
1
Operative
Dr Maan
Histopathology of caries
Enamel caries
Histology of enamel
Characteristic of enamel caries
Zones of the lesion
Dentin caries
Histology of dentin
Characteristic of dentin caries
Zones of the lesion
Histology of enamel: Enamel is composed of very tightly packed
hydroxyapatite crystallites, organized into long columnar rods (prisms).
The rods are somewhat key-shaped in cross-section.
Both the striae of Rebus and the inherent spaces in prism boundaries
provide sufficient porosity to allow movement of water and small ions,
such as hydrogen ions.
Characteristic of enamel caries
On clean, dry teeth, the earliest evidence of caries on the smooth
enamel surface of a crown is a white spot.
White spots are chalky white, opaque areas that are revealed only when
the tooth surface is desiccated, and are termed incipient caries.

2
Care must be exercised to distinguish white spots of incipient caries
from developmental white spot hypocalcifications of enamel.
Incipient caries will partially or totally disappear visually when the
enamel is hydrated (wet), while hypocalcified enamel is relatively
unaffected by drying and wetting.
It has been shown that incipient caries of enamel can remineralize.
Calcium and phosphate ions from saliva can then penetrate the enamel
surface and precipitate in the enamel lesion.
Remineralized (arrested) lesions can be observed clinically as intact, but
discolored, usually brown or black spots These discolored,
remineralized, arrested caries areas are intact and are more resistant to
subsequent caries attack than the adjacent unaffected enamel.
Zones of the enamel lesion:
(1) translucent zone.
(2) dark zone
(3) body of the lesion
(4) surface zone
A, Cross-section of small carious lesion in enamel examined in quinoline with
polarized light (x100). Advancing front of lesion appears as a dark band below body
of lesion.
B, Same section after exposure to artificial calcifying solution examined in quinoline
and polarized light. Dark zone (DZ) covers a much greater area after remineralization
has occurred (x100).
C, Schematic diagram of Fig. 3-28A and B. Left side indicates small extent of zones 1
and 2 before remineralization. Small circles indicate relative sizes of pores in each
zone. Right side indicates increase in zone 2, the dark zone, after remineralization.
This micropore system must have been created where previously the pores were
much larger.
3
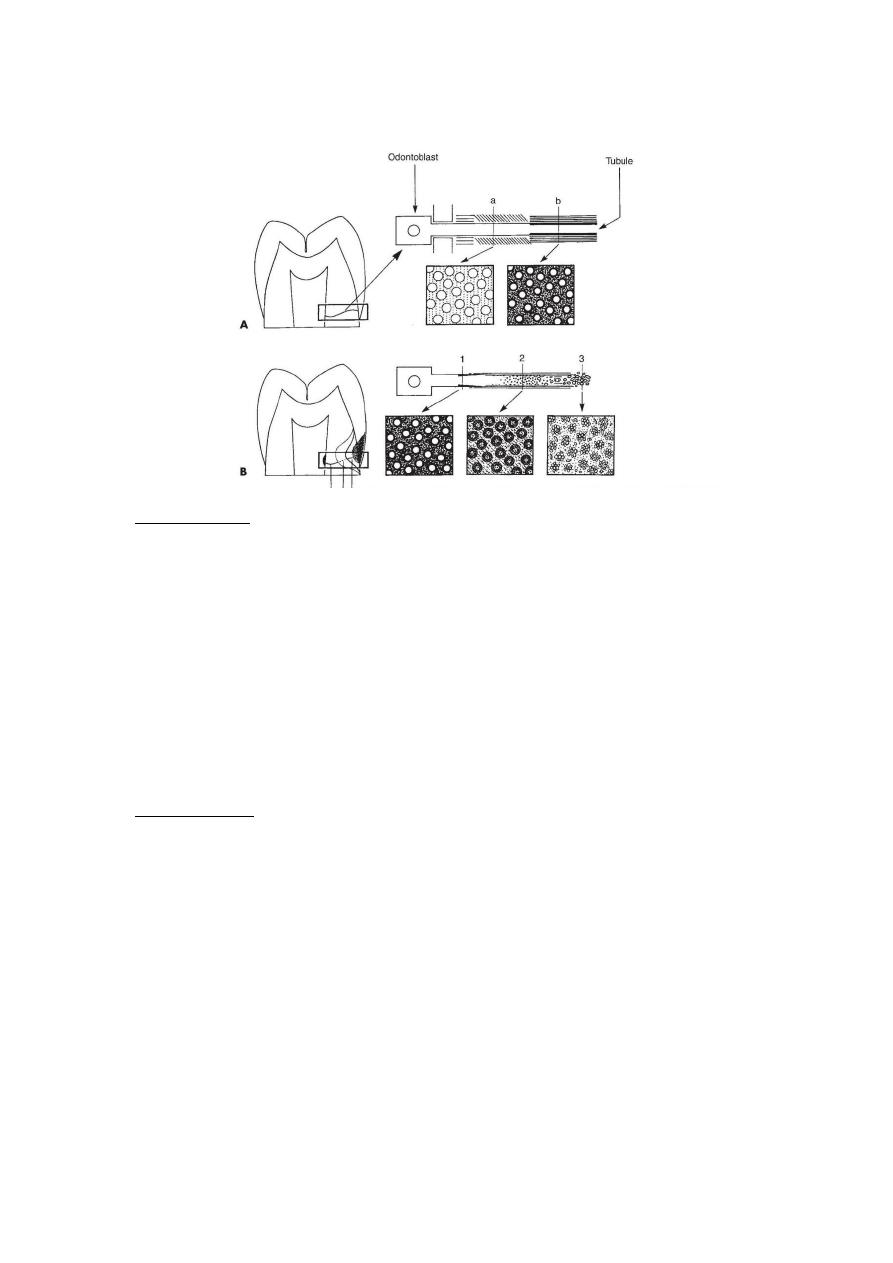
Histology of dentin
Normal dentin. A, has characteristic tubules that follow a wavy path from the
external surface of the dentin, and grows inward. The more recently formed
dentin near the pulp (a) has large tubules with little or no peritubular dentin
and calcified intertubular dentin filled with collagen fibers. The older dentin,
closer to the external surface
(b), is characterized by smaller, more widely separated tubules and a greater
mineral content in the intertubular dentin.
Horizontal lines indicate predentin; diagonal lines indicate increasing density
of minerals; darker horizontal lines indicate densely mineralized dentin and
increased thickness of peritubular dentin.
Carious dentin B, The most superficial infected zone of carious dentin (3) is
characterized by bacteria filling the tubules and granular material in the
intertubular space. Pulpal to (below) the infected dentin is a zone where the
dentin appears transparent in mounted whole specimens. This zone (2) is
affected (not infected) carious dentin and is characterized by loss of mineral in
the intertubular and peritubular dentin. Many crystals can be detected in the
lumen of the tubules in this zone. Normal dentin (1) is found pulpal to (below)
the transparent dentin.
4
Characteristic of dentin caries
Progression of caries in dentin is different from progression of caries
enamel.
-Dentin contains much less mineral and possesses microscopic tubules
that provide a pathway for the ingress of acids and egress of mineral.
-The dentinoenamel junction (DEJ) has the least resistance to caries
attack and allows rapid lateral spreading once caries has penetrated the
enamel. Because of these characteristics, dentinal caries is V-shaped in
cross-section with a wide base at the DEJ and the apex directed pulpally.
-Caries advances more rapidly in dentin than in enamel because dentin
provides much less resistance to acid attack because of less mineralized
content.
-Caries produces a variety of responses in dentin, including pain,
demineralization and remineralization.
-Once bacterial invasion of the dentin is close to the pulp, toxins and
possibly even a few bacteria enter the pulp, resulting in inflammation of
the pulpal tissues.
-The pulp-dentin complex reacts to caries attacks by attempting to
initiate remineralization and blocking off the open tubules. These
reactions result from odontoblastic activity and the physical process of
demineralization and remineralization.
-Dentin responds to the stimulus of its first caries demineralization
episode by deposition of crystalline material in both the lumen of the
tubules and the interlobular dentin of affected dentin.
Hypermineralized areas may be seen on radiographs as zones of
increased radiopacity (often S-shaped following the course of the
tubules) ahead of the advancing, infected portion of the lesion. This
repair only occurs if the tooth pulp is vital.

5
Three levels of dentinal reaction to caries:
(1) reaction to slowly advancing caries lesion ,
a long-term, low-level of acid Sclerotic dentin formation occurs
ahead of the demineralization front of a slowly advancing lesion and
may be seen under an old restoration.
These areas are harder (more mineral content than normal dentin),
denser, less sensitive, and more protective of the pulp against
subsequent irritations. Sclerosis also resulting from aging (
physiologic dentin sclerosis); sclerosis resulting from a mild irritation
( reactive dentin sclerosis).
(2) reaction to a moderate-Intensity caries ;
The pulp may be irritated sufficiently from high acid levels or
bacterial enzyme production to cause the formation (from
undifferentiated mesenchymal cells) of replacement odontoblasts
(secondary odontoblasts).
These cells produce reparative dentin or tertiary dentin or
reactionary dentin
(3) reaction to severe, rapidly advancing caries;
Acute, rapidly advancing caries with very high levels of acid
production overpowers dentinal defenses and results in infection,
abscess, and death of the pulp.
6
Primary dentin: The dentin forming the initial shape of the tooth and is
usually completed 3 years after tooth eruption.
Secondary dentin: It formed after the primary dentin, as dentin
deposition continues at a reduced rate even without stimuli.
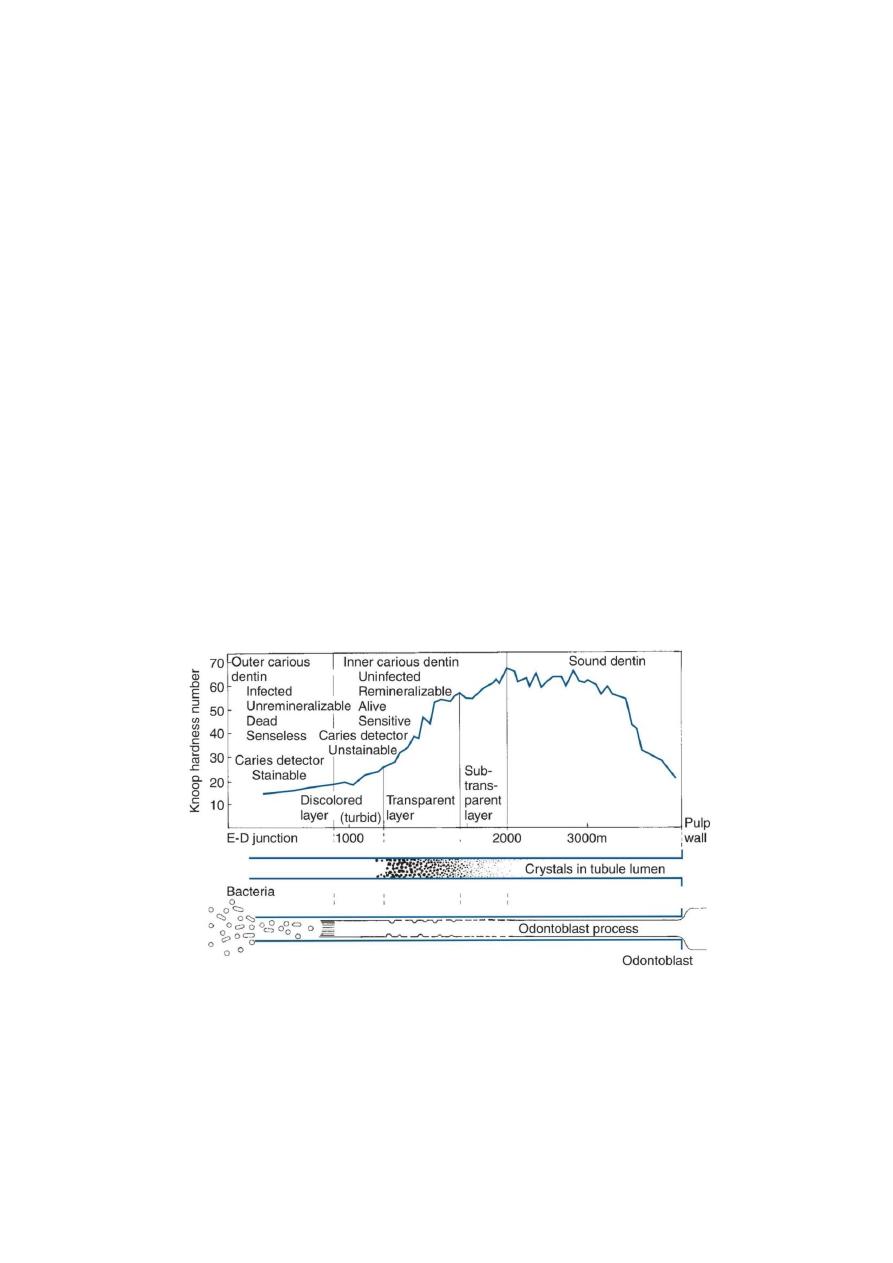
Zones of the dentin lesion:
Zone 1 normal dentin (no bacteria)
Zone 2 sub-transparent dentin (no bacteria, demineralized zone, and
remineralizable)
Zone 3 transparent dentin (no bacteria, crystals in tubule, also
remineralizable)
Zone 4 turbid dentin (bacterial invasion, not remineralizable)
Zone 5 infected dentin (bacterial invasion, decomposed dentin, no
mineral or collagen)