1
L6 Gynecology D. Huda Adnan
Ovarian cancer
Epidemiology
Median age at diagnosis 63
Life time risk 1/70.
Fourth commonest cause of cancer death in women in developed countries
>60% of women diagnosed with Stage III/IV
o symptoms of abdo pain, bloating, distension, constipation, back pain usually
happen in advanced stage
To date, no mortality benefit demonstrated with CA125 and TVUS screening.
Subtypes
Epithelial
High grade serous 75%,Mucinous 10%,Endometrioid 10%, Clear cell,Low grade
serous.
Germ cell tumour
Dysgerminoma
,endodermal
sinus
tumour,
embryonal
cell
carcinoma,choriocarcinoma.
Sex cord tumour
granulosa cell tumour, sertoli ledyg cell tumour, gynandroblastoma.
Metastasis from other site called krukenberg especially from stomach.
Epithelial ovarian cancer
Epithelial ov. Cancer is the leading cause of death from gynecological cancer. It
derived from ceolomic epithelium of the ovary, fallopian tube, and peritoneum. It is
hetrogenous group of neoplasm differ in histological and molecular feature and
clinical behavior (low malignat potential, frankely invasive malignant neoplasm).
15-20% of all epithelial neoplasms are LMP, type I tumor low grade(serous,
mucinous, endometriod,clear cell,and transitional Brenner tumor) compremise 25%
of malignant ov. Cancer.
Type II include high-grade serous, endometriod, malignant mixed mesodermal and
undifferentiated carcinomas.
Serous tr
. 1/2 of epith. tr. Have serous histology; psammoma bodies are pathognomonic of
ov. Type serous carcinoma. Mostly present in advance disease, can be bilateral).
Endometroid tumor
2
nd
. Common is associated with endometriosis, endometrial cancer.
It vary in size 12cm-25 cm fleshy ii k.k.

2
Mucinous tr
. 15% of epith. Ovarian cancer.majority benign, 15% of LMP, only 3.5%
malignant.it grow quite large reaching 30 cm and wt 40 kg. malignant mucinous bilateral in
10-20%, benign is unilateral.
pseudomyxoma peritonei is clinical term used to describe abundant of mucoid or gelatinous
material in the pelvis or abdominal cavity surrounded by thin fibrous capsules, ov. Cancer
+this cond. Is always metastases rather than 1ry.
Secondary tr. Malignant tr.
That metast. To ovary are bilateral (krukenberg tr.refer to
metst. Mucinous-signet ring cell adenocarcinoma originate from stomach.
Germ cell tumour
These tumors comprise approximately 20 to 25 percent of ovarian neoplasms overall, but
account for only about 5 percent of all malignant ovarian neoplasms .Ovarian germ cell tumors
arise primarily in young women between 10 and 30 years of age and represent 70 percent of
ovarian tumors in this age group . Dysgerminoma is the most common type.
Dysgerminoma
Although dysgerminomas are relatively uncommon among all ovarian tumors (accounting for
only about 2 percent), they account for 32.8 percent of malignant OGCTs
The majority of cases (75 percent) arise in adolescents and young adults, in whom they account
for about one-third of all ovarian malignancies .Because of their predilection for young women,
they are one of the more common ovarian malignancies detected during pregnancy.
Nevertheless, dysgerminoma can occur at any age.
Lymphocytic infilteration is charecteristic on histopathology.
Granulosa cell tr.
They are solid, but as they grow larger they develop many small cystic spase, cut
surface k.k yellow tinge bec, lipid content. Histology call-exner body, tr. Usually
occur at late reproductive age or after menopause but can seen at any age. Both
granulosa, thecoma produce estrogen.
If before puberty/ precocious puberty.
Reoroductve life/small amount of E cycle remain regular, discovered if complication
occure like tortion.
If E is high ther will be menstrual irregularity, amenorrhea.
After menopause/ post menopausal bleeding, 4% endometrial ca., breast enlargement.
3
Ovarian Cancer Risk Factors
50 years of age or older
Familial factors
o Family history of breast, ovarian, or colon cancer ?3x baseline risk
o Personal history of breast or colon cancer
o Familial cancer syndrome (10%)
BRCA (breast cancer) gene mutation
Hereditary nonpolyposis colon cancer (HNPCC)
Other potential risk factors
Early menarche (younger than 12 years of age)
Late menopause (older than 52 years of age)
Hormone replacement therapy
First pregnancy at older than 30 years of age
Infertility, endometriosis
(fertility Rx does not increase risk)
Certain factors may reduce a woman's risk of developing ovarian cancer :
Taking birth control pills for more than 5 years
Breastfeeding
Pregnancy
A hysterectomy or a tubal ligation
Prophylactic oophorectomy in case of BRCA mutation.
4
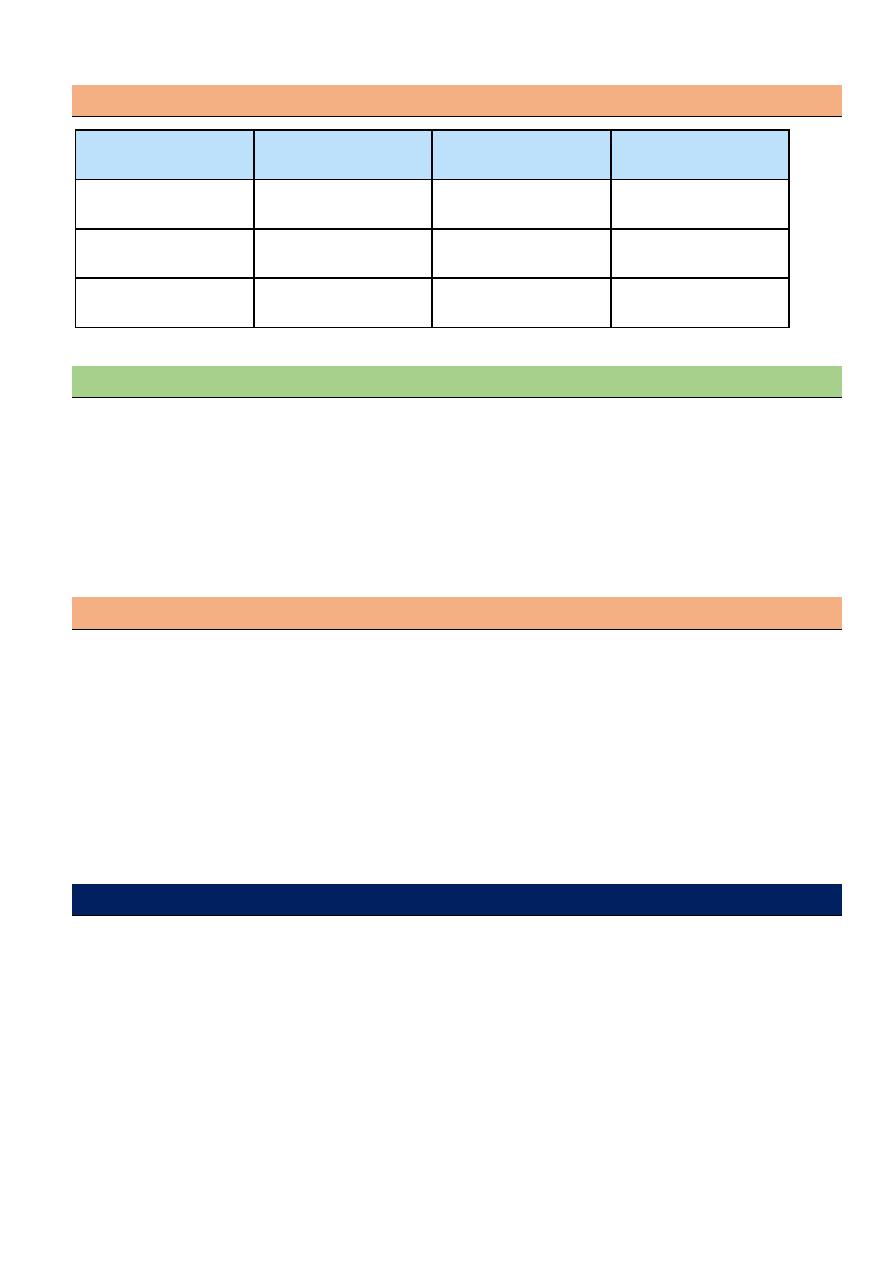
Lifetime Risk of Cancers Associated With Specific Genes
Cancer, %
BRCA1
BRCA2
MMR*
Breast
35-60
30-55
0
Ovarian
35-45
15-25
6-20
Endometrial
0
0
40-60
Red Flags for Cancer Susceptibility: BRCA1/BRCA2 screening indication:
Multiple family members with ovarian or breast cancer
Age of onset of breast cancer
o Younger than 50 years of age (premenopausal)
Bilateral breast cancer
Both breast and ovarian cancer in same patient
Ashkenazi Jewish ancestry (2% chance of BRCA)
Male breast cancer
Ovarian Ca screening
Major organisations do not recommend ovarian cancer screening:
o Poor understanding of natural history
o Poor performance of current test in detecting early stage disease
o
No survival benefit demonstrated even in ‘high risk grp”
o Potential for harm
Genetic study remains the standard of care for BRCA carriers and reduces risk of OC by
75-96%.
Ovarian cancer screeningin high risk group by annual transvaginal ultrasound and serum
CA125.
Clinical manifestations
The growth of dysgerminomas is usually rapid; as a result, patients often present with
abdominal enlargement and pain due to rupture with hemoperitoneum or torsion.
Menstrual abnormalities may occur if the tumor is hormonally active.
Seventy-five percent of women with dysgerminomas present with stage I disease the
contralateral ovary is involved in 10 to 15 percent .Bilateral ovarian disease is more
common with dysgerminoma than with any other malignant OGCT.
Surgery is performed for definitive diagnosis, staging, and initial treatment. For a
unilateral tumor confined to the ovary without capsular involvement or rupture (stage
IC), simple salpingo-oophorectomy is curative in over 95.
5
Sign and symptoms
Ovarian ca. previously called a silent killer without appreciable signs or symptom
until advanced disease is obvious clinically.
Commonly increase abdominal size, bloating,abdominal or pelvic pain. urinary
urgency,frequency, fatigue,upset stomach, indigestion, inability to eat normally,
constipation and back pain.pain during sex. Abnormal vaginal bleeding rarely occur
menstrual changes, nausea, vomiting or intestinal obstruction, weight loss.
Urological symptom such as urgency, frequency.
Physical examination
A pelvic-abdominal mass is palpable in most patients with ovarian cancer, malignant
tumor is tend to be solid, nodular, fixed, but no pathognomonic sign distinguish these
growth from benign tumor. Rectovaginal exam should be performed.
The presence of fluid wave or flank bulging suggests the presence of ascites dx. of
ovarian ca. until prove otherwise. In advance disease upper central abdominal mass
signifying omental caking.
Auscultation of the chest (malignant pleural effusion).
Palpation of L.N supraclavicular, inguinal L.N.
Breast and rectum exam to assess tumor originated from these organs.
laboratory investigations
1-CBP thrombocytosis
2- Electrolyte hyponatremia
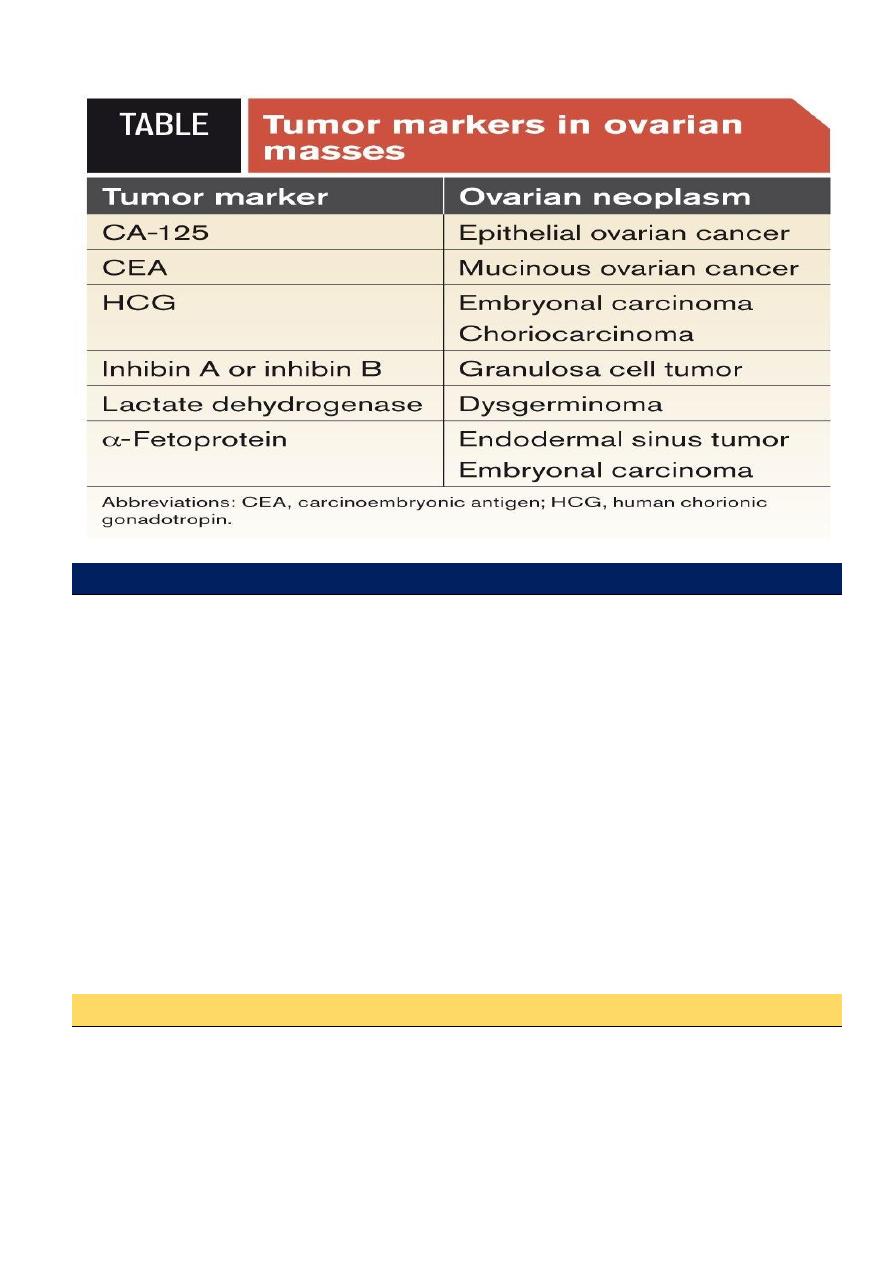
3- Serum CA125 is glycoprotein not produce by normal epithelium but produced by
benign and malignant tumor normal value less than 35 ml unit /ml.
Half of stage 1 ovarian ca. normal value (false negative), false positive in PID,
endometriosis, fibroid, pregnancy, menstruation. Antigen 19-9 in mucinous tr. And
CEA, AFP,LDH, HCG, inhibin , estrogen and testosterone .
Imaging
A. Sonography TVS, malignant multiloculated, solid, or echogenic, large than 5cm.
thick septa, area of nodularity, papillary projection, neovascularity by Doppler flow.
Ascites is easily detected.
B. Radiography CXR (pleural effusion, lung metastases).
C. CT scan do not detect small ovarian tumors see larger tumor and may able to see if
tumor is gowing into near by structures, and enlarge L.N. In advance disease (detect
tr. In liver, retroperitoneal, omentum, abdomen--) and guide surgical cytoreduction.
D. MRI, PET, bone scan of little benefit.
E. Barium enema X-ray to see if the cancer invaded colon or rectum, rarely used now
colonoscopy instead can be used.
6
Risk of malignancy index
for any ovarian mass we can calculate the risk of malignancy index by
ca125 *menopausal status * ultrasonic features
premenopause give 1, post menopause give 3
ultrasonic features give one for each multilocular,solid component, ascites, metastasis,
bilateral. If no any sign give 0, if 1 give 1, if 2-5 give 3.
low risk (3%) if RMI < 25
mod. Risk (20%) if RMI 25-250
High risk (>75%) if RMI >250
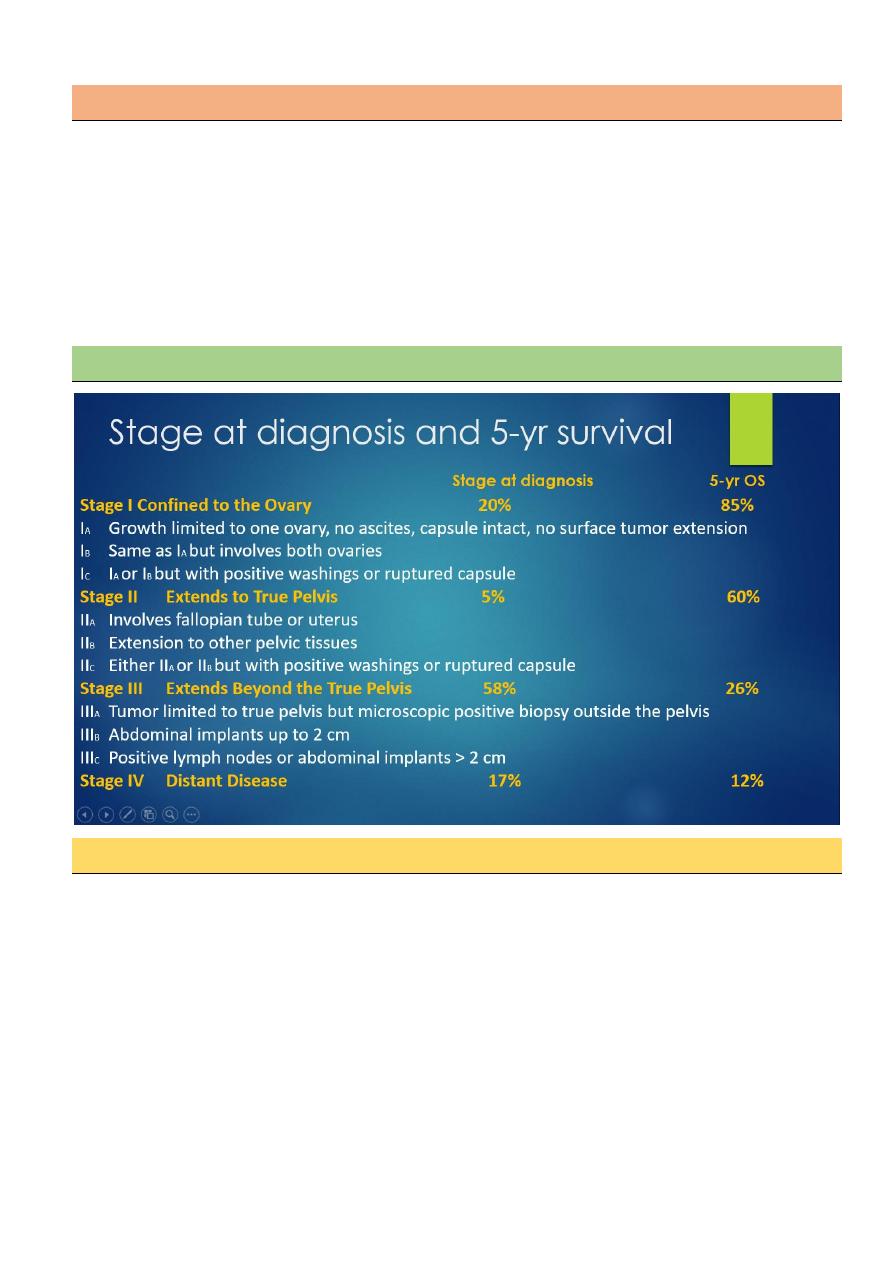
Stage at diagnosis and 5-yr survival
Treatment
After the diagnostic tests are done, your cancer care team will recommend 1 or both treatment
options.
Surgery
Chemotherapy
Early stage disease
(stage 1a, stage 1b )grade 1 managed by debulking suregery include
bilateral salpingoophorectomy plus total abdominal hysterectomy plus infracolic omentectomy
plus systemic pelvic lymphadenectomy , ascitic fluid for cytology and removal of any visible
deposits , no need for chemotherapy.
7
Advanced stage disease
1a and 1b high grade and stage 1c- stage 4 managed by debulking
surgery plus chemotherapy in form of 6 cycles carboplatin and paclitaxil.
No role for 2
nd
look surgery.
In case of recurrent disease treatment by additive chemotherapy.
Surveillance
After treatment early stage ov. Ca. followed every 2-4 m. for 1
st
, 2 Y. then twice/Y. for 3 Y. and
then annually, by complete physical and pelvic exam, serum CA. 125, imaging.
Prognosis depends on
1. stage of disease
2. Histo. mucinous, clear cell type poor prognosis
3. Smaller disease volume prior to surgical debulking
4. Smaller residual disease following cytoreductive surgery.
5. Age at presentation.
FIGO 5 Survival
I 85
II 60
III 26
IV 10-20
Mubark A. Wilkins