Association and causation
Dr. Sijal Fadhil Farhood AL-joborae
F.I.C.M.S community (Baghdad)
M.Sc. Community (Nahrain)
M.B.Ch.B (Babylon University)

introduction
In previous lectures we studied the designs of
epidemiologic studies that are used to determine whether
an association exists between an exposure and a disease
,We then addressed different types of risk measurement
that are used to quantitatively express an excess in risk.
If we determine that an exposure is associated with a
disease.
The next question is whether the observed association
reflects a causal relationship????
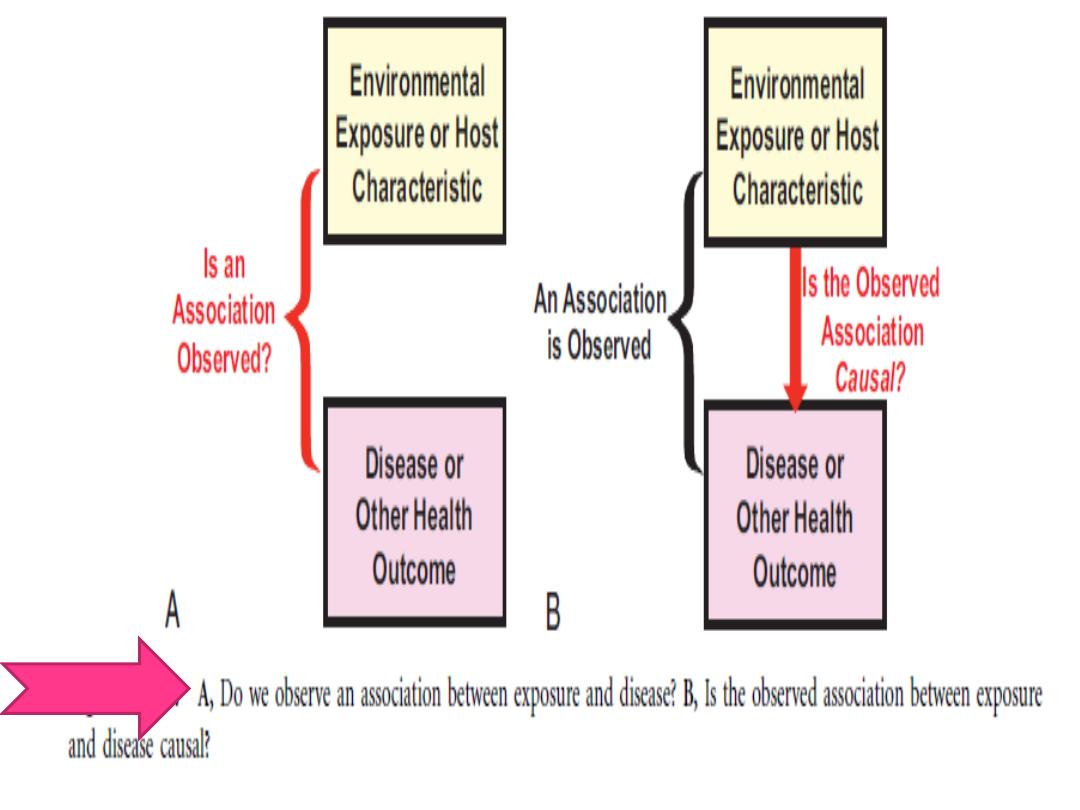
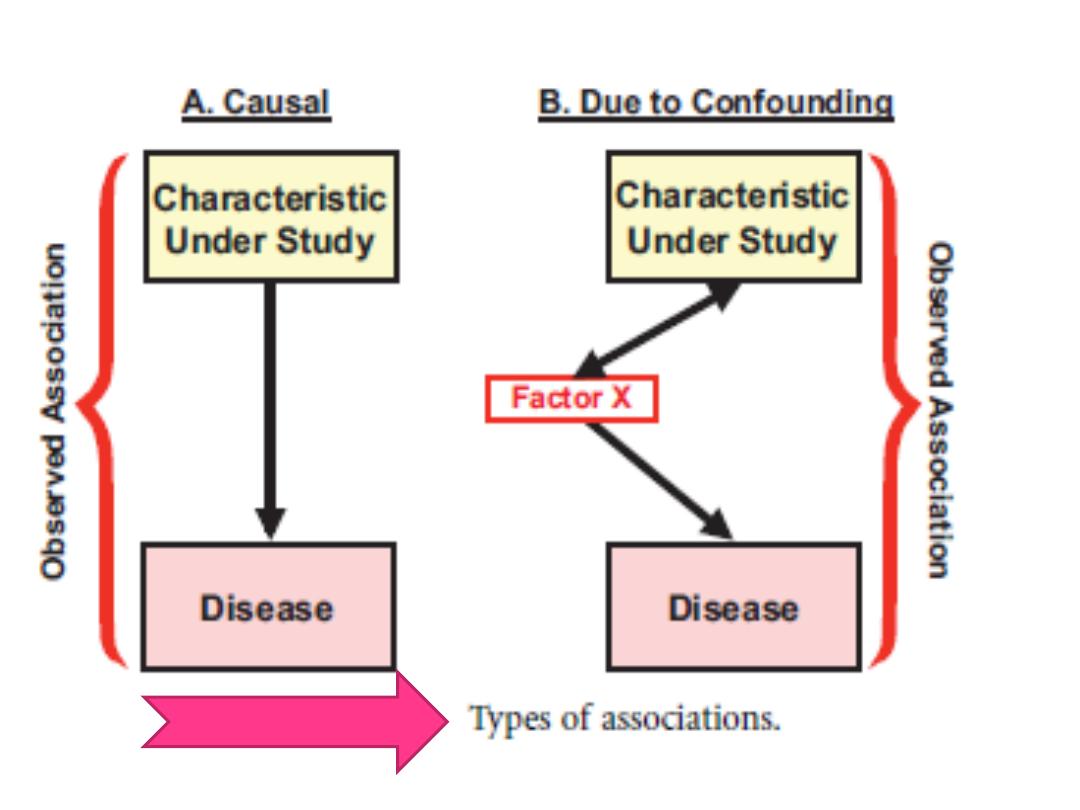
TYPES OF ASSOCIATIONS
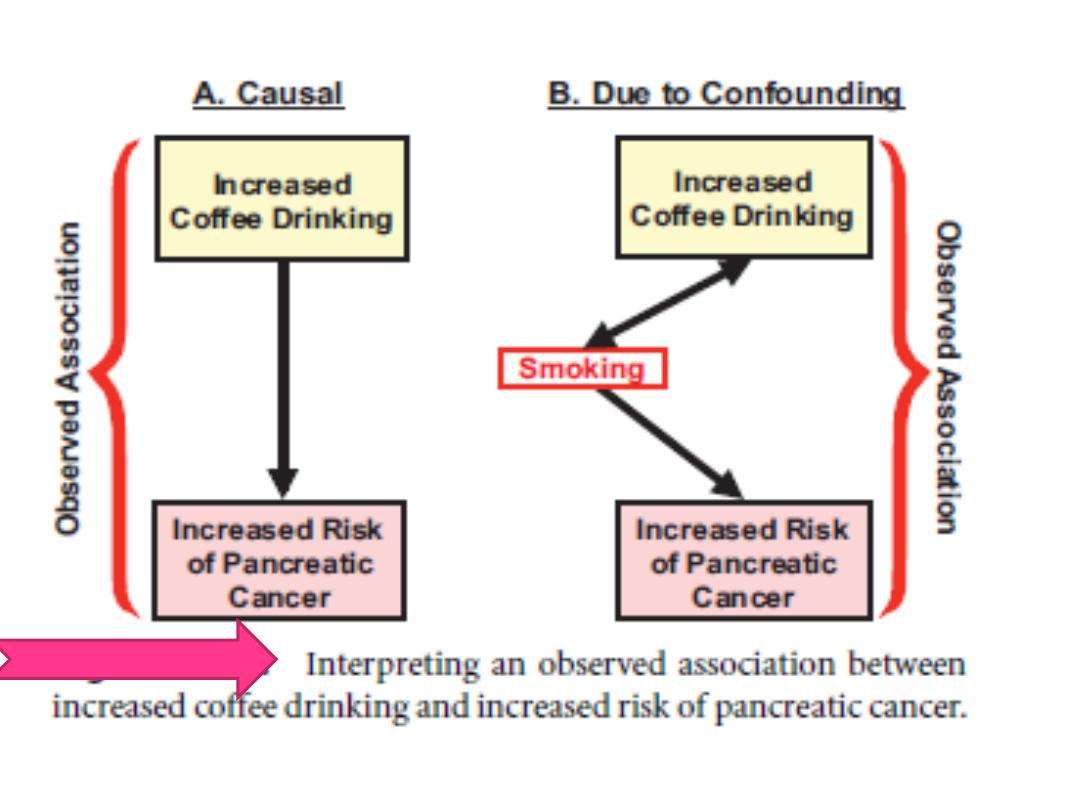
Real or Spurious Associations
Interpreting real association:
A :shows a causal association: we observe an association of
exposure and disease and the exposure induces development of
the disease.
B:shows the same observed association of exposure
and disease, but they are associated only because they are both
linked to a third factor, designated here as factor X. This
association is a result of confounding and is non-causal.
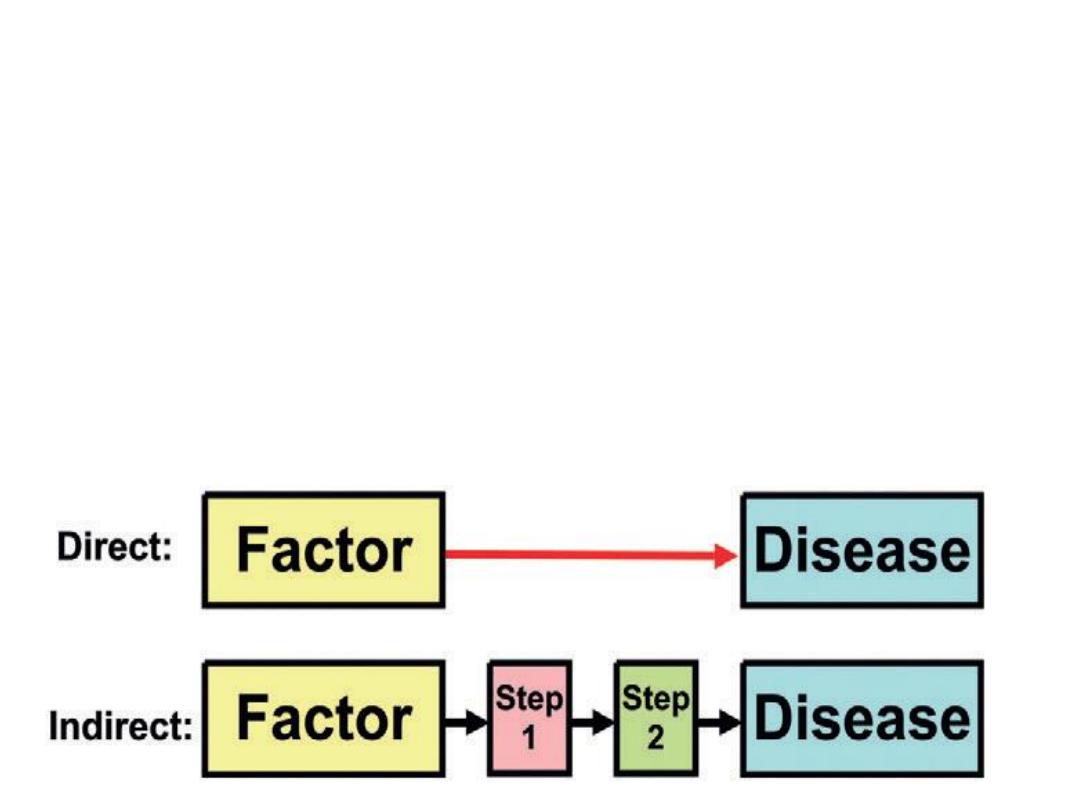
TYPES OF CAUSAL
RELATIONSHIPS
•
A causal pathway can be either
direct
or
indirect
In
direct
causation, a factor directly causes a disease without any
intermediate step. In
indirect
causation, a factor that causes a
disease, but only through an intermediate step or steps. In
human
biology, intermediate steps are virtually always present in any
causal process.

If a relationship is causal; four types of causal relationships are
possible:
(1) necessary and sufficient.
(2) necessary, but not sufficient.
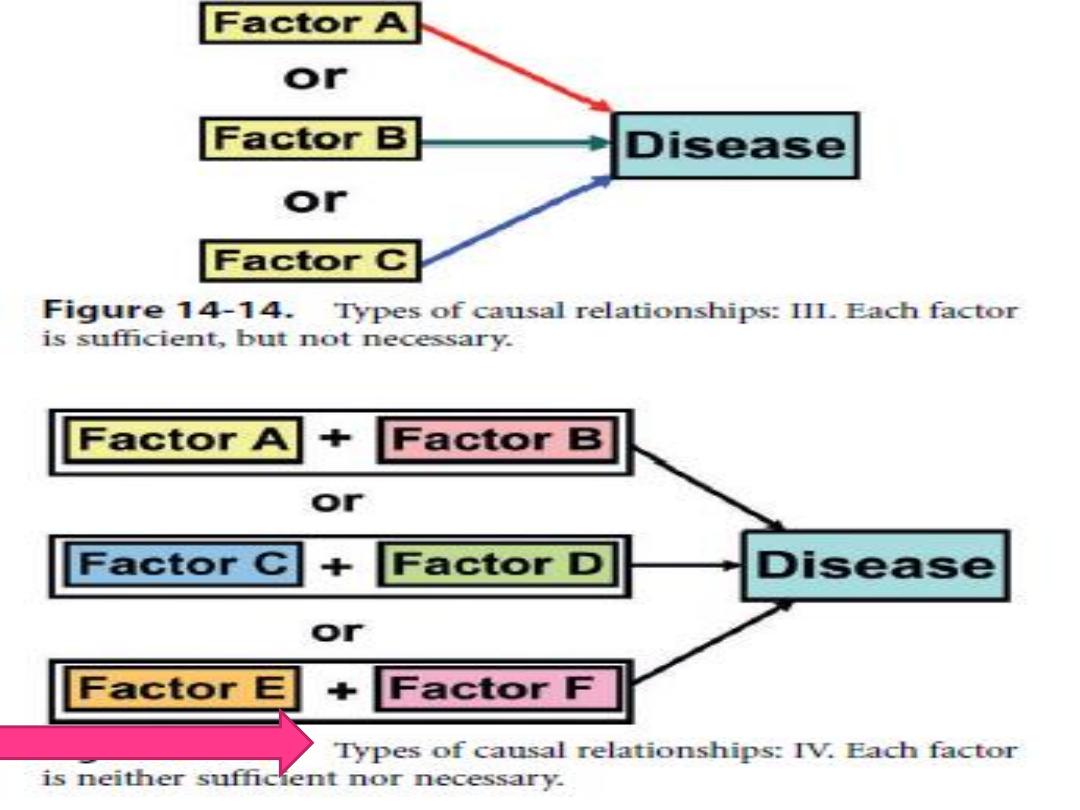
(3) sufficient, but not necessary.
(4) neither sufficient nor necessary.
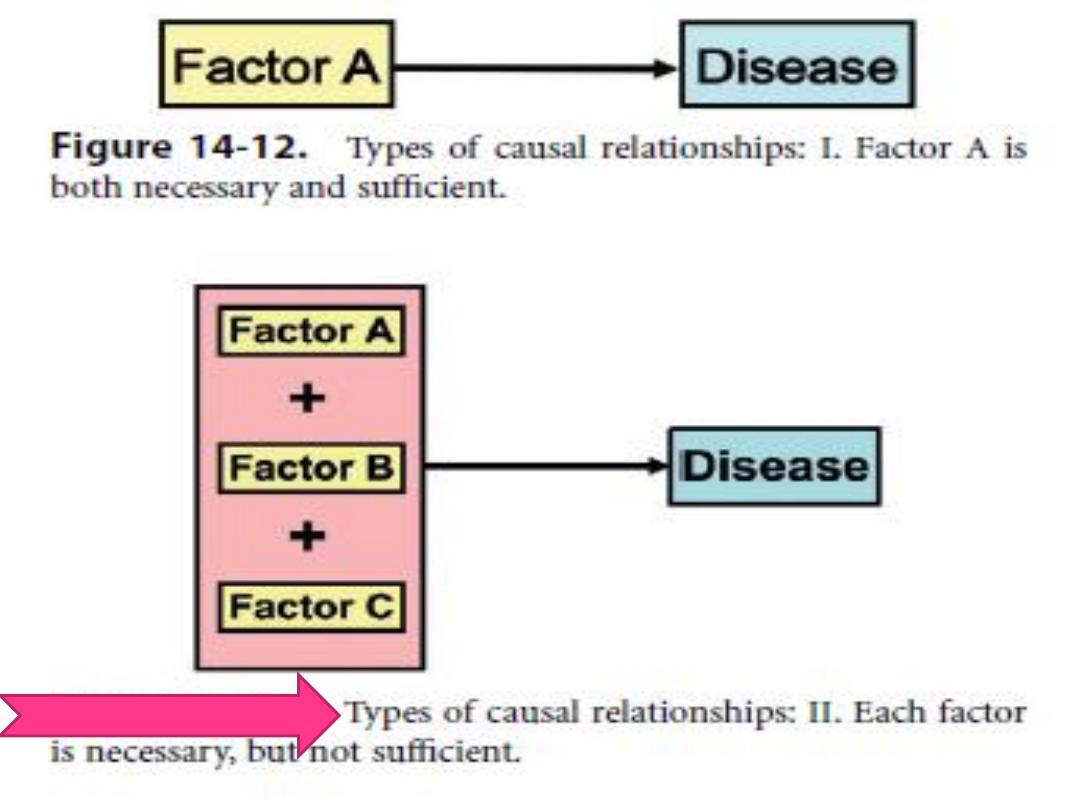

Necessary and Sufficient
A factor is both necessary and sufficient for
producing the
disease. Without that factor, the disease never
develops(the factor is necessary), and in the
presence of that factor, the disease always develops
(the factor is sufficient)

For example, in most infectious diseases, a number of
people are exposed, some of whom will manifest the
disease and others who
will not. Members of households of a person with
tuberculosis do not uniformly acquire the disease from
the index case. If the exposure dose is assumed to be the
same, there are likely differences in immune status,
genetic susceptibility, or other characteristics
that determine who develops the disease and who does
not. A one-to-one relationship of exposure to disease,
which is a consequence of a necessary and sufficient
relationship, rarely if ever occurs.
Necessary, But Not Sufficient
Each factor is necessary, but not, in itself, sufficient
to cause the disease Thus, multiple factors are
required, often in a specific temporal sequence

carcinogenesis is considered to be a multistage
process involving both initiation and promotion.
For cancer to result, a promoter must act after an
initiator has acted. Action of an initiator or a
promoter alone will not produce a cancer.

Sufficient, But Not Necessary
In this model, the factor alone can produce the disease, but
so can other factors that are acting alone ,Thus, either
radiation exposure or benzene exposure can each produce
leukemia
without the presence of the other. Even in this situation,
however, cancer does not develop in everyone who has
experienced radiation or benzene exposure, so although
both factors are not needed, other cofactors probably are.
Thus, the criterion of
sufficient
is rarely met by a single
factor.

Neither Sufficient Nor Necessary
In the fourth model, a factor, by itself, is neither
sufficient nor necessary to produce disease ,This is a
more complex model, which probably most
accurately represents the causal relationships that
operate in most chronic diseases.

•
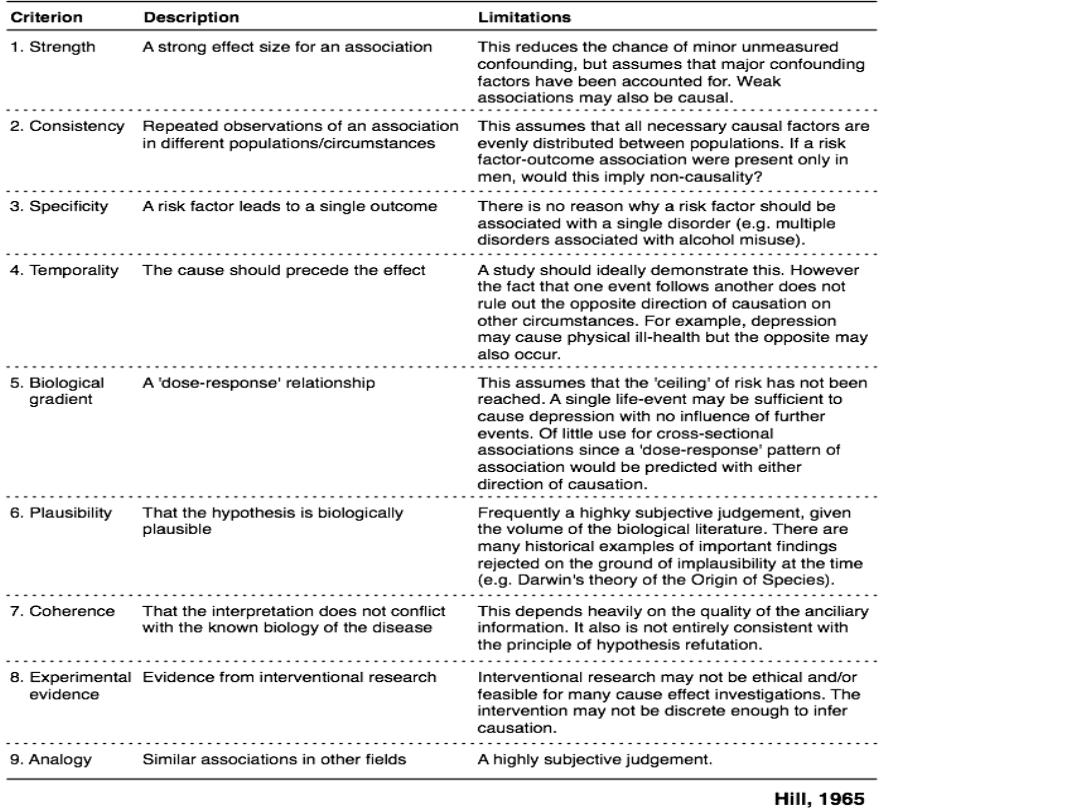
The Bradford Hill criteria ((Hill's criteria))
for causation, are a group of guidelines
that can be useful for providing evidence
of a causal relationship between a putative
cause and an effect, established by
the
(1897–1991) in 1965.
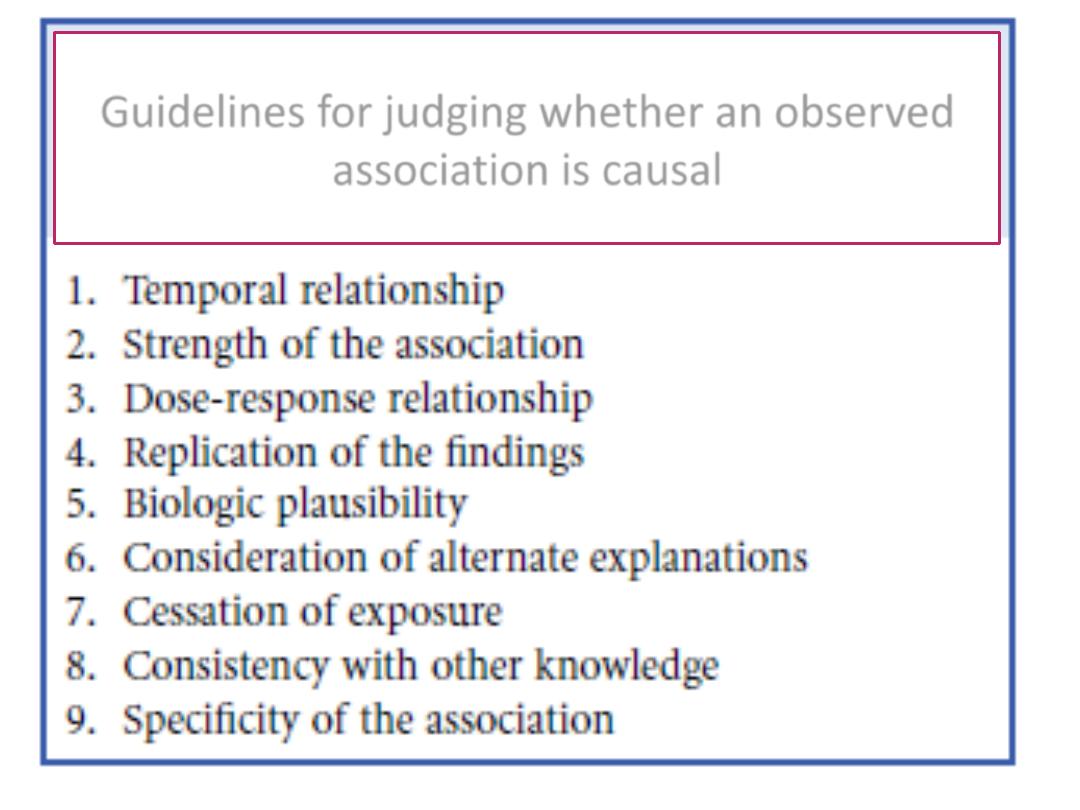
Guidelines for judging whether an observed
association is causal

1.
Temporal Relationship.
It is clear
that if a factor is believed to be the
cause of a disease, exposure to the
factor must have occurred before the
disease developed.

2-
Strength of the Association:
The strength of
the association is measured by the relative risk (or
odds ratio). The stronger the association, the more
likely it is that the relation is causal.
3-
Dose-Response Relationship:
As the dose of
exposure increases, the risk of disease also
increases.

4-Replication of the Findings.:
If the
relationship is causal, we would expect to
find it consistently in different studies and
in different populations.
5-Biologic Plausibility: Biologic plausibility
refers to coherence with the current body of
biologic knowledge.

6-Consideration of Alternate Explanations:
We have discussed the problem in interpreting an observed
association in regard to whether a relationship is causal or is the
result of confounding. In judging whether a reported association
is causal, the extent to which the investigators have taken
other possible explanations into account and the extent to
which they have ruled out such explanations are important
considerations.
7-Cessation of Exposure.:
If a factor is a cause of a
disease, we would expect the risk of the disease to decline when
exposure to the factor is reduced

8-Consistency with Other Knowledge:
If a
relationship is causal, we would expect the
findings to be consistent with other data.
9-Specificity of the Association:
An
association is specific when a certain exposure is
associated with only one disease; this is the
weakest of all the guidelines.

Question:
** All of the following are important criteria when
making causal inferences except:
a. Consistency with existing knowledge
b. Dose-response relationship
c. Consistency of association in several studies
d. Strength of association
e. Predictive value