1
Operative
Caries diagnosis Dr Maan
The process of caries diagnosis involves both risk assessment and the
application of diagnostic criteria to determine the disease state.
The primary objectives of caries diagnosis are to identify those lesions
that
require surgical (restorative) treatment
,
those that require non-
surgical treatment,
and those persons who are at high risk for
developing carious lesions.
Knowing which patients are at high risk for developing caries provides an
opportunity to implement specific preventive strategies that may
prevent canes. These strategies are specific to high-risk individuals and
are not intended for all patients (Box 3-1). However, for patients at low
risk for canes, preventive measures may be limited to oral hygiene.
Caries risk assessments
During the initial history, examination and treatment for every patient, it
is important to assess the risk of developing further carious lesions or
progression of existing lesions. This procedure is termed caries risk
assessment which is based on the following factors:
1.Caries experience
- The extent and number of previous restorations
(indicator of past
disease)
- The extent and number of new lesions .
- The progression of new lesions.
2.Fluoride use - type and frequency. • Oral hygiene and the extent of
plaque.

2
3.Dietary factors - eating habits, number of main meals, snacks,
frequency of carbohydrate intake.
4.Bacterial activity- the presence and amount of cariogenic bacteria,
specifically Lactobacillus and Streptococcus mutans.
5. Saliva - both the amount (quantity) and buffering capacity (quality).
6.Socio-economic status - to evaluate the patient for compliance. Caries
tends to be a disease of deprivation and is more prevalent in patients
with lower socio-economic status.
Assessment tools for caries diagnosis
Patient history:
knowing factors through patient history can assist in caries diagnosis
such factors include age, gender, fluoride exposure, smoking habits,
alcohol intake, medications, dietary habits, economic and educational
status, and general health (case sheet).
Clinical Examination or Visual examination: General information
regarding inadequate salivary functioning, plaque accumulation,
inflammation of soft tissues, poor oral hygiene, cavitated lesions, and
existing restorations also are instructive in determining potential risk to
caries development (light source, mirror, and explorer). The tooth must
be clean, dry and well illuminated when carrying out a visual
examination.
Enhanced visual examination: (Transillumination, Fibre-optic
transillumination, Magnification, Dyes)
Radiographic Assessment: Dental radiographs provide useful
information in diagnosing carious lesions (interproximal caries).
Nutritional Analyses: Frequent exposure to sucrose increases the
likelihood of plaque development by the more cariogenic MS organisms.

3
Salivary Analyses: Analyzing saliva may provide important information
about appropriateness of secretion rates and buffering capacity as well
as numbers of both MS and lactobacilli.
Treatment of advanced carious lesion:
Removal of the bacterial infection is an essential part all operative
procedures. It is not necessary to remove all the dentin that has been
affected by the caries process.
It is not necessary to remove all the dentin that has been affected by the
caries process. In operative procedures, it is convenient to term dentin
as either infected, and thus requires removal, or affected, which does
not require removal.
Affected dentin is softened. Demineralized dentin that is not yet invaded
by bacteria (zones 2 and 3).
Infected dentin (zones 4 and 5) is both softened and contaminated with
bacteria.
Caries treatment
Early restorative intervention should be avoided if possible, why?
1. As tooth preparation is irreversible and commits the tooth to the
restorative cycle.
2. All restorations fail at some time and require either repair or
replacement, resulting in yet another insult to the tooth tissues.
3. This repeated insult can ultimately lead to the loss of the tooth.
Caries prevention
Diet
Decreasing the frequency of fermentable carbohydrate consumption
and elimination or substitution is essential.
Fluoride
Fluoride has produced the following reductions in caries.

4
Oral hygiene
A well maintained oral hygiene regime helps to maintain the bacterial
balance within the oral cavity.
In high risk caries development patient, the treatment should consist of
both restorative and preventive measures. If patient has cavitated
carious lesions should be restored first then fissure sealant and fluoride
should be applied. Patient education is important in treatment success
to increase motivation to obtain good oral health.
Principles of operative intervention:
In contrast to Black's principles of cavity preparation, which included the
establishment of outline form including extension for prevention, the
development of resistance and retention form, creation of convenience
form, the treatment of residual caries, the finishing of cavity margins
and cavity toilet, now the general principles of tooth preparation are
determined by:
• The nature and extent of the lesion.
• The quantity and quality of the tooth tissue remaining following
preparation.
• Functional load.
• The nature and properties of the restorative system to be used.
To be able to prepare teeth efficiently and effectiveness is essential to
understand the processes of the diseases of teeth, have a defined
working knowledge of tooth anatomy, the structure and properties of
the tooth tissues and pulp biology, and have a clear understanding of the
basic principles of occlusion. In addition, one must understand the mode
of action, functions and limitations of the instrumentation used to shape
and fashion enamel and dentine in the oral environment.

5
Tooth preparation involve the following stages:
Gaining access In order to remove caries, create the required form of
reparation, and enable restorative materials to be placed, adapted and
contoured to restore form and function, it is generally necessary initially
to cut through and then cut away part of the enamel of the tooth to be
treated.
Removal of caries With access established, caries is removed, first from
around the amelodentinal junction and then, working apically, towards
the areas overlying the pulp. When caries extends down to a vital pulp,
one should aim to remove all soft, stained, infected dentine leaving
either some stained but firm dentine or possibly some slightly softened,
unstained dentine protecting the pulp from exposure. The rationale for
this is that affected dentine (rather than infected dentine) may be
retained and remineralised with the use of a therapeutic liner. It is
common to experience difficulties in distinguishing between dentine
that should be removed, and that which should be left.
Development of final form
it is necessary to consider the biological, functional mechanical
demands that will be placed on the final tooth restorative 'system'.
The following should be considered:
a. Minimization of the effect of preparation on tooth strength
b. Choice of restorative material
c. Integrity of the remaining tooth structure
d. Placement of margins
e. Planning of the retentive form
f. Integrity of the restoration
6
ALTERNATIVE PREPARATION METHODS :
1. Chemomechanicalcaries removal (Carisolv)
Application of the isotonic solution on tooth structure that lead to
softening of the carious lesion then facilitating excavation via specially
designed hand instrument. Through this technique removal of sound
tooth structure will be reduced less irritation to the pulp and painless
procedure.
2. Sonic preparation
Sonic instruments have been used within the field of dentistry principally
for scaling and root surface debridement.The newer sonic handpieces
allow for interchangeable tips and multiple applications, such as
minimally invasive caries therapy, cavity preparations, endodontics,
periodontics.
3. Air abrasion
Steam of aluminum oxide particles with the aid of compressed air that
particle will strike tooth under high power and velocity .
4. Lasers The most commonly used device in operative dentistry and for
cavity preparation is Er:YAG.

7
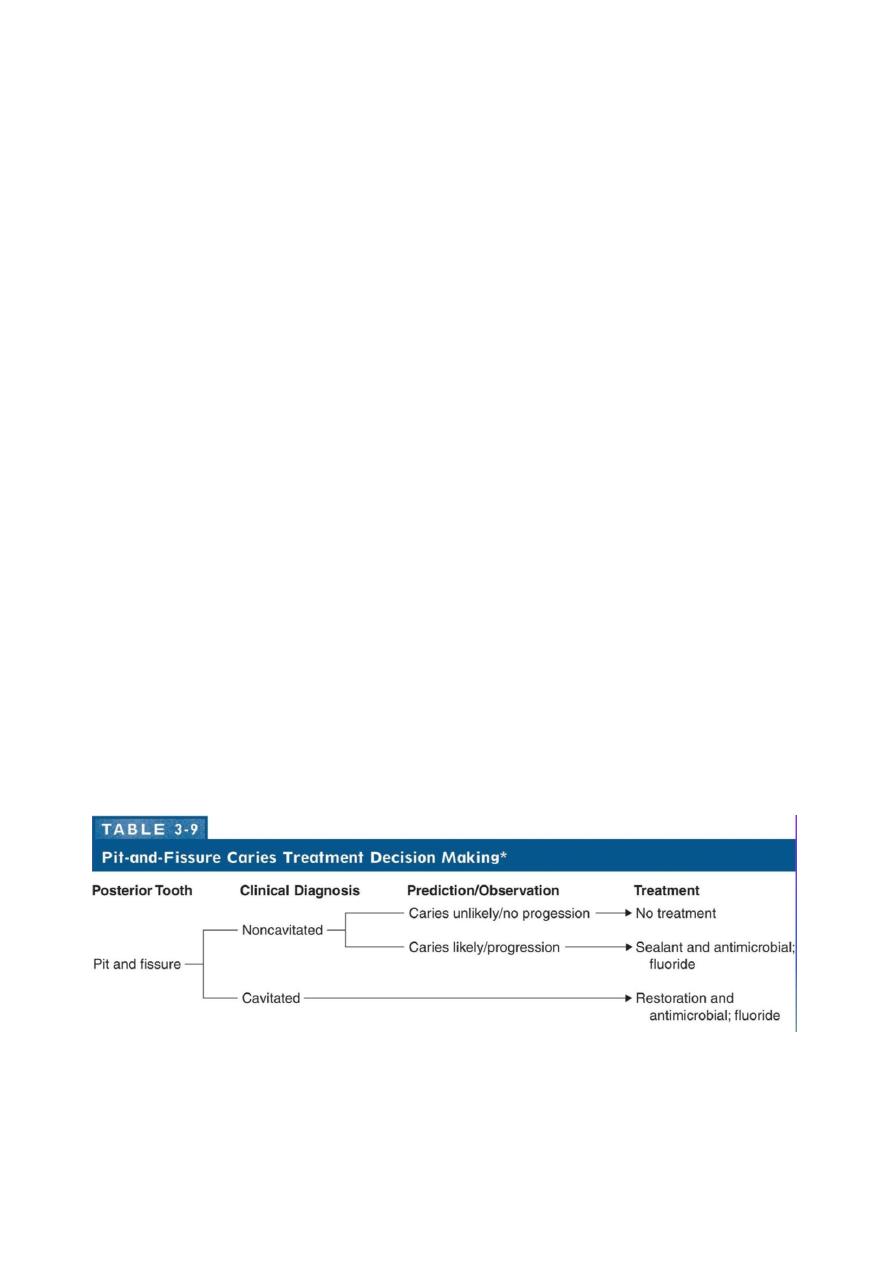
Noncavitated (caries-free):
• No radiolucency below occlusal enamel
• Deep grooves may be present
• Superficial staining may be present In grooves
• Mechanical binding of explorer may occur
Cavitated (diseased):
extensive enamel demineralization has lead to destruction of the walls
of the pit or fissure and bacterial Invasion has occurred
• Chalkiness of enamel on walls and base of pit or fissure
• Softening at the base of a pit or fissure
• Brown-gray discoloration under enamel adjacent to pit or fissure
• Radlolucency below occlusal enamel