1
L5
HHV
D. Haider
HHV
HUMAN HERPES VIRUS INFECTIONS
Enveloped, dsDNA viruses. Similar morphologically but differ clinically and biologically. Three
groups:
1. ALPHA-HRPES VIRUSES (HSV-1, HSV-2, AND VZV).
2. BETA-HERPESVIRUSES (CMV, HUMAN HERPESVIRUSES (HHV)-6 AND
HHV-7, SIMIAN HERPES B).
3. GAMMA-HERPESVIRUSES (EBV AND HHV-8).
There are eight human herpes virus, they are capable of establishing lifelong latency after acute
infections, and are also capable for oncogenesis and reactivation under certain conditions, these
are DNA viruses and divided into subgroups according to their site of latency and their infectious
manifestations.
HHV are acquired by direct contact with clinically active infected person or through
asymptomatic shedding of virus, for many HHV infected saliva is a common source of infection,
sexual contact, intrauterine infection and acquiring the infection at time of delivery, blood
transfusion, and transmission at time of transplantation are modes of acquisition depending on
HHV type.
Airborne infection occurred only with VZV, humoral immunity is required to protect against
primary infection but after infection is established it does not control its spread. The cell-
mediated immune system is responsible for controlling spread, transmission, and severity of
HHV infections.
Infection prevention relies on screening, safe sexual practices, and infection control measures.
Vaccines exist only for VZV. Effective antiviral medications are available for treatment and
reducing of reactivation of some of the HHVs. Immunoglobulin preparation for VZV and CMV
are indicated under certain circumstances in immunocompromised persons.
Although they are closely related and cause similar diseases, herpes simplex viruses 1 and 2
(HSV-1 and HSV-2) are genetically and serologically distinct. HSV-1 infection occurs earlier in
life, with nearly 90% of adults worldwide having detectable antibodies by age 40 years. HSV-2
is less prevalent, ranging from 20% to 60% depending on number of sexual partners, sex, and
geographic location.
Numerous infection syndromes are caused by HSV, depending on the virus type, host age,
immune status, and anatomic site involved. HSV-1 most frequently manifests as
gingivostomatitis and pharyngitis
HSV-2 is a common cause of genital ulcer disease worldwide Primary genital infection during
pregnancy may be transmitted to the fetus and lead to spontaneous abortion.
2
Although recurrent infection occurs more often during pregnancy, neonatal outcome is usually
unaffected in seropositive women.
HSV-1 and HSV-2 may cause other cutaneous manifestations, including infection of the finger
(herpetic whitlow) or skin (herpes gladiatorum). Involvement of the eye, with keratitis and acute
retinal necrosis, occurs infrequently. Proctitis may occur secondary to anal intercourse.
HSV infection (primarily HSV-1) is the most common cause of nonepidemic viral encephalitis.
Aseptic (sometimes recurrent) meningitis, sacral radiculopathy, and transverse myelitis may also
occur after HSV-2 genital infection.
Infection of visceral organs, including the esophagus, lung, and liver, may result from viremia
or direct extension from nearby mucosal surfaces. The common association of erythema
multiforme and HSV infection is a consequence of the host's immune response to the virus.
Management:
The nucleoside analogues acyclovir, valacyclovir, and famciclovir are effective for treating
episodic HSV-1 and HSV-2 infections and suppressing recurrent infections. Topical antiviral
agents have limited usefulness for treating mucocutaneous disease; however, they are
recommended for treatment of HSV eye infections.
Intravenous acyclovir is required to treat HSV encephalitis. No studies of efficacy of systemic
antiviral therapy for HSV aseptic meningitis exist.
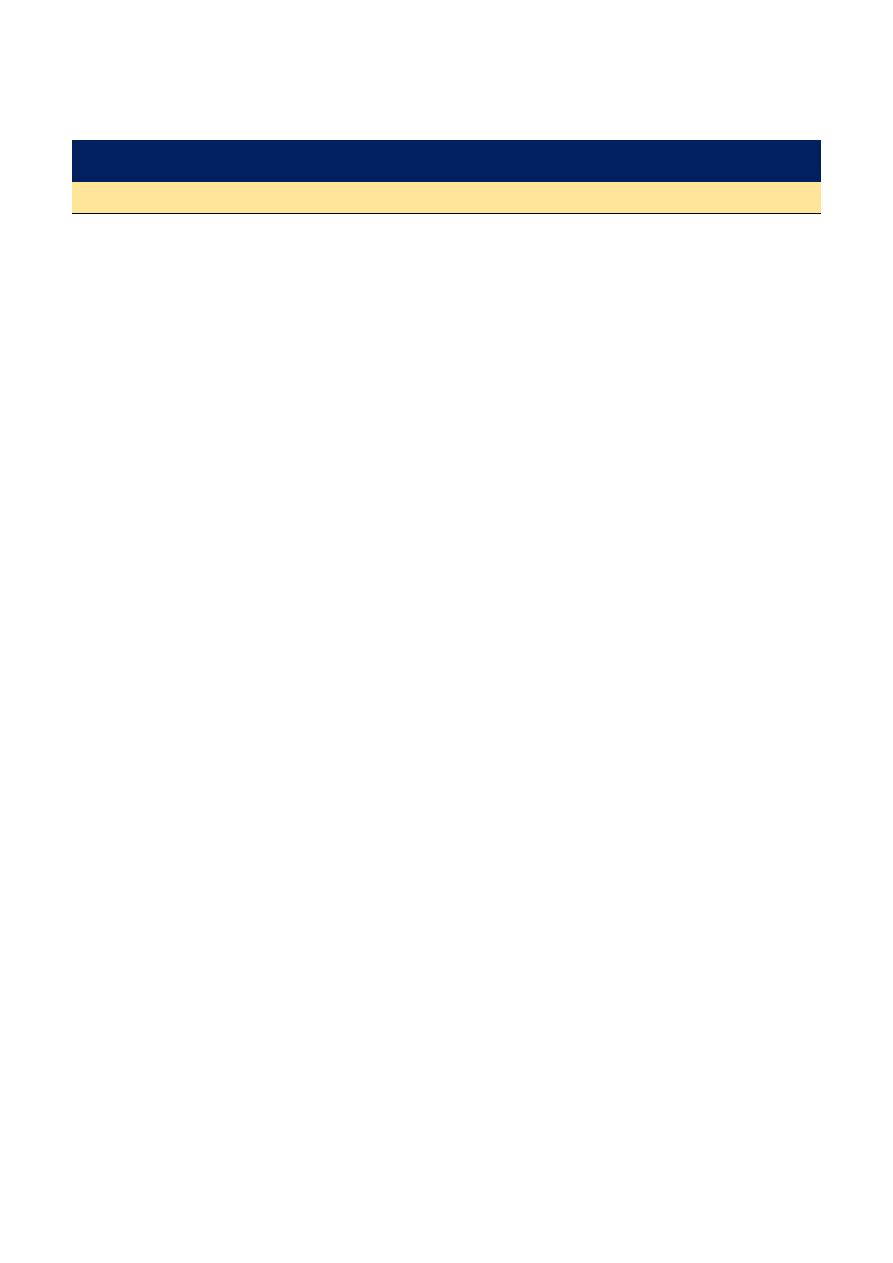
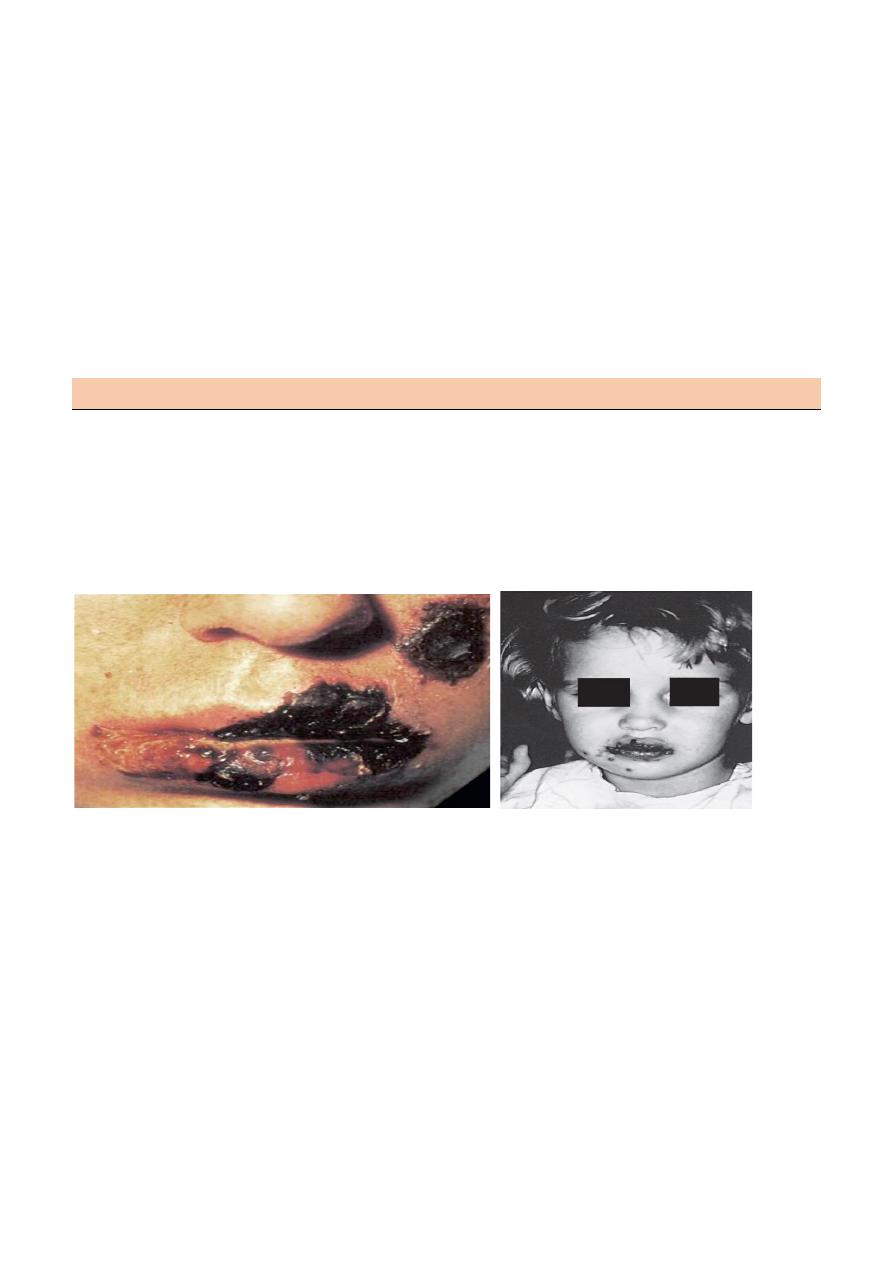
Severe Mucocutaneous
Primary Herpes Simplex Jinjivostomatitis in a Child
Herpes Simplex
In Renal Transplant Recipient
Mubark A. Wilkins