
Orthopaedic surgery
فرع الجراحه
\
كلية طب الموصل
upper limbs trauma 2
د
.
ساهر حبيب
دكتوراه
(
بورد
)
اختصاص جراحة العظام والكسور

Fracture of the shaft of the humerus.
This fracture is common in adults, caused by fall on out stretched hands or by direct blow on the
arm , it might be spiral, oblique, transverse , or comminuted.
The displacement is variable, the fractures may be pathological. The arm is painful, bruised and
swollen.
Fracture above the deltoid insertion (deltoid tuberosity), the proximal segment is adducted by
pectoralis major muscle , and if the fracture below the deltoid insertion then the proximal segment
is abducted by the effect of the deltoid muscle .
Injury to the radial nerve is common with this fracture mainly at the junction of the middle third
and the lower third of the shaft due to close contact of the nerve to the bone at that site( Holstein
lewis fracture).
It is very important to test for the radial nerve function before and after treatment and this is done
by assessing active extension of fingers and wrist .
X – ray shows the site of the fracture, type of the fracture , degree of displacement, or any
evidence of pathological fracture.


Treatment
Fracture of the humerus heal readily .
Displaced fractures treated by manipulation , if reduction is
stable, or the fracture is undisplaced ; fractures treated by
p.o.p cast made from the axillae to the wrist with elbow flexed
90`, the limb is slinged from the wrist , this can be left for 2-3
weeks and then replaced by well fitted prefabricated plastic
brace from shoulder to elbow further 4-6 weeks .
Exercise of the wrist and the fingers should be started from
the beginning to avoid stiffness . Exercise of the shoulder
should be started as early as possible to avoid stiffness(
mainly in elderly).

If the fractures unstable, or unreducible ( 30 degrees varus /valgus
,3cm shortening and 20 degree anterior angulation), severe multiple
injuries, an open fracture, segmental fractures , displaced intra-
articular extension of the fracture , a pathological fracture ,a ‘floating
elbow’ (simultaneous unstable humeral and forearm fractures) ,
radial nerve palsy after manipulation, bilateral , obese with big
breast, non-union and problems with nursing care in a dependent
person.
Fixation can be achieved with either (1) a compression plate and
screws, (2) an interlocking intramedullary nail or semi-flexible pins,
In open fractures or infected fractures external fixation used.
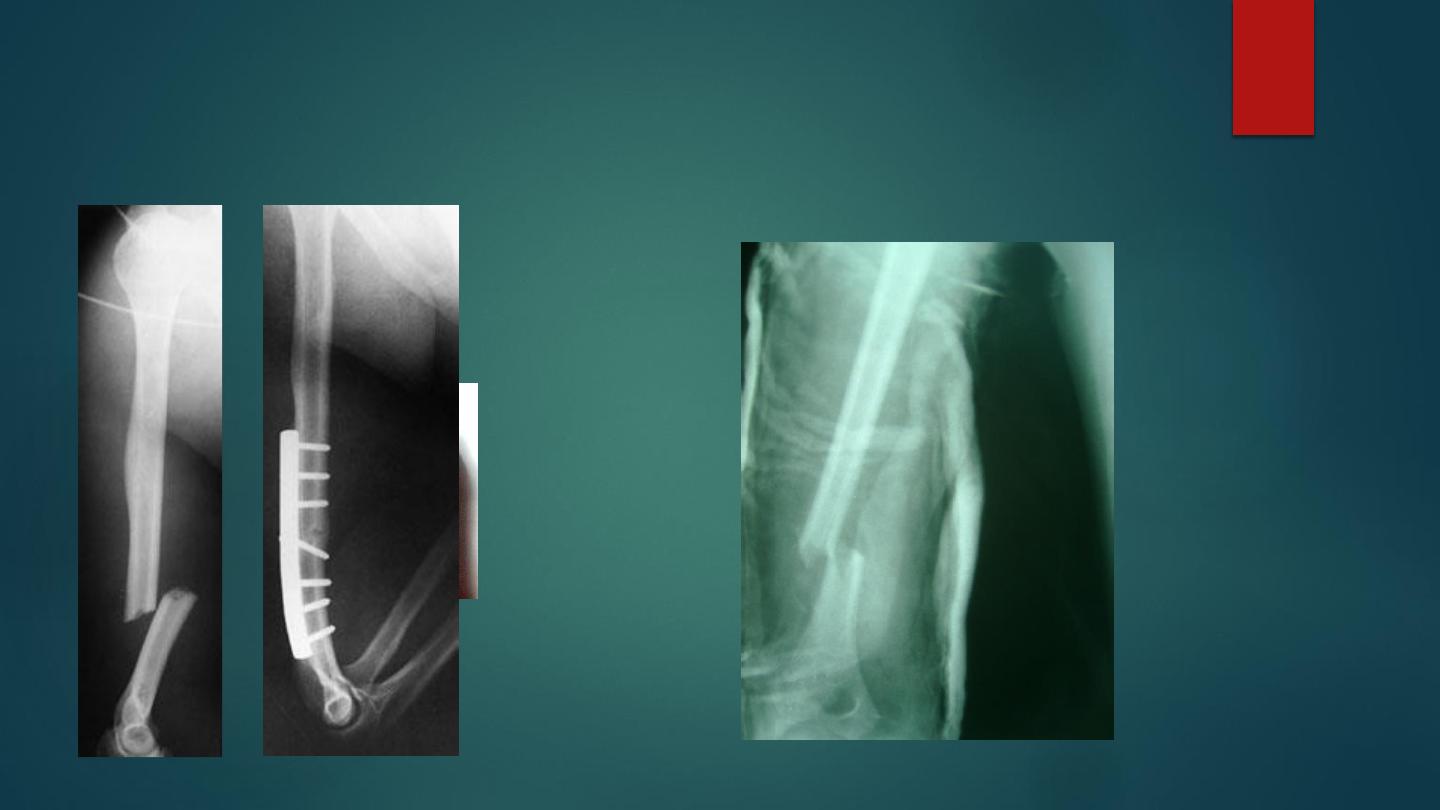
Fractured humerus

Complications :
Early :
1-vascular injury (brachial artery) .
2- radial nerve injury is common; it
cause wrist drop .
Late complication :
1- delayed union and non union .
2- malunion.
3- joint stiffness (minimized by
early activity).

Supracondylar fractures
It is very common and important fracture in children , it regarded as
potentially dangerous because of risk of ischemia , caused by fall onto the out
stretched arm hand.
posterior type is the commonest type about 95% of the cases , , the humerus
breaks just above the condyles , the distal fragment is displaced and tilted
backward , anterior type is rare due to direct blow on the elbow posteriorly .
Classification ( cartland classification ) :
Grade one : undisplaced fracture .
Grade two : angulated fracture with the posterior cortex is still in continuity .
Grade three :completely displaced fracture .
Clinically : History of fall on out stretched hand , the child is in pain ,
swelling , deformity (which is S shape in posterior type) .
It is very important to check the distal pulsation (radial pulse) and capillary
refilling to assess the distal circulation , and checking the nerves for any
injuries( mainly the anterior interossous nerve ) .
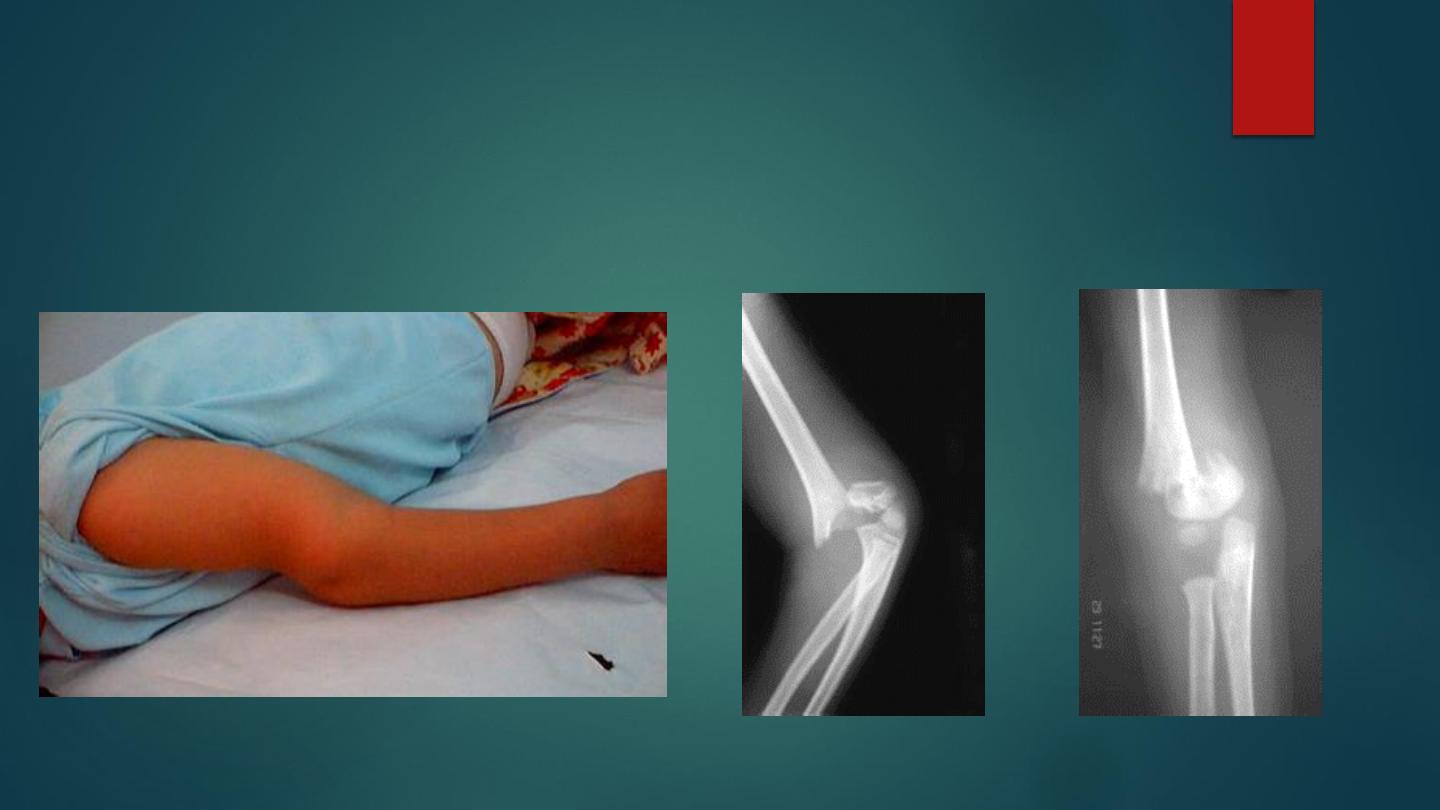
S shape deformity of supracondylar fracture of
the humerus , with AP and lateral x ray of the
elbow

X-ray : the fracture is seen clearly in A-P , and lateral views just above the condyles . In
undisplaced fracture the fat-pad sign which is triangular lucency in front of the distal humerus
this will raise the suspicion of the fracture . In A-P view we can measure the Baumans’ angle
which is helpful in assessing the degree of angulation of the distal segment ( normally less than
80° ).
Treatment depend on the degree of displacement, and careful watch should kept on circulation.
Grade one (undisplaced fracture.) : the elbow is immobilized at 90` flexion and neutral rotation in
plaster cast and hanged by sling for 3 weeks.
Grade two (posterior angulated fractures) : treated by manipulation under anesthesia by
continuous traction for 2-3 minute in the length of the arm in (semiflexion position elbow) with
counter traction , correction of the side way tilt and rotation , gradual flexion of the elbow to
120`then feel the radial pulsation if ( –ve ) then do gradual extension tell the pulsation become
(+ve), add 10 degrees for safety . Then back slab and x-ray checking ; after 10 days, full plaster
cast done for another 3 weeks . If manipulation failed manipulation and percutaneous pining or
open reduction and fixation by Kirschner wires.
Grade three (completely displaced fracture.) : Manipulation under anesthesia if fail then do close
pining or open reduction and fixation by Kirschner wires .
Indications of open reduction : 1- closed unreducable fracture. 2-open fracture . 3- associated
vascular damage .
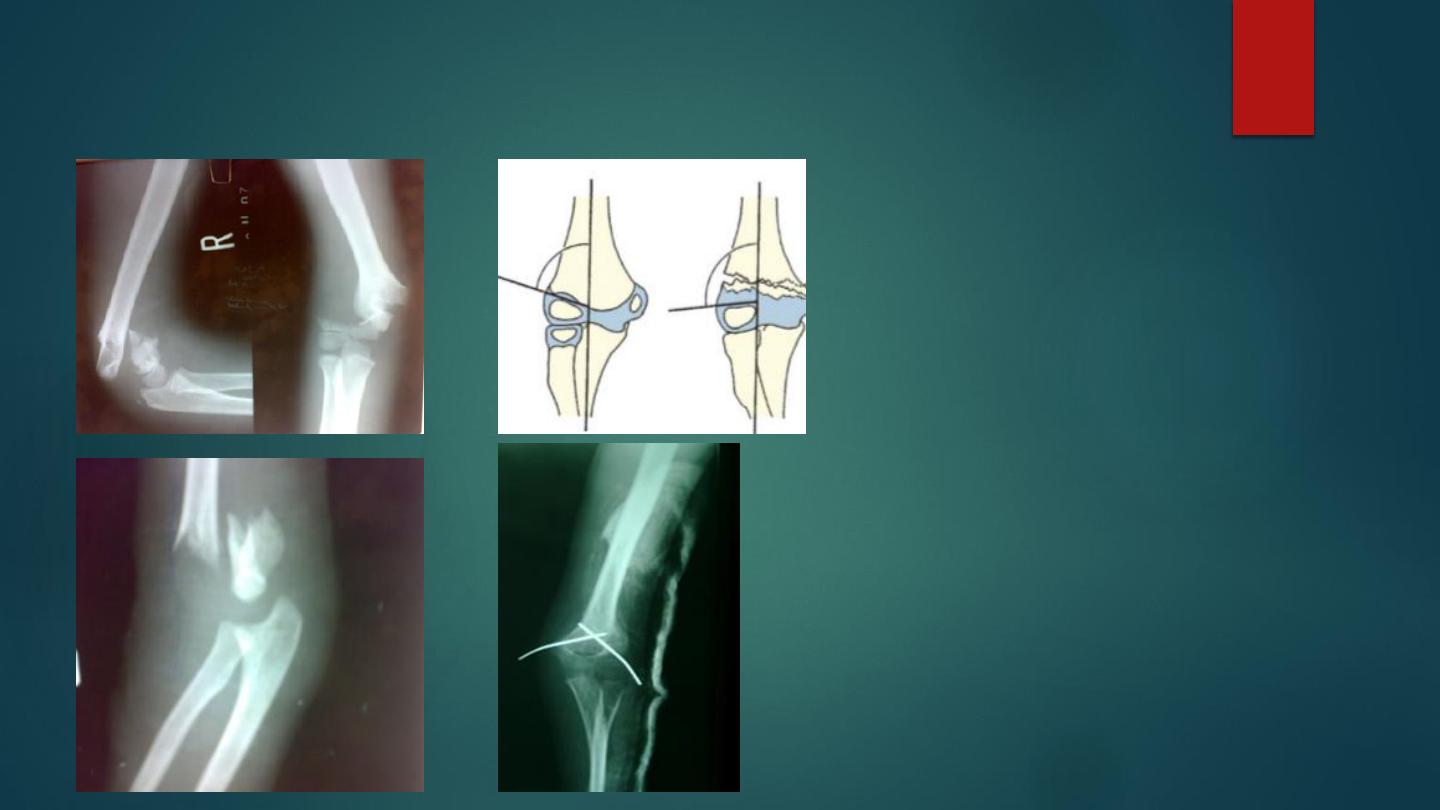
Supracondylar fractures showing baumann angle

Complications
Early :
1- vascular damage and compartment syndrome : mainly brachial artery; this will lead to ischemia of the forearm
(Volkmann's ischemia ) . The ischemia also occur in the forearm due to edema in the muscles in close facial space
caused increase in the pressure and more edema and ischemia this called( compartment syndrome)
This condition can be caused by proximal arterial injury , soft tissue bleeding from fractures and operations , and tight
dressing.
The early symptom very sever pain and the earliest sign is painful dorsiflexion of fingers or toes , to wait until the 5 p
appear is criminal.
The classic features of ischemia are the 5 p ( pain , paler , pulseless , paraesthesia , paralysis ).
The diagnosis can be confirmed by measuring the intracompartmental pressure by special catheter introduced into the
compartment if the difference between diastolic pressure and compartment pressure less than 30, or if it is more than
40 mm mercury is an indication of urgent decompression
Treatment of compartment syndrome : The compartment should be decompressed by immediate and complete removal
of the cast, the bandages and the dressing ; the limb should be nursed flat with slight elevation above the level of the
heart , and if no response in few minutes then immediate open fasciotomy should be done and the wound should be left
opened .
2-nerve injury : Median nerve easily injured by the displaced fracture , ulnar and radial nerves can be injured also.

Late complications :
1- malunion : it is a common complication ,.
Uncorrected side tilt or angulation and rotation lead to deformity ; mainly varus
deformity called cubitus varus and rarely valgus called cubitus valgus deformity .
Varus deformity is disfiguring and called (gun stock) deformity, which is permanent
deformity that may need surgical correction .
Valgus deformity is rare and cause late ulnar nerve palsy .
2- elbow stiffness and myositis ossificans :
Elbow is very liable for stiffness after injury ;passive physiotherapy is contraindicated
in elbow stiffness because it make the condition worse and aggravate myositis
ossificans , it is advisable to do active physiotherapy .
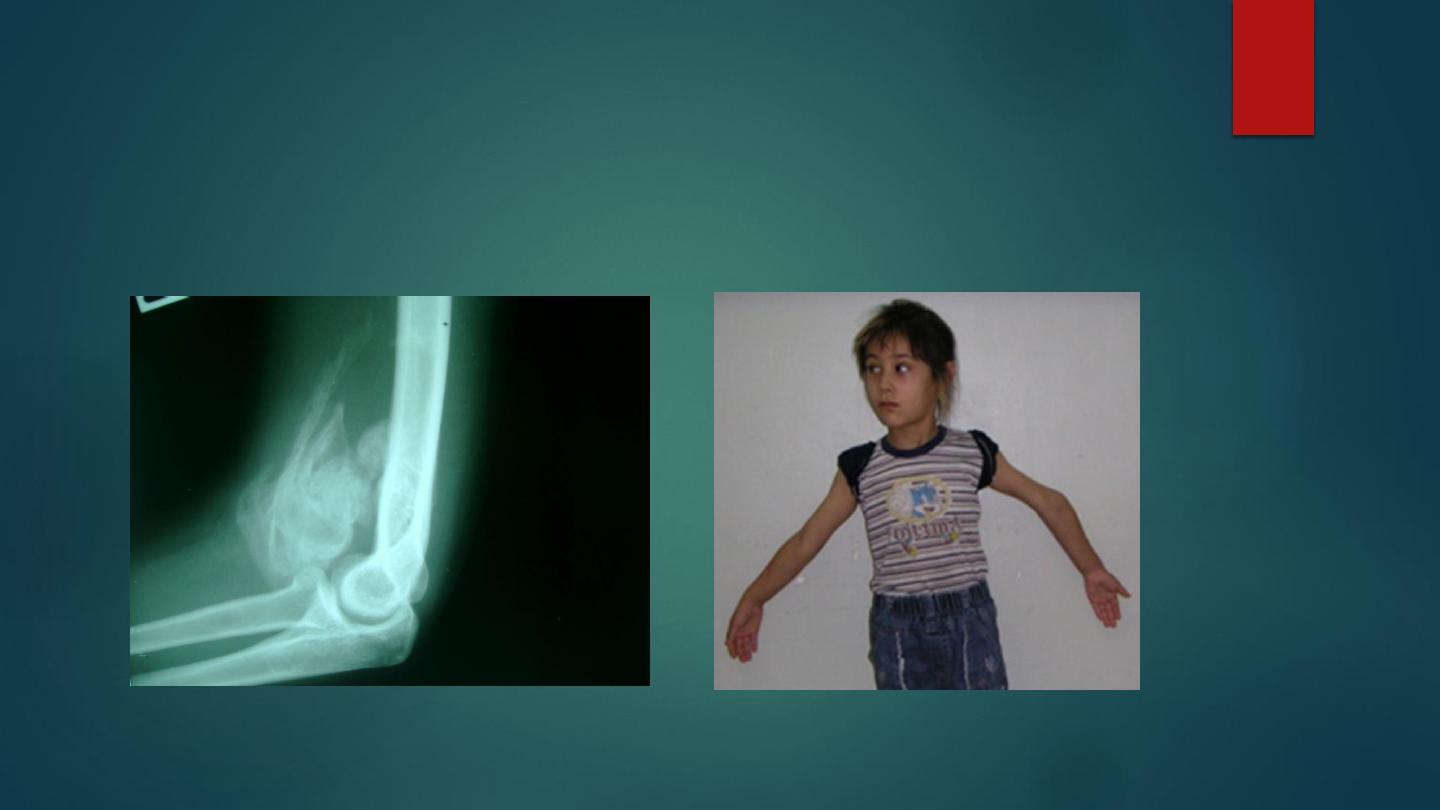
Myositis ossificans
gun stock deformity

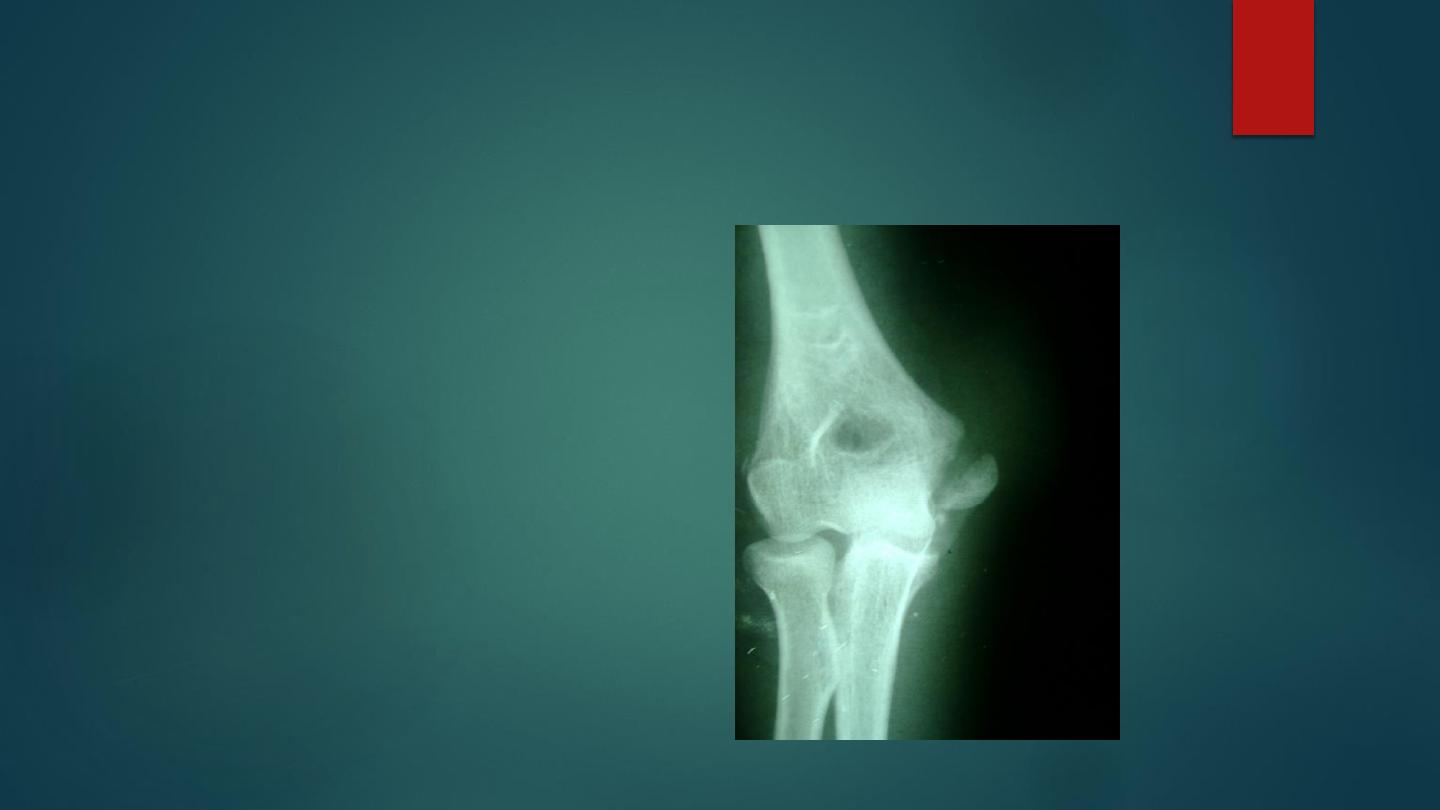
Fracture of the lateral condyle of the humerus
This fracture occur due to fall on out stretched
hands.
The fracture piece although it look small in the x-
ray but it in fact is large and it pulled by extensor
muscle of the wrist which attached to it.
In severe cases the piece is rotated by the action of
the extensor muscle and become capsized lead to
nonunion later on if not treated .
The elbow swollen and deformed , tenderness at
the site of the fracture .
Treatment
:
If there is no or minimal displacement we can do back slab above the elbow
which is 90` flexed and the forearm is neutral ; after 7 days repeat the x-ray for
checking and full p.o.p. for 3-4 weeks , followed by active exercises .Displaced
fracture need open reduction and fixation by K-wire or screw .
Complications :
1- nonunion : this complication is inevitable if the distal piece is capsized and
not treated ; this will lead to disturbing of the growth at the distal end of the
humerus lead to cubitus valgus and late ulnar nerve palsy .
2-malunion in form of cubitus valgus and growth changes in lower humerus
which may lead to late ulnar nerve palsy and recurrent dislocation of the
elbow .
3-friction neuritis of ulnar nerve.
4-
Osteoarthritis.
Fractures of medial condyle of the humerus is less common and treated on
same principles
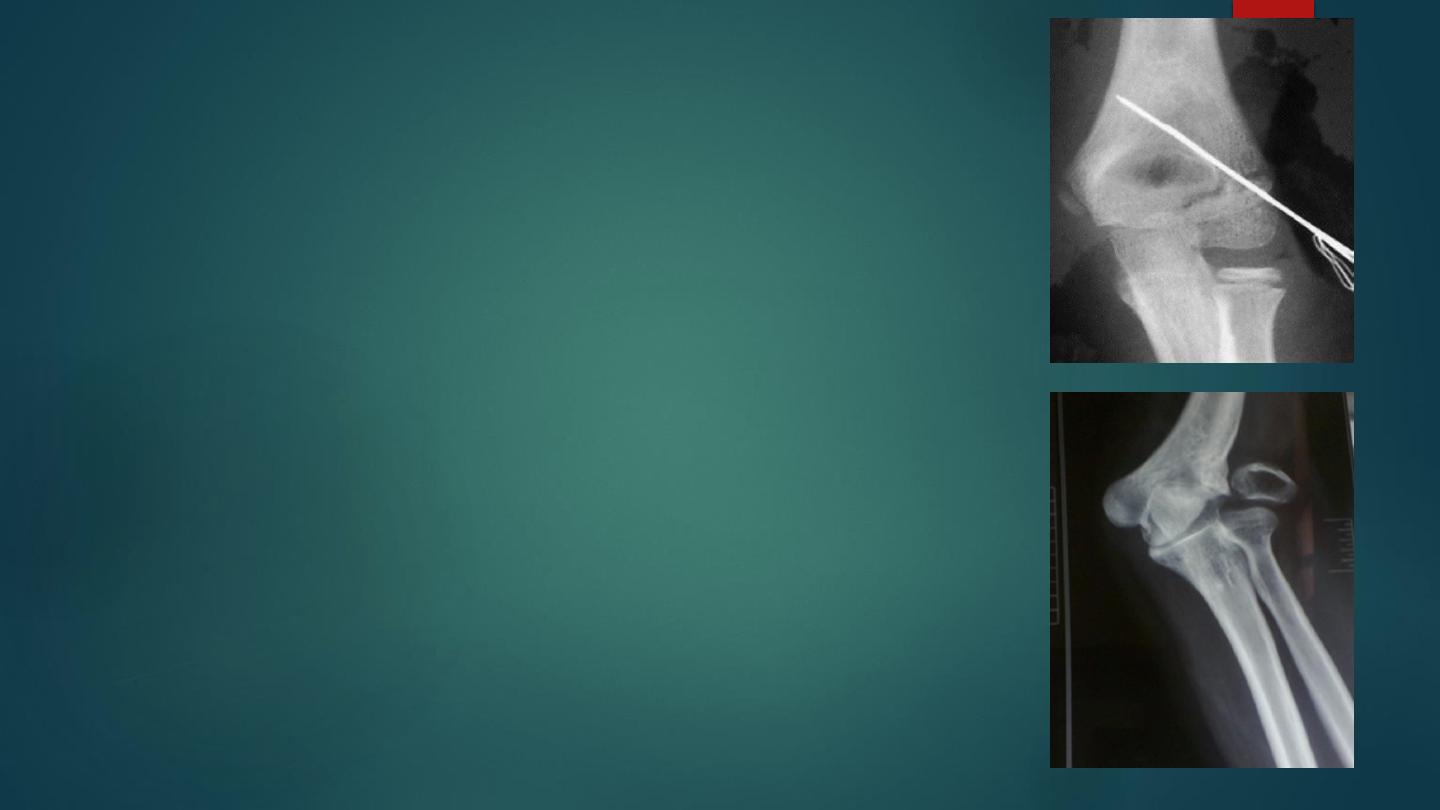
Fracture medial epicondyle of the humerus
It occurs more often in children due to fall
on out stretched hands ; the medial
epicondyle is avulsed by the effect of the
strong flexor muscles of the wrist .
If the elbow joint is dislocated or
subluxated even momentarily , the medial
epicondyle may entrapped inside the joint .
Clinically there is history of trauma , pain ,
swelling and tenderness, the sensation and
power of the fingers should be tested to
exclude ulnar nerve damage .

Treatment
Minor displacement less than 5 mm treated by back slab in flexion position for 7 days
followed by plaster cast for 2-3 weeks , followed by active exercises.
If the piece is trapped into the joint , then it must be freed either by manipulation
under anesthesia , if failed or the piece is severely displaced then we should do open
reduction and fixation by Kirschner wire or suture.
The commonest early complication is ulnar nerve damage . Stiffness of elbow is late
complication.
Fractures of lateral epicondyle is less common and treated on same principles.
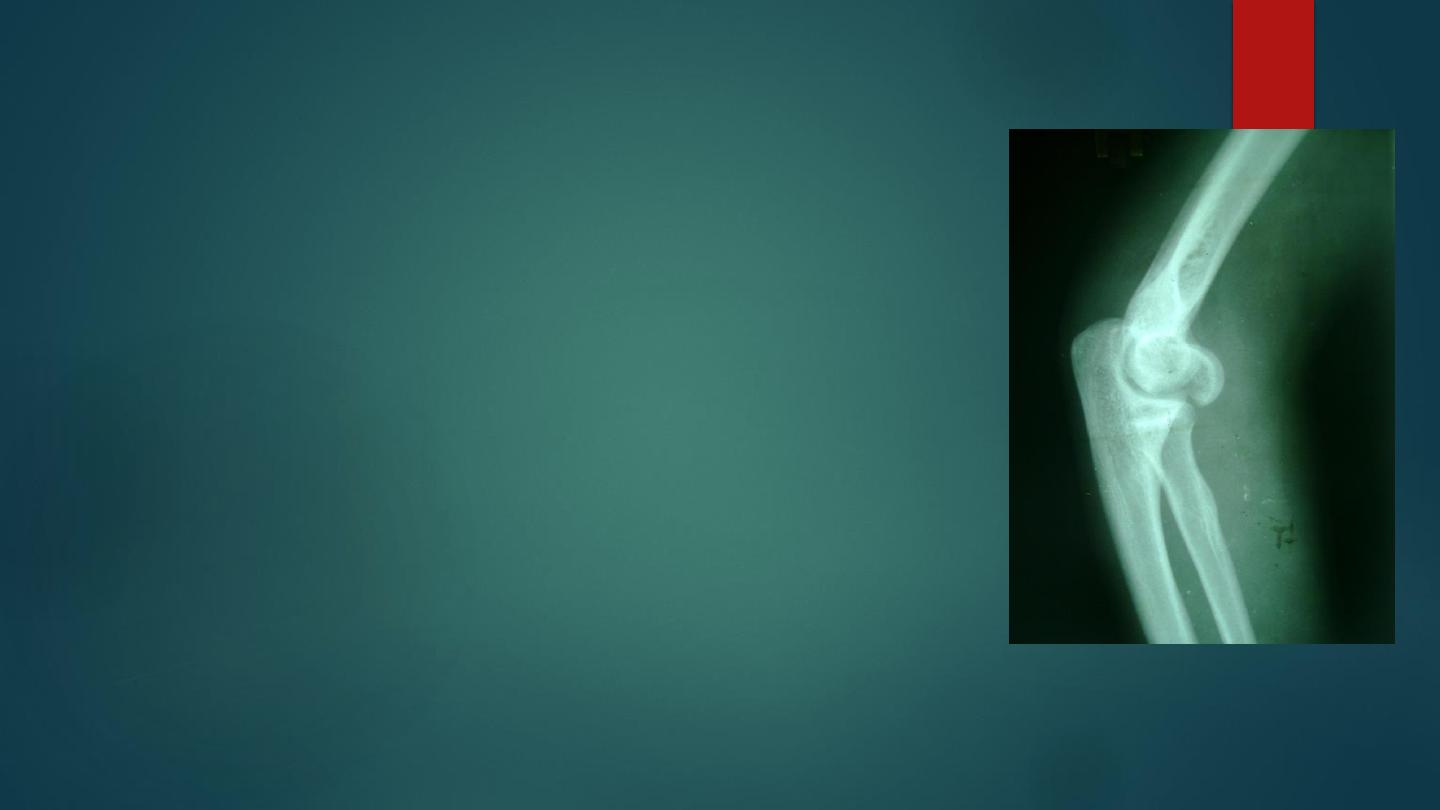
Fracture capitulum
This is an articular fracture occur in adult .
The patient fall on the hands with the elbow straight .
The capitulum or the anterior part of it only is sheared off
and displaced proximally .
There is pain and fullness in front of the elbow , flexion is
completely restricted .
X-ray in lateral view shows that the capitulum or part of it
is seen in front of the lower part of the humerus .
Simple undisplaced fracture ( rare) treated by splintage for
4 weeks .
Displaced fracture should be treated by open reduction and
internal fixation .

Fractures of distal humerus in adults
Fractures around the elbow in adults
– especially those of the distal
humerus – are often high-energy
injuries which are associated with
vascular and nerve damage. Some
can be reduced and stabilized only by
complex surgical techniques; and the
tendency to stiffness of the elbow
means that with all severe injuries the
striving for anatomical perfection has
to be weighed up against the realities
of imperfect postoperative function.
three types of distal humeral fracture:
Type A – an extra-articular
supracondylar fracture;
Type B – an intra-articular
unicondylar fracture (one condyle
sheared off);
Type C – bicondylar fractures with
varying degrees of comminution

bicondylar fractures

Treatment
Non displaced managed
conservative by casting
Displaced managed by open
reduction and rigid internal
fixation with early physiotherapy
Other modalities includes ,
skeletal traction , elbow
replacement and bag of bone
technique
Complications
Early
Vascular injury.
Nerve injury(median and ulnar
nerve).
late
Stiffness
Heterotopic ossification

Dislocation of the elbow
Dislocation of the ulno -humeral joint is common , more in adult.
In 90% of cases the ulna is displaced posteriorly or postero -lateral . It is caused by heavy fall on
out stretched hand with the elbow in extension .
If the dislocation is not associated with fracture the reduction of the dislocation will be stable and
recurrent dislocation is unlikely.
The dislocation might associated with fracture on medial epicondyle, coronoid process, radial
head, capitulum, or tear of the ligaments then the reduction will be unstable and recurrent
dislocation is suspected .
Anterior dislocation of the elbow rarely occur in ( side swipe) injury .
The patient support his or her forearm with the elbow in slight flexion , if the swelling is not so
sever , the deformity is obvious . The relation of the olecranon to the epicondyles will be
abnormal, the hands must be examined for nerve and vascular injuries .
X-ray done to confirm , the presence of the dislocation and the associated fracture .


Treatment :
Uncomplicated dislocation reduction should be done under general anesthesia with muscle
relaxant ; the surgeon pull on forearm while the elbow is slightly flexed , the olecranon pushed by the
thumb forward , then do gradual flexion of the elbow ; full flexion is cannot be obtained unless
perfect reduction done ; then checking of the range of movement , stability , distal neurovascular
injuries , and new x-ray performed to confirm the reduction . The arm is held in a collar and cuff with
the elbow flexed above 90 degrees. After 1 week the patient gently exercises his elbow; at 3 weeks
the collar and cuff is discarded. Elbow movements are allowed to return spontaneously and are
never forced. The long-term results are usually good
Complication :
Early :
1- vascular injury (brachial artery ) .
2- nerve injury median , ulnar, radial nerves.
Late :
1- stiffness .
2- myositis ossificans ,if this occur then put the joint in splintage until pain subside then gentile active
movement advised with anti – inflammatory drug .
3- recurrence.
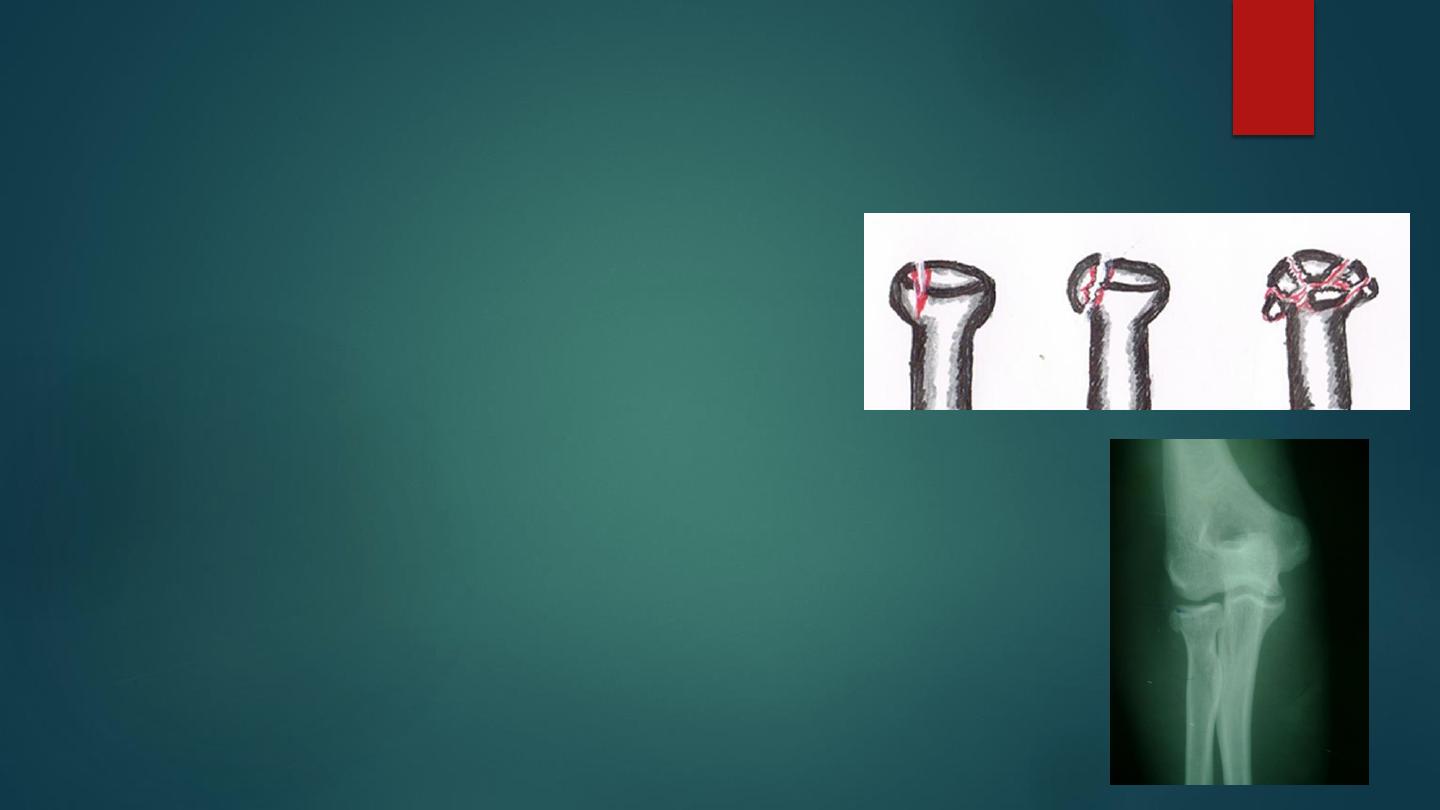
Fractured head of the radius
It is common injury in adults, occur due to fall on out
stretched hands with elbow extended and pronated.
The fracture may simple undisplaced vertical split ,
single depressed fragment, or whole head comminuted .
Clinically there is history of fall with pain and
tenderness over head of radius, restriction of elbow
movement especially pronation and supination.
Treatment :
Undisplaced fractures treated by back slab above elbow for
3 weeks followed by active exercises , if the fracture
segment displaced then it should be reduced and fixated by
screw or wire .
Comminuted fractures treated by excision of the head of
the radius and some time replace it by prosthesis .
Complications : joint stiffness , myositis ossificans, and
osteoarthritis.
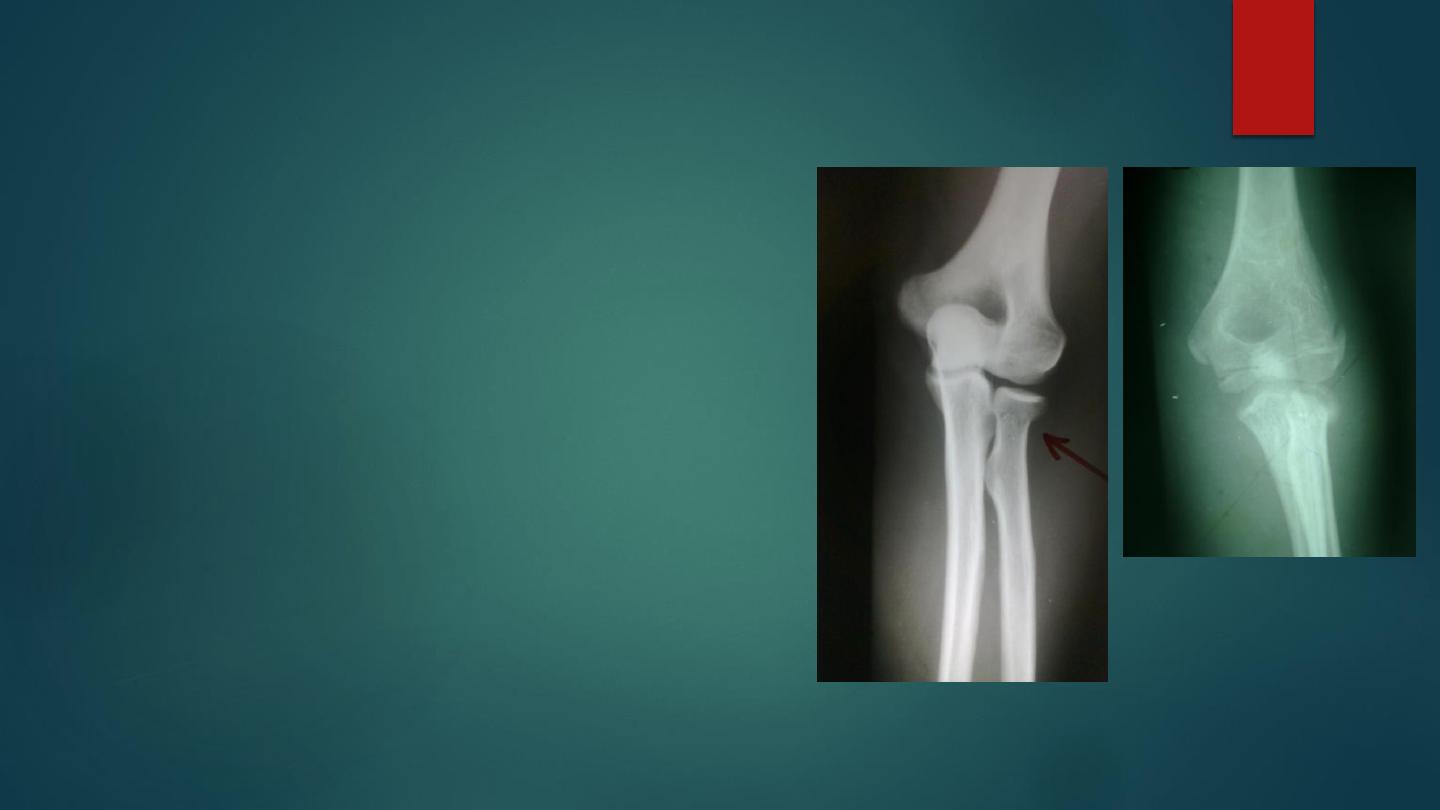
Fracture neck of the radius
It occur due to fall on out stretched hands
especially in children .
There is pain and localized tenderness on the
head of the radius and pain on rotating the
forearm .
X-ray shows fracture and its displacement.
Children up to 30` of radial head tilt and up to
3mm of transverse displacement is acceptable ,
and it treated by back slab with flexed elbow 90`
for 3 weeks .
Displaced fracture more than this limit need
manipulation under anesthesia , if failed then
open reduction and fixation by Kirschner wires .
Radial head should never excised in children .
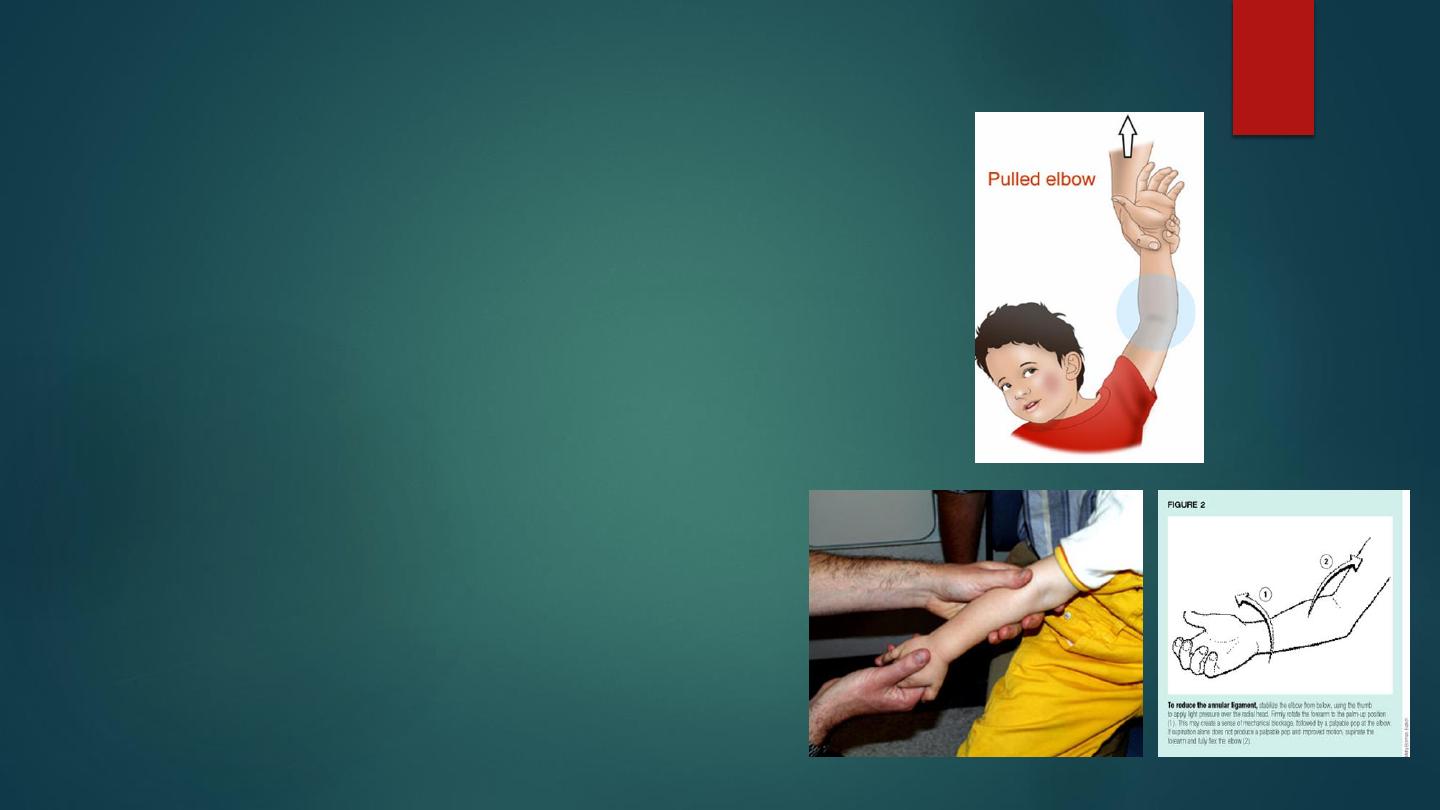
Pulled elbow
In young children the elbow may be injured
by pulling on the arm. usually with the
forearm pronated.
It is due to slipping of the orbicular ligament
over the head to the joint.
A child age with 2-3 years brought with a
painful dangling arm with history of jerky
movement of the arm .
The forearm held with pronation and
extension, there is no x-ray changes.
Dramatic cure obtained by forcefully
supinating and then flexing the elbow.
Recurrence are common until age of 6
years.
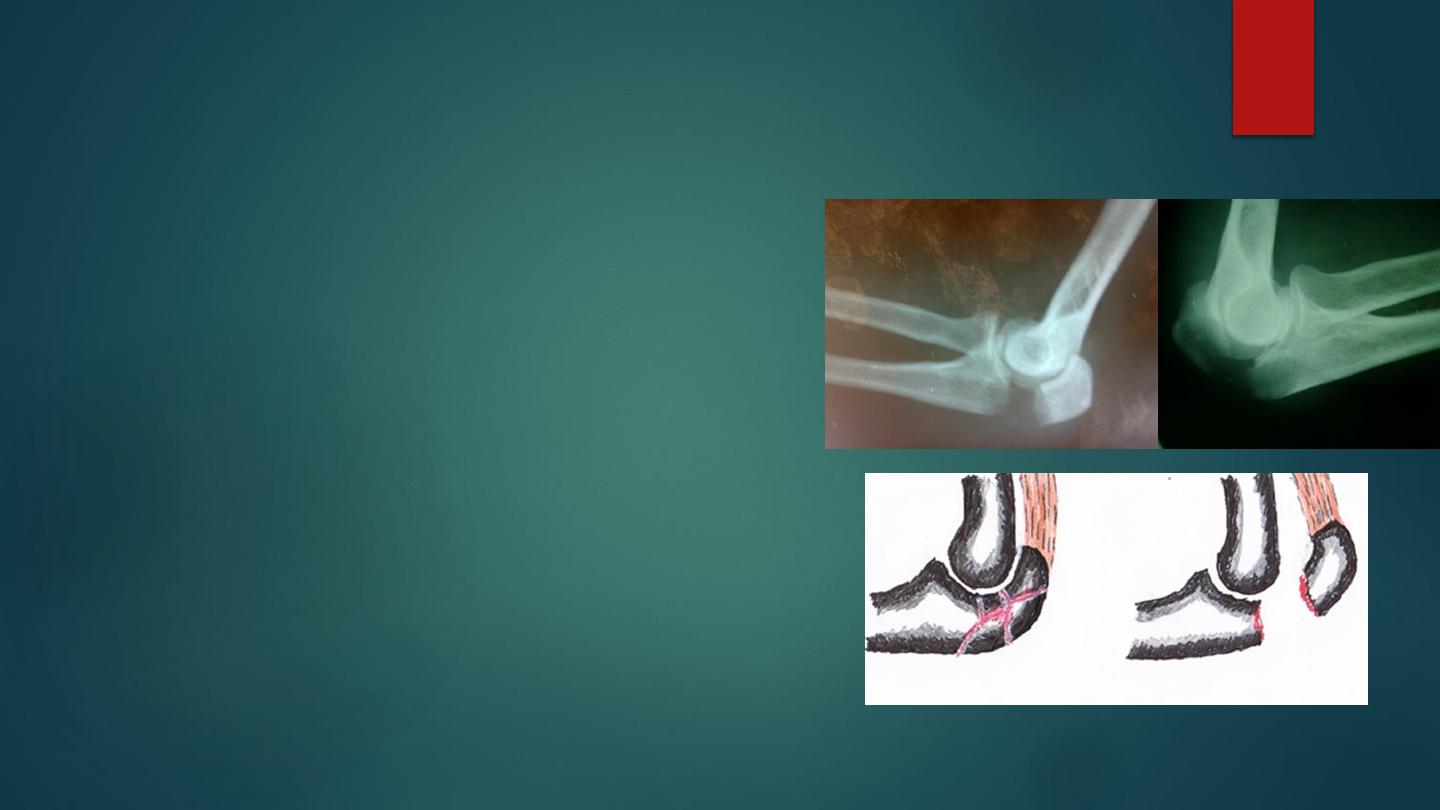
Fractures of the olecranon
The olecranon is fractured by direct trauma
cause fracture without displacement or a
comminuted fracture, while a transverse
displaced fracture caused by indirect trauma,
due to traction when the patient falls onto the
hand while the triceps is contracted suddenly.
There will be pain, bruises over the elbow,
swelling and tenderness ; some time we feel a
gap in case of transverse fracture .
X-ray demonstrated the fractures types and
their displacement .
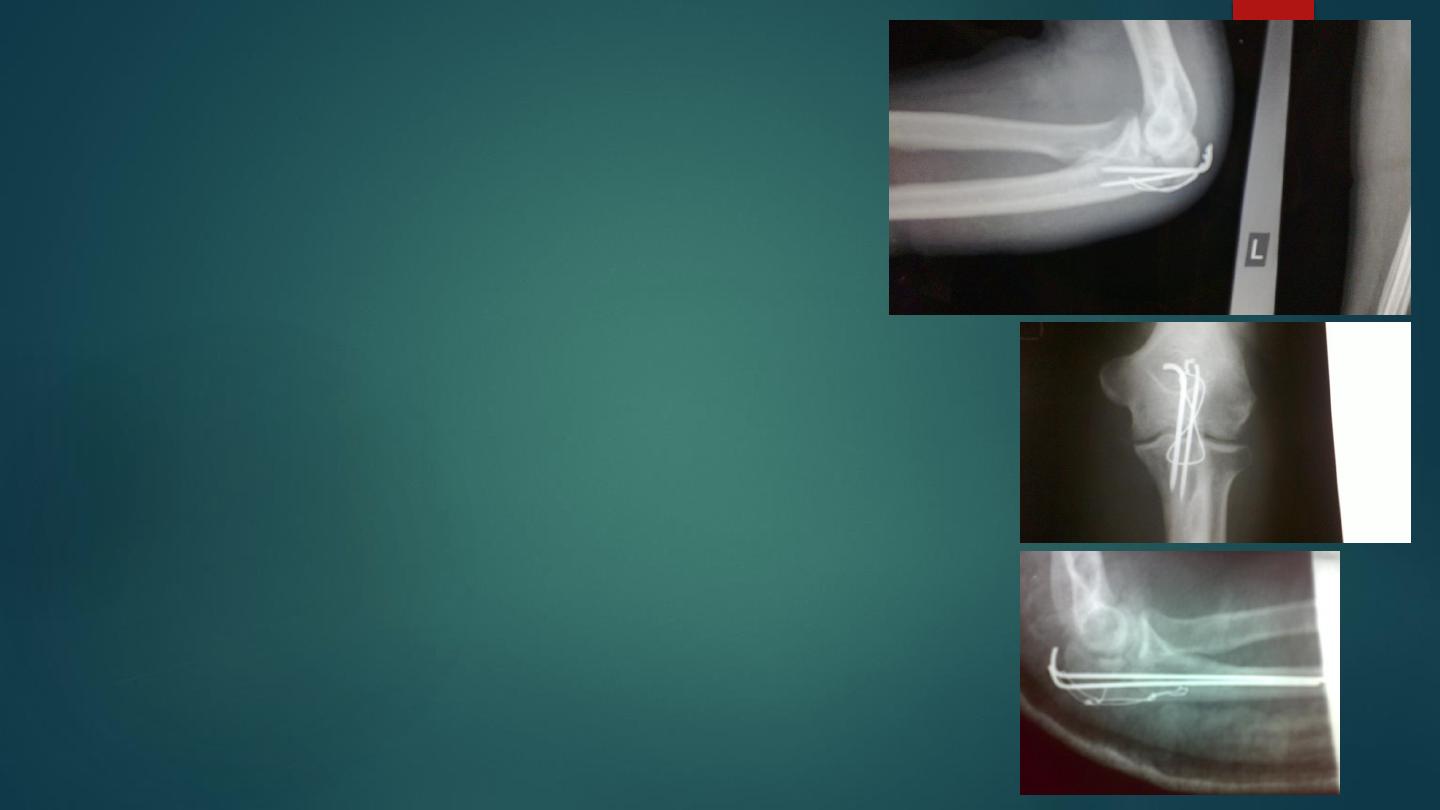
Treatment :
In case of single undisplaced or comminuted
fracture with triceps aponeurosis is intact , the
treatment is by plaster cast for 3 weeks in flexion,
then simple active movement is encouraged to
avoid stiffness .
For displaced transverse fracture it need open
reduction and internal fixation because it reduced
only when the elbow is extended and stiffness of
the elbow in that position is disastrous. The
fixation is by tension band wire or by screws.
Complications of olecranon fractures include
stiffness of the elbow , non union, and osteoarthritis
of elbow joint.

Fractures of the shaft of the radius and ulna
Fractures of the shaft of both bones occur commonly in road traffic accidents , it can be
caused by twisting force , which cause spiral fracture in both bones in different levels , or
direct blow lead to transverse fractures at the same level.
Additional rotation which lead to more displacement can be caused by the pronator
muscles (pronator teres , pronator quadratus ) inserted in the middle and the lower thirds
and the supinator muscles (biceps , supinator ) inserted in the upper third of the forearm
The displacement is variable and may be in any direction.
Fracture is usually quite obvious but we should do checking of the nerves and arteries
distal to the site of the fracture which can be affected by injuries or compartment
syndrome .
The fracture in children might be greenstick.
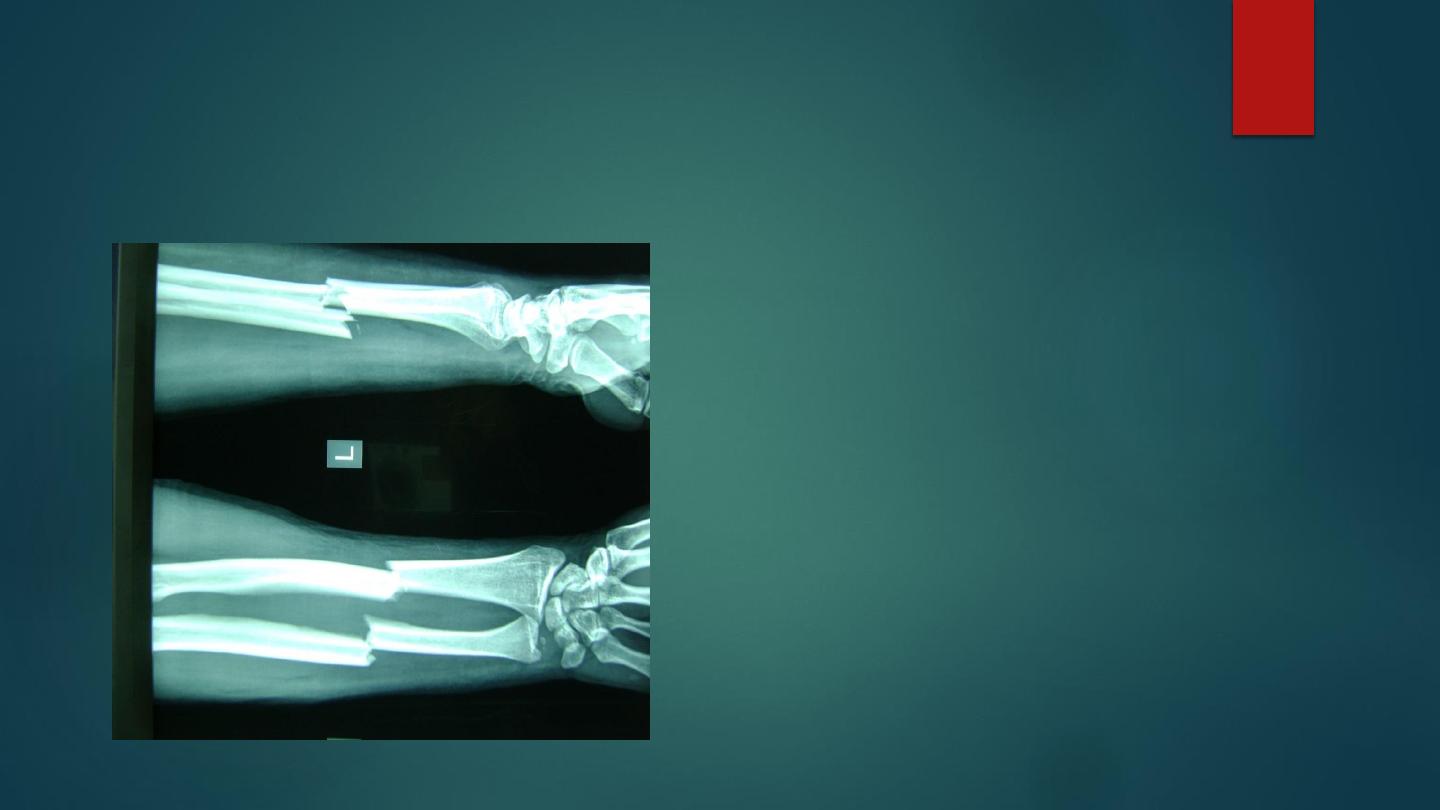
AP and lateral x ray of forearm showing transverse
fracture of both radius and ulna at same level

Treatment:
Accurate reduction is important in fracture of radius and ulna, to preserve the pronation and
supination.
In children with green stick fracture , the closed treatment is usually successful because the thick
periosteum tend to guide and control the reduction ; after reduction we put back slab above elbow
which is 90` flexed and ask the patient to elevate the limb to decrease the edema ; after 10 days we
change the slab to complete plaster cast, if the fracture is in the upper third we put the forearm in
supination , if it in the middle third we put the forearm in neutral and if it in the distal third we put the
forearm in pronation .
The plaster cast should be left for another 4-6 weeks . Followed by physiotherapy .
Open reduction is indicated in children :
1-if the fracture cannot be reduced .
2- if the reduction is unstable .
The fixation will be by plate and screw or intramedullary nail.
In adult the best treatment is open reduction and internal fixation , closed reduction of this fracture in
adult is very difficult and redisplacement in the cast is common .
Most of the surgeons prefer the open reduction and fixation from the beginning by plate and screws .

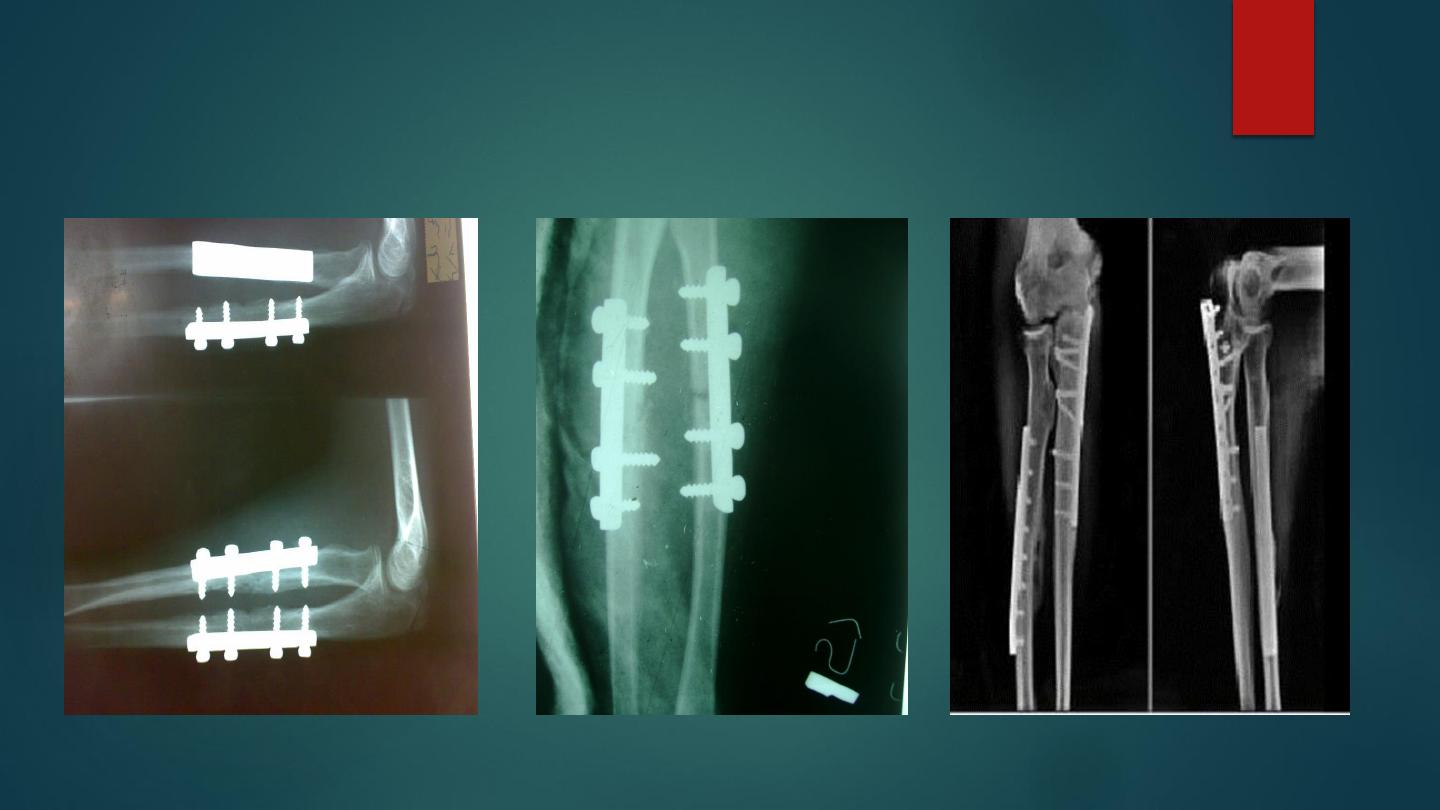
ORIF by plate and screws

Open fracture treated by debridement and external fixation or internal fixation can
be used in compound fracture.
Complication:
Early : the early complication include nerve injury , vascular injury, compartment
syndrome , and infection if the fracture is open.
Late :
1- delayed union and nonunion .
2-malunion and cross union ( radio ulnar synostosis ) which lead to limitation of
pronation and supination