Here is the normal appearance of a benign reactive lymph node. At the top is the capsule and just under that a subcapsular sinus where lymphatics enter that drain tissues peripheral to the node. Beneath the capsule is the paracortical zone with lymphoid follicles having a pale germinal center in which the immune responses are often generated. Beneath this are sinusoids extending to the center of the node.
At high magnification is seen a lymph node follicle with a germinal center containing larger lymphocytes undergoing activation. At the lower right is the subcapsular sinus.
At high magnification, the germinal center in this reactive lymph node follicle has prominent macrophages with irregular cellular debris (so-called "tingible body macrophages"). Blood vessels are also more prominent.
this is a cross section through the mesentery to reveal multiple enlarged lymph nodes that abut each other. Unlike metastases, nodes with lymphoma tend to have little necrosis and maintain a solid, fleshy tan appearance. High grade non-Hodgkin's lymphoma (NHL) tends to involve a single node, localized group of nodes or extranodal site. Low grade NHL tends to involve multiple lymph nodes.
Here is a lymph node involved by lymphoma, a malignant process characterized by the proliferation of neoplastic lymphoid cells. The capsule of the node has been invaded and the lymphomatous cells extend into the surrounding adipose tissue. Note that the follicles are numerous and irregularly sized. This is a malignant lymphoma, small cleaved cell type, follicular (also known as: malignant lymphoma, poorly differentiated lymphocytic type, nodular).
The malignant lymphocytes here are very large with a moderately abundant cytoplasm, and the nuclei are round to ovoid with prominent nucleoli and occasional mitoses. The diagnosis is diffuse malignant lymphoma, large cell type (also known as: immunoblastic lymphoma). The major differential diagnosis in this case would be a metastatic carcinoma. The presence of monoclonal immunoglobulin as demonstrated by immunoperoxidase technique would help to confirm this lesion as a malignant lymphoma.
here are neoplastic glandular configurations representing metastatic adenocarcinoma. The nodes draining from the primary site of a carcinoma are most commonly involved, but distal nodal groups may be involved as well. Similar to lymphoma, nodal metastases produce firm, painless enlargement
This is a high power view of a Reed-Sternberg cell seen with Hodgkin's disease. Note the large, prominent nucleoli.
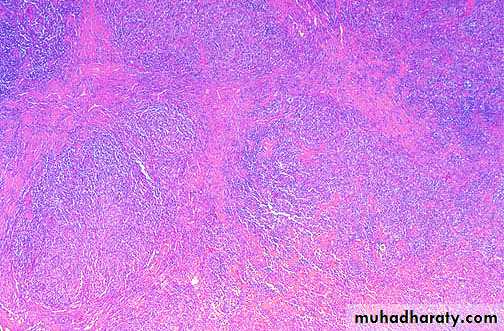
This is Hodgkin's disease, nodular sclerosis type. Note the bands of pink collagenous tissue dividing the field in this lymph node.
At high power, there are scattered large cells with a surrounding prominent clear space, an artefact of formalin fixation. These are the lacunar cells characteristic for the nodular sclerosis type of Hodgkin's disease.
This is a markedly enlarged spleen (the ruler is 15 cm long). Such massive splenomegaly is usually indicative of some myeloproliferative disease such as chronic myelogenous leukemia or myelofibrosis. There are subcapsular yellow-tan infarcts. Congestive splenomegaly (as with portal hypertension in cirrhosis of the liver) is unlikely to increase the size of the spleen over 800 gm. A spleen >1000 gm suggests a myeloproliferative, lymphoproliferative, or hematopoietic disorder.
Here is a 5 cm lymph node (obviously from a patient with lymphadenopathy). The node should normally be soft and pink and less than 1 cm in size. This lymph node is involved with Hodgkin's disease. This gross appearance could pass for a non-Hodgkin's lymphoma as well.