Dysmenorrhea
Dysmenorrhea is defined as pain and cramping during menstruation that interferes with normal activities.Most women experience some degree of pain at least on the first day of the period, when the loss is heaviest. Discomfort during menstruation ranges from mild to severe pain that causes some patients to be bedridden. Fifty percent of menstruating women suffer from dysmenorrhea and 10% of these are incapacitated for 1 to 3 days each month.
Aetiology
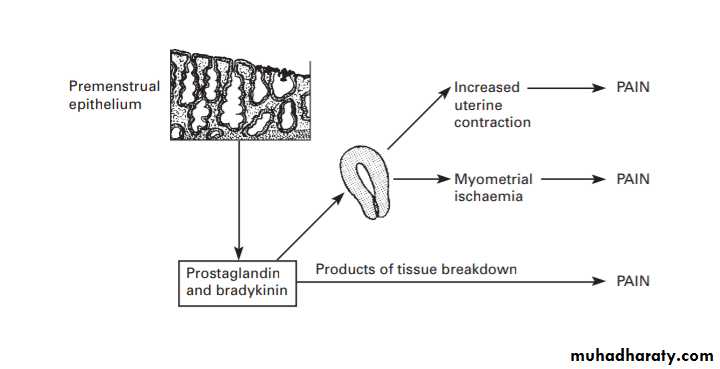
There is increased myometrial activity during the periods in women with dysmenorrhoea and uterine blood flow is reduced, especially during intense contractions. It is thought that this hyperactivity is the result of excessive quantities of prostaglandins synthesised during the breakdown of the premenstrual endometrium.
Theories accounting for 1° dysmenorrhoea include:
*Abnormal PG ratios or sensitivity.
*Neuropathic dysregulation.
*Venous pelvic congestion.
*Psychological causes.
Classification:
1° dysmenorrhoea is idiopathic menstrual pain without identifiable pathology.Usually occurs before age 20, pain in the menstrual cycle is a feature of ovulatory cycles and is due to uterine vasospasm and ischaemia, nervous sensitization due to PGs and other inflammatory mediators, and uterine contractions. A maternal or sibling history of dysmenorrhea is very common and the problem usually starts soon after menarche.
2° dysmenorrhoea is painful menses due to underlying pathology , these include:
Endometriosis: pain from endometriosis may begin 1 to 2 days to weeks before mense, worsens 1 to 2 days before menstruation, and is relieved at or right after the onset of menstrual flow
Adenomyosis.
PID.
Pelvic adhesions.
Fibroids (though not always causal).
Cervical stenosis (iatrogenic post-LLETZ or instrumentation).
Asherman’s syndrome.
Congenital abnormalities causing genital tract obstruction, e.g. non-communicating cornua.
Diagnosis
History
• Timing and severity of pain (including degree of functional loss): commonly premenstrual pain i in the first 1–2 days of bleeding, then seases. Pelvic pain and deep dyspareunia (may signify pelvic pathology).
• Previous history of PID or STIs.
• Previous abdominal or genital tract surgery (may cause adhesions).
Examination
Abdominal exam to exclude pelvic masses.
Pelvic exam: cervical excitation, adnexal tenderness, mobility, and masses.
Investigations
STI screen (including Chlamydia swab).
USS endometrioma, PID sequelae, fibroids, congenital abnormalities.
Laparoscopy is usually reserved for women with USS abnormalities, medical treatment failures, or those with concomitant subfertility.
Management
Appropriate reassurance and analgesia may be all that is required. Often, primary dysmenorrhea will decrease throughout a patient’s 20s and early 30s. In addition, a pregnancy carried to viability will usually decrease the symptoms of primary dysmenorrhea.
Symptom control:
Nonmedical options include the use of heating pads and patches to the lower abdomen, exercise, massage, acupuncture, hypnosis vitamin B1, and magnesium
NSAIDs : Mefenamic acid 500mg tds with each period is effective
COCP to abolish ovulation (data on Mirena IUS demonstrate benefit )
TENS may be of benefit to some women.
Treat any underlying causes:
Endometriosis : COCP, progestagens, GnRH analogues
PID antibiotics
Cervical stenosis : relief of obstruction (usually surgical)
Therapeutic laparoscopy for above indications: gold standard for diagnosis + management of endometriosis/adhesions/complicated PID.
Hysterectomy is now rare for this indication alone.
Laparoscopic uterine nerve ablation (LUNA) is not currently recommended.
When no disease is identified then ovulation suppression by tricycling COCP or GnRH analogues for up to 6–12mths will limit the number of ‘periods’ and therefore pain. This is an empirical trial of hormonal therapy.
Pain clinic, psychological support, and self-help groups may be of benefit to some women who wish to maintain their fertility, especially when they have other pelvic pain symptoms.
Premenstrual Syndrome
Premenstrual syndrome (PMS) : Distressing psychological, physical, and/or behavioural symptoms in the absence of organic or psychiatric disease, regularly recurs during the luteal phase of cycle and disappears or regresses by the end of menstruation.
premenstrual dysphoric disorder (PMDD) is its more severe variant.
In the general population 15% of women are asymptomatic, 50% have mild premenstrual syndrome (PMS) symptoms, 30% moderate, and 5–10% severe.
The highest incidence occurs among women in their late 20s to early 30s. PMS more prevalent in women who are obese, perform less exercise and are of lower academic achievement , lower prevalent in women using hormonal contraception.
1) Psychological symptoms:
mood swings
depression
anxiety
irritability
loss of confidence
feeling out of control
2) physical symptoms:
Headaches
bloating
mastalgia
3) behavioural symptoms:
reduced visuospatial cognitive ability
increase in accidents
These symptoms must occur in the 2 weeks prior to menstruation and there must be at least a 7-day symptom-free interval in the first half of the menstrual cycle. Symptoms must occur in at least two consecutive cycles for the diagnosis to be made.
Aetiology
unknown but cyclical ovarian activity and the effect of estradiol and progesterone on the neurotransmitters serotonin and GABA appear to be key factors.
Absence of PMS before puberty, in pregnancy and after the menopause supports this theory.
Diagnosis:
Most women self-diagnose.A detailed history can suggest a diagnosis of PMS, but only prospective assessment with a symptom diary can establish its true nature.
A variety of symptom charts are available from the National Association of Premenstrual Syndrome.
Moderate/severe PMS involves disruption of work and interpersonal relationships, or interference with normal activities.
It is important to exclude organic disease and significant psychiatric illness.
Perimenopausal women may have increasing premenstrual symptoms as well as menopausal symptoms.
Symptome diary of PMS :
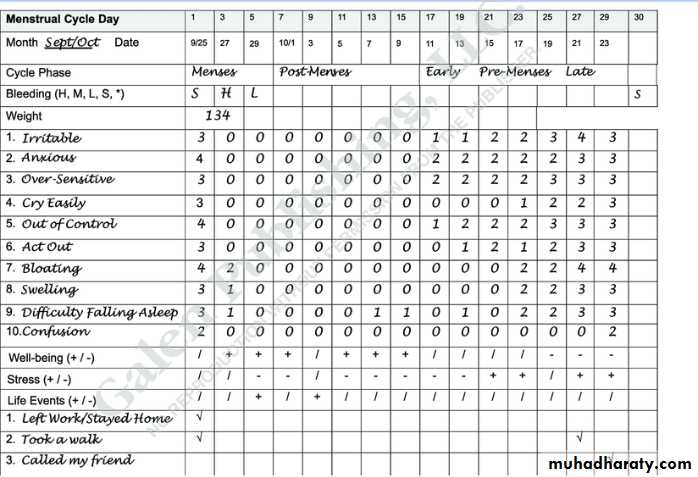
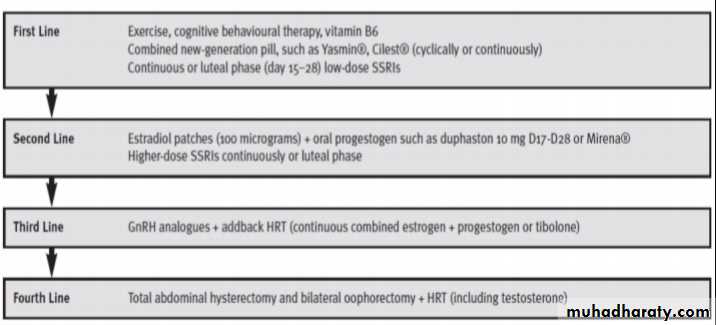
Management of PMS