Lacrimal system
DR. Hussein Al-Ani
TUCOM-Ophthalmic department
FJMC ophth ,ICO Cambridge UK,FOVR
Delhi INDIA,MBCHB

Development
• Secretory Apparatus:
The lacrimal gland develops from multiple
solid ectodermal buds in the anterior supero lateral orbit The lacrimal glands
are small and do not function fully until approximately 6 weeks after birth.
This explains why newborn infants do not produce tears when crying.
• Excretory Apparatus:
By the end of the fifth gestational week, the
nasolacrimal groove forms as a furrow lying between the nasal and
maxillary prominence. In the floor of this groove, the nasolacrimal duct
(NLD) develops from a linear thickening of the ectoderm. A solid cord
separates from adjacent ectoderm and sinks into the mesenchyme. The
cord canalizes, forming the NLD and the lacrimal sac at its cranial end. The
canaliculi are thought to form similarly from invaginated ectoderm
continuous with the distal cord.
Normal Anatomy
• Secretory Apparatus
:The main lacrimal gland is an exocrine gland
located in the superior lateral quadrant of the orbit within the lacrimal gland
fossa. Embryologic development of the lateral horn of the levator aponeurosis
indents the lacrimal gland and divides it anteriorly into orbital and palpebral
lobes, The superior transverse ligament (Whitnall ligament) inserts at the
division of the 2 lobes, with some fibers also projecting onto the lateral orbital
tubercle, Some 8- 12 major lacrimal ducts empty into the superior cul-de-sac
approximately 5 mm above the lateral tarsal border after passing posterior to
the aponeurosis, through the Muller muscle and the conjunctiva.
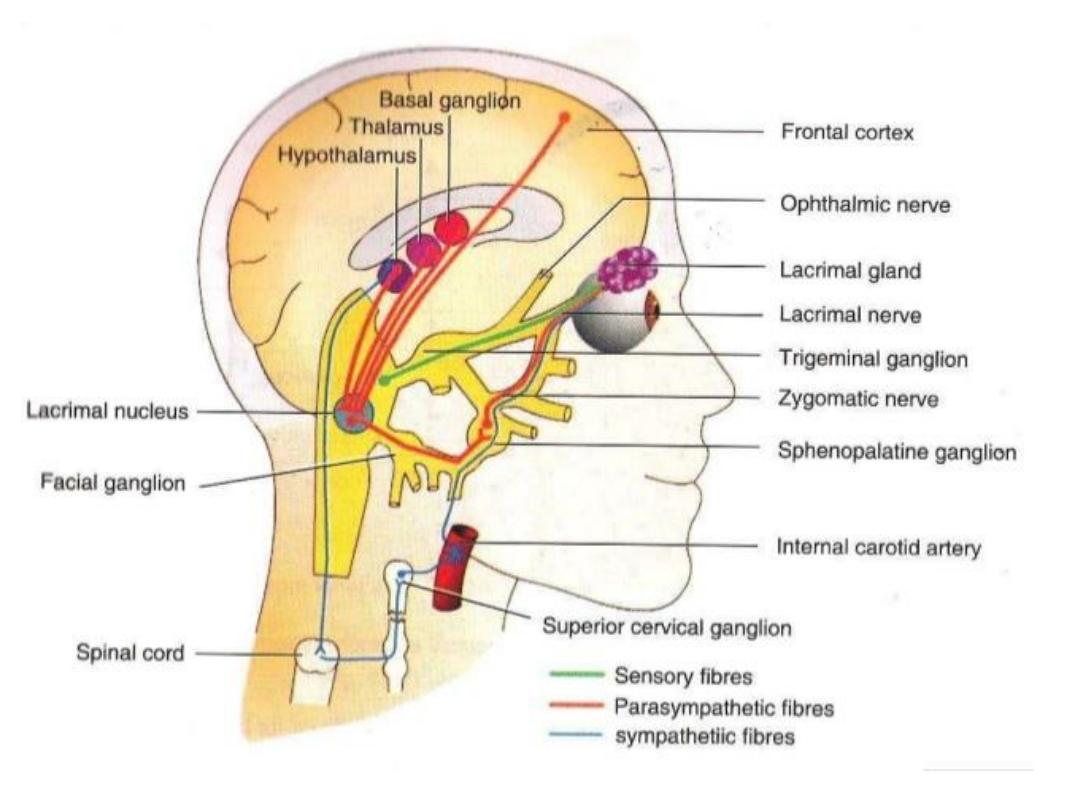
• Nerve supply
is ophthalmic division of trigeminal nerve (afferent pathway)
The( efferent pathway) Parasympathetic fibers, originating in the superior salivary
nucleus of the pons, exit the brain stem with the facial nerve, cranial nerve VII (CN
VII). Lacrimal fibers leave CN VII as the greater superficial petrosal nerve and pass
to the sphenopalatine ganglion. From there, they are thought to enter the
lacrimal gland via the superior branch of the zygomatic nerve, via an anastomosis
between the zygomaticotemporal nerve and the lacrimal nerve.
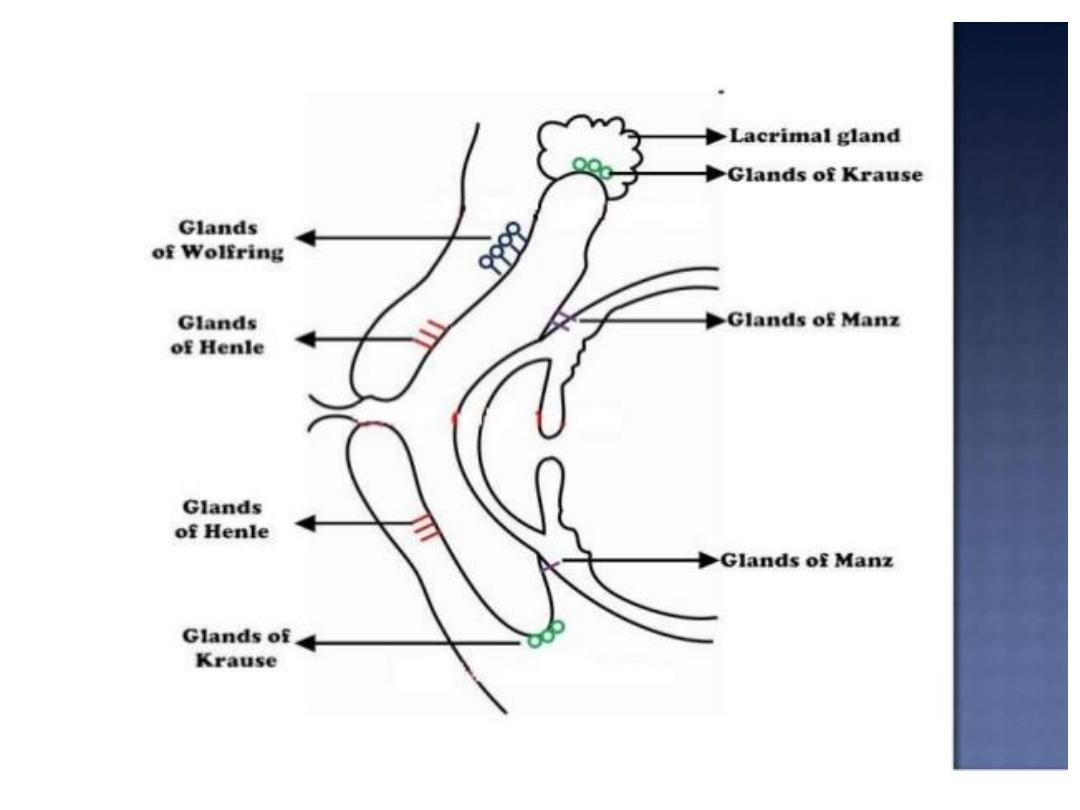
• The accessory exocrine glands of Krause and Wolfring are located deep
within the superior fornix and just above the superior border of the tarsus,
respectively.

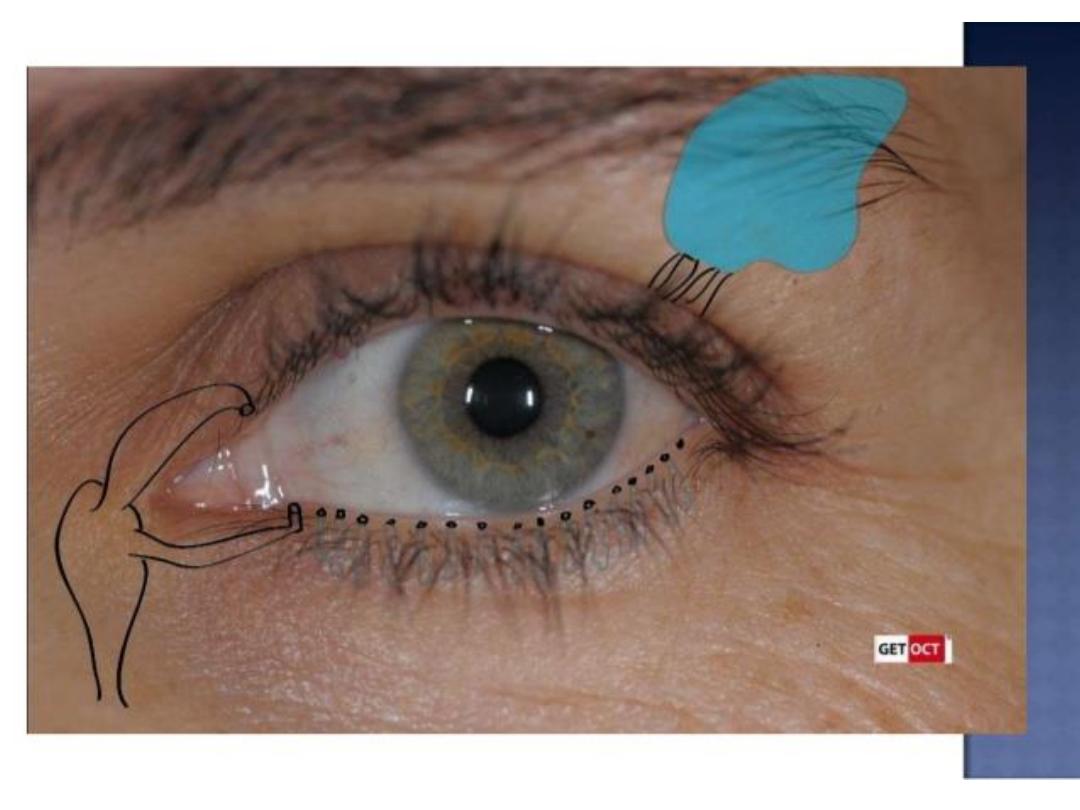
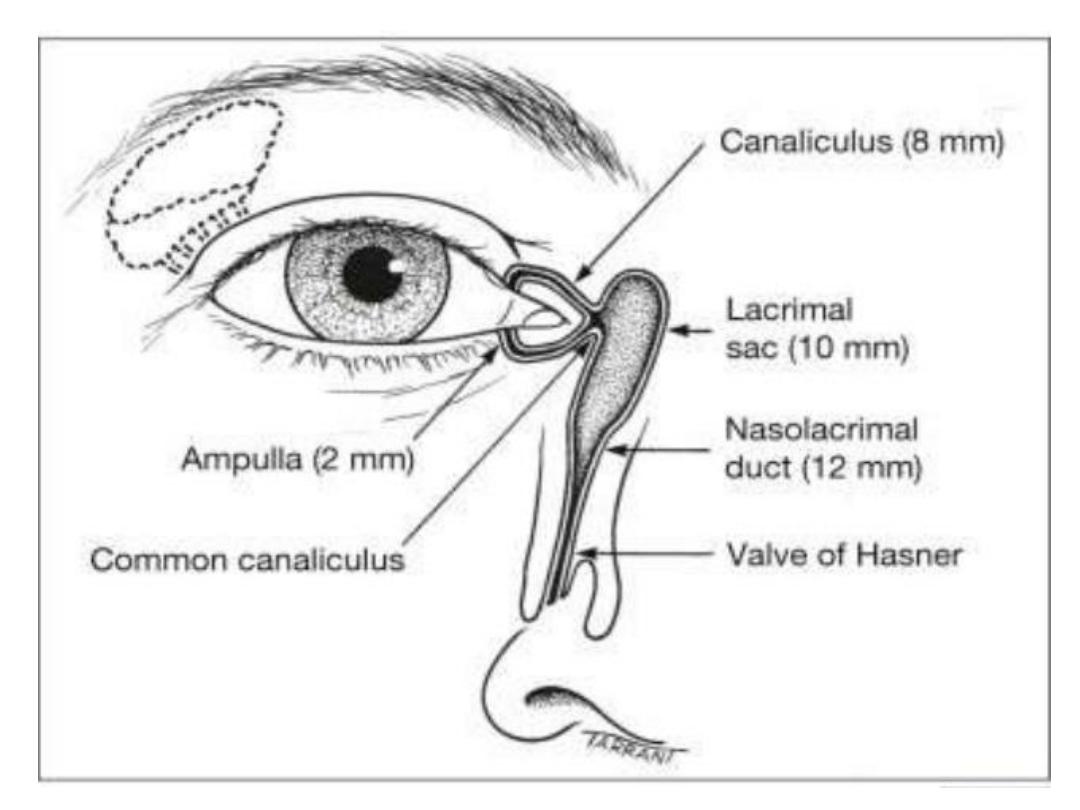
• Excretory Apparatus
:The entrance to the lacrimal drainage
system is through puncta located medially on the margin of both the
upper and the lower eyelidsEach punctum is surrounded by its respective
ampulla, fleshy elevation oriented perpendicular to the eyelid margin.Each
punctum leads to its respective canaliculus. The canaliculi are lined with
nonkeratinized, non-mucin-producing stratified squamous epithelium.
They run roughly 2 mm vertically, and then turn 90° and run 8- 10 mm
medially to connect with the lacrimal sac. In more than 90% of patients,
the canaliculi combine to form a single common canaliculus before
entering the lateral wall of the lacrimal sac. The NLD measures 12 mm or
more in length. It travels through bone within the nasolacrimal canal,
which initially curves in an inferior and slightly lateral and posterior
direction. The NLD opens into the nose through an ostium under the
inferior turbinate (the inferior meatus), which is usually partially covered
by a mucosal fold (the valve of Hasner).
Physiology
• Evaporation accounts for approximately 10% of tear elimination in the
young and for 20% or more in the elderly
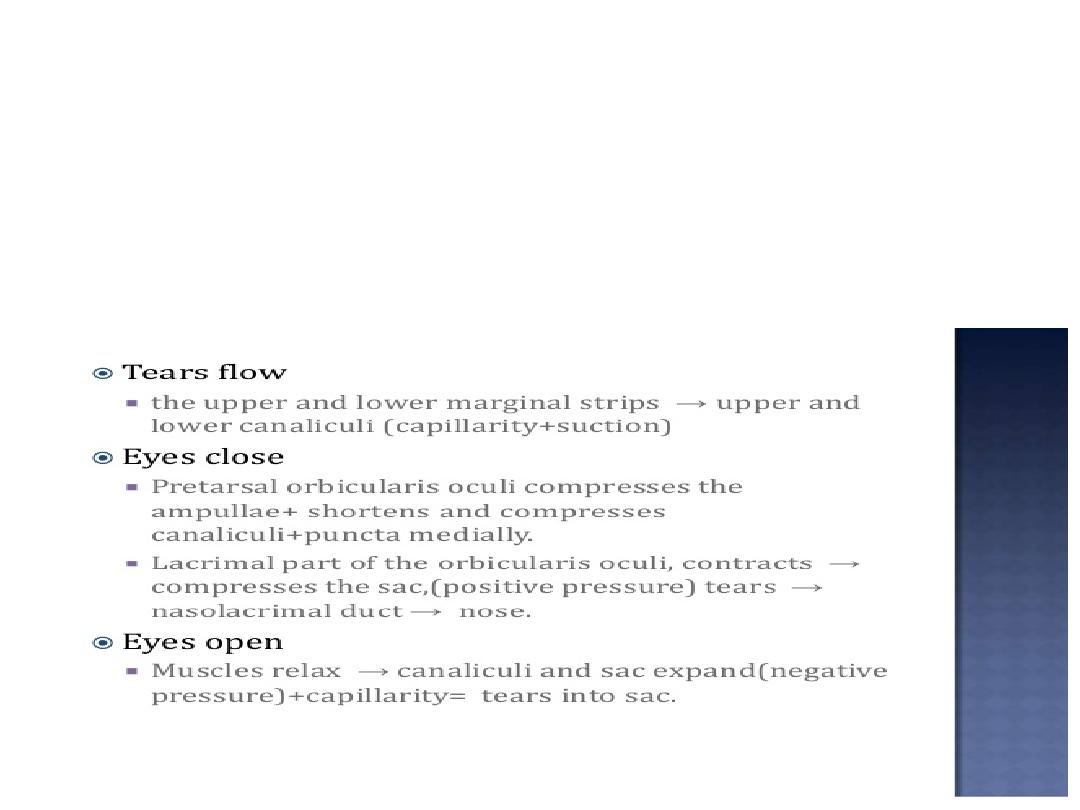
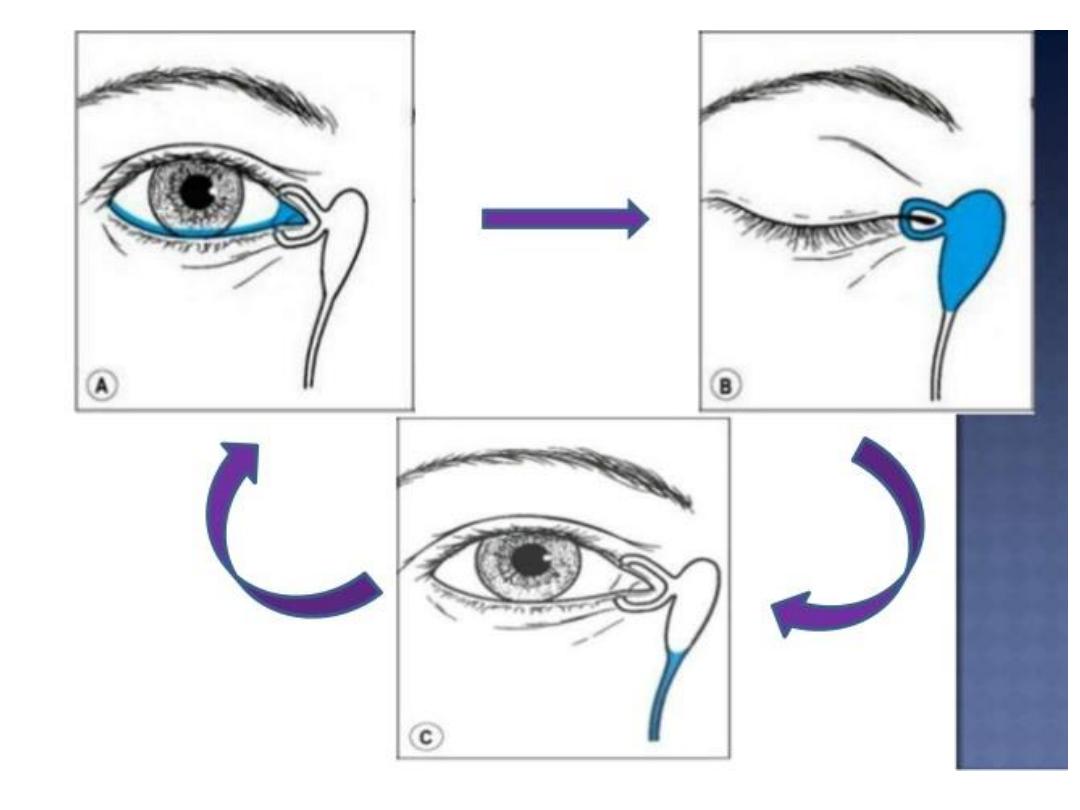
Rosengren-Doane theory:
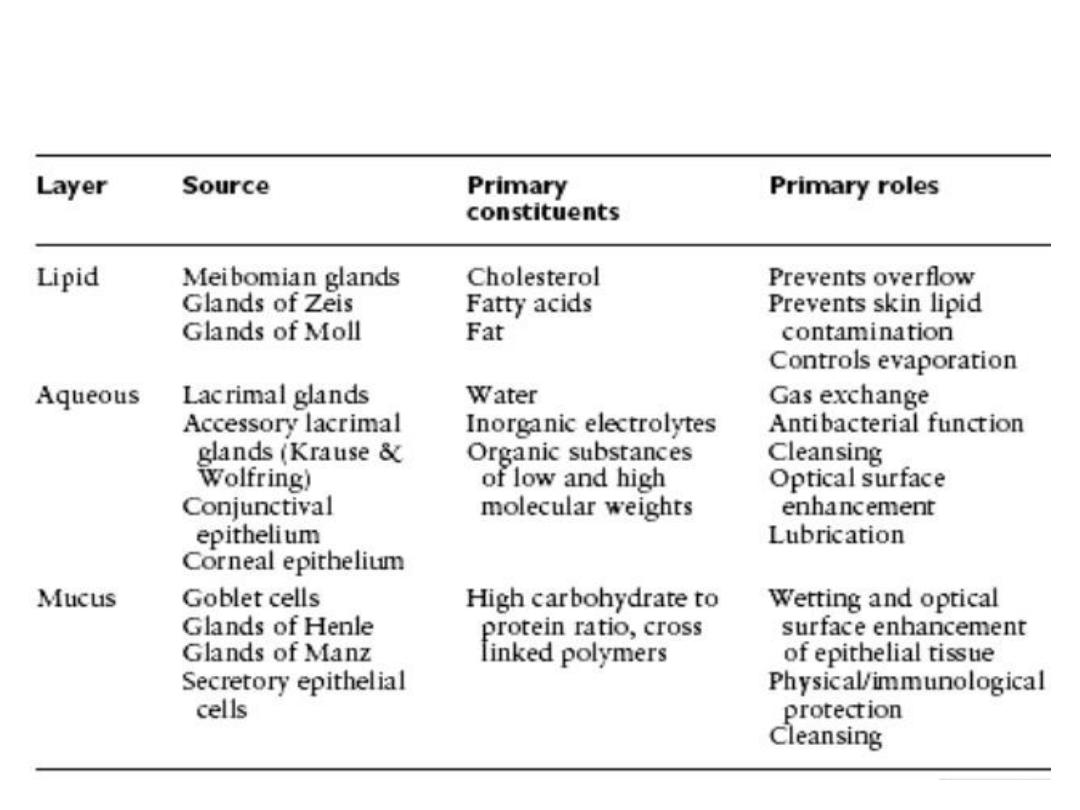
TEAR FILM

Evaluation of watering eye
• Lacrimation is watering occur secondary to
excessive tear production in presence of
normal excretory system.
• Epiphora is watering occur secondary to
abnormal excretory system in presence of
normal tear production.

Congenital Lacrimal Drainage
Obstruction
• Evaluation
:
• constant tearing with minimal mucopurulence, which
suggests an upper system block caused by punctal or
canalicular dysgenesis
• • constant tearing with frequent mucopurulence and
matting of the lashes, which suggests complete
obstruction of the NLD
• • intermittent tearing with mucopurulence, which
suggests intermittent obstruction of the NLD, most
likely the result of impaction of a swollen inferior nasal
turbinate, such as in association with an upper
respiratory tract infection.

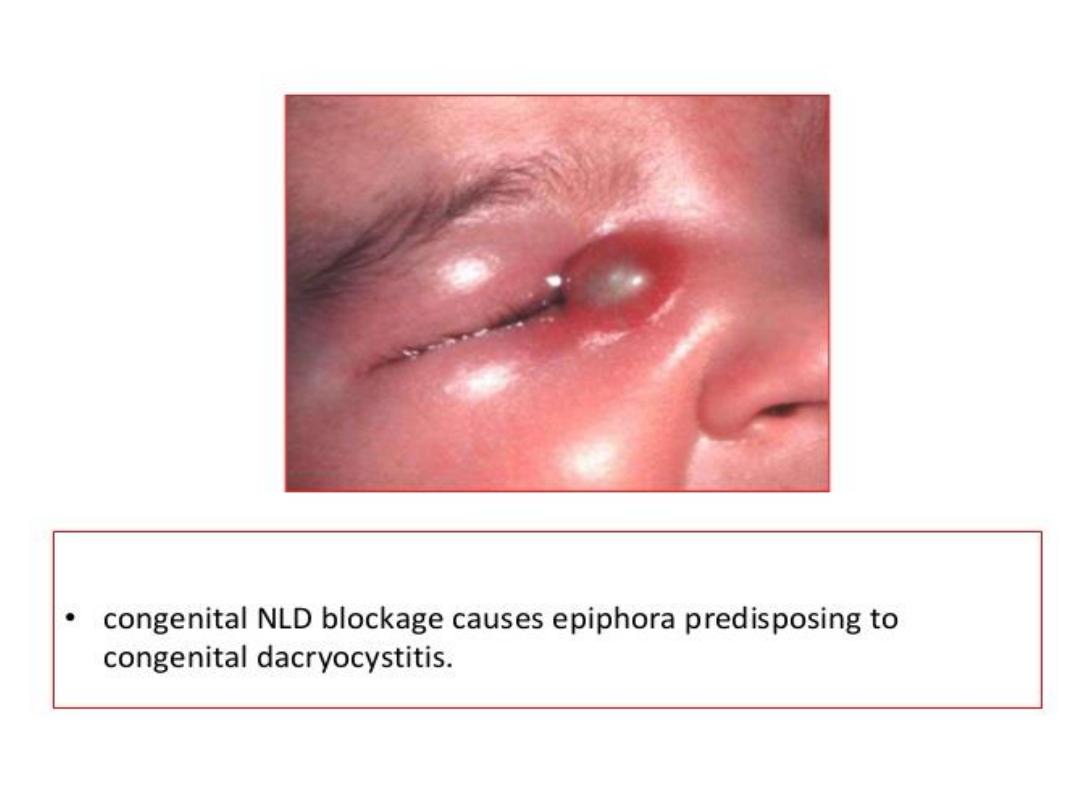
Congenital Nasolacrimal Duct
Obstruction
• Congenital obstruction of the lacrimal drainage system, which
is usually caused by a membranous blockage of the valve of
Hasner covering the nasal end of the NLD, may be present in
roughly 50% of newborn infants. Most obstructions open
spontaneously within 4- 6 weeks after birth. Such an
obstruction becomes clinically evident in only 2%- 6% of full-
term infants at 3- 4 weeks of age. Of these, one-third have
bilateral involvement. Approximately
• 90% of all symptomatic congenital NLD obstructions resolve in
the first year of life
.
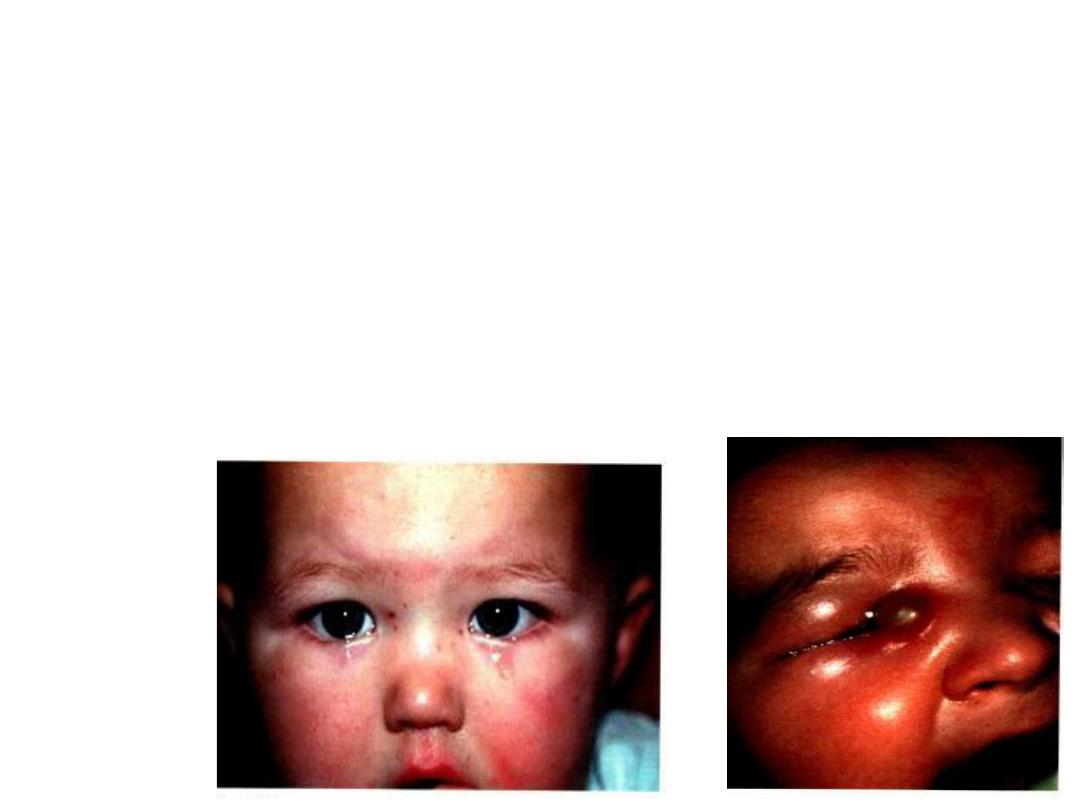
• SIGNS OF
CNLDO:
1.Epiphora and matting of lashes
2.Reflex purulent discharge from puncti
3.Acute dacryocystitis uncommon
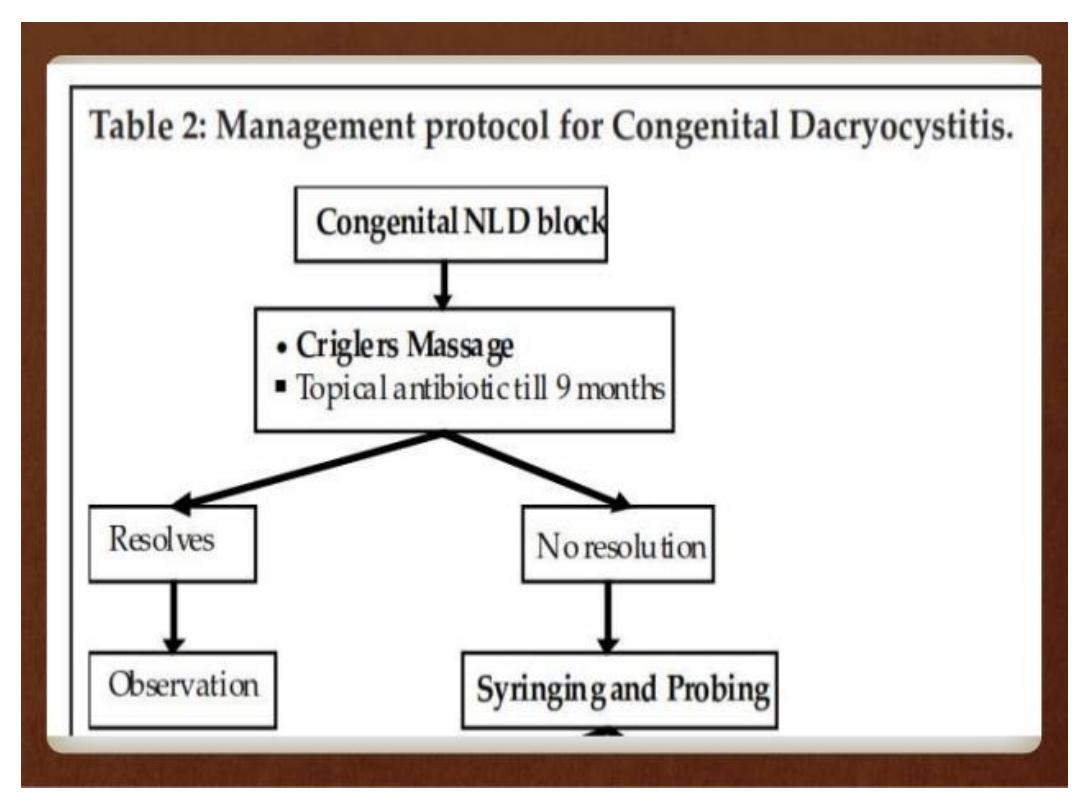
• Treatment :
• Medical treatment with lacrimal sac massage
and antibiotics
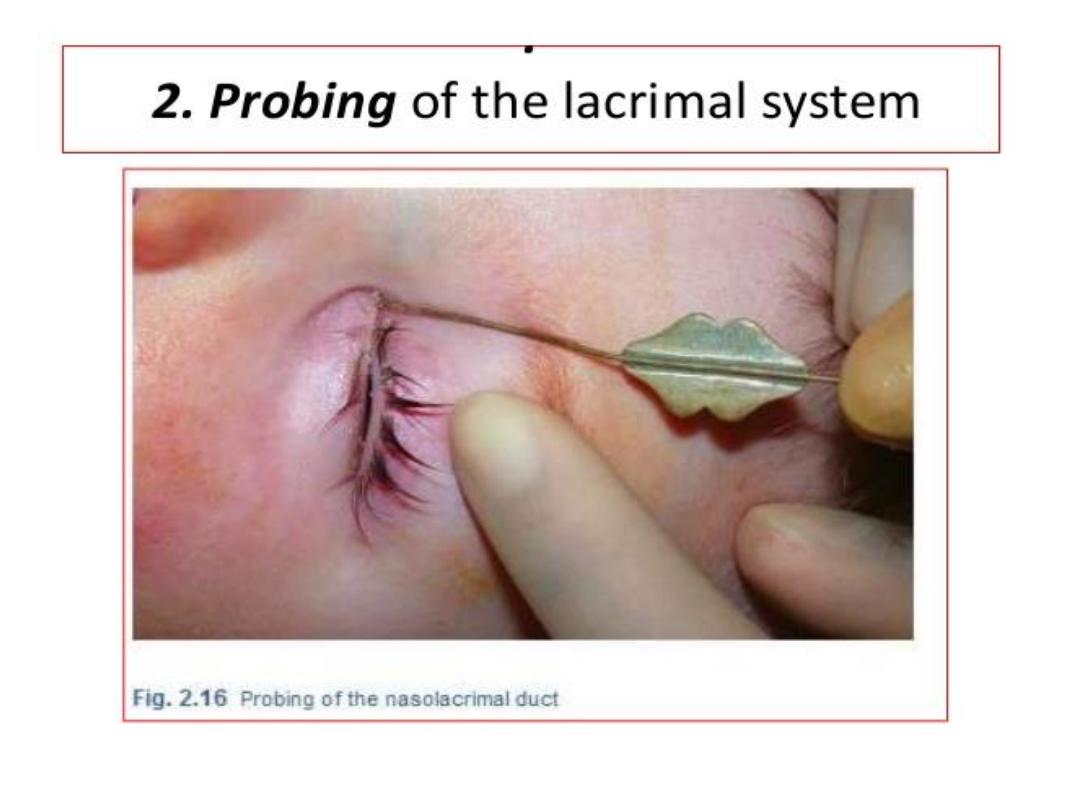

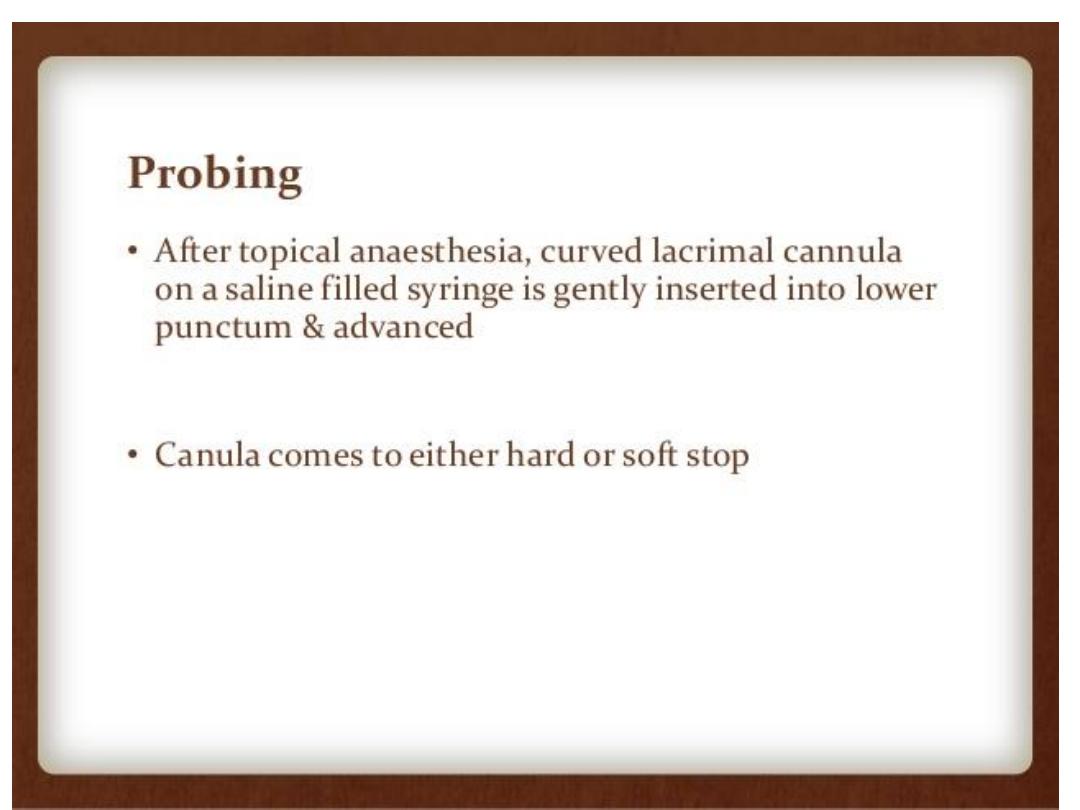
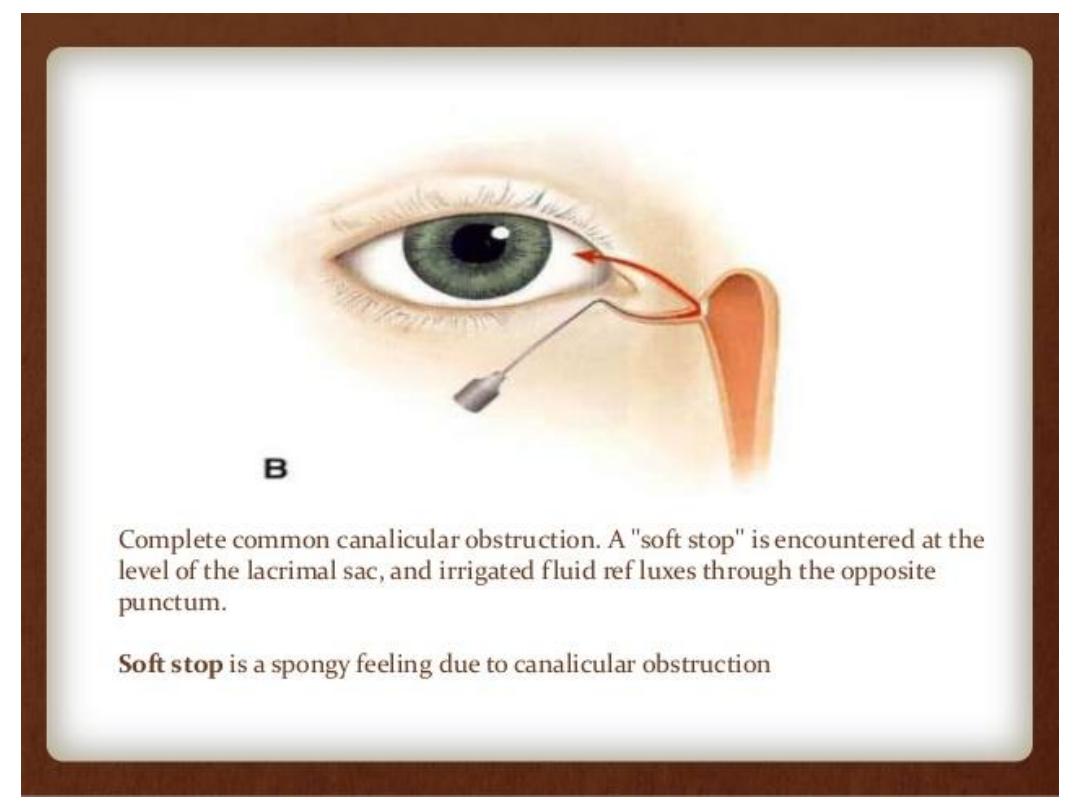
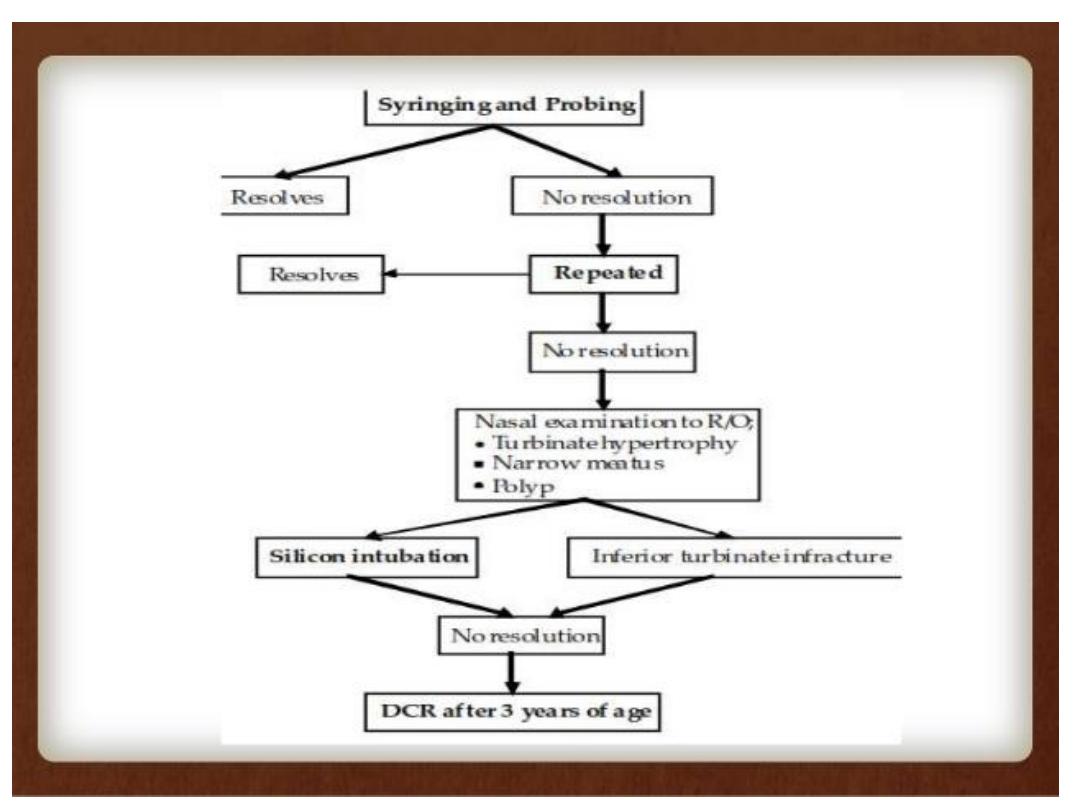
• When probing, the physician should recall that the upper
system begins at the punctum,followed first by a 2-mm
vertical segment and then by a horizontal segment of 8-10
mm (canaliculus). Punctal dilation is often needed to safely
introduce a size 0 or smaller Bowman probe. The surgeon
initially inserts the probe into the punctum perpendicular to
the eyelid margin and then advances it down the canalicular
system toward the medial canthal tendon while maintaining
lateral traction with the opposite hand. Manual lateral
traction of the eyelid straightens the canaliculus and
decreases the risk of damage to the canalicula mucosa and
creation of a false passage.
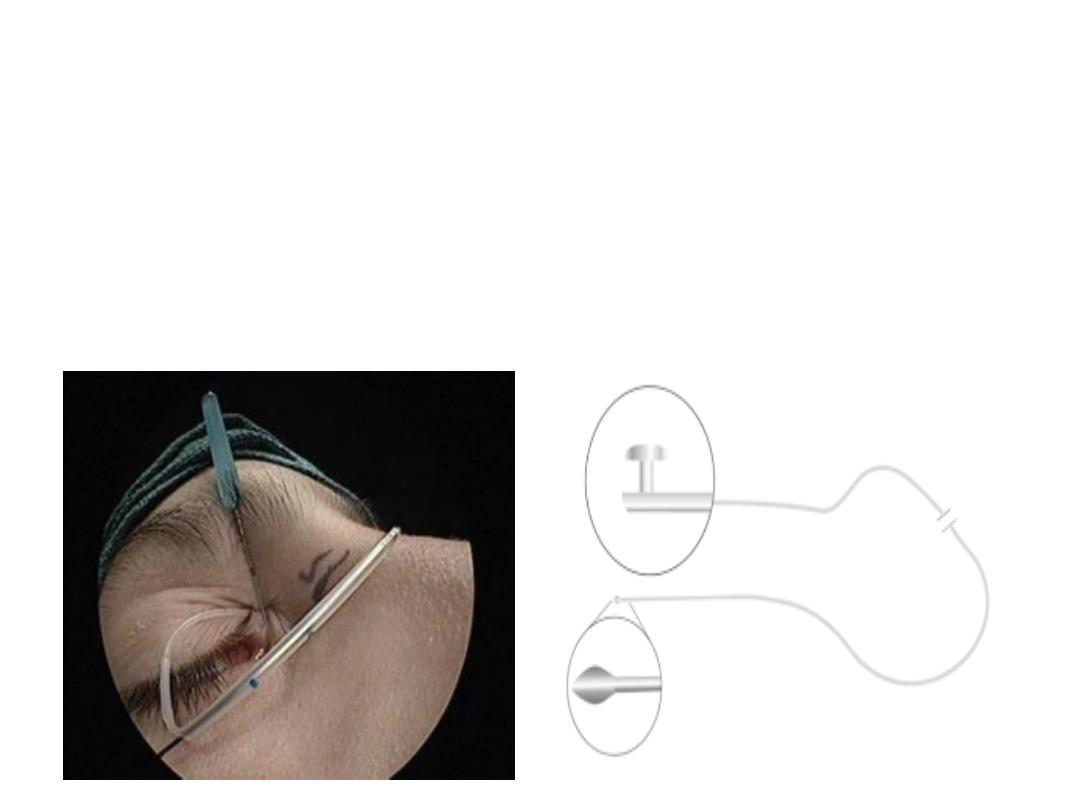
3.
Intubation
:Intubation is usually performed with a silicone stent and is
indicated for children who have recurrent epiphora following nasolacrimal
system probing or for older children when initial probing reveals significant
stenosis or scarring.

4.Balloon dacryoplasty:
A collapsed balloon catheter
is placed in a manner similar to probing and inflated
inside the duct at multiple levels, balloon dacryoplasty
is now generally limited to complicated cases or to
recurrence following standard probing techniques

5.Turbinate infracture :
If the inferior turbinate seems to be
impacted on the NLD at the time of probing and irrigation,medial in
fracturing of the inferior turbinate should be performed. This condition
should be suspected in patients whose symptoms appear primarily
related to upper respiratory tract infections, when swelling of the
mucosa over the turbinate may cause intermittent obstruction of the
inferior meatu
S
6. Dacryocystorhinostomy:
Dacryocystorhinostomy (DCR) is
usually reserved for children who have persistent epiphora following
intubation and balloon dacryoplasty and for patients with extensive
developmental abnormalities of the nasolacrimal drainage system that
prevent probing and intubation.
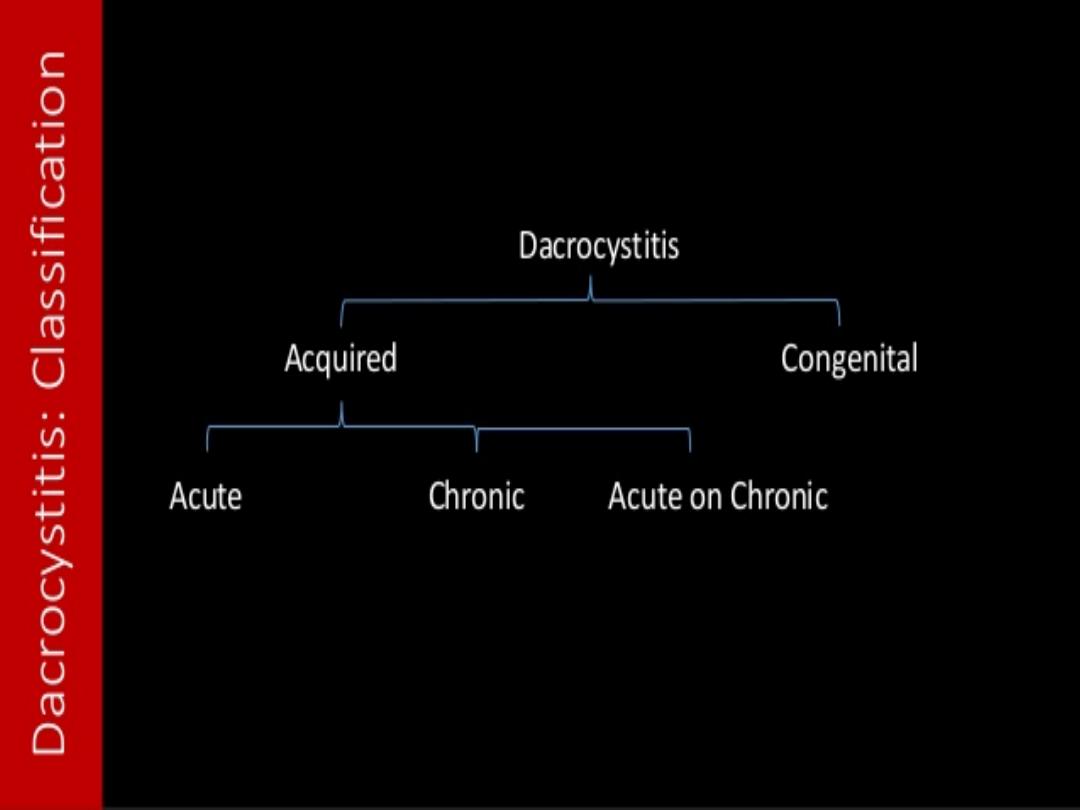

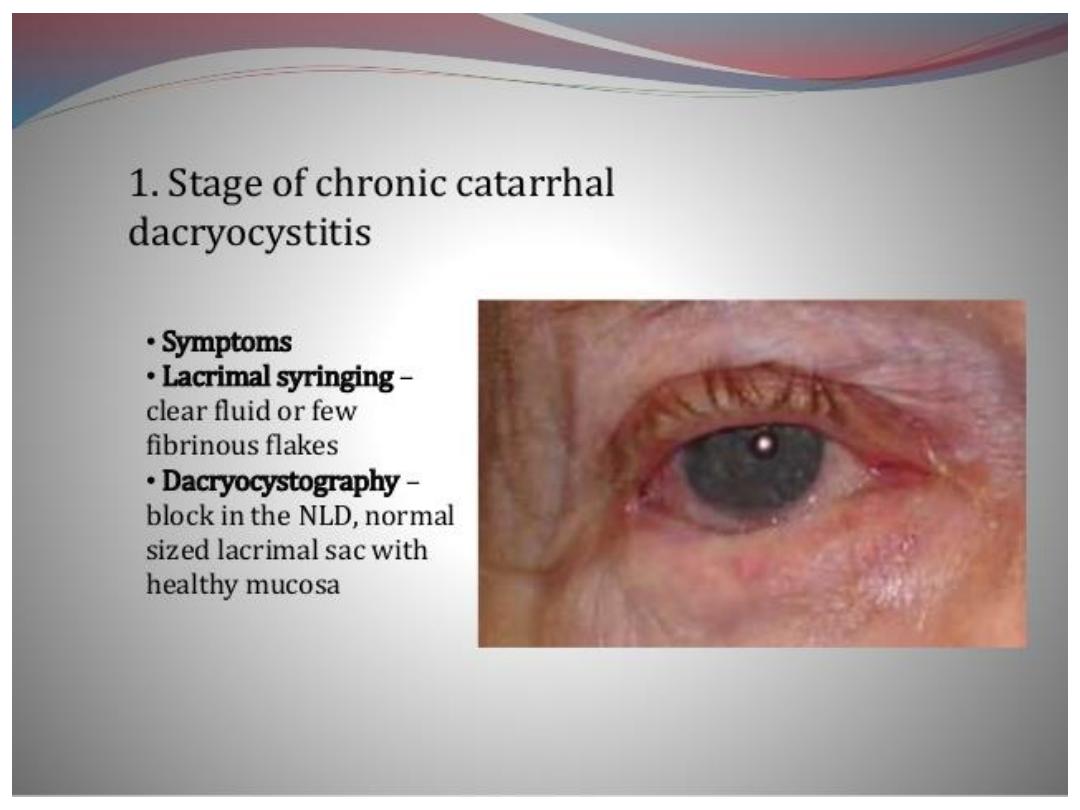
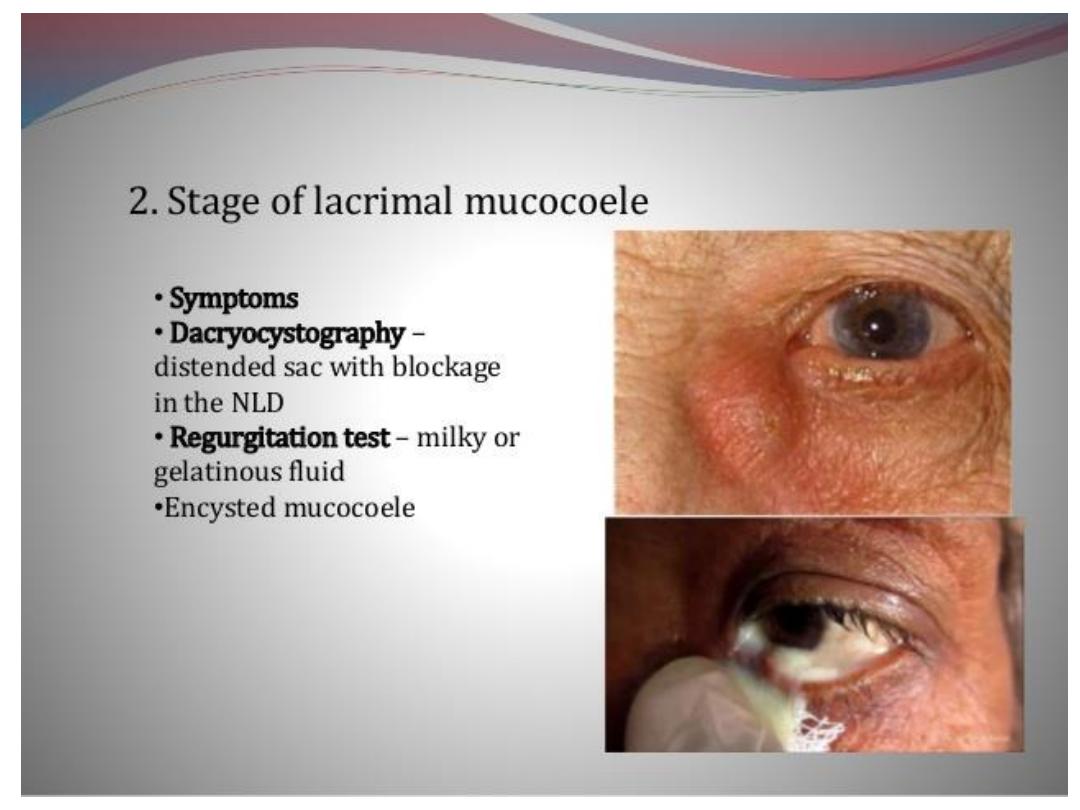
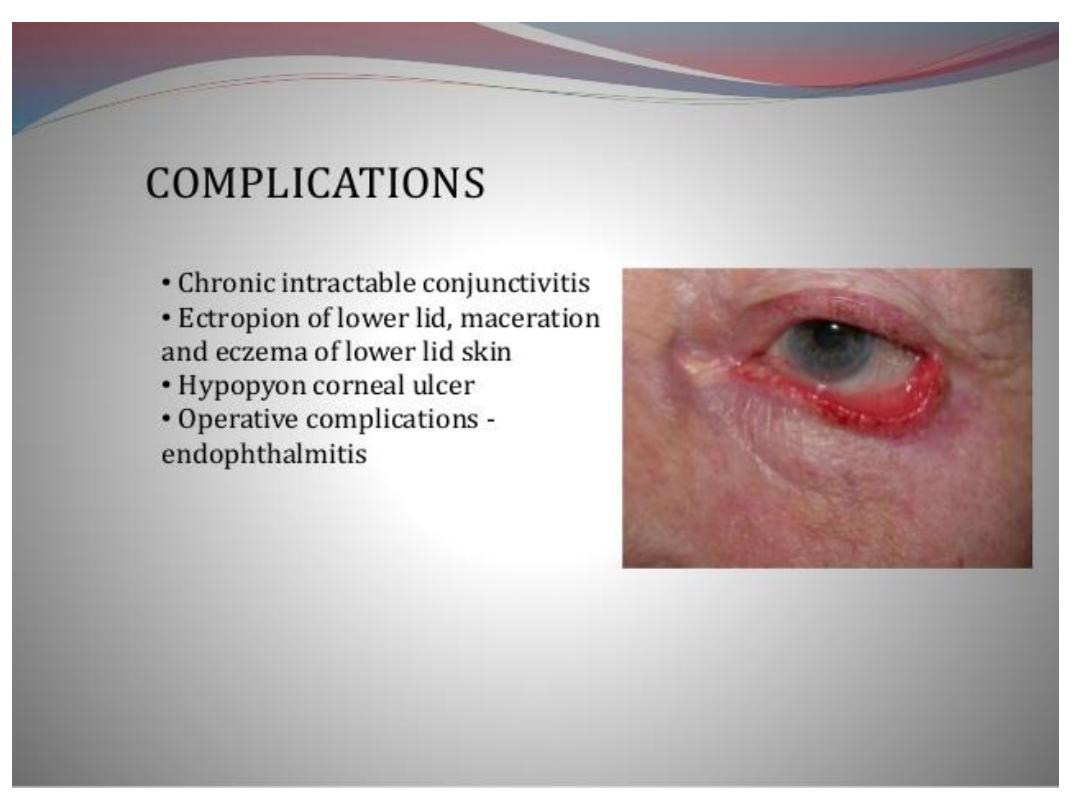
Chronic dacryocystitis