Prevention Dr.Jihan Abdulhussein
Lec.15 Dietary counseling in dental practice
There are two ways in which the diet may act upon the oral tissue and play its role in
the prevention of the diseases:
First through the oral environment.
Second through general nutrition.
Nutritional status assessment using Body Mass Index (BMI)
What is BMI?
Body Mass Index (BMI) is a person’s weight in kilograms divided by the square of
height in meters.
(weight (kg) / height
2
)
For children and teens, BMI is age- and gender-specific and is often referred to as
BMI-for-age.
What is a BMI percentile?
After BMI is calculated for children and teens, it is expressed as a percentile which can
be obtained from either a graph or a percentile calculator
(BMI-for-age growth charts) (for either girls or boys)
Percentiles used to assess the size and growth patterns of individual children.
The growth charts show the weight status categories used with children and teens
(underweight, healthy weight, overweight, and obese).
How is BMI calculated and interpreted for children and teens?
By using the BMI Percentile Calculator and involves the following steps:
1. obtain accurate height and weight measurements.
2. Calculate the BMI using the Child and Teen BMI Calculator.online or
The BMI number is calculated using standard formulas.
(weight (kg) / height
2
)
3. Review the calculated BMI-for-age percentile and results.
These criteria are different from those used to interpret BMI for adults — which do not
take into account age or gender.
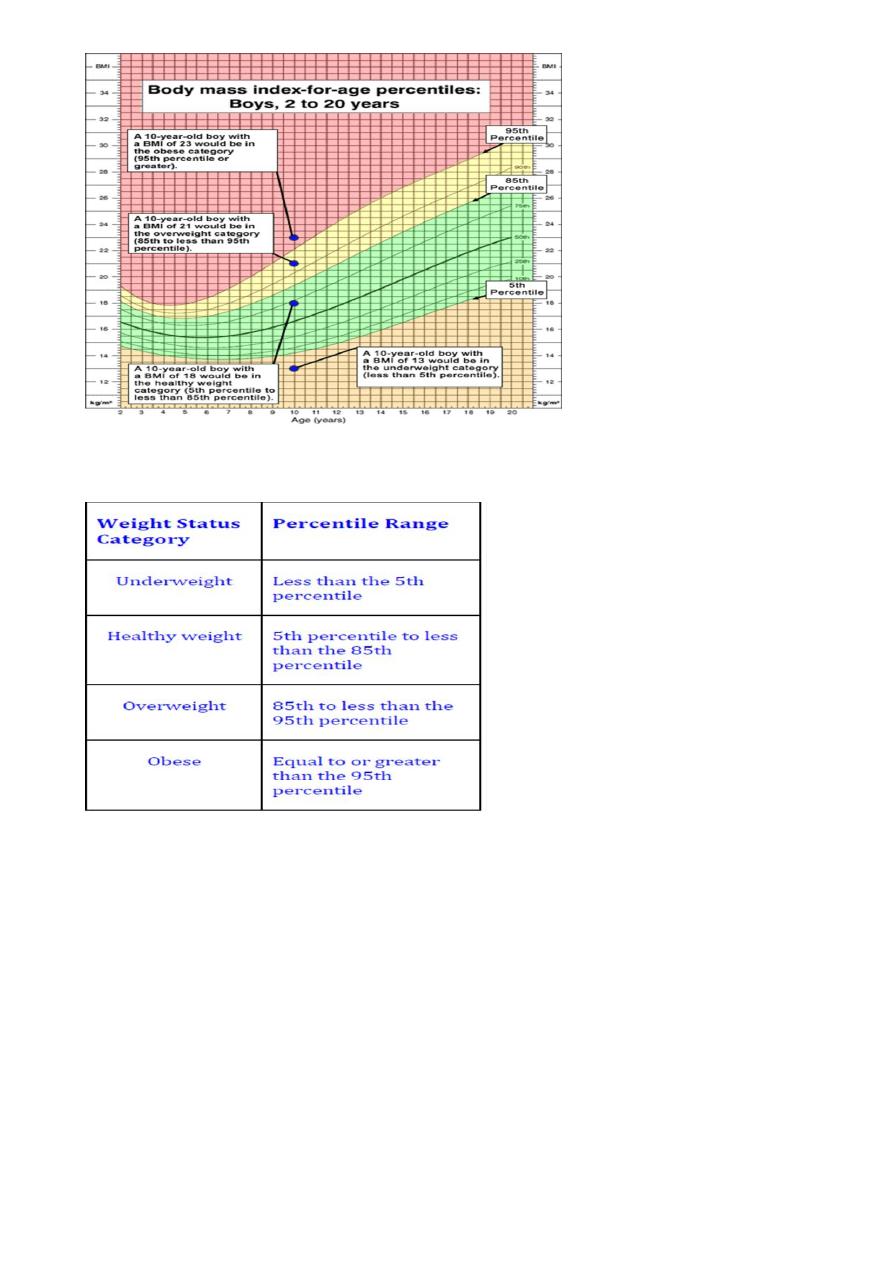
4. Find the weight status category for the calculated BMI-for-age percentile as shown
in the following table.
Age and gender are considered for children and teens for two reasons:
· The amount of body fat changes with age.
· The amount of body fat differs between girls and boys.
Two children have the same BMI values, but one is considered overweight and the
other is not. Why is that?
The explanation of BMI-for-age varies by age and gender so if the children are not
exactly the same age and of the same gender, the BMI numbers have different
meanings.

Assessment of dietary intake:
The modern dental practitioner is not only concerned with educating patients for the
prevention of caries and periodontal disease, but also plays an important role in
screening patients for other health risks.
The role of the dental team should be to
Screen patients for nutritional risk,
Provide dietary guidance related to oral health,
and refer patients to nutrition professionals
Objectives of dietary assessment
To study personal dietary habit objectively
To obtain an overall picture of the types of food, food preferences and quantity
of food eaten
To study food habit and snacking pattern
To record the frequency and when the cariogenic food is consumed
changes in the diet that is important to the health of the oral mucosa and the
periodontium
The methods commonly used to assess dietary intake are: 24-hour recall ,dietary
record, and food frequency questionnaires.
24-hour recall
This is widely used method to assess dietary intake.
A trained person from the dental team interview the patient on the intake of food
and beverages during the latest 24-h period. Consistency in the technique and
skill of the interviewer are important, since these influence the communication
and cooperation of the patient and thereby the result.
Food models and life- size illustrations are recommended by most research as a
support to estimate eaten quantities. The portion size can also be given in
household measures, such as glass, cup, tablespoon, deciliters and grams.
To reduce bias, the 24-h recall is requested without giving the patient prior
notice.
For nutrient with large day-to-day variations, the number of days increased. The
day should select to represent ordinary day.
Dietary record: In dietary record, also called food diaries, the patient records type and
amount of everything consumed during the prescribed period, usually 3-7 days.
Estimates of portion size and selection of days are done in the same way as for the 24-
h recall method.
The patient is thoroughly instructed and motivated to fill in the record and to keep to
normal dietary habits during the record period.
The dietary record and 24 h method are both reported to underestimate the intake.
Food frequency questionnaires: A food frequency questionnaires contains a list of
food items usually 50-150 items. They are selected to illustrate the whole diet or a
specific nutrient (sucrose).The patient mark his / her consumption on a scale ranging
from never to several time per day. It can be used to estimate nutrient intake.
It is uncomplicated and cheap to perform and may be useful as a screening instrument
or to collect dietary data on a group level.
Semi quantitative food frequency questionnaire
Is used to indicate a general food frequency questionnaire that allows for quantification
of serving size
Evaluation of dietary assessment
After a completion of the dietary registration, the intake is evaluated
Evaluation of cariogenic potential.
The frequency of intake and the consistency of refined carbohydrate are key facto r in
the initiation and continuation of the caries process, to identify type of carcinogenic
food we should look at this form a public health view point not a purely biochemical
view point even bread contain sugar but overall bread is not threat to teeth. Therefore
evaluation of cariogenic potential includes an estimation of factors such as number of
intakes containing fermentable carbohydrate, taking snacks during the night, and
retentiveness of the cariogenic products (length of time food might remain on the tooth
surface
Sugar that are added to provide sweetness are classified into
Solid and sticky cakes, sweet roll, pastry, canned fruit candy, toffee, sugared
chewing gum
Liquid soft drink sugar and honey in beverage, ice cream, custard
Slowly dissolved canned
Other properties of the food, known to modify the caries process, should be regarded.
An example of this chewing stimulation provide by the food. The periods with lowered
pH in plaque are reduced by a diet, which increase saliva secretion.
Evaluation of nutritive value
Several, inexpensive software for evaluation of energy and nutrients in the diet are
available, and computer- based analysis of diet registrations are common also in dental
practice, this is a convenient way to evaluate the nutritive value of the intake.
Computing the nutritive of each food eaten by each person in to its different nutrient
was following food composition table, this table convert food that are most commonly
prepared and eaten in to their major nutrient component such as protein, vitamins and
minerals.
Compare the result with Recommended Dietary Allowance (RDAs) Which is a
standard dietary adequacy, was prepared by National Academy of Science for certain
nutrients . RDAs reflects adequate intake for healthy individual to prevent deficiency
state, the value are adjusted for age and gender.
Another way to estimate nutritive value of the diet is to estimate the number of intakes
representing specific food groups. An attempt to translate scientific knowledge of
nutrient need into clear guideline to help people select an adequate diet therefore five
food group were required for health these are:
Bread and cereal group 6-11 serving/day
Vegetable group 3-5 serving /day
Fruit group 2-4 serving /day
Milk group 2- 3 serving /day
Meat, poultry, fish, egg 2-3 serving /day
Dietary counseling
Approach to counseling:
Non-directive:
counselor role is just to aid the patient in understanding his or her own situation
and the patient can make his or her own final decision
Directive
the role of the patient is passive
the decision are made by the counselor for the patient.
In some patients, a single habit e.g., frequent eating of sugar containing lozenges or
taking snacks at night, may explain the caries activity, and this may easily be
corrected .
In others, a complex eating situation, a change in basic behavior is req uired. Change in
behavior is a process affected by the fact that human is neophobic. (a fear of new
things. Therefore, forced dietary changes cannot be successful unless the benefit occur
rapidly and is of demonstrable advantage. This can be seen for some weight- reducing
program. Otherwise, a successful change in diet behavior relies on a program with
repeated, small steps. This is shown to be true for introduction of a new food items and
habits to small children as well as adults.
Motivation
To modify a patients diet the clinician can only seek and encourage the patient's own
motivation. The basic factors that motivate people
self-preservation
recognition
religion
money