Bone functions
1- support2- protection
3- leverage
4- minerals reservoir
Metabolic bone diseases
1- the matrix2- bone mineral
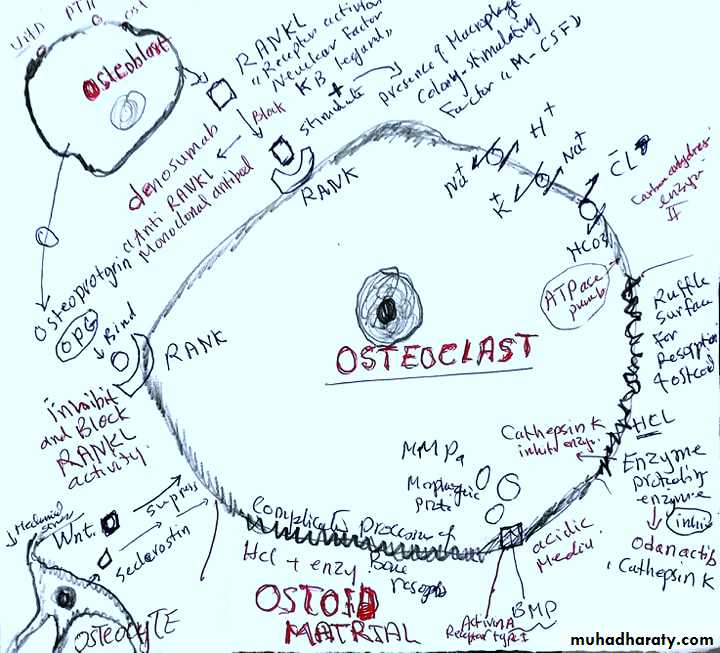
3- bone cells
Bone composition
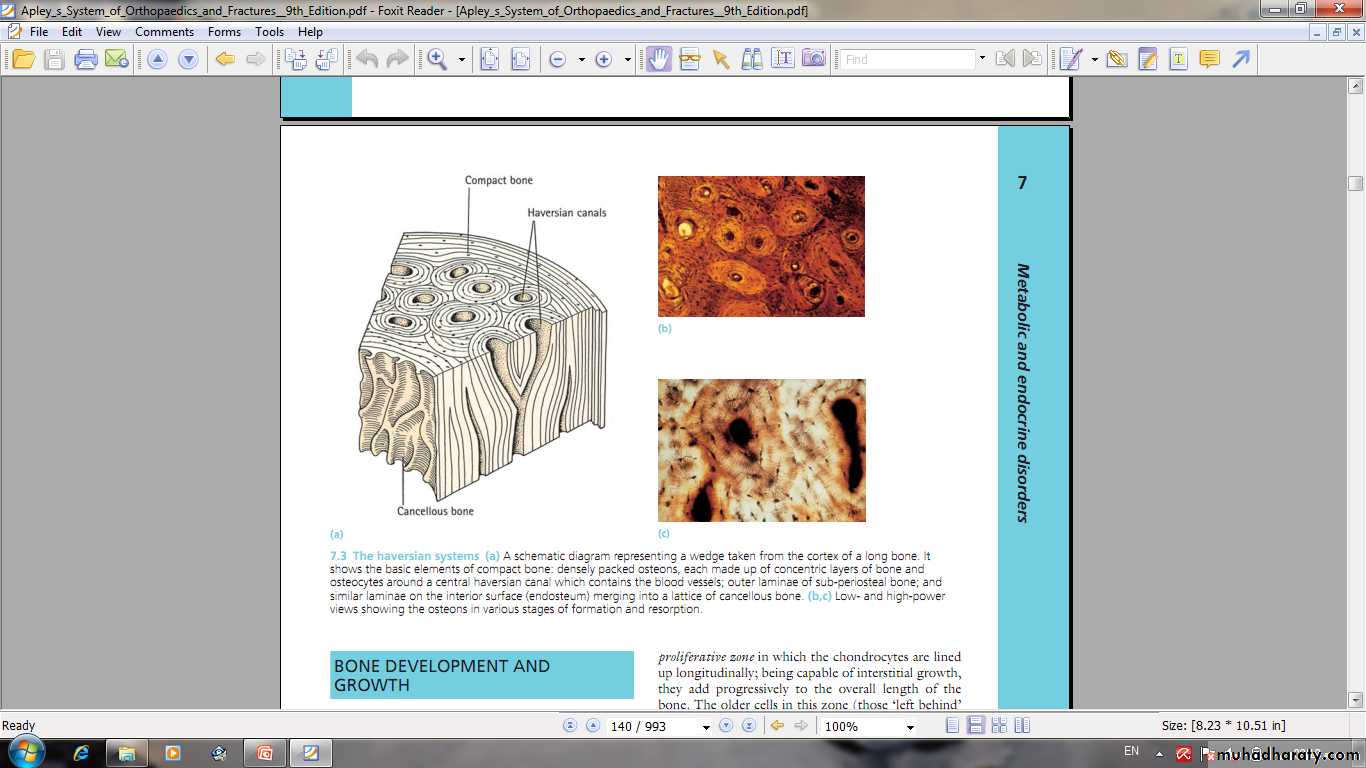
Compact boneCancellous bone
Haversian system
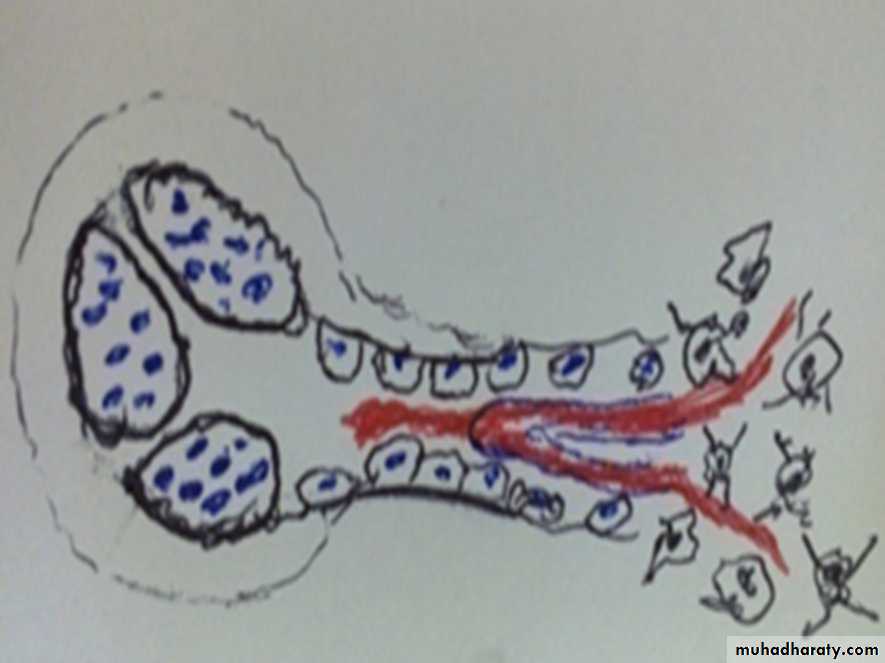
Bone structure
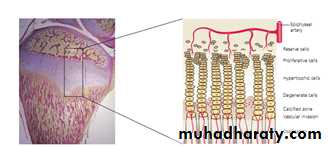
Endochondral ossification
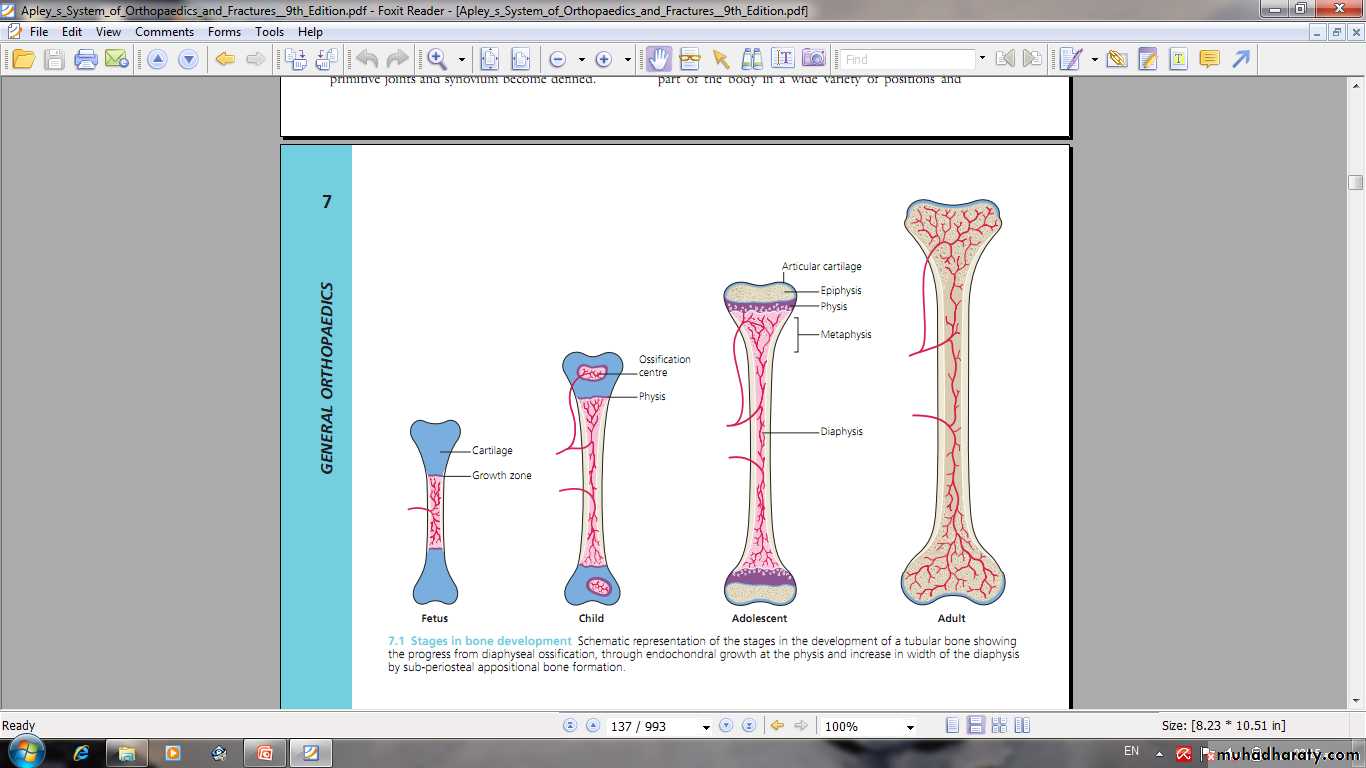
Epiphyseal growth plate
Periosteal new bone formation
Intramembranous ossificationBone formation and resorption.Bone remodelling
1- calcium.
2- phosphorus.3- magnesium and fluoride.
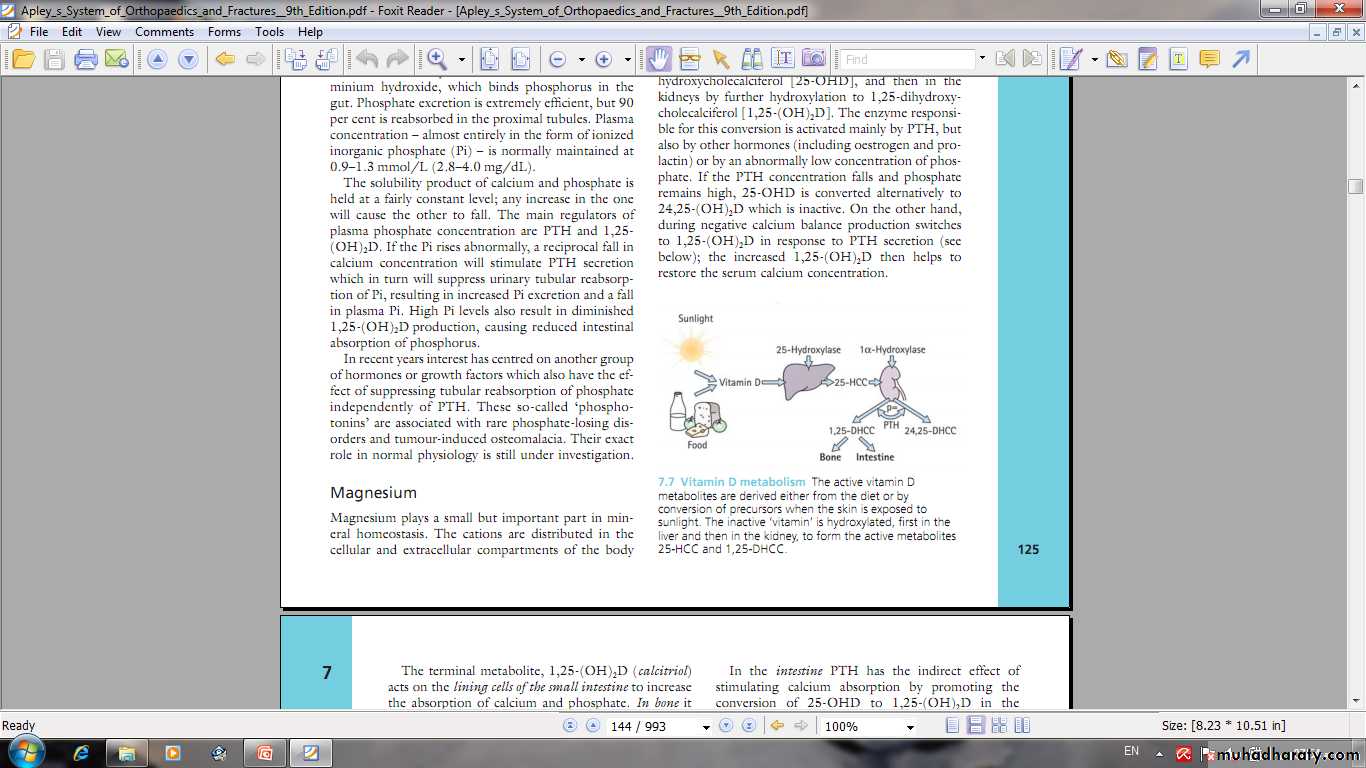
4- Vitamin D .
5- Parathyroid hormone.
6- calcitonin.
7- glucocorticoids, gonadal hormone, thyroxine , growth hormone.
8- mechanical factors.
9- electrical stimulation and other factors.
Minerals and Factors affect bone metabolism
Wolff’s Law: Wolff’s Law is beautifully demonstrated
in the trabecular pattern at the upper end of the femur.The thickest trabeculae are arranged along the trajectories
of greatest stress.
1- Early onset menopause.
2- Malnutrition and ill health
3-Lack of Vit D, calcium and phosphate.
4- Chronic illness.
5- High consumption of alcohol.
6- Smoking.
7- Inactivity.
8- Drugs :
corticosteroids,
cytotoxic, anti-inflammatory drugs, diuretics, anticoagulants, thyroid hormone, antiepileptic's.
Factors adversely affecting bone mass
It is a clinical disorder characterized by an abnormally low bone mass and defects in bone structure, render the bone fragile.
or
A state in which bone is fully mineralized but its structure is abnormally porous and its strength is less than normal person of that age and sex
OSTEOPOROSIS Reduction of normally mineralized bone mass per volume.
It may result from increased bone resorption or
decrease bone formation or both.Osteopenia: bone which appears to be less dense than normal X-ray.
Any density reduction in DEXA more than 2.5 standard deviation define as osteoporosis.
Between 1-2.5 name osteopenia
OSTEOPOROSIS
1- Osteoporosis is one of the most serious global disease and will increase due to increased aging.
2- Osteoporosis is a problem in both genders.
3- Osteoporosis may primary or secondary.
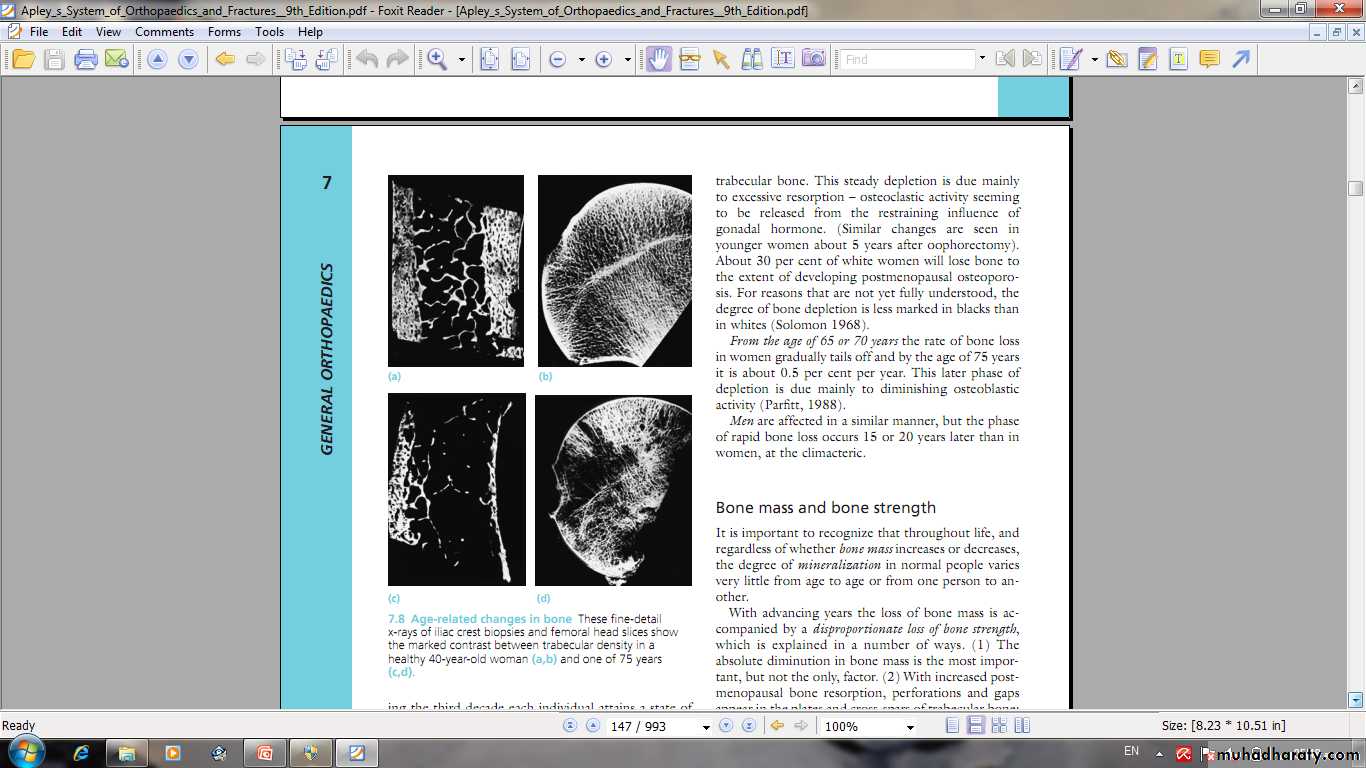
Primary osteoporosis may be postmenopausal or senile .
4- Osteoporosis is common cause of fractures especially femoral neck fractures , vertebral fractures and distal radial fractures .
5- Bone mineral density commonly measured by dual-energy X-ray absorptiometry ( DEXA)
Osteoporosis
Malnutrition .Hypercortisonism ( Cushing’s disease).
Gonadal hormone insufficiency.
Hyperthyroidism and hyperparathyroidism.
Multiple myeloma & carcinomatosis.
Drugs ( steroids, heparin, antiepileptic, cytotoxic, ….).
Alcohol and smoking.
Immobilization.
Chronic disease ( renal failure, TB, rhumatic disaeses... )
Other factors
Secondary osteoporosis
Hormone therapy.
Bisphosphonates Bisphosphonates is the first-line drugs for treating postmenopausal women with osteoporosis, Alendronate and risedronate reduce risk of both vertebral and nonvertebral fractures.Parathyroid hormone: Teriparatide (PTH 1-34) is reserved for treating women at high risk for fracture, including those with very low bone mineral density (BMD) with a previous vertebral fracture. PTH improves BMD and reduces the risk of vertebral and non-vertebral fractures. Dosage requirements of daily subcutaneous injections may limit use.
Selective oestrogen receptor modulators (SERMs) Raloxifene.
Denosumab This is an antibody to RANKL
Fluoride, calcium, and vitamin D, calcinotin.
Fracture treatment
Treatment of osteoporosis
Osteoporosis
Bone tissue throughout the skeleton is abnormally less calcified and therefore soften ( Osteomalacia).Rickets and Osteomalacia is same disease.
Osteomalacia and ricketsinadequate mineralization of bone





Osteoporosis and Osteomalaciacommon in aging women, prone to pathological fractures, and decreased bone density.
Osteomalacia
-------------------------------
Unwell
Generalized chronic ache
Muscles weak.
Losser’s zone
decreased serum phosphate
elevated serum alka. Phosphatase.
Ca × p < 2.4 mmol/ L
Osteoporosis
--------------
Well
Pain after fractures
Muscles normal.
No Losser's zone
Normal serum phosphate
Normal serum alka.
Phosphatase
Ca × p > 2.4 mmol/ L
Treatment of the cause.
Treatment of pathological fractures.Osteomalacia treatment
Excessive secretion of PTH.
May be primary , secondary, or tertiary.PTH- enhance calcium conservation resulting in hypercalcaemia and hypercalciuria and
Hyperphosphouria.Bone resorption manifest by ostitis fibrosa cystica and subperiosteal resorption.
hyperparathyroidism

hyperparathyroidism
Clinical features1- features of hypercalcaemia.
2-polyuria and renal disorders
3- bone pain and pathological fractures.
Treatment
1- treatment of hypercalcemia.
2- surgery.
This disease characterized by increased bone turnover and enlargement and thickening of bone, but internal architecture is abnormal and bone is usually brittle.
Paget’s disease
Paget’s disease
Complications1- fractures.
2- osteoarthritis
3- nerve compression and spinal stenosis.
4- bone sarcoma.
5- high cardiac output failure.
6- hypercalcaemia in immobilization.
Treatment
1- calcitonin.
2- Bisphosphonate.3- surgery