1
) ﻋﺪد اﻻوراق
10
(
ﻋﯿﻮن
24
/
1
1
/
2019
.د
ﻋﺰام
Lec: 7
Lens
Objectives:
1 To describe anatomy and physiology of the crystalline lens.
2 To discuss age-related cataract and illustrate its management
lines.
3 To compose management plans of congenital cataract.
4 To sketch a diagram of leucokoria.
5 To demonstrate cases of ectopia lentis. 6- To review a video of
cataract surgery.
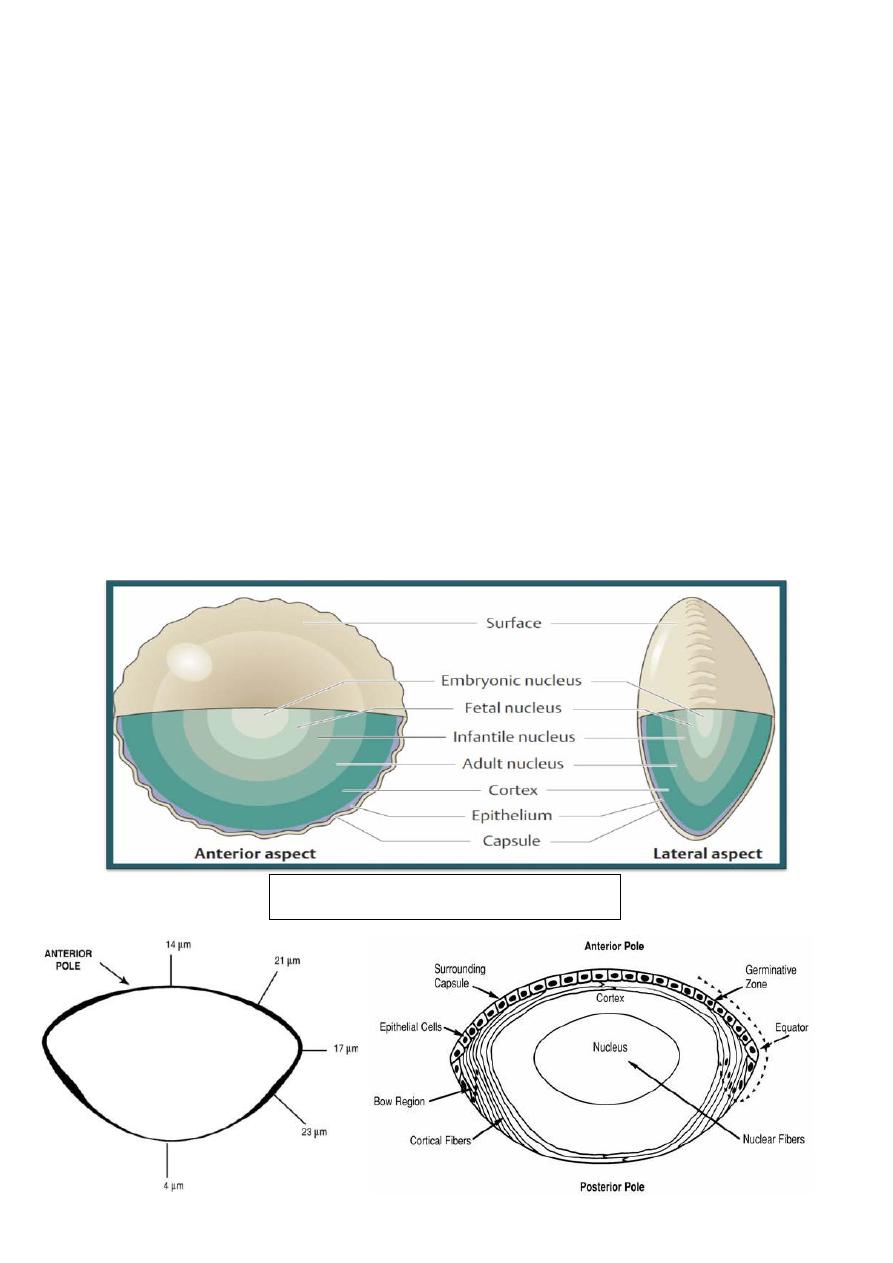
Anatomy and physiology:
Anterior and posterior capsule
2
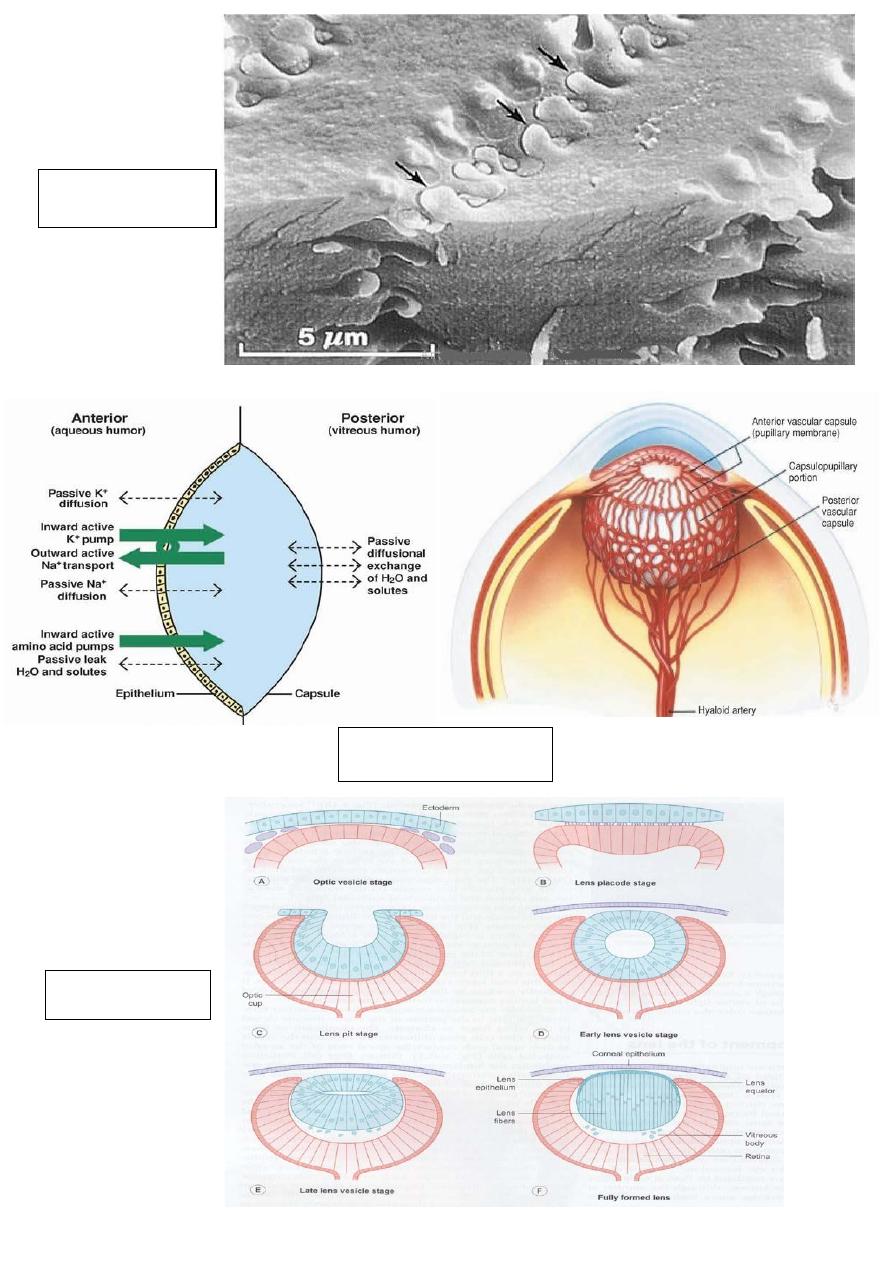
Lens fibres
physiology
Embryology
3
Age-related cataract
Definition:
Cataract is an opacity of the natural
crystalline lens. It is an extremely
common cause of visual impairment in
older patients.
Presentation and symptom:
Gradual painless decline in visual acuity.
Terminology:
• Phakia= presence of natural lens
• Pseudophakia= presence of artificial lens (IOL implantation)
Aphakia= absence of natural and artificial lens
4
Classification:
Acquired cataract:
• Classification
1 According to location
2 According to maturity
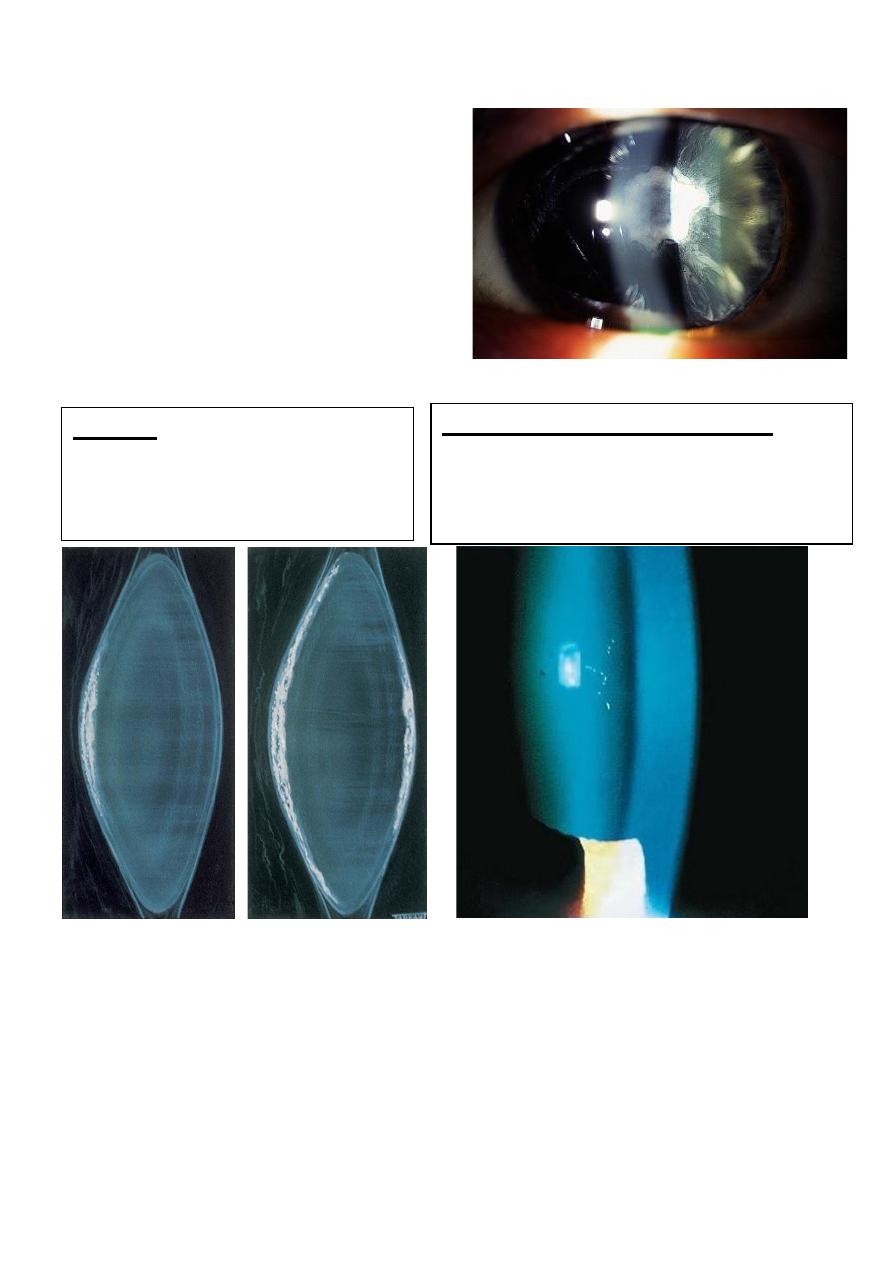
Immature:
In which the lens is partially opaque.
Mature:
In which the lens is completely opaque.
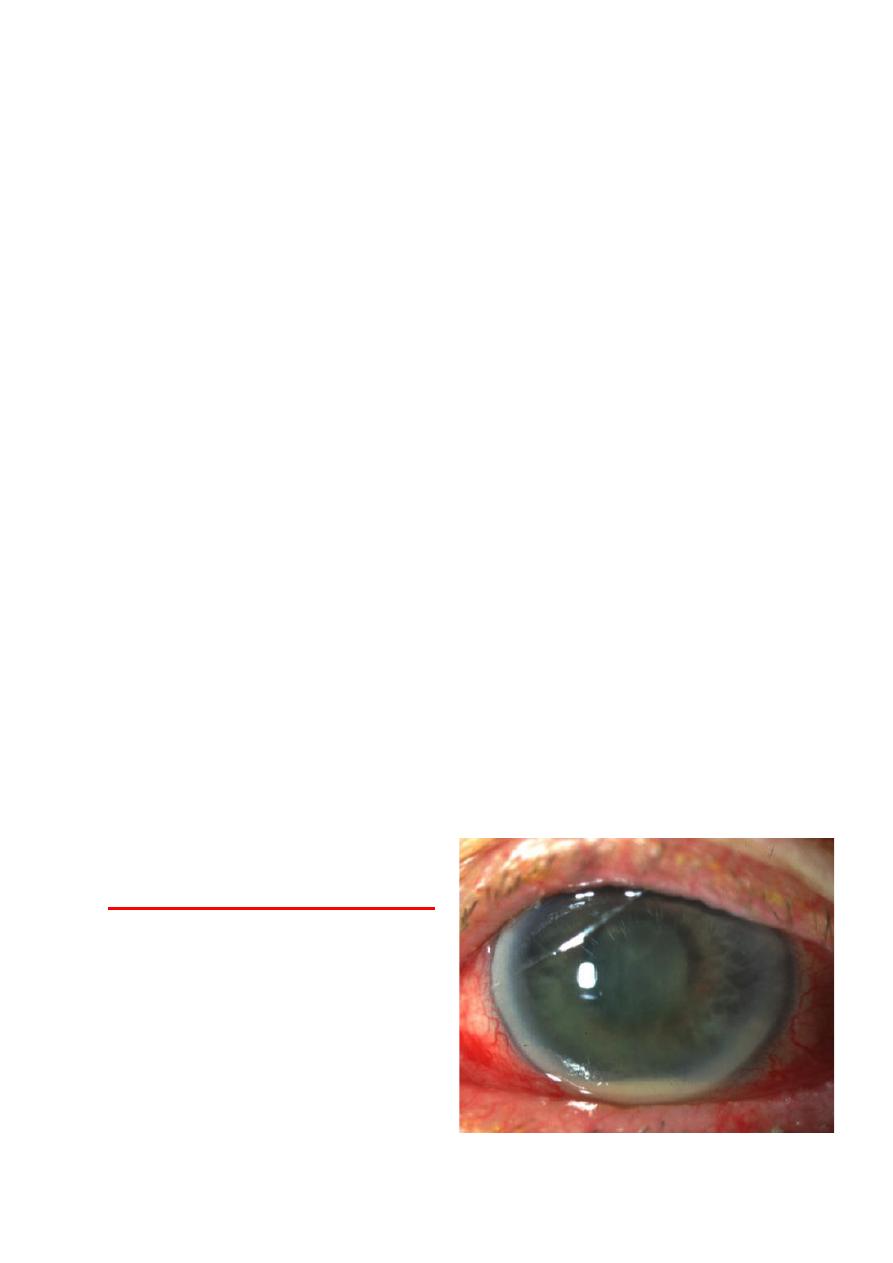
Hypermature:
• Which is characterized by
shrunken and wrinkled
anterior capsule.
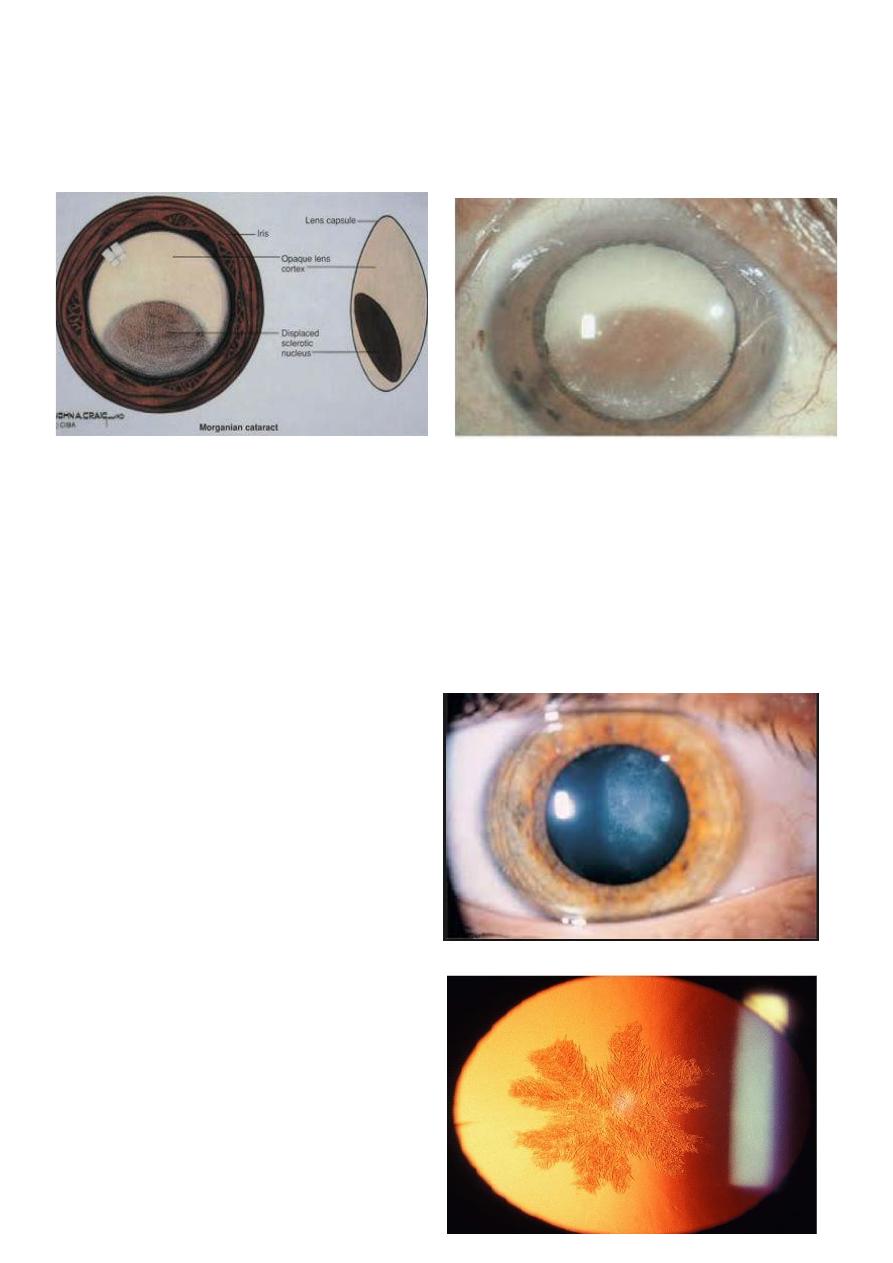
5
Morgagnian:
Is a Hypermature cataract in which the
nucleus has sunk inferiorly.
Causes and management:
Causes of presenile cataract:
1 systemic diseases.
2 systemic drugs.
3 Secondary (complicated) cataract.
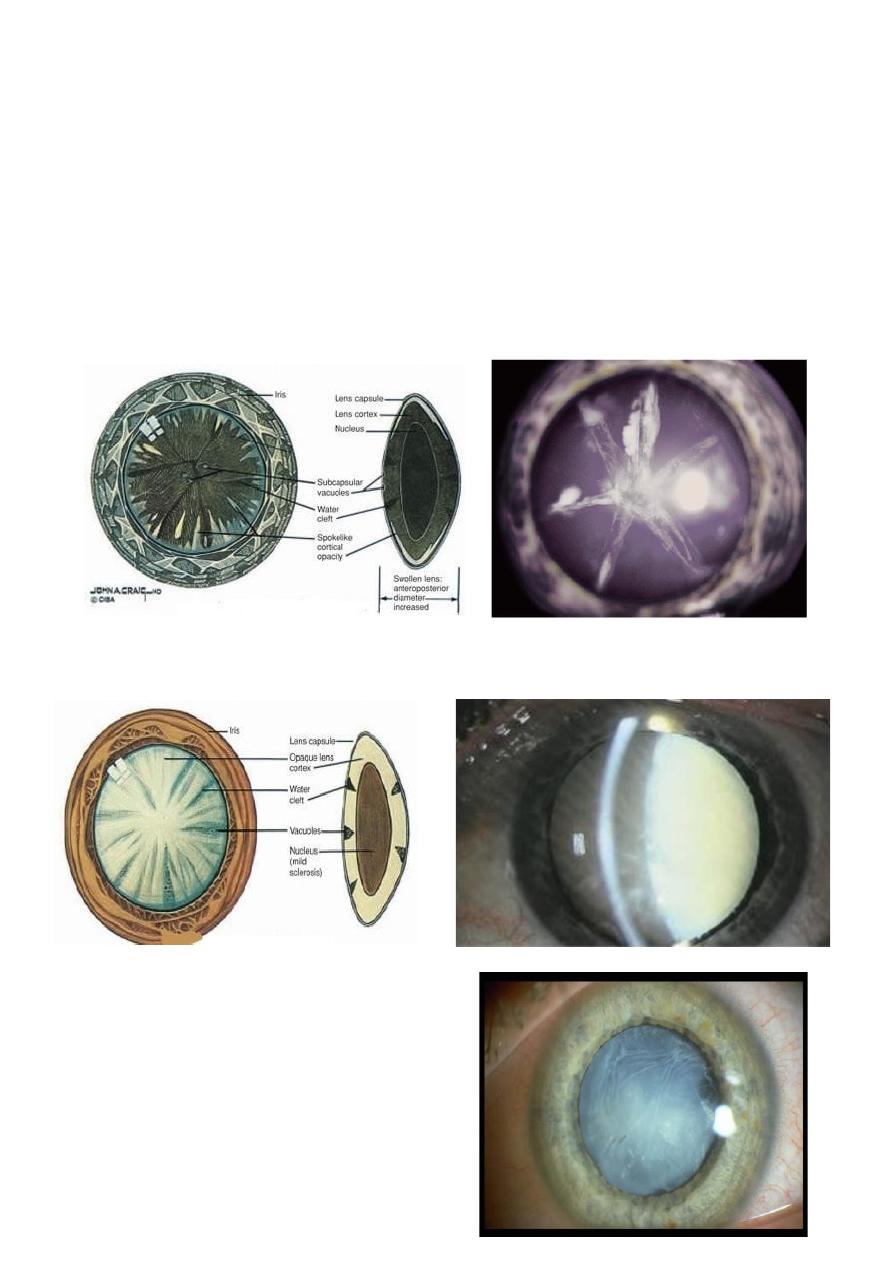
Systemic diseases:
1-Diabetes mellitus
• Classic diabetic cataract is
characterized by snowflake
cortical opacities in young
diabetic.
2- Myotonic dystrophy
• Stellate posterior
subcapsular cataract.
6
Steroids: initially posterior
subcapsular and later the anterior
subcapsular opacities.
Chlorpromazine and amidarone:
stellate, yellowish brown granules on
anterior lens capsule within the pupillary
area.
3- Atopic dermatitis
• Dense, shield-like anterior
subcapsular plaque with
capsular wrinkling.
Systemic drugs:
Secondary (complicated) cataract:
1 Chronic anterior uveitis.
2 Acute congestive angle-closure glaucoma.
3 High (pathological) myopia.
4 Trauma.
7
5 Hereditary fundus dystrophies.
Complications which occur during maturation of cortical
cataract:
1 phacomorphic glaucoma: occur due to intumescences ( swollen)
lens causing blockage of anterior chamber angle.
2 phacolytic glaucoma: (secondary open angle glaucoma) it
occurs due to blockage of trabecular meshwork by
macrophages laden with protein leak through Morgagnian
hypermature cataract.
3 phacoanaphylctic (phaco-antigenic) glaucoma. 4- lens
sublaxation.
Preoperative evaluation:
1 general physical examination to rule out D.M, HTN, COPD and
any potential source of infection e.g. septic gum and UTI.
2 visual acuity and pupillary reactions.
3 Intraocular pressure (IOP).
4 retinal examination after pupillary dilatation.
5 search for local source of infection, e.g.
conjunctivitis, blepharitis, and dacryocystitis.
Biometry:
• Measurement of IOL power:
• Axial length of eye globe.
• K- readings.
• Special formulas.
8
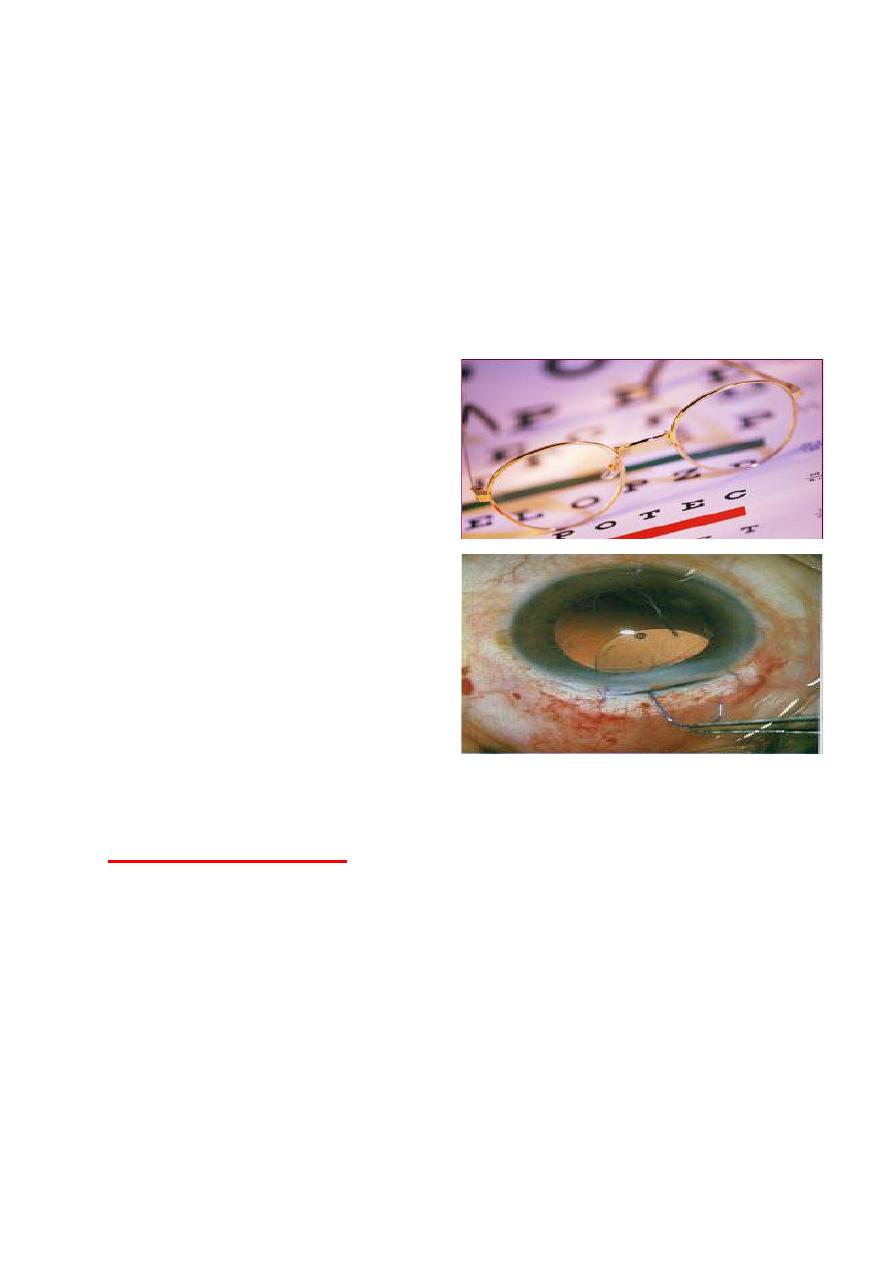
Advantages of IOL implantation over spectacles:
1 No object magnification.
2 Elimination of aberration of prismatic effect.
3 Wider and better field of vision.
4 No problem in uniocular aphakia.
5 Cosmetically more acceptable.
Indications of lens extraction:
1 Grossly diminished vision hampering easy living.
2 Medical conditions:
A. diabetic retinopathy.
B. lens induced glaucoma. C- phacoanaphylaxis.
3 Cosmetic indication: to obtain black pupil.
9
Complications of cataract surgery:
1 Intraoperative complications.
2 Early post operative complications.
3 Late post-operative complications.
Operative complications:
1 Vitreous loss.
2 Posterior loss of lens fragments.
3 Suprachoroidal (expulsive) haemorrhage.
Early postoperative complications:
1 Iris prolapse.
2 Striate keratopathy.
3 Acute bacterial endophthalmitis.
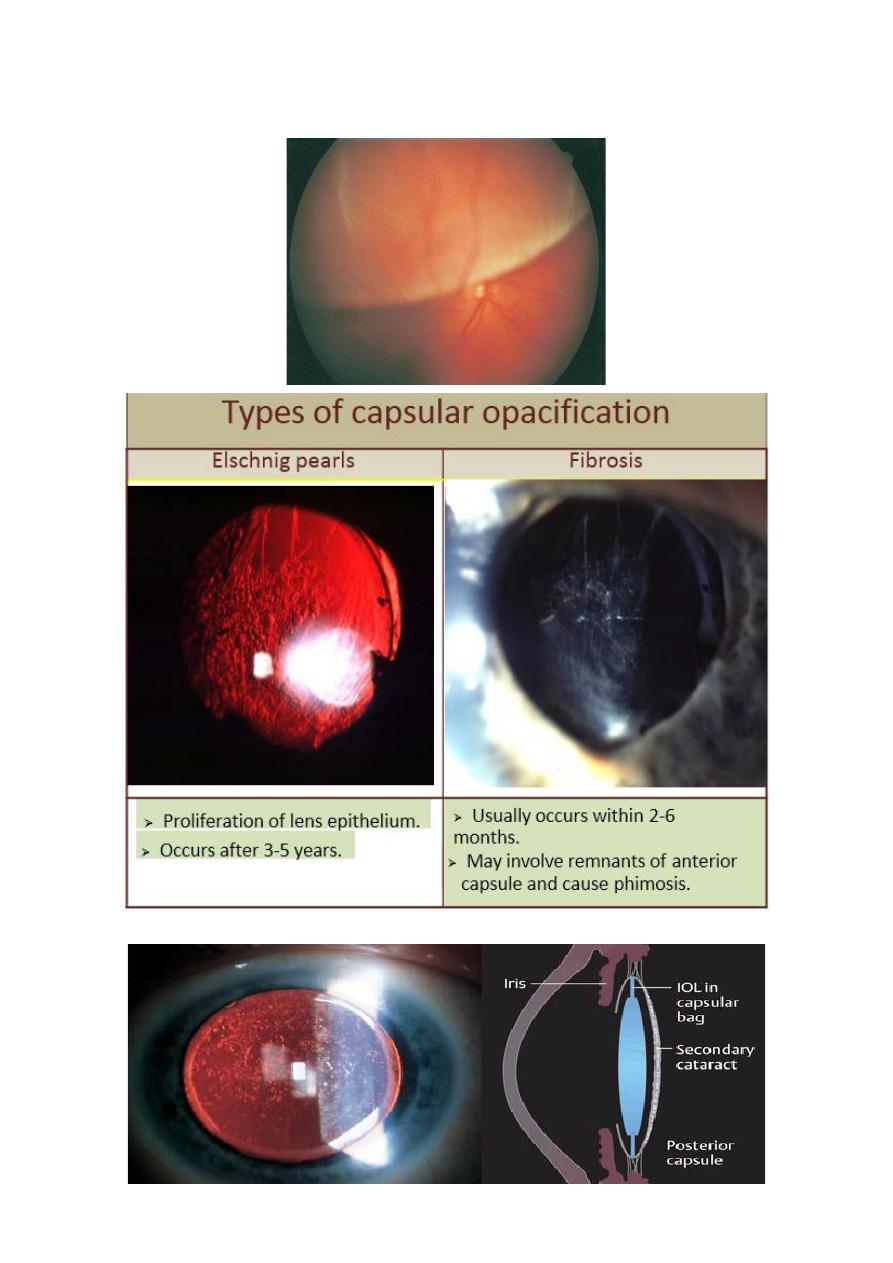
Late postoperative complications:
1 Capsular opacification.
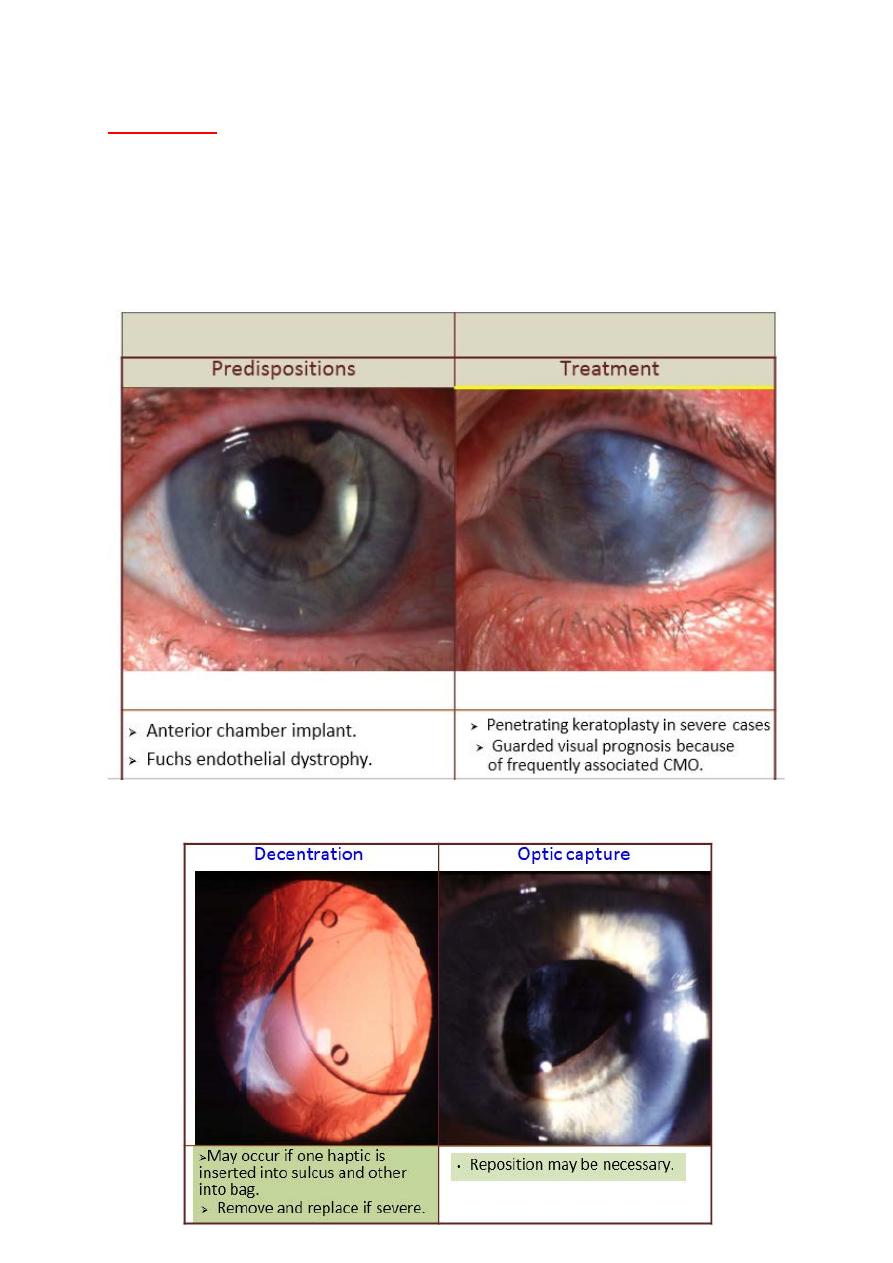
2 Implant displacement.
3 Corneal decompensation.
4 Retinal detachment.
5 Chronic bacterial endophthalmitis.
Acute bacterial endophthalmitis:
Incidence - about 1:1,000
Common causative Organisms:
• Staph. epidermidis
• Staph. aureus
• Pseudomonas sp.
10
Source of infection:
• Patient’s own external bacterial flora is most frequent culprit.
• Contaminated solutions and instruments.
• Environmental flora including that of surgeon and operating
room personnel.
Preoperative prophylaxis
Meticulous prepping and draping
Instillation of povidone-iodine
Postoperative injection of Antibiotics.
Sampling and injections:
Striate keratopathy:
Corneal edema and folds in
Descemets membrane.
Cause
• Damage to endothelium during
surgery.
Make partial-thickness
sclerotomy 3 mm behind
limbus
Insert mini vitrector.
11
Treatment
• Most cases resolve within a few days.
• Occasionally persistent cases may
require penetrating keratoplasty.
Corneal decompensation:
Implant displacement
12
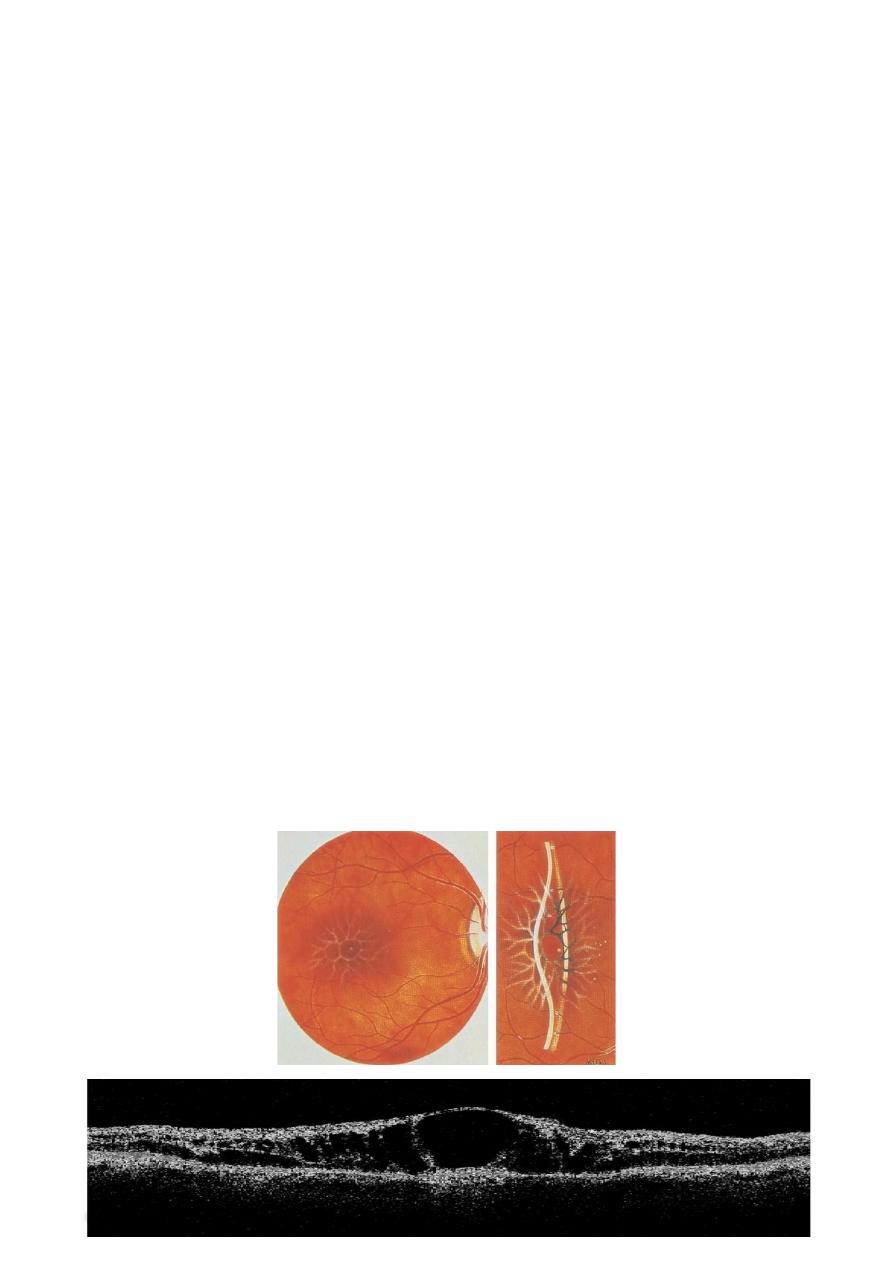
Cystoid macular edema (CME):
• Fluid accumulation in outer Plexiform and inner nuclear layers
of retina with formation of cyst like changes.
Signs:
• Loss of foveal depression, thickening of the retina and multiple
Cystoid areas in the sensory retina.
• Amsler chart testing demonstrates central blurring and
distortion.
• Fluorescein angiography shows early hyperfluorescent spots due
to leakage that progress to a characteristic petaloid pattern
• OCT shows cyst like hyporeflective spaces within the retina.
Causes:
• 1- Ocular surgery and laser
• 2- Retinal vascular disease (diabetic retinopathy, retinal vein
occlusion and hypertensive retinopathy).
• 3- Inflammation: intermediate uveitis, scleritis and
toxoplasmosis.
• 4-choroidal neovascular membrane (CNV).
• 5- Systemic disease (multiple myeloma and leukemia).
13
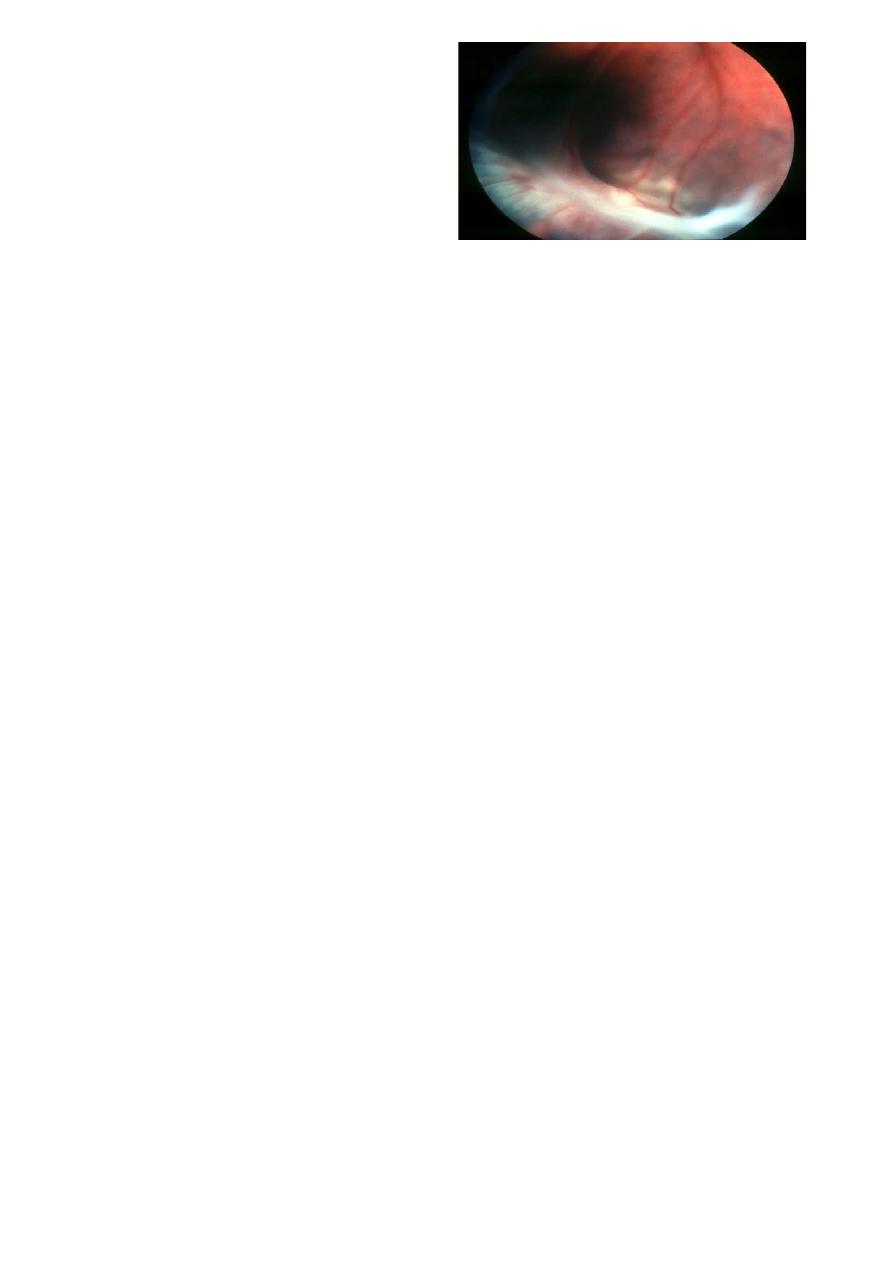
Retinal detachment (RD)
14
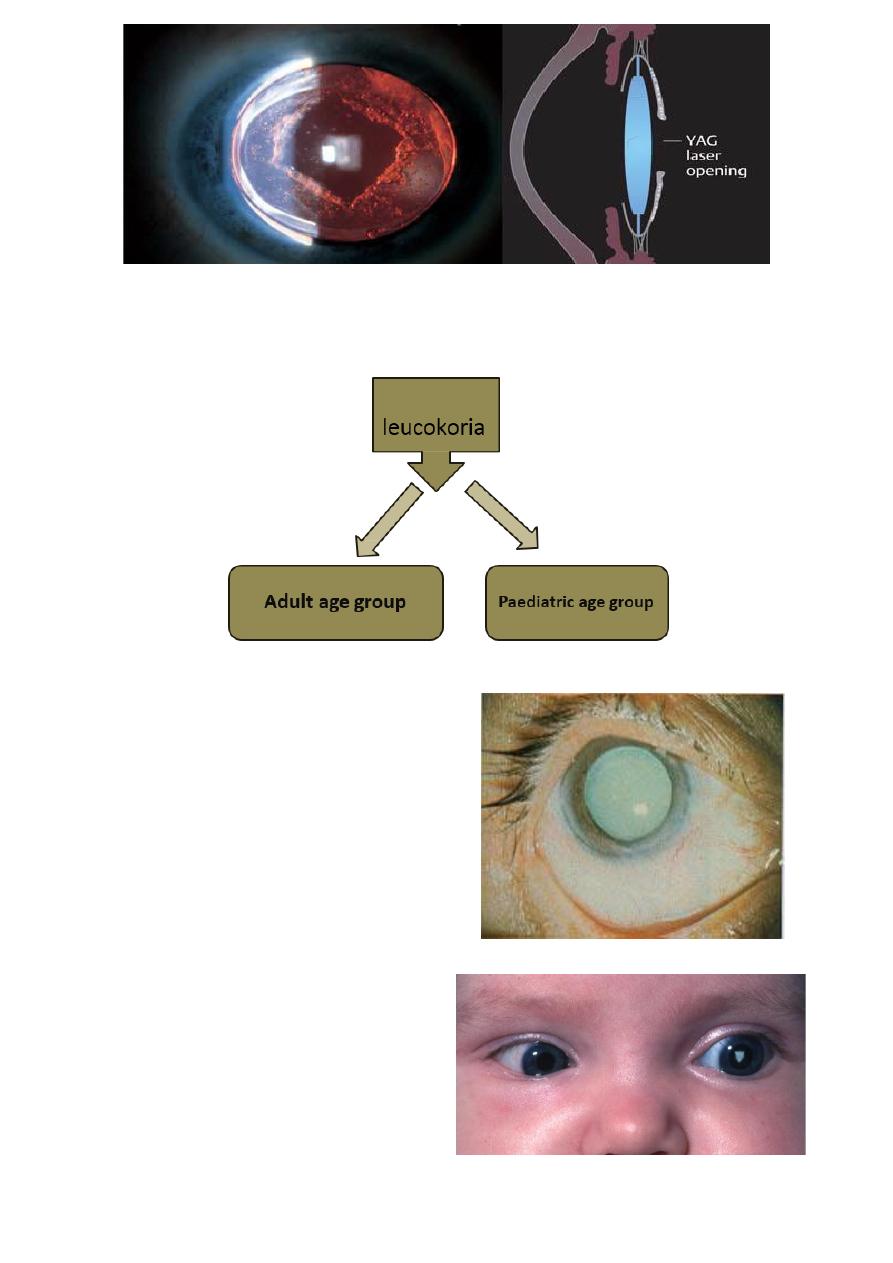
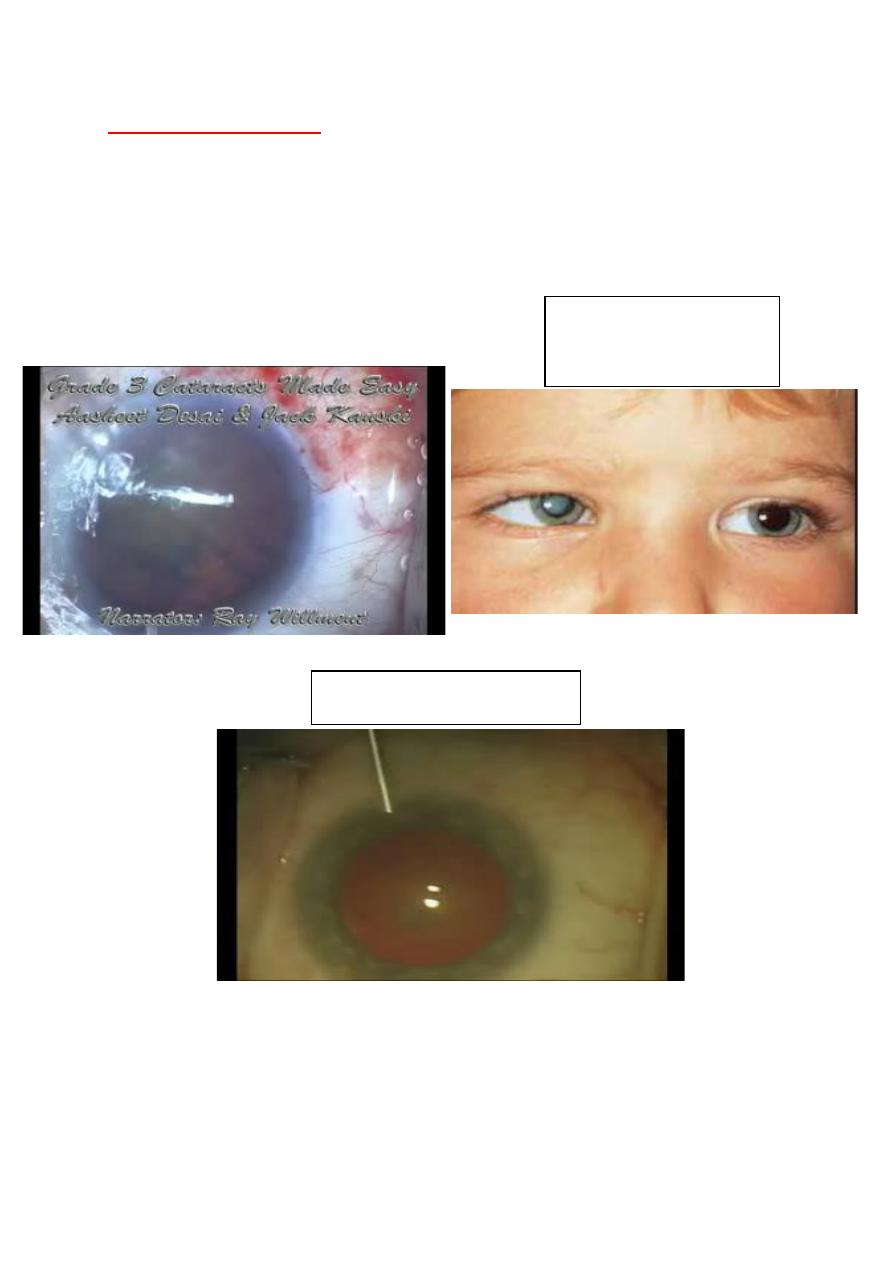
Leucokoria:
Leucokoria white pupillary light reflex
Leucokoria:
Adult age group:
• Mature cataract
Paediatric age group:
1 Congenital cataract.
2 Retinoblastoma.
15
3 Retinopathy of prematurity
(ROP).
Causes:
1- Congenital cataract (most common)
2- Retinoblastoma (most dangerous)
3- Retinopathy of prematurity (most tragedic)
4- Toxocariasis
5-Coats disease.
6- Incontinenta pigmenta.
7- Extensive myelinated nerve fibre layer of retina.
8- Chorioretinal coloboma.
9- Persistent primary hypoplastic vitreous (PHPV).
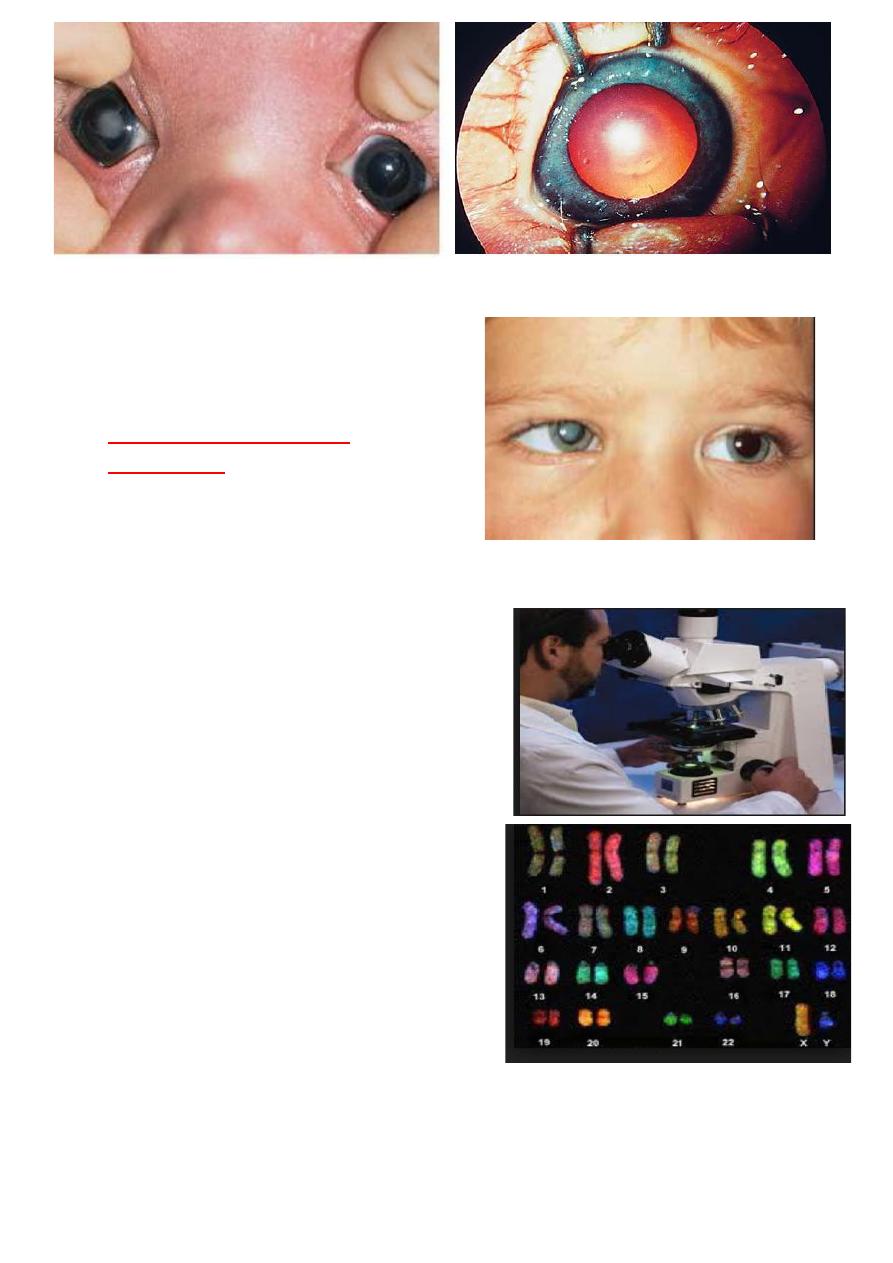
Congenital cataract:
Congenital cataract occur in about 3 in 10 000 live births. Two third
of cases are bilateral. The most common cause is genetic mutation,
other causes include:
Chromosomal abnormalities (Down syndrome, Edward syndrome, Cri
du chat syndrome).
Metabolic disorders (Galactosaemia, Lowe syndrome, Fabry disease,
hypo- and hyperglycaemia).
Intrauterine infections (congenital rubella, toxoplasmosis,
cytomegalovirus, varicella).
Unilateral cataracts are usually sporadic, without a family history or
systemic disease and affected infants are usually full-term and
healthy.
16
1-Management:
• 1- ocular exam(density,
morphology, associated ocular
pathology).
Indicators of sever visual
impairment:
Absence of central fixation.
Nystagmus.
Strabismus.
2- Systemic investigations:
1 Serology for intrauterine infection.
2 Urinalysis for reducing substances
after drinking milk (galactosemia
) and chromatography for amino acids
(Lowe syndrome)
3 Other investigations.
Fasting blood glucose, serum
calcium and galactokinase level.
4 Referral to paediatrician for
dysmorphic features or suspicion
of systemic
disease(chromosomal analysis).

17
3- Treatment:
• Unilateral dense cataract merits
urgent surgery followed by
aggressive anti-amblyopia
therapy.
• Bilateral dense cataract require
early surgery to prevent
deprivation amblyopia.
4- Visual rehabilitation:
A. spectacles.
B. contact lenses.
C. IOL implantation.
D. occlusion to treat or prevent amblyopia.
18
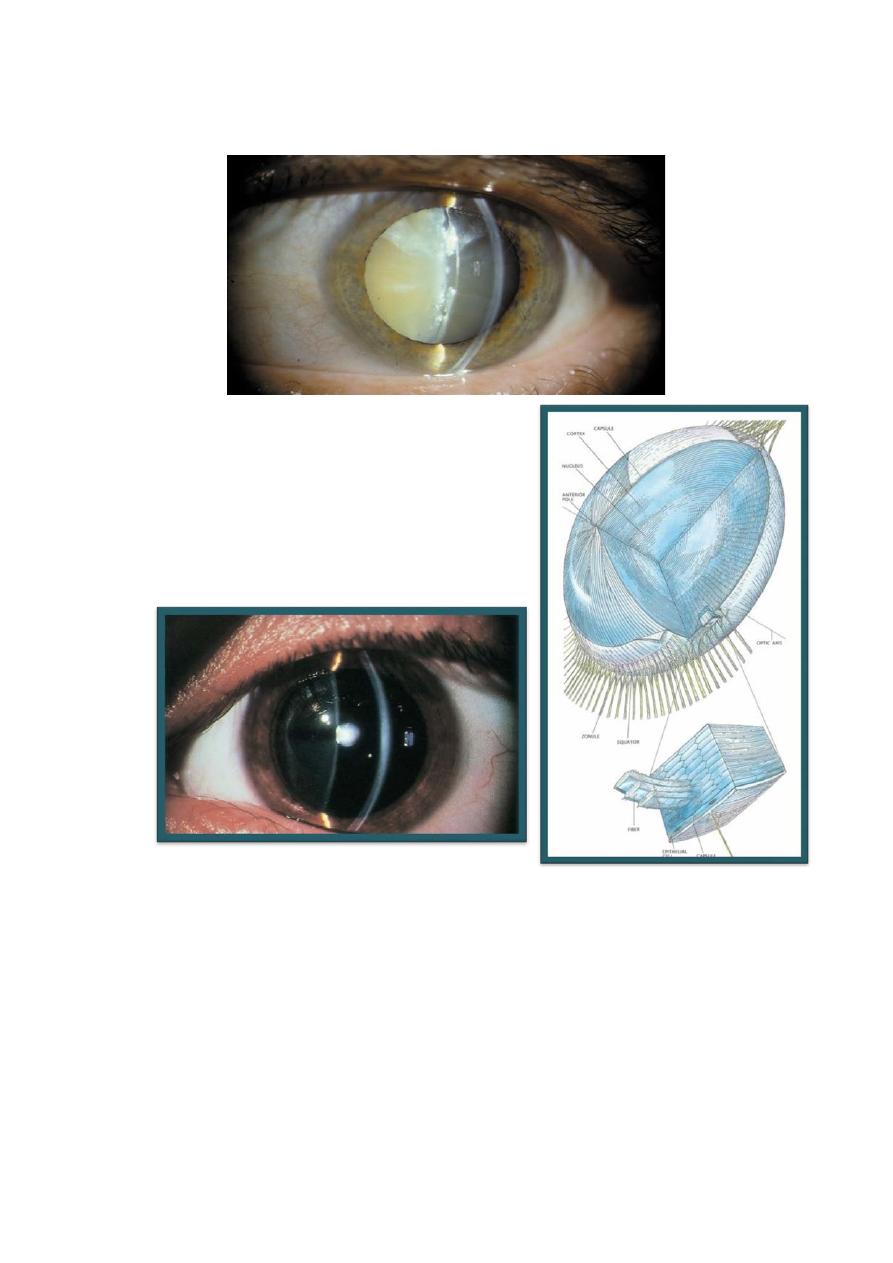
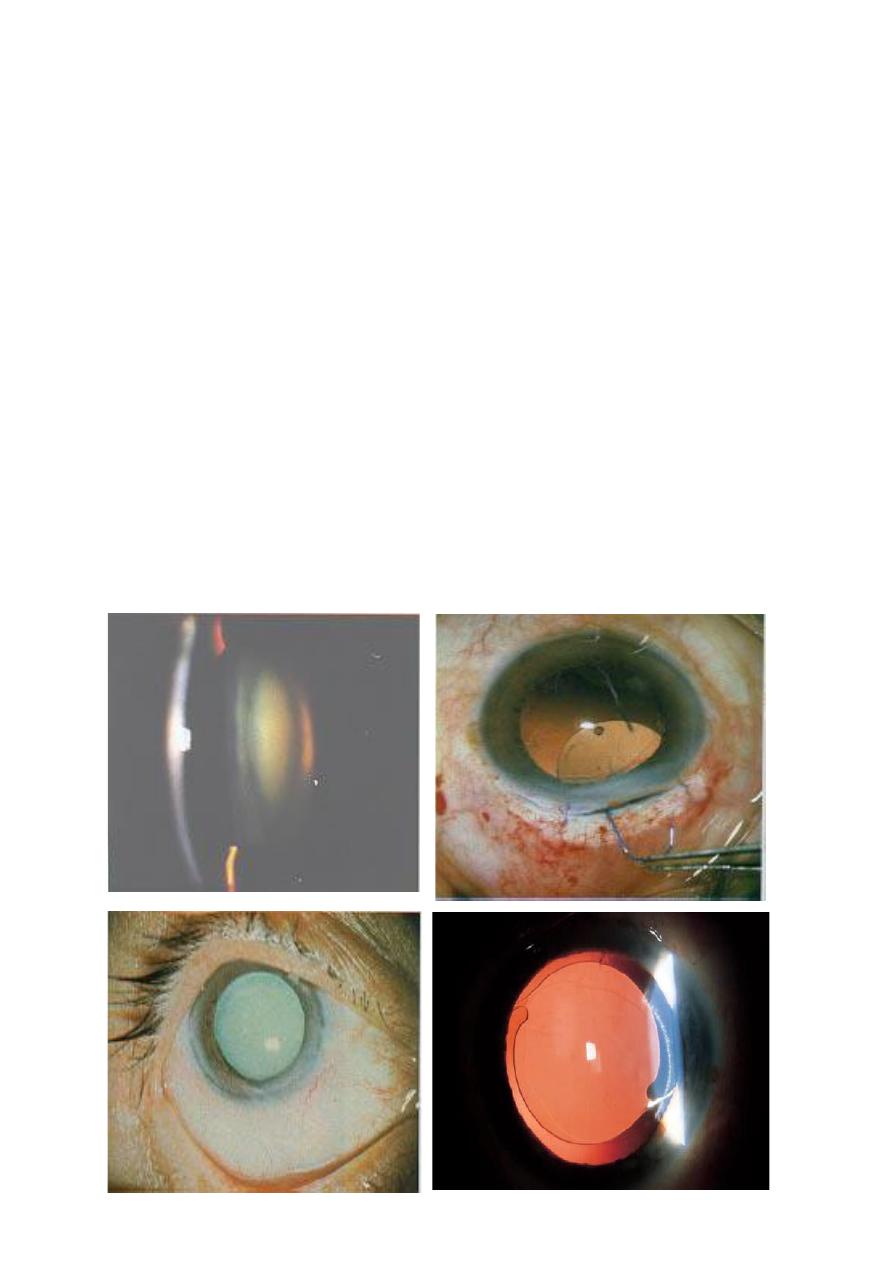
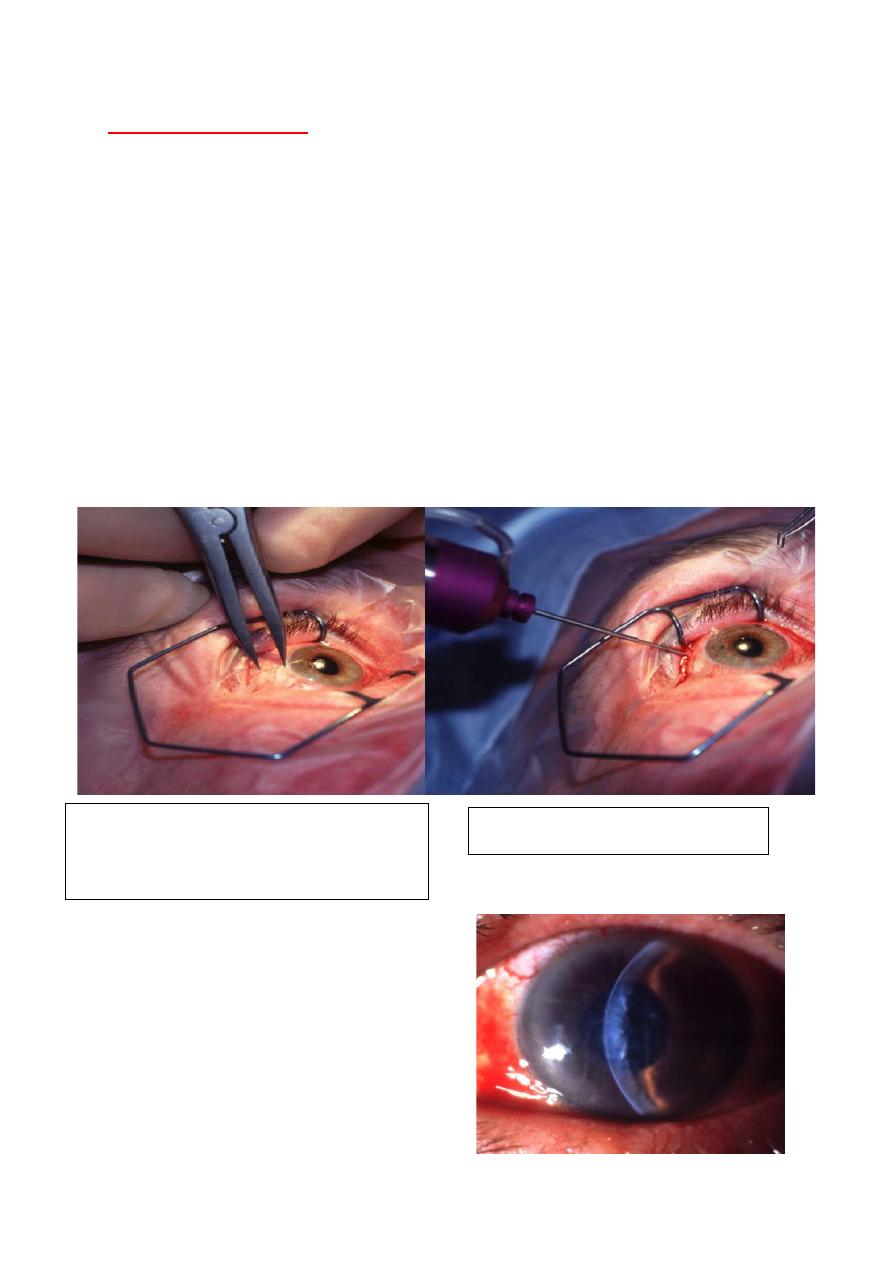
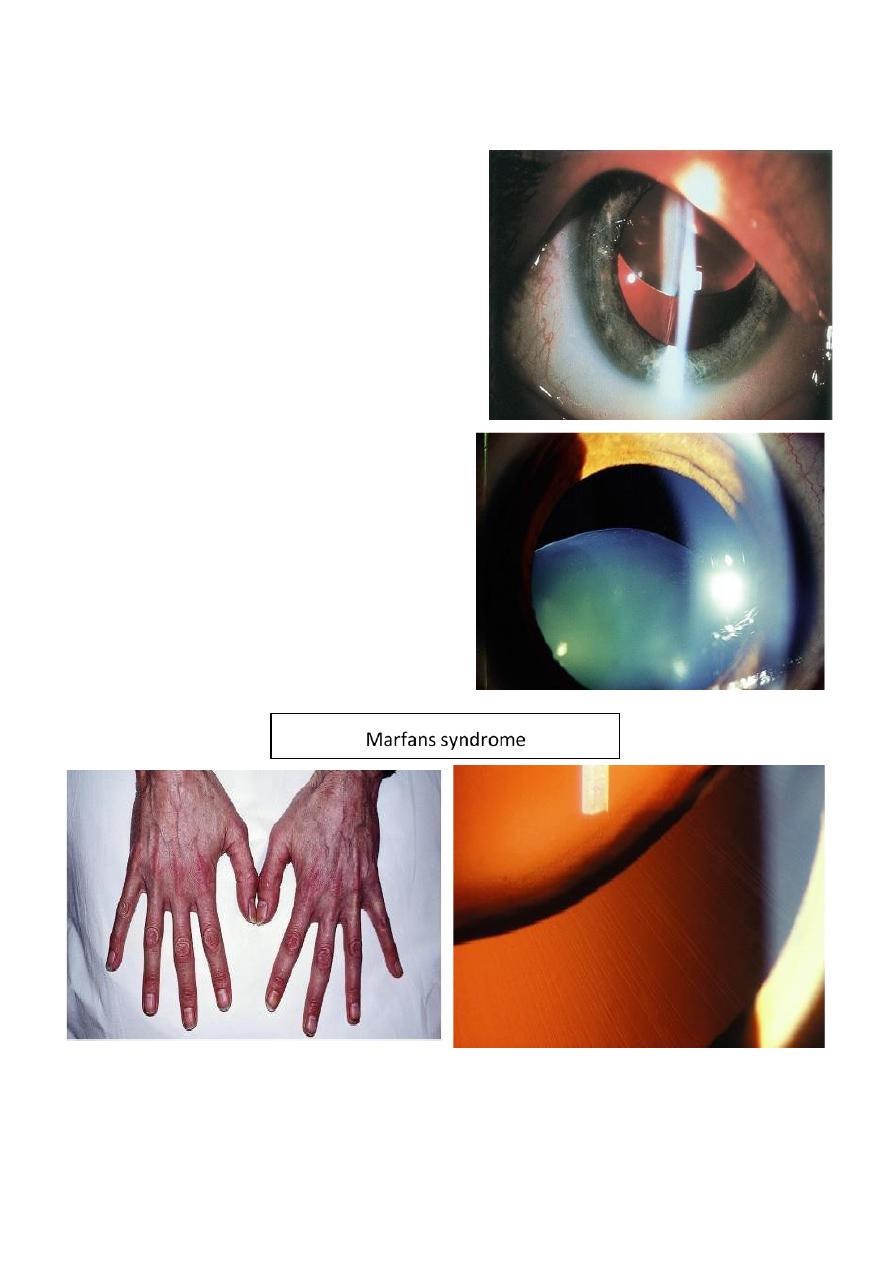
Ectopia lentis:
Acquired causes:
• 1- Trauma.
• 2-large eye.
high myopia.
Buphthalmos.
• 3- Anterior uveal tumour.
• 4- Hypermature cataract.
Hereditary causes:
1 familial ectopia lentis.
2 Ectopia lentis et pupillae.
3 Marfans syndrome.
4 Homocystinuria.
5 Aniridia.
19
Complications:
1 refractive errors (myopia and hypermetropia).
2 optical distortion due to astigmatism and/or lens edge effect.
3 lens induced glaucoma.
4 cataract.
5 endothelial damage.
Management:
• Spectacle correction for
astigmatism or aphakic correction.
• Surgical removal for cataract,
lens induced glaucoma or
endothelial touch.
Causes of cataract in unwell neonate:
Intrauterine infections:
• Rubella.
• Toxoplasmosis.
• Cytomegalovirus.
• Varicella.
20
Metabolic disorders:
• Galactosaemia.
• Hypoglycaemia.
• Hypocalcaemia.
• Lowe syndrome.
Post test:
Diagnosis: leucokoria
Video: cataract surgery