Fifth Stage
Internal Medicine
Dr. Aamer – Lecture 2
1
Thrombotic Thrombocytopenia Purpura (TTP)
History:
•
Seizure
•
Pallor
•
High grade
fever
o
In general, fever is sign of infection, so it needs localization:
▪
Fever + CNS manifestation
Meningitis/Encephalitis
▪
Fever + Cough
Respiratory infection
▪
Fever + Diarrhea
GIT infection
▪
…
So, for first look, it is CNS-related condition (seizure)
Examination:
•
Bilateral ecchymosis & purpura.
Next step?
•
CBC:
o
WBC = Normal
o
Platelets = low
o
Hb = Low
i.e.
bicytopenia
2
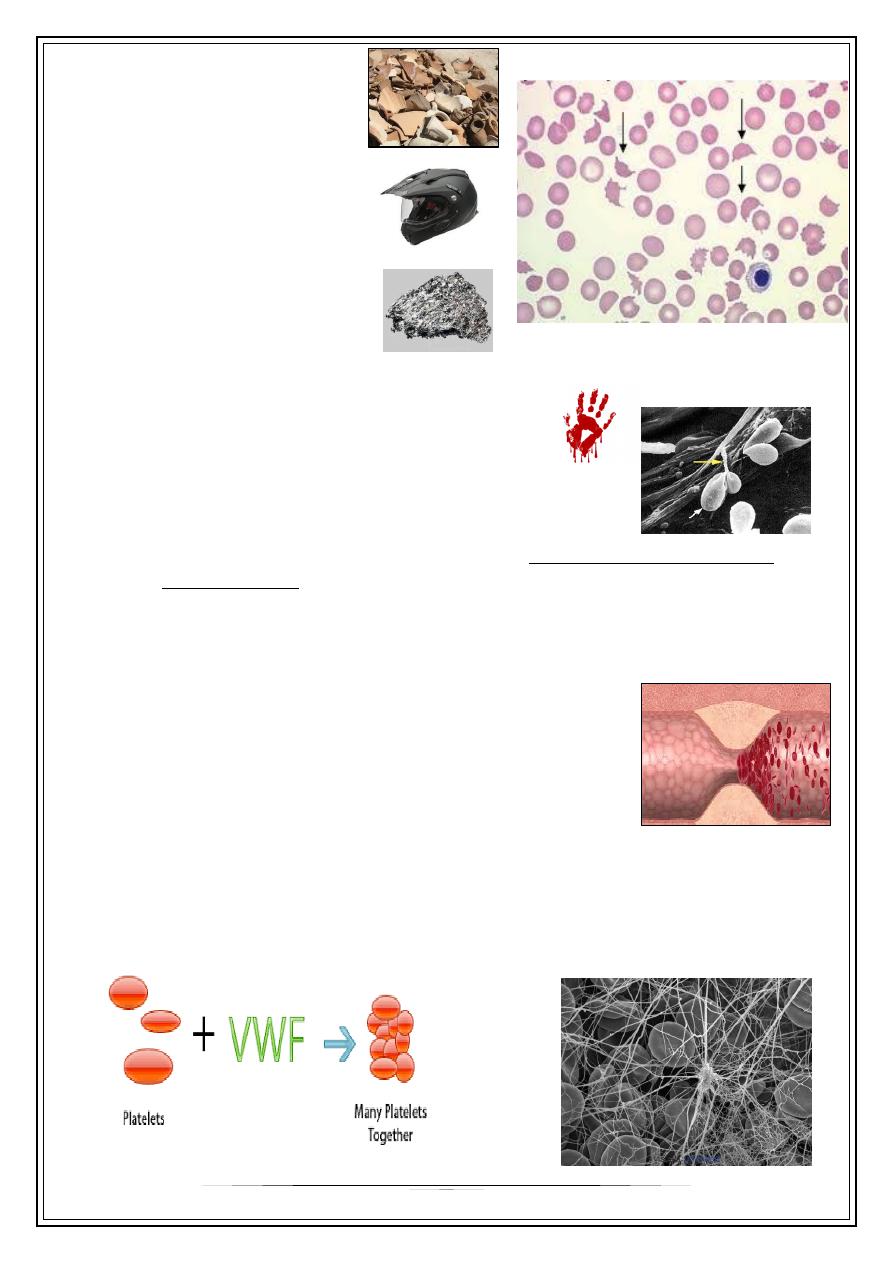
•
Blood film:
o
Fragmented RBCs:
▪
Helmet cells
▪
Schistocytes
-This means, the RBCs are murdered!
-Under electronic microscope, the RBCs
appear hanged by fibrin band!.
o
So, this is intravascular hemolysis, called microangiopathic hemolytic
anemia (MAHA)
What is MAHA?
•
Microangiopathic subgroup of hemolytic anemia (loss of red blood cells through
destruction) caused by factors in the small blood vessels.
•
Occurs when red cells are forced to squeeze through
abnormally narrowed (obstructed) small vessels.
•
Features:
o
Microvascular lesion causing mechanical injury to circulating red cells
o
Red cells damaged when they move rapidly in the blood vessel and collide
with that Platelets/Von-Willebrand net (Platelet aggregation).
3
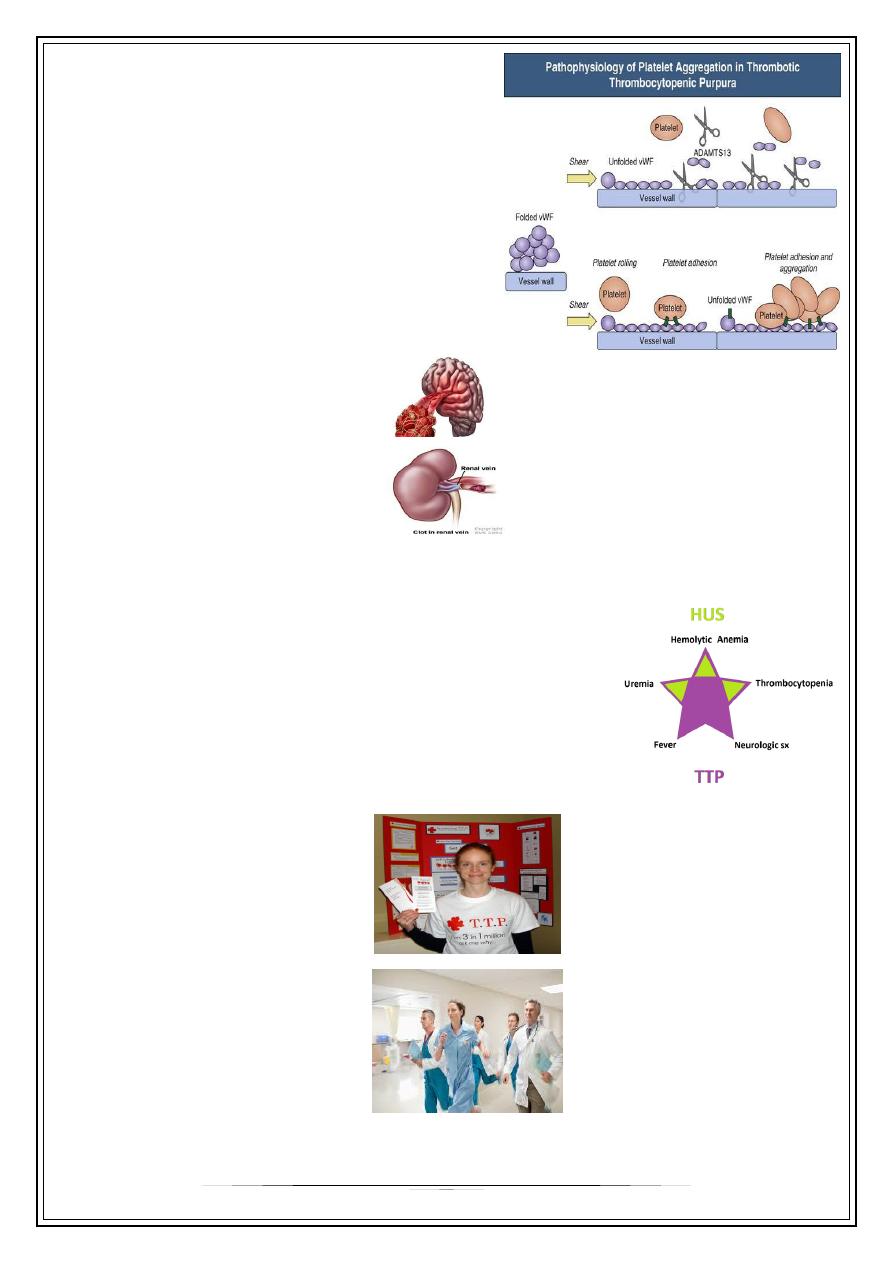
Why platelet aggregation occurs?
•
With congenital or acquired loss of
ADAMTS-13 (a vWF cleaving
metalloprotease) activity, very large vWF
multimers persist in circulation and induce
aggregation by activating platelet surface
glycoproteins.
This involve the small vessels in:
•
Brain Repeated seizures
•
Kidney sometimes uremia
•
Tissue reaction Reactionary fever (i.e. not due to infection)
•
And other organs.
So, what we need for diagnosis is 2 criteria (
not all the 5 of HUS
):
•
Thrombosis (manifested by MAHA)
•
Thrombocytopenia (due to consumption)
And, the diagnosis is:
TTP
!
It is a top super EMERGENCY!
So, when a neurologist consults a
hematologist, there is an impending
disaster…
4
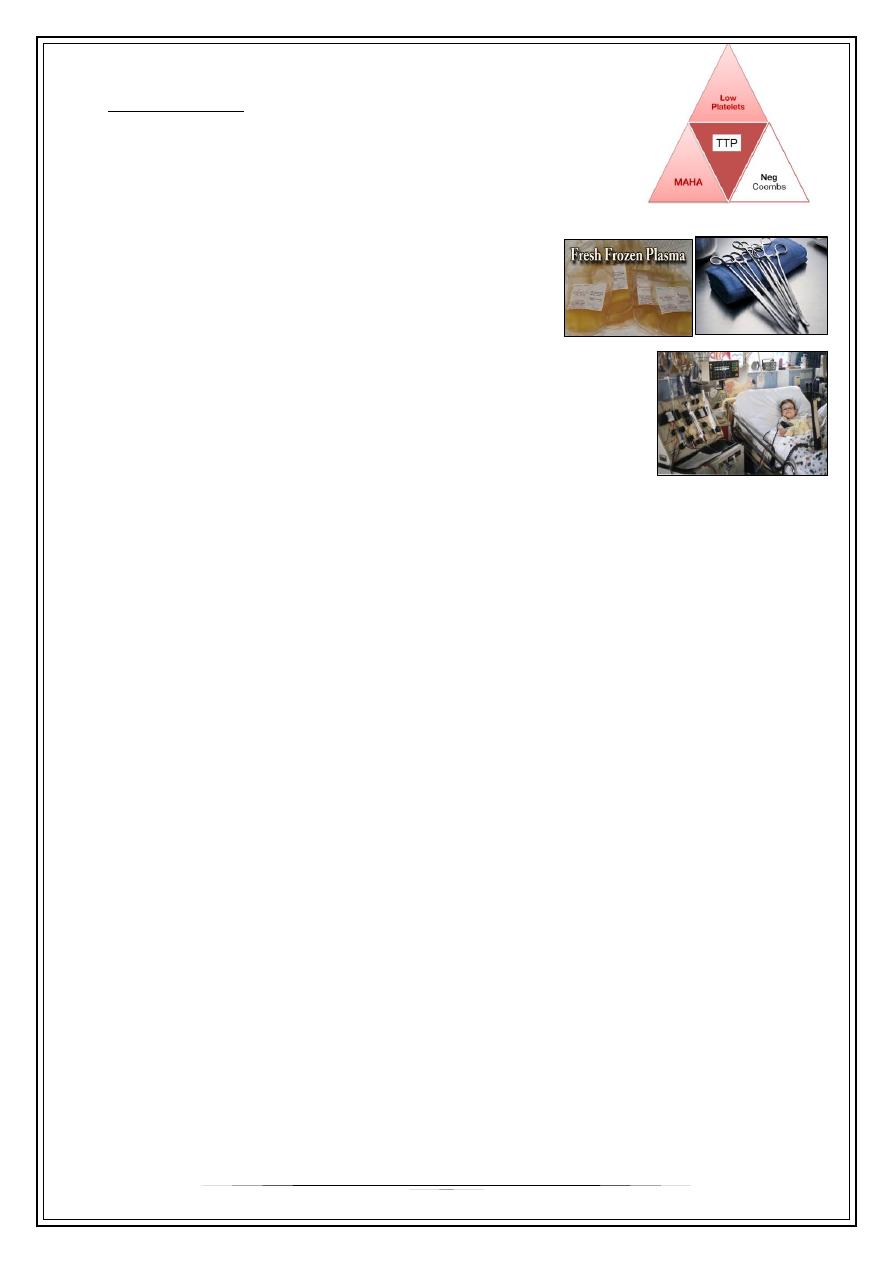
Differential Diagnosis
•
Evan syndrome: an autoimmune hemolytic anemia,
differentiated by investigating with Coombs test
Positive in this syndrome, while negative in TTP
Management
•
Instantons Fresh frozen plasma administration
to replenish ADAMTS-13 (scissors therapy), to
reduce the size of the large multimer vWF.
•
If delayed or severe condition, plasma exchange is
performed (not plasma paresis)
•
Glucocorticoid, a mild hope for reducing the auto antibodies against ADAMTS-13.
So, TTP is very SERIOUS disease, but it is very TREATABLE if caught early.
Thank you,,,
Notes were written from real-time lecture…