1
Eyelids
(
2 lec.)
Dr Abdulmelik shallal
Anatomy:
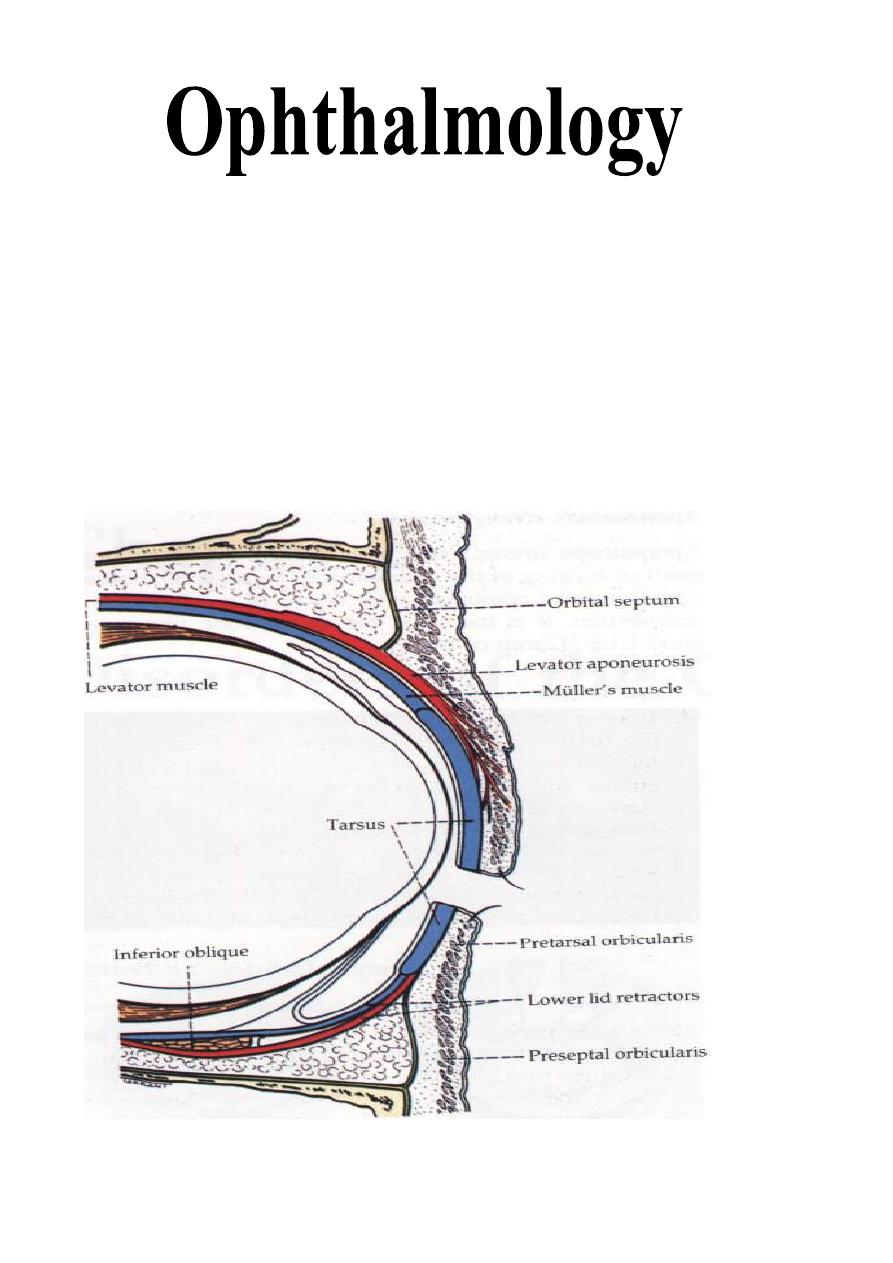
Eyelids are thin movable curtains composed of skin on their anterior surface
and mucus membrane (conjunctiva) on the posterior surface, they contain:
1- Smooth muscles (Müller's muscles).
2- Striated muscles (Orbicularis oculi and Levator palpebrae superioris
"LPS").
3- Dense fibrous plates (Tarsal plates).
4- Glands.
5- Nerves and blood vessels.
2
The contents of the lid are distributed as follows: the anterior surface is made
of skin which has a round edge with the lid margin, the subcutaneous tissue,
muscular layer, the submuscular (areolar tissue) layer, the orbital septum which
end as a tarsal plate (that forms the architecture of lid) and finally the
conjunctiva (palpebral) which is situated most posterior.
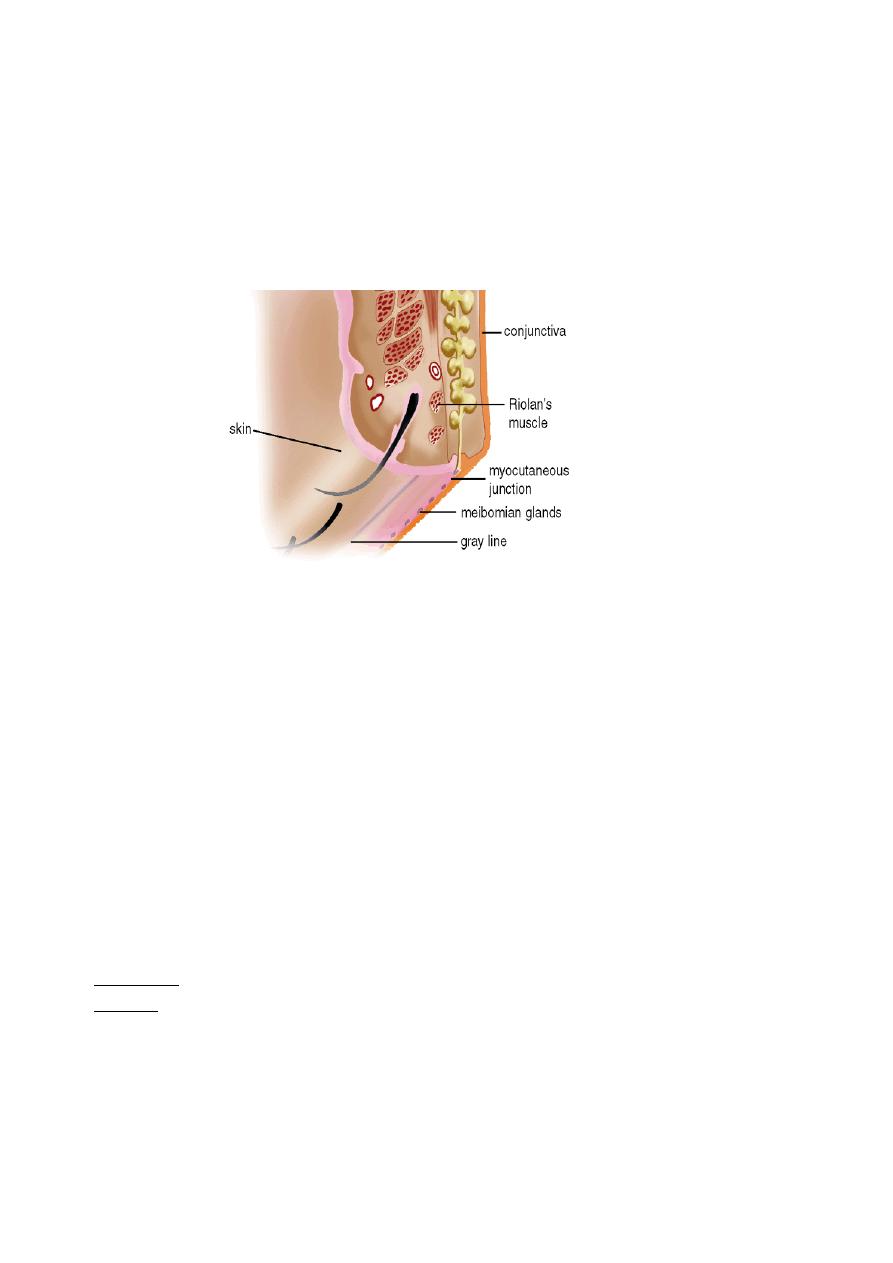
The free margin of the eyelids contains:
1- The lashes (Cilia).
2- Grey line.
3- Orifices of Meibomian glands.
4- Mucocutaneous junction
5- Superior and inferior puncti of Naso-Lacrimal System (NLS).
Muscles of the eyelids:
1- Orbicularis oculi muscle:
It is a thin oval sheet of concentric striated muscle surrounding the palpebral
fissure.
It can be divided into:
a- Peripheral (orbital) part: This is involved in forceful closure of lids.
b- Central (palpebral) part: This is involved in involuntary blinking, voluntary
nonforceful closure and participates in forceful closure with the orbital part.
c- Muscle of Rioland's: this part is represented by the gray line of lid margin.
d- lacrimalis muscle: that attached to the fundus of lacrimal sac. This part is
involved in pumping action of lacrimal drainage system.
Nerve supply:
Sensory: Ophthalmic branch of trigeminal nerve
Motor: Facial nerve.
2- Levator palpebrae superioris muscle:
It is originates from the periosteum covering the lesser wing of sphenoid bone
at the apex of the orbit.
The aponeurosis inserts into:
a- Skin of the upper eyelid, so it forms skin creases on the eyelid.
3
b- Upper edge and anterior surface of the tarsal plate.
c- Medial and lateral palpebral ligaments.
Function: To keep the palpebral fissure open against gravity & tone of
orbicularis oculi muscle.
Nerve supply:
Sensory: Ophthalmic branch of trigeminal nerve
Motor: Oculomotor nerve.
3- Superior palpebral muscle (Müller's muscle or superior tarsal muscle):
It is a small sheet of smooth muscle originated from the under surface of the
LPS muscle and inserted to the upper edge of the upper tarsal plate.
Nerve supply: Sympathetic nerves.
Function: Like LPS, is to keep the palpebral fissure open against gravity.
Glands in the eyelids:
1- Meibomian glands (Tarsal glands):
Modified sebaceous gland located in the tarsal plate. The upper tarsus
contains 30-40 glands, while the lower tarsus contains 20-30 glands.
Function: It secret the lipid forms the outer layer of the tear film.
2- Zeis glands:
Modified sebaceous gland opened with lash follicles.
3- Glands of Moll:
They are modified sweat gland whose ducts also open into lash follicle or
directly in the anterior lid margin between the lashes.
Congenital anomalies of eyelids:
1- Ablepharon: Absence of the eyelids.
Treatment:
Reconstructive plastic surgery.
2- Ankyloblepharon: Imperfect separation of the eyelids.
Treatment:
Open the adhesion in between.
3- Coloboma of the eyelids: Common congenital anomaly in which there is
failure of a portion of the lid to develop leading to notch in the lid margin.
Treatment:
Plastic surgery.
4- Blepharophimosis: Narrowing of the palpebral fissure.
Treatment
: Plastic surgery at pre-school age.
5- Epicanthus: Common anomaly. There is a vertical skin fold in the medial
canthal region, which conceals the medial angle and caruncle giving a picture
simulates convergent squint (pseudosquint).
Abnormalities in shape and position:
1- Entropion:
It is an inward rolling of the lid margin causing continuous rubbing of the
cornea, which leads to conjunctival congestion, painful watery eye (tears

4
production due to stimulation of cornea) and sometimes epithelial defect and
even corneal ulceration. So, it is a vision threatening disease.
Causes (Types) of entropion:
a- Congenital: which is very rare.
b- Spastic entropion: secondary to any condition that causing severe ocular
irritation (irritation leads to overriding of Orbicularis oculi muscle fibers),
e.g.: conjunctivitis, keratitis and ocular surgery.
Treatment
:
of underlying cause and taping of lid (turned outward).
c- Senile entropion (involutional entropion): affecting elderly patients and
usually involves the lower lid.
Treatment
: is surgical correction.
d- Cicatricial entropion: secondary to any condition causing scaring and
shrinkage of conjunctiva, e.g.:
i- Chlamydial conjunctivitis.
ii- Chemical conjunctivitis (whether it is acidic or alkaline).
iii- Autoimmune conjunctivitis. e.g.
Cicatricial pemphigoid
and
Stevens-
Johnson syndrome
iv- Irritation conjunctivitis.
2- Ectropion:
It is an outward rolling of the lid margin causing exposure of the palpebral
and bulbar conjunctiva. This exposure leads to exposure conjunctivitis,
exposure keratitis and watery eye. Long-standing cases lead to:
i- Dry and thick conjunctiva and even keratinization.
ii- Corneal ulceration. So, it is vision threatening disease too.
iii- Redness, crusting and dermatitis of skin due to?
Causes (types) of ectropion:
a- Congenital ectropion.
b- Paralytic ectropion (Atonic): seen in cases of facial nerve palsy.
Treatment
: we should wait for 6 months for spontaneous recovery e.g. (Bell's
palsy) then lateral tarsorrhaphy is indicated.
c- Senile ectropion (involutional): due to atrophy of orbicularis oculi muscle
and tarsal plate.
Treatment
: surgical correction.
d- Cicatricial ectropion: which is occur secondary to:
i- Chemical burns of skin.
ii- Infection of skin.
iii- Radiation of skin.
5
iv- Improper suturing of lid wound.
v- Trauma to the lid.
e-
Mechanical ectropion of lower lid, when there is large mass that evert it.
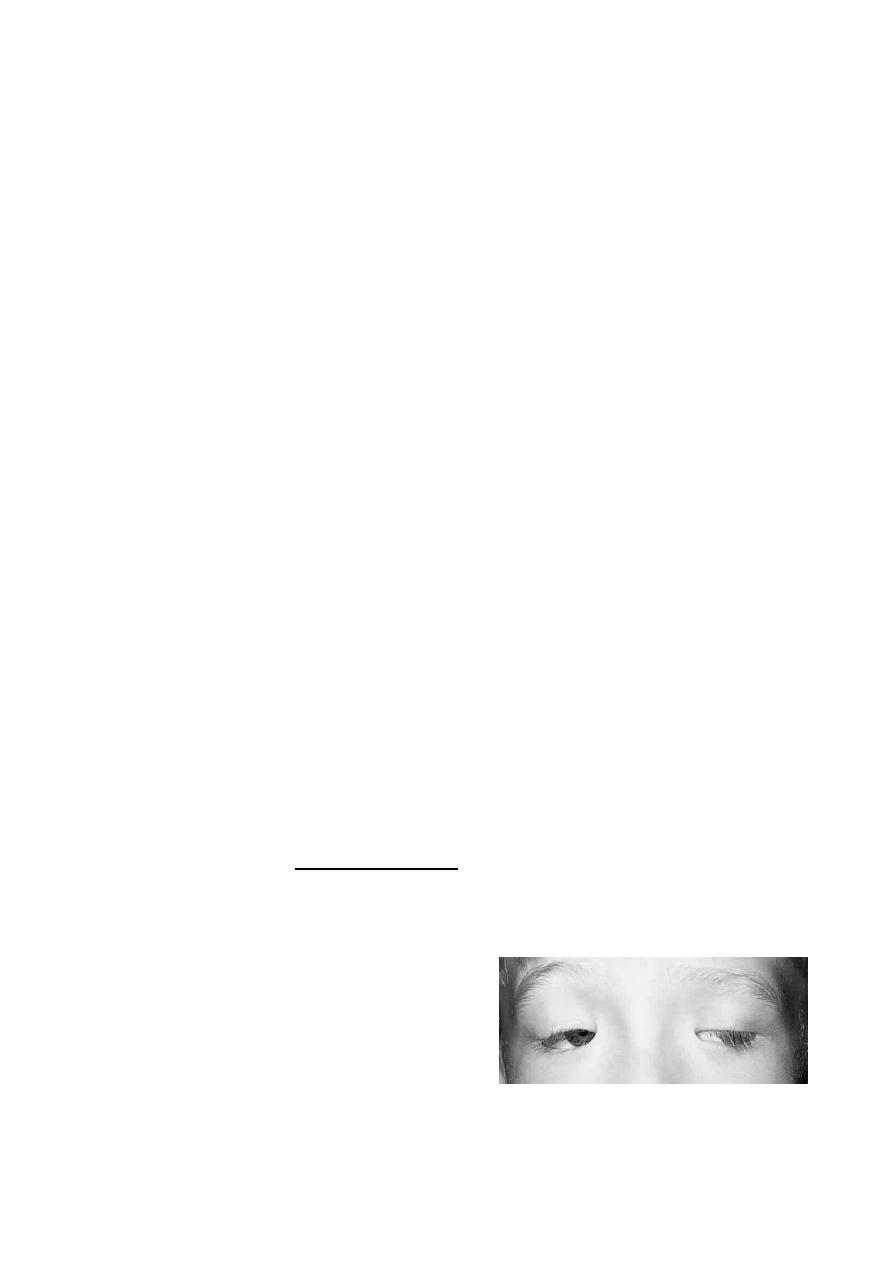
3- Blepharoptosis:
It is an abnormal low position or drooping of the upper eyelid. It could be
unilateral or bilateral, and both of them could be partial or complete. Normally
the upper lid covers only 2 mm from cornea but if more, this called
blepharoptosis.
Causes of blepharoptosis:
a- Simple congenital blepharoptosis: the LPS muscle is very poor and there is
absence of skin creases.
b- Neurogenic blepharoptosis:
i- Oculomotor nerve palsy ( congenital or acquired) : causing severe
blepharoptosis.
ii- Horner's syndrome ( congenital or acquired): causing mild
blepharoptosis.
iii- Marcus Gunn Jaw-winking syndrome: it is a congenital anomaly in
which, nerve to LPS is a branch from nerves to mastication muscle (i.e. from
trigeminal nerve).
iv- 3
rd
nerve misdirection: either acquired or congenital.
* Why it is severe in (i) and mild in (ii)?
c- Myogenic blepharoptosis:
i- Myasthenia gravis: there is a defect in the neuro-muscular junction
(damage to acetyl choline receptors).
Treatment :
medical treatment.
ii- Myotonic dystrophy.
iii- Ocular myopathy (localized defect similar to myasthenia gravis).
iv- Simple congenital myogenic blepharoptosis.
v- Blepharophimosis syndromes: it is a
syndrome in which, there are bilateral
ptosis,
bilateral
palpebral
fissure
narrowing,
bilateral
ectropion,
and
increase in the distance between the two
medial canthi (telecanthus).
d- Aponeurotic blepharoptosis:

6
there is atrophy or damage in aponeurosis(specialized tendon) of LPS muscle.
i- Involutional (senile).
ii- Post operative.
e- Mechanical blepharoptosis:
There is increases weight of the eyelid:
Causes:
i- Trachoma, VKC, large chalazion, abcess and eyelid tumor.
ii- Cicatricial (due to LPS and superior rectus muscles fibrosis).
iii- Trauma (collection of fluid).
iv- Lack of support (phthisical or nanophthalmos): it is not a real ptosis, but
the lid drops as there is no support below it due to small size of eyeball & best
called pseudoptosis.
Treatment of ptosis: The treatment of all types is surgical except in
myasthenia gravis, where the treatment is medical. Surgical procedures are:
a- Levator resection.
b- Frontalis brow suspension (Sling operation).
c- Tarso-conjunctival resection (Fasanella servete procedure).
Choice of one of these three types depends on:
a- Aetiology of ptosis.
b- Severity of ptosis: Mild, moderate or severe.
c- Function of LPS: Good, fair or poor.
4- Trichiasis:
Backward misdirection of the eyelashes (cilia), sometimes it is associated
with entropion and it is called pseudotrichiasis.
Causes:
a- Any cause leads to entropion of the eyelid, so, it is Pseudo-trichiasis.
b- Trachoma without or with entropion, so it is True or pseudo-trichiasis
respectively.
c- Chronic blepharitis: which causes True trichiasis.
Treatment
: For isolated misdirection cilia (true trichiasis)
a- Epilation: Repeated every few weeks.
b- Electrolysis: Destruction to hair follicles by cauterization.
c- Cryosurgery: Destruction to hair follicles by freezing.
d- Laser ablation: Destruction to hair follicles by laser.

7
For pseudo-trichiasis: done by correction of entropion surgically.
5- Blepharospasm:
Involuntary sustained closure of the eyelids which occurs either
spontaneously (essential blepharospasm) or by sensory stimuli (2ndary
blepharospasm).
Treatment:
Is to treat the underline cause and in sever, and resistance cases Botulinum
toxin injection is indicated. It is temporary measure and can be repeated
frequently.
6- Madarosis:
It is a decrease in number or complete loss of lashes.
Causes:
Local Causes: chronic blepharitis, burns, radiation and infiltrating tumor.
Systemic causes: generalized alopecia, psoriasis, SLE, syphilis and leprosy.
Benign nodules and cysts:
1- Chalazion (Meibomian cyst):
It is a chronic lipogranulomatous inflammatory lesion caused by blockage of
meibomian gland orifices and stagnation of sebaceous secretions and there is
NO infection.when there is infection this called internal hordeolum.
It is more frequent and multiple in patients with acne rosacea or seborrhoeic
dermatitis and other sebaceous gland dysfunctional diseases.
Presentation: Painless nodule and occasionally blurred vision (Why?)
Signs:
a- Round, firm lesion in the tarsal plate.
b- Polypoid granuloma on eversion of lid (i.e. seen from the palpebral part of
conjunctiva).
c- Sometimes there is associated blepharitis.
d-Mechanical ptosis may present.
Treatment:
a- Surgical:
The most common method, if the lesion is recurrent or multiple then biopsy
should be taken specially in old age patient (to exclude sebaceous gland
carcinoma which is extremely rare).
b- Steroid injection:
Good alternative to surgery, 0.1-0.2 ml triamcinolone infiltrated around the
lesion, the success rate is 80%. In unresponsive cases, another injection is

8
given two weeks later. Chalazion should be small in size to be treated with
steroid injection.
c- Systemic tetracyclines:
As prophylaxis, particularly in acne rosacea and seborrhoeic dermatitis
where chalazion is frequently recurrent.
2- Internal Hordeolum:
It is a small abscess caused by an acute staphylococcal infection of
Meibomian glands.
Signs: Tender, inflamed swelling within the tarsal plate.
Treatment:
a- which is done through using topical antibiotics (ointments more important
than drops). (Why?). Systemic antibiotics are needed if there is associating lid
infection.
b- Incision and curettage for the residual nodule after the acute infection has
subsided.
3- External hordeolum (Stye):
It is an acute small staphylococcal abscess of a lash follicle and its associated
gland of Zeis.
Signs:
- Tender inflamed swelling in the lid margin, which points anteriorly through
the skin.
- More than one lesion may present.
- Occasionally minute abscess may involve the entire margin.
Treatment:
a- Hot compresses to produce vasodilatation of blood vessels: is to increase
the circulation in the area and also for liquefaction of sebum to prevent
stagnation in the duct of affected gland.
b- Topical antibiotics to prevent infection of neighboring glands (ointment is
a must).
c- Epilation (removal of eyelashes by a forceps) to enhance drainage of pus.
d- Systemic antibiotics if there is no response on topical or in 2ndary
preseptal cellulitis.
Note: An infection anterior to the orbital septum (affecting anterior lamella of
eyelid) is "preseptal cellulitis" while infection posterior to orbital septum is
orbital cellulitis.

9
Marginal Chronic Blepharitis
Chronic blepharitis is a very common condition which is usually bilateral
symmetrical.
Types of chronic blepharitis:
1- Anterior: a- Staphylococcal infection.
b- Seborrheic dysfunction.
c- Mixed.
2- Posterior: a- Meibomianitis.
b- Meibomian seborrhea.
c- Mixed.
3- Mixed (any one of the anterior type plus any one of the posterior).
Pathogenesis of chronic blepharitis:
1- Anterior chronic staphylococcal blepharitis: due to staphylococcal over
proliferation.
2- Anterior chronic seborrhoeic blepharitis: is usually associated with
seborrhoeic dermatitis e.g. scalp, naso labial folds, retro auricular area and
sternum.
Neutral lipids are converted by Bacterial lipase into irritating fatty acids
responsible for increase of symptoms.
3- Posterior chronic blepharitis: Associated with dysfunction of Meibomian
gland (ocular rosacea) which is in some patients associated with acne rosacea of
the face.
Symptoms of chronic marginal blepharitis: (anterior and posterior)
They are: Burning, grittiness, mild photophobia, crusting and redness of the
lid margin & sometimes red eye. Although it is chronic disease its symptoms
are characterized by remissions and exacerbations. The symptoms are usually
worse in the mornings(in contrast to dry eye). There is much discrepancy
between symptoms & signs.
Signs of anterior blepharitis:
a- The anterior lid margins show (by slit-lamp) hyperaemia and telangiectasia.
In longstanding cases the lid margin became scarred and hypertrophied (due to
recurrent infections), intrafollicular abscess may be present (staphylococcal
blepharitis).
b- Two types of scales: (important in differentiation)
i- Staphylococcal blepharitis: Are hard and brittle and are centered around
the lashses (collarettes).

10
ii- Seborrhoeic blepharitis: Are soft and greasy and located anywhere on lid
margin or on the lashes.
c- In longstanding cases, trichiasis, madarosis and occasionally poliosis
(whitening of the eyelashes) will occur.
Complications of anterior blepharitis:
a- External hordeolum (stye).
b- Tear film instability (due to the abnormal lipid secretion that affects the tear
film).
c- Hypersensitivity to staphylococcal exotoxins papillary conjunctival
reaction, punctuate epitheliopathy and marginal keratitis.
Treatment:
a- Lid hygiene: removing crusts and toxic products by scrubbing the lid
margins daily with either commercially lid scrub or a cotton bud tipped in 25%
solution of baby shampoo.
b- Topical antibiotic ointment: fusidic acid or chloramphenicol.
c- Weak topical steroids: e.g. fluorometholone to control hypersensitivity to
exotoxins.
d- Tear substitutes.
Signs of posterior blepharitis (Meibomian seborrhea or meibomianitis):
a- Small oil globules capping the meibomian gland orifices.
b- Pressure on tarsal plate results in expression of copious amounts of
abnormal toothpaste like meibomian oil.
c- The posterior lid margin shows diffuse or localized inflammation centered
around meibomian gland orifices.
d- Blockage of the main meibomian ducts gives rise to secondary cystic
dilatation and occasionally meibomian cysts.
e- Frothy secretion at lid margins & ocular canthi.
Complications:
a- Tear film instability & dry eyes.
b- Papillary conjunctivitis plus punctuate epitheliopathy.
c- Internal hordeolum.
d- chalazia.
Treatment:
a- Systemic tetracyclines (Corynebacterium acnes) for 6-12 weeks: one of the
followings,
i- Tetracycline: Four times daily for 1 week, then twice daily for 5-11 weeks.
ii- Doxycycline: Twice daily for 1 week, then once daily for 5-11 weeks.
iii- Minocycline.
b- Erythromycin when (a) is contraindicated.

11
c- Lid hygiene.
d- Topical steroids.
e- Tear substitutes.
f- Warm compresses to melt solidified sebum and mechanical expression (to
evacuate meibomian glands from their contents).
Benign tumours
Capillary haemangioma
Capillary haemangioma (strawberry naevus), although rare, is one of the most
common tumours of infancy and presents shortly after birth. The female to male
ratio is 3:1. Eyelid haemangiomas have a predilection for the upper lid and may
have orbital extensions. Occasionally the lesion may also involve the skin of the
face and some patients have strawberry naevi on other parts of the body. It is
important to be aware of the association between multiple cutaneous lesions
and visceral haemangiomas. Histology shows proliferation of varying-sized
vascular channels in the dermis and subcutaneous tissue.
Signs: Unilateral, raised bright red lesion which blanches on pressure and may
swell on crying. A large lesion on the upper lid may cause mechanical ptosis.
Treatment:
1-Observation: Rx may not needed especially in small lesions that not causing
visual axis impairment & because the fact that 50% of cases resolved
spontaneously by 5 yrs of old & about 70% by 7yrs.
2-Systemic Beta blockers.
3-Steroids: systemically, topically & more effectively by local injection.
Pyogenic granuloma
A pyogenic granuloma is a fast-growing vascularized proliferation of
granulation tissue which is usually antedated by surgery, trauma or infection,
although some cases are idiopathic. Histology shows granulation tissue with
wide, thin-walled vascular channels and inflammatory cells infiltrating a loose
stroma.
Signs: A painful, rapidly growing, vascular polypoidal lesion that may bleed
following relatively trivial trauma.
Treatment: involves excision.
12
Xanthelasma
Xanthelasma is a common, frequently bilateral condition which is usually found
in middle-aged and elderly individuals. Xanthelasma (and corneal arcus) can be
associated with increased levels of serum cholesterol, especially in young
males. Histology shows lipid-laden histiocytes in the dermis.
Signs: Multiple yellowish subcutaneous plaques usually located at the medial
aspects of the eyelids.
Treatment: for cosmetic reasons is either by excision or preferably destruction
with a carbon dioxide or argon laser. Patients with the highest recurrence rate
are those with persistently elevated cholesterol levels.
Malignant tumours
Predisposing conditions:
General: old age, sun exposure, irradiation, immune suppression, smoking, fair
skin, Scandinavian ancestry.
Rare:Young patients who suffer from one of the following conditions may
develop eyelid malignancies;
1-Xeroderma pigmentosum is an AR disease characterized by skin damage on
exposure to natural sunlight, which gives rise to progressive cutaneous
pigmentation abnormalities , affected patients have a a great propensity to the
development of basal cell carcinoma (BCC), squamous cell carcinoma (SCC)
and melanoma, which may be multiple. Conjunctival malignancies have also
been reported.
2-Gorlin–Goltz syndrome (naevoid basal cell carcinoma syndrome) is a rare
AD disorder .
3 -Muir–Torre syndrome is a rare AD condition.
4-Bazex syndrome is an XLD condition.
5-Other predispositions include immunosuppression, prior retinoblastoma and
albinism.
Basal cell carcinoma
General features
BCC is the most common human malignancy and most frequently affects
elderly patients. The most important risk factors are fair skin, inability to tan
and chronic exposure to sunlight. Ninety per cent of cases occur in the head and
neck and about 10% of these involve the eyelid. BCC is by far the most
common malignant eyelid tumour, accounting for 90% of all cases. It most

13
frequently arises from the lower eyelid, followed in relative frequency by the
medial canthus, upper eyelid and lateral canthus. The tumour is slow-growing
and locally invasive but non-metastasizing. Tumours located near the medial
canthus are more prone to invade the orbit and sinuses, are more difficult to
manage than those arising elsewhere and carry the greatest risk of recurrence.
Tumours that recur following incomplete treatment tend to be more aggressive.
Histology:
The tumour arises from the cells that form the basal layer of the epidermis. The
cells proliferate downwards and characteristically exhibit palisading at the
periphery of a tumour lobule of cells.
Clinical types:
The main clinical features of epidermal cell malignancy are ulceration, lack of
tenderness, induration, irregular borders and destruction of lid margin
architecture.
1-Nodular BCC; is a shiny, firm, pearly nodule with small dilated blood
vessels on its surface.
2-Noduloulcerative BCC (rodent ulcer); has central ulceration, pearly raised
rolled edges and dilated and irregular blood vessels (telangiectasis) over its
lateral margins & with time it may erode a large portion of the eyelid.
3-Sclerosing BCC (morphoeic) is less common and may be difficult to
diagnose because it infiltrates laterally beneath the epidermis as an indurated
plaque. The margins of the tumour may be impossible to delineate clinically
and the lesion tends to be much more extensive on palpation than inspection.
4-Other types not usually found on the lid are cystic, adenoid, pigmented and
multiple superficial.
Squamous cell carcinoma
General features
SCC is a much less common, but typically more aggressive tumour than BCC
with metastasis to regional lymph nodes in about 20% of cases. Careful
surveillance of regional lymph nodes is therefore an important aspect of initial
management. The tumour may also exhibit perineural spread to the intracranial
cavity via the orbit. SCC accounts for 5–10% of eyelid malignancies. The
tumour has a predilection for the lower eyelid and the lid margin.

14
Histology:
The tumour arises from the squamous cell layer of the epidermis. It is
composed of variable-sized groups of atypical epithelial cells with prominent
nuclei and abundant eosinophilic cytoplasm within the dermis. Tumours may
show characteristic keratin ‘pearls’ and intercellular bridges (desmosomes).
Clinical types:
The clinical types are variable and there are no pathognomonic characteristics.
The tumour may be indistinguishable clinically from a BCC but surface
vascularization is usually absent, growth is more rapid and hyperkeratosis is
more often present.
1-Nodular SCC is characterized by a hyperkeratotic nodule which may develop
crusting erosions and fissures.
2-Ulcerating SCC has a red base and sharply defined, indurated and everted
borders but pearly margins and telangiectasia are not usually present.
3-Cutaneous horn with underlying invasive SCC
Sebaceous gland carcinoma
General features
Sebaceous gland carcinoma (SGC) is a slowly-growing tumour which most
frequently affects the elderly, with a predisposition for females. It usually arises
from the meibomian glands, although on occasion it may arise from the glands
of Zeis or from sebaceous glands in the caruncle. In contrast to BCC and SCC,
the tumour occurs more commonly on the upper eyelid where meibomian
glands are more numerous. Sometimes there is simultaneous involvement of
both lids on one side, probably due to intraepithelial spread or to spontaneous
development of multiple primaries. The clinical diagnosis of SGC is frequently
difficult because, in its early stages, external signs of malignancy may be subtle
so that the tumour may resemble a chalazion or blepharitis. However, the
presence of yellowish material within the tumour is highly suggestive of SGC.
Histology
The tumour consists of lobules of cells with pale foamy vacuolated lipid-
containing cytoplasm and large hyperchromatic nuclei.
Clinical types:
Although SGC does not have a characteristic clinical appearance it may present
with the following:

15
1-Nodular SGC presents as a discrete, hard nodule, most commonly within the
upper tarsal plate, that may exhibit yellow discoloration due to the presence of
lipid. Because the lesion may masquerade as a chalazion, it is recommended
that any ‘chalazion’ of an unusual consistency should undergo full-thickness
resection and histological examination.
2-Spreading SGC infiltrates into the dermis and causes a diffuse thickening of
the lid margin that may result in loss of lashes and be mistaken for ‘chronic
blepharitis’.
3-Pagetoid spread refers to extension of the tumour within epithelium including
the palpebral, forniceal or bulbar conjunctiva. This may lead to the mistaken
diagnosis of an inflammatory chronic conjunctivitis.
Treatment of malignant tumours
1-Biopsy
The two types of biopsy are (a) incisional, using a blade or a biopsy punch, in
which only part of the lesion is removed to allow histological diagnosis, and (b)
excisional, in which the entire lesion is removed and a histological diagnosis
made.
2-Surgical excision:
Surgical excision aims to remove the entire tumour with preservation of as
much normal tissue as possible. Most small BCCs can be cured by excision of
the tumour together with a 2–4 mm margin of clinically normal tissue. More
radical surgical excision is required for large BCC and aggressive tumours such
as SCC, SGC and melanoma. It may not be possible to close the defect at the
time of initial removal, but it is necessary to ensure complete clearance of
tumour prior to undertaking any reconstruction.
3-Radiotherapy:
The recurrence rate following irradiation is higher than after surgery, and
radiotherapy does not allow histological confirmation of tumour eradication. So
Indicated for Small BCC which does not involve the medial canthal area in
patients who are either unsuitable for or refuse surgery.
4-Cryotherapy:
May be considered for small superficial BCC.
-