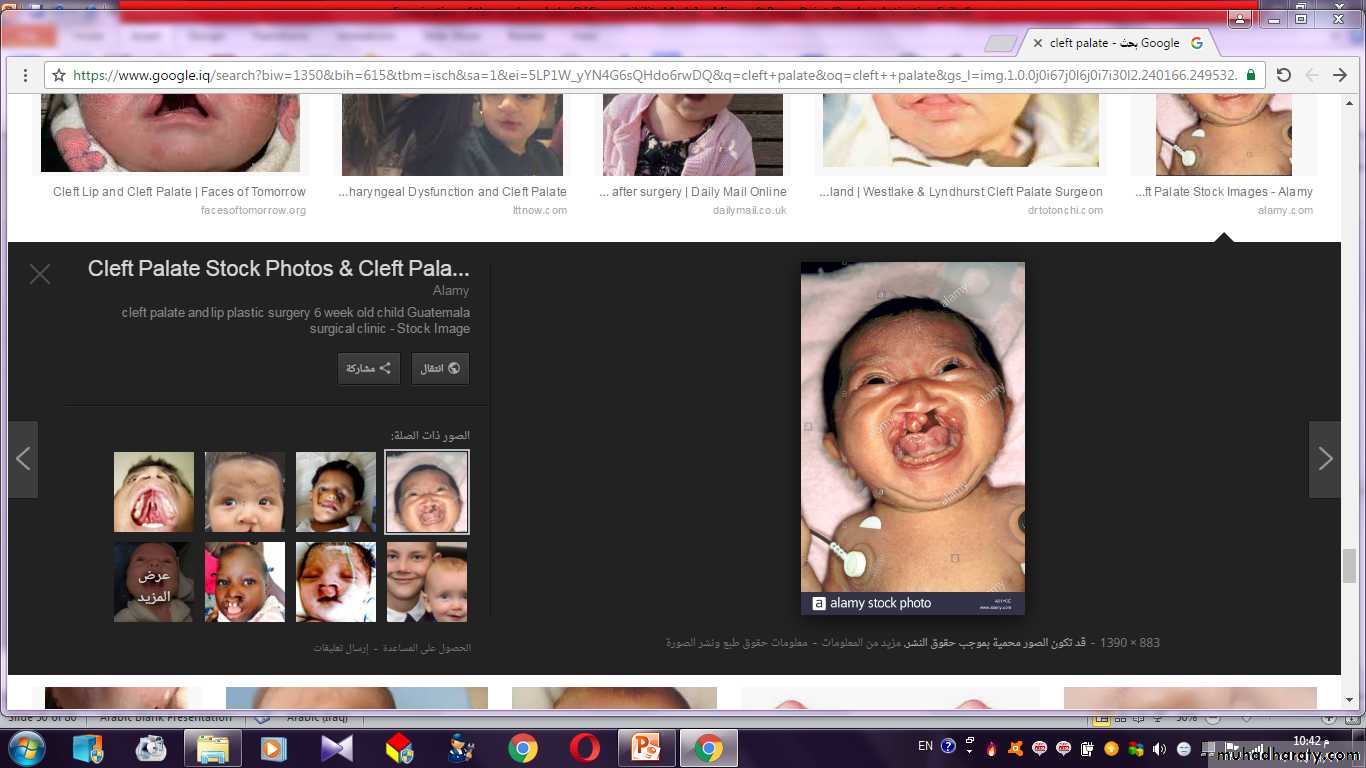
Cleft lip and pallet
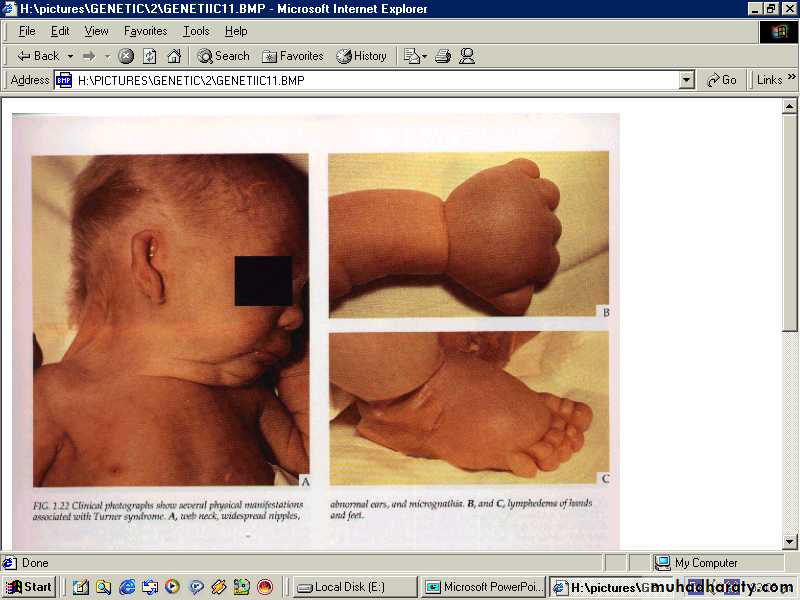
Neck:It is relatively short in the newborn, there may be goiter, cystic hygroma, sternomastoid tumor, webbing of the neck in female suggest Turner syndrome, both clavicles should be palpated for fractures.

Chest:
Breast hypertrophy is common & milk may be present. Asymmetry, erythema. tenderness, induration suggest abscess formation. Widely spaced nipples suggest turner syndrome.
Also observe the respiratory rate which is normally between 30-40/min in full term baby and in resting state, a rate of >60 is abnormal. The resp rate in preterm baby is higher, the premature infant may have a periodic breathing.
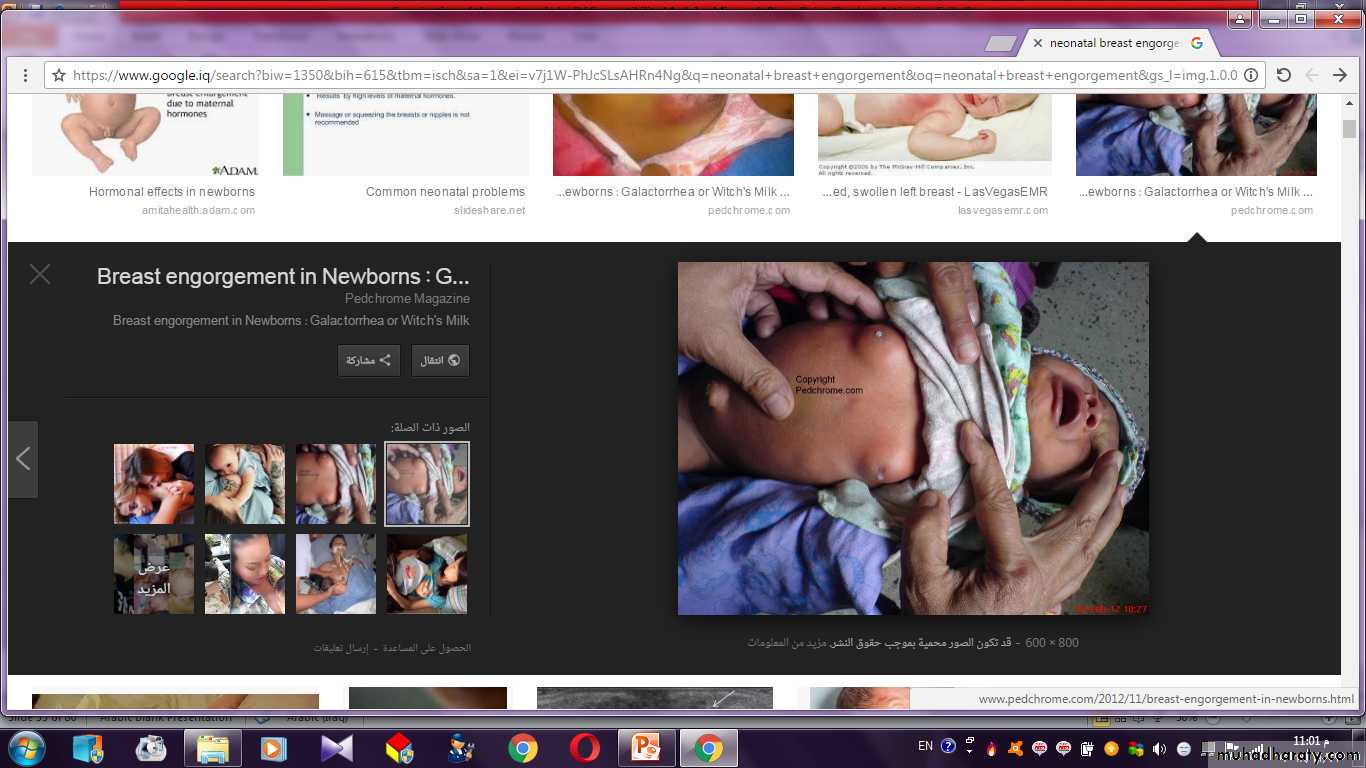
Breast Engorgement
Heart:localize the heart to exclude dextrocardia & there may be transitory murmur in normal heart and congenital heart disease may not initially produce a murmur that will be present later.
The rate may vary from 100 per min in relaxed sleep to 180 per min during activity, the pulse should be palpated in the upper & lower extremities to detect coarctation of the aorta.
Abdomen:
the liver is usually palpable sometimes as much as 2cm less commonly the spleen tip may be felt , the abdominal wall is usually weak especially in premature infant , umbilical hernia is a common finding.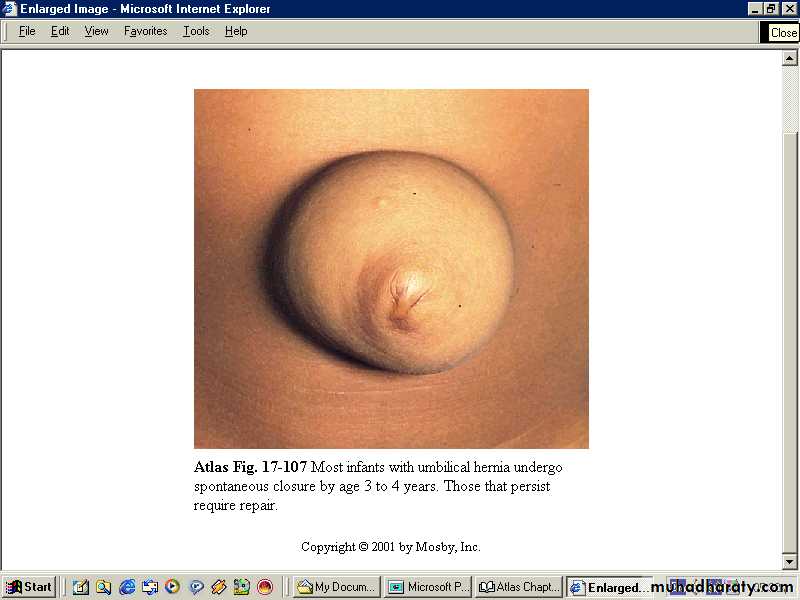
Omphalitis:-
Is an acute local inflammation of the periumbilical tissuethat may extent to the abdominal wall, the peritoneum, the
umbilical vein and portal vessels, or the liver and may
result in later portal hypertension.

omphalitis
Abdominal masses:-may be cystic as in:-
1. Hydronephrosis.2. Polycystic kidney.
3. Adrenal hemorrhage.
4. Intestinal duplication.
5. Choledocal cyst.
6. Ovarian, omental, or pancreatic cyst.
Or the abdominal masses are solid as in:
1. Neuroblastoma.
2. Hepatoblastoma.
3. Teratoma.
4. Renal vein thrombosis(flank mass).
Abdominal distention at or shortly after birth suggests either intestinal obstruction or GIT perforation.
Later distention suggests lower bowel obstruction, sepsis, or peritonitis. A scaphoid abdomen suggests diaphragmatic hernia.
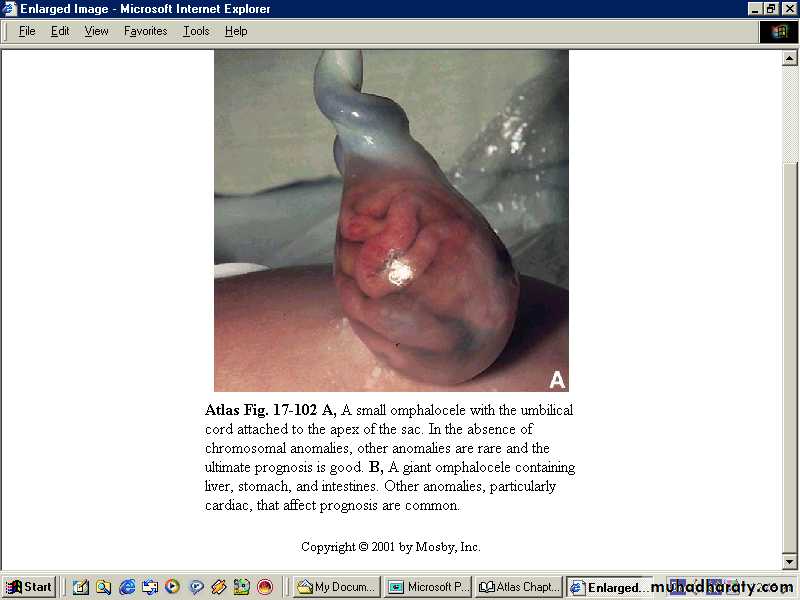
Omphalocele is an abdominal wall defect through the umbilicus where a herniation of the abdominal viscera which are covered by the peritoneum.

Gastroschisis:
The abdominal defect lies to the right of an intact umbilical cord, and the intestine lie exposed without a covering sac, free in the amniotic fluid.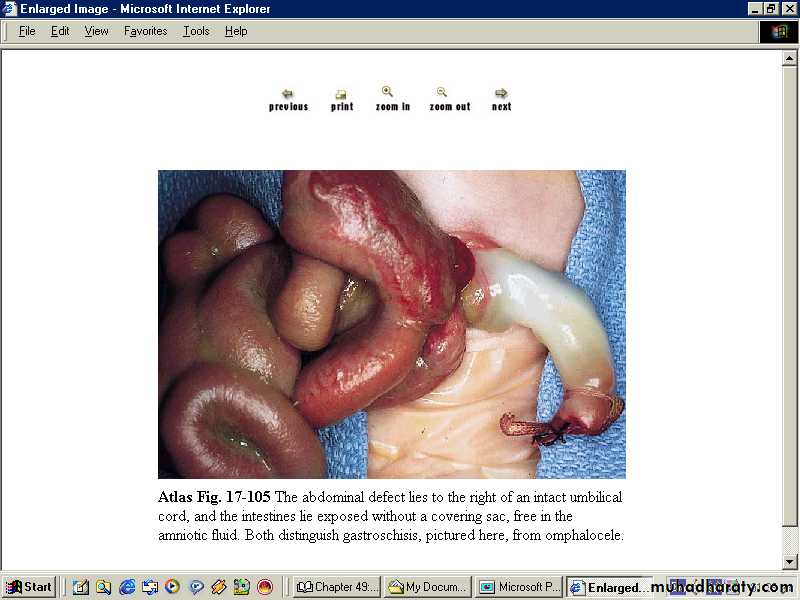
gastroschisis
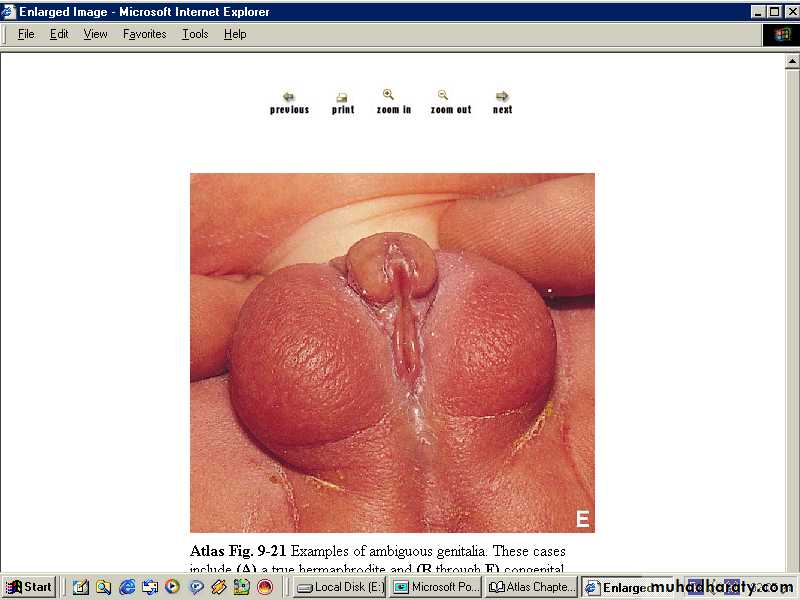
Genitalia:look for ambiguous genitalia, vaginal discharge or bleeding may occur normally after birth, it is transient due to the effects of maternal hormones.
Also look for undescended testes in male babies.
Anus:
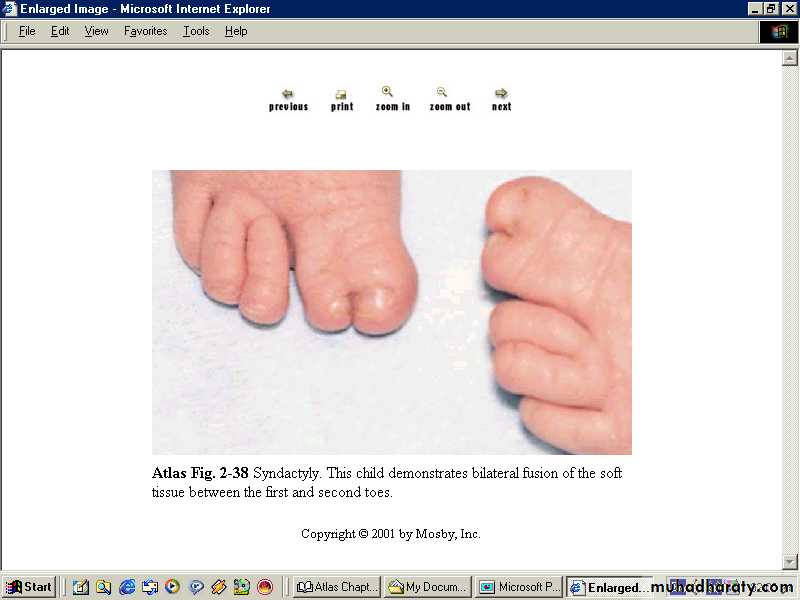
should be examined for unperforated anus although not all the cases are visible you may need to have gentle insertion of the little finger or a rectal tube.Extremities:
hands &feet for polydactyly or syndactyly, nerve injury or fracture seen by observing spontaneous or stimulated movements of the extremities.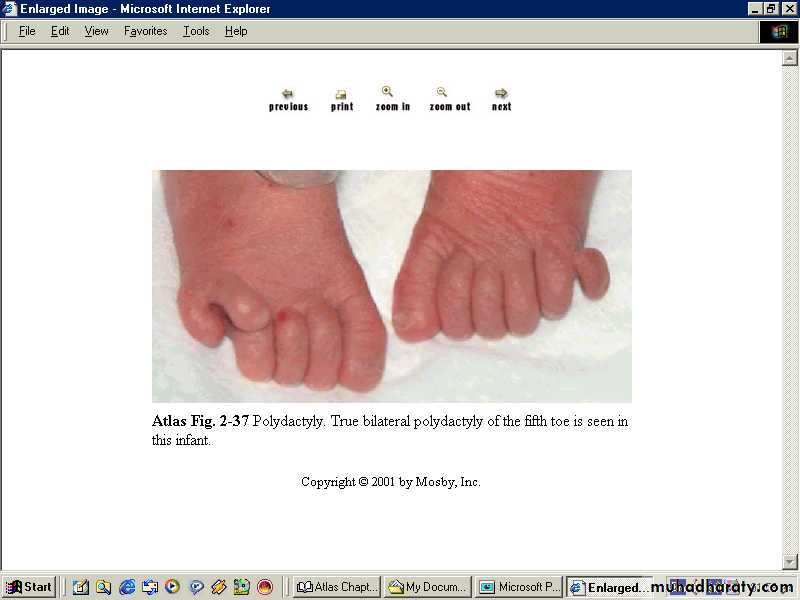

Clubfeet
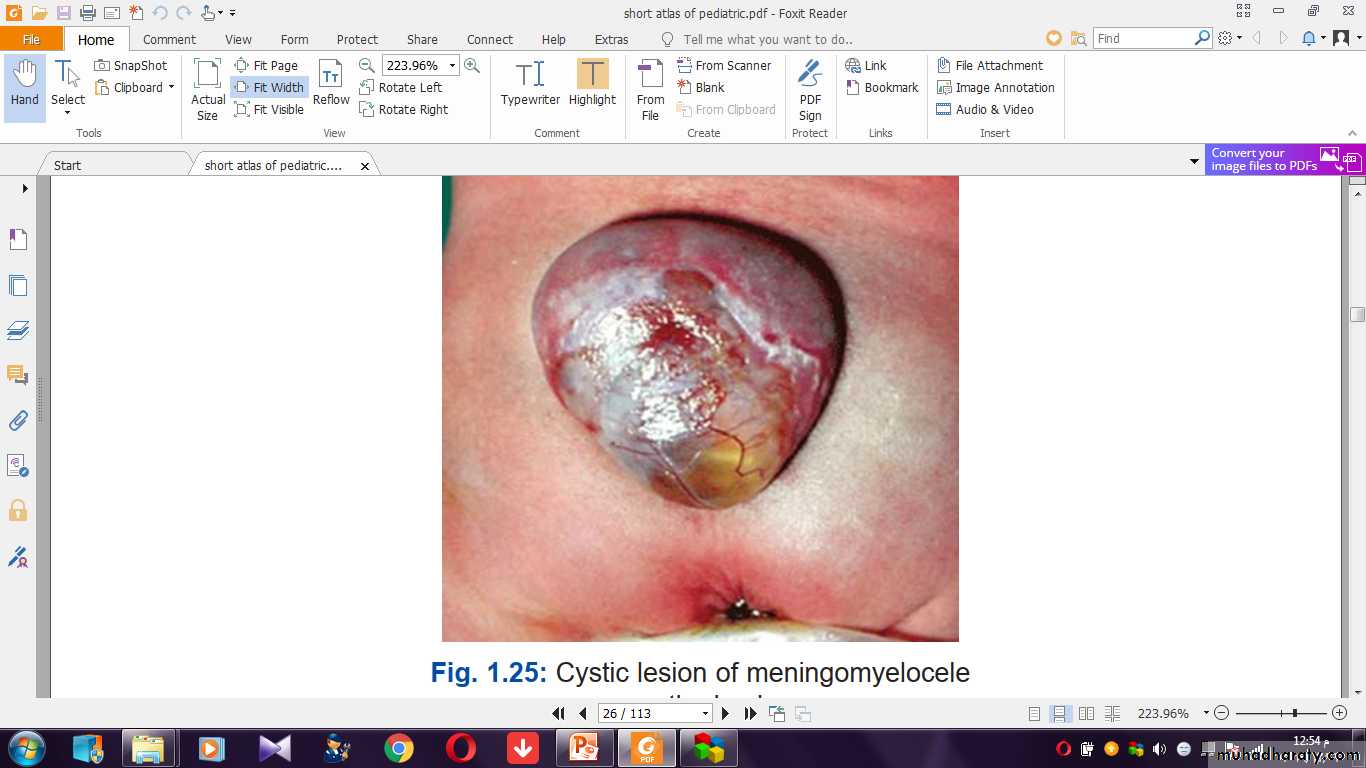
The Back:Look for meningocele and meningomyelocele.
Primitive neonatal reflexes:-
Moro reflex:To elicit the reflex, the head is supported and allowed to drop to the level of the bed. There will be initial extension response of the upper limbs, followed by flexion and crying.
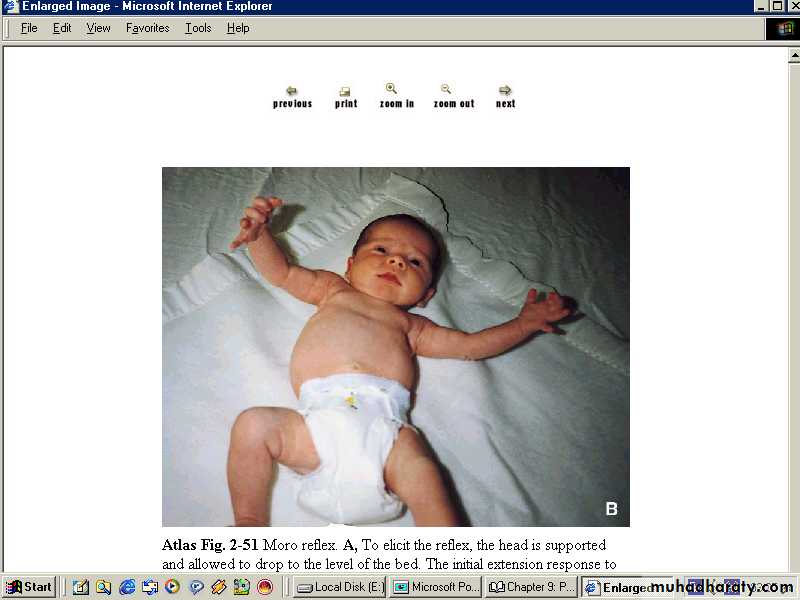
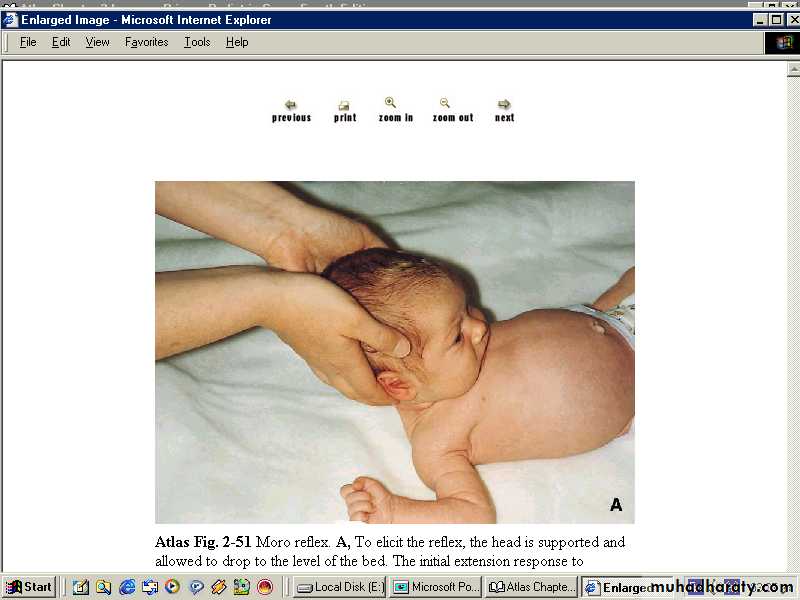
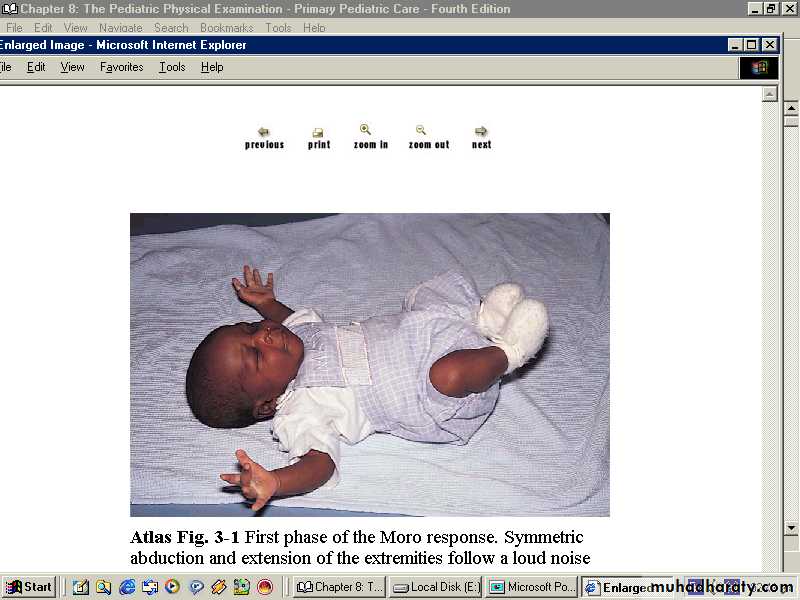
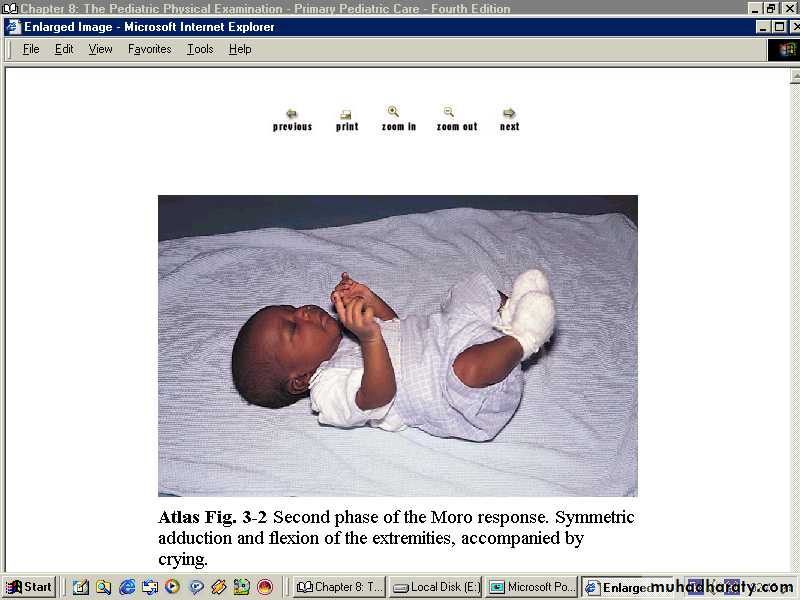
Moro reflex
2nd phase1st phase
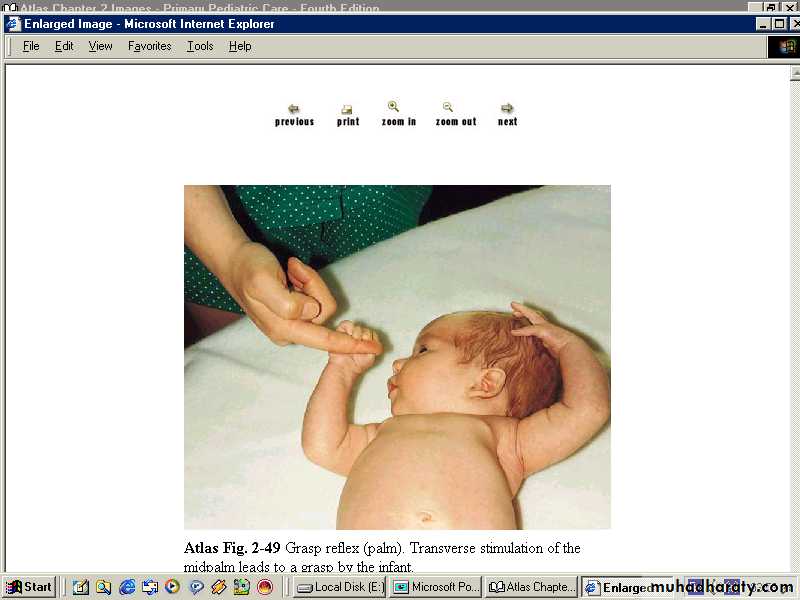
Grasp reflex: it is elicited by placing a finger or object in the open palm, the normal infant will grasp the object and with attempted removal the grip is reinforced.
Rooting reflex:-
The infant opens the mouth and turns the head towards the pacifier or the examiner finger stimulating the cheek.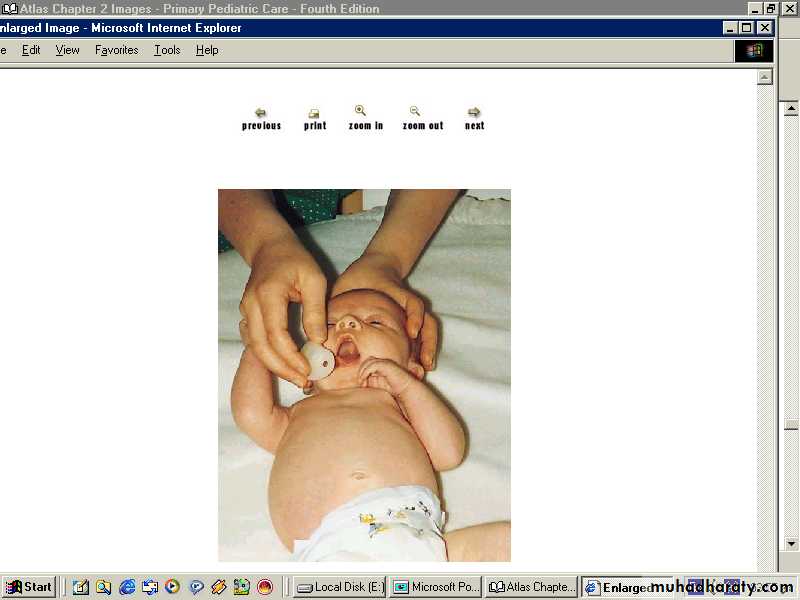
Sucking reflex:-
Vigorous sucking movements are initiated when an object is placed in the infant's mouth..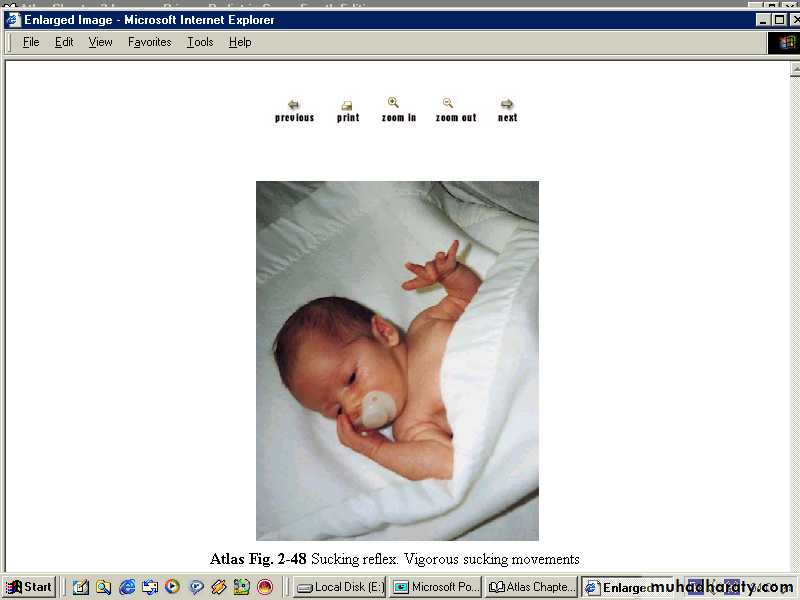
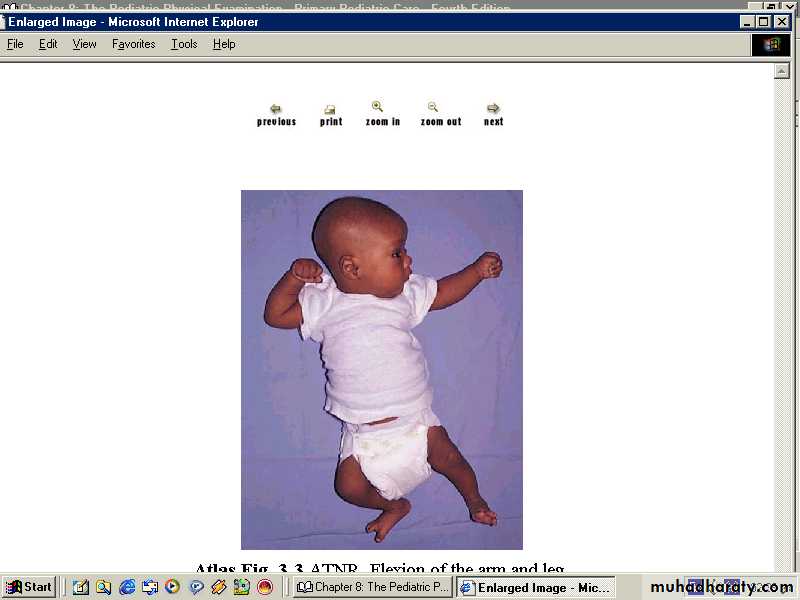
Tonic neck reflex:-
when manually turning the head to one side while supine,extension of the arm occurs on that side of the body
corresponding to the direction of the face while flexion
develops on the contralateral extremities.