Fifth Stage
Internal Medicine
Dr.Fadhil – Lecture 5
1
Serongeative arthritis
What does the term “seronegative” mean when applied to the term seronegative
spondyloarthropathy?
a) Patients do not form antibodies
b) Patients are negative for HLA-B27
c) Patients are negative for RF
d) Patients are negative for ANA
Spondyloarthropathies
Seronegative Spondyloarthropathy: a misnomer !!
thought to be variant of RA, hence “seronegative”
Definition: A group of inflammatory arthropathies that share distinctive clinical,
radiographic and genetic features. These diagnoses include:
Ankylosing spondylitis
Reactive arthritis (Reiter's syndrome)
Psoriatic arthritis
Enteropathic arthritis (Crohn’s, Ulcerative colitis)
Spondyloarthropathy: several criteria have been proposed
Key Features:
Inflammatory axial arthritis (sacroiliitis and spondylitis)
Peripheral arthritis (often asymmetric and oligoarticular)
Enthesitis
HLA-B27 positivity
XRay evidence of erosions + hyperostosis (reactive bone)
Extra-axial, Extra-articular Features
2
Back to basics: Enthesis
Enthesis is the site of bony attachment of
Tendon
Ligament
Cartilage
Joint capsule
Fascia
Etiology
The common etiological thread of these disorders is their striking association with
HLA-B27, particularly ankylosing spondylitis(AS). HLA type B27 is a finding in more
than 90% of Caucasians with AS but only 8% of controls. The role of class 1 HLA
antigens in the pathogenesis is supported by the fact that HLA-B27 transgenic
mice spontaneously develop arthritis, skin, gut and genitourinary lesions.
What is HLA-B27?
a) It is an antibody
b) It is an MHC I molecule
c) It is an MHC II molecule
d) It is an antigen
There are clues that infections play a role, possibly by molecular mimicry, with
parts of the organism which are structurally similar to the HLA molecule triggering
cross-reactive antibody formation. This is unproven. AIDS is shown to increase the
prevalence of reactive arthritis and spondylitis in sub-Saharan Africa even in the
absence of HLA-B27. The explanation for this changing epidemiology is unclear.
The types of arthritis that fallow a precipitating infection are called reactive
arthritis.
The specialized immune systems of the gut and genito-urinary mucous
membranes may also play a causal role, perhaps reacting to local infections or to
antigens which across the damaged mucosa.
3
Ankylosing Spondylitis
A type of arthritis that causes inflammation and eventually fusion of the
spine and the spinal joints. Involvement of peripheral joints and
extraarticular manifestations.
AS causes pain, stiffness, disability, decreased spinal mobility, and decreased
quality of life
The prevalence ranges from 0.1 to 1 percent of the population
– Men are affected three times more than women
– Commonly develops between the ages of 15 and 40
95 percent of people with AS share the genetic marker HLA-B27
CLINICAL FEATURES:--
Episodic inflammation of the sacroiliac joints in the late teenage years or early
twenties is the first manifestation of AS. Pain in one or both buttocks and low back
pain and stiffness are typically worse at morning and relieved by exercise. Initially
the diagnosis is often missed because the patient is asymptomatic between
episodes and radiological abnormalities are absent.
4
Retention of the lumber lordosis during spinal flexion is an early sign. Later, para
spinal muscle wasting develops.
The presence of three of the four fallowing indices in adult more than 50 years
with chronic back pain indicate AS:-
1- morning stiffness more than 30%.
2-improvement of back pain with exercise but not rest.
3-awakening because of back pain during second half of the night only.
4-alternating buttock pain.
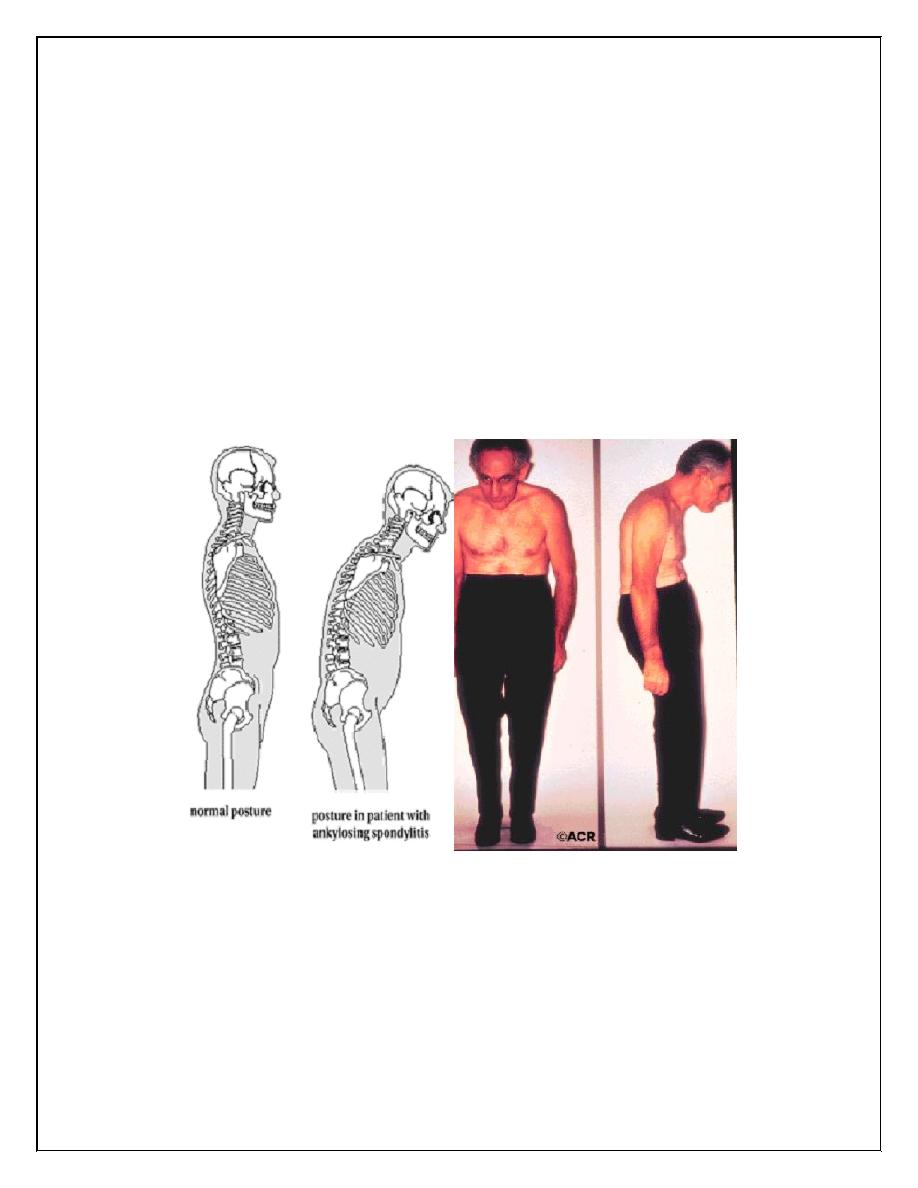
Salient features:
1- 'question mark' posture(due to retention of lumber lordosis, fixed
kyphoscoliosis of the thoracic spine with compensatory extension of the cervical
spine)
2- protuberant abdomen.
Extra-articular features
1- anterior uveitis(25%)& conjunctivitis(20%)
2- prostatitis (80%) of men ; usually asymptomatic
3- cardiovascular disorders ;aortic & mitral incompetence(4% of patients who
have had the disease for over 15 years), conduction defects, pericarditis
4- amyloidosis
5- apical pulmonary fibrosis.
Remember:
Five 'A's of AS: apical fibrosis, anterior uveitis, aortic regurgitation, achilles
tendinitis& amyloidosis.
INVESTIGATION:---
-Blood :- the ESR and CRP are usually raised
-HLA-testing is rarely of value because of high frequency of HLA-B27 in the
population.
5
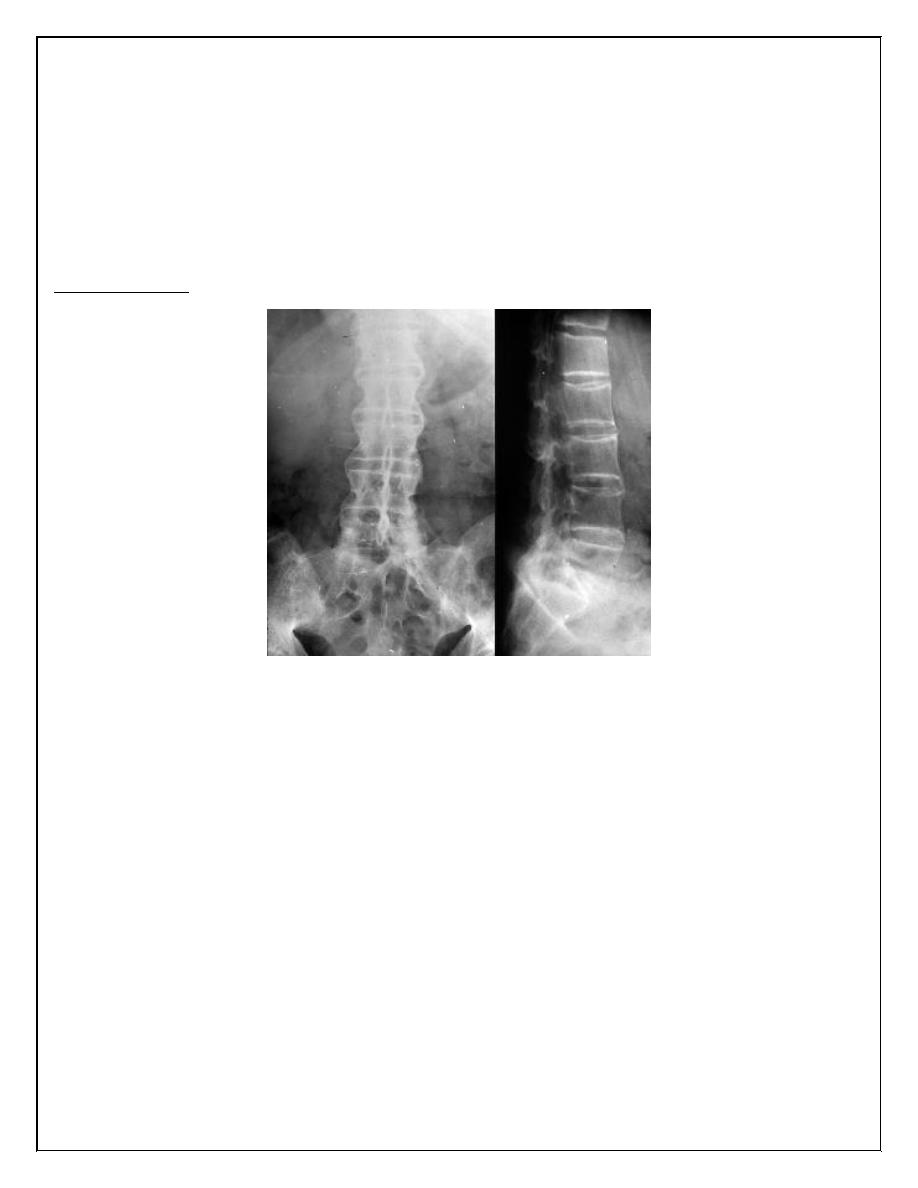
-X-rays:- The earliest radiological appearances in the spine are blurring of the
upper or lower vertebral rims at the thoracolumbar junction(seen on lateral X-
ray) caused by an enthesitis at the insertion of the intervertebral ligaments.
Sacroilitis, sclerosis, squaring of vertebrae, & bridging syndesmophytes ( marginal
bony spurs that bridge the adjacent vertebral bodies) .
-MRI: demonstrates sacroiliitis before it seen on x-ray.
Bamboo spine:
TREATMENT:----
--The key to the effective management of AS is early diagnosis so that a regimen
of preventive exercises is started before syndesmophytes have formed. Morning
exercise aims to maintain spinal motility, posture and chest expansion.
--when the inflammation is active, the morning pain and stiffness are too sever to
permit effective exercise , an evening dose of a long acting or slow release NSAIDs
to improve sleep, pain control, and exercise compliance. Peripheral arthritis and
enthesitis are managed with NSAIDs or local steroid injections.
--Methotrexate is effective for peripheral arthritis but not for spinal disease.
-- In patients with persistent, active inflammation TNF-alpha blocking drugs
produce rapid, dramatic and sustained reduction of symptoms and of spinal and
joint inflammation.
6
PROGNOSIS:--
With exercise and pain relief, the prognosis is excellent and over 80% of patients
are fully employed. Anti-TNF therapies are likely to reduce the morbidity of sever
disease, reducing the risk of permanent spinal stiffness and progressive peripheral
joint disease.
Patients should be made aware that there is a risk of passing HLA-B27 gene to50%
of their children. HLA-B27 positive offspring then have a 30% risk of developing
AS.
Recative Arthritis
In 1916, Hans Reiter reported Reiter’s syndrome: a triad of nongonococcal
urethritis, conjunctivitis, and arthritis that occurred in a young German officer
following an episode of bloody dysentery
Subsequently, more cases were reported following enteric infections OR
venereally acquired genitourinary infections.
In 1967, the term reactive arthritis was applied to similar cases following Yersinia
gastroenteritis
The two terms should be considered synonymous
The term reactive arthritis is increasingly preferred
Reactive arthritis is a sterile synovitis, which occurs fallowing an infection.
Seronegative spondyloarthropathy develops in 1-2% of patients after an acute
attack of dysentery, or sexually acquired infections like nonspecific urethritis in
the male& nonspecific cervicitis in female. In male patients who are HLA-B27
positive, the relative risk is 30-5-%, being HLA-B27 positive is not obligatory.
However, women are less commonly affected.
Reiter's syndrome is a special entity of reactive arthritis in which the fallowing
triad of symptoms are found:-
-arthritis of large joints
- inflammation of the eyes in the form of conjunctivitis or uveitis and
-urethritis in male and cervicitis in women.
7
Reactive arthritis have been associated with all the following except:
a) Chlamydia
b) Ureaplasma
c) Campylobacter
d) Gonorrhea
CLINICAL FEATURES
The onset is typically acute, with urethritis, conjunctivitis(50%)& oligoarthritis of
large & small joints of lower limbs 1-3 weeks after sexual experience or bacillary
dysentery.
There may be systemic disturbances like weight loss, fever, & vasomotor changes
in feet. The onset could be sub-acute or insidious.
There may be only asymmetric oligoarthritis with no clear preexisting urethritis or
dysentery but radiological features & Achilles tendonitis are further clues.
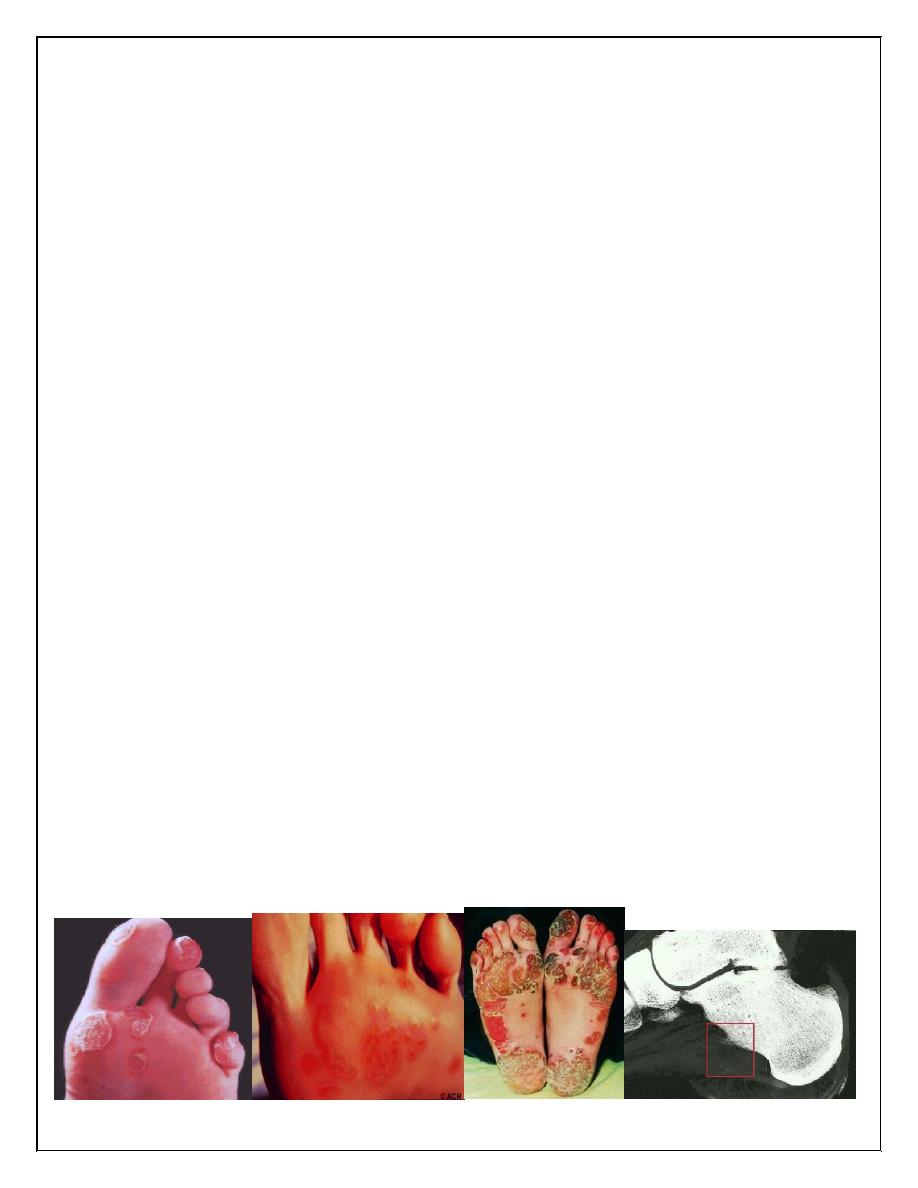
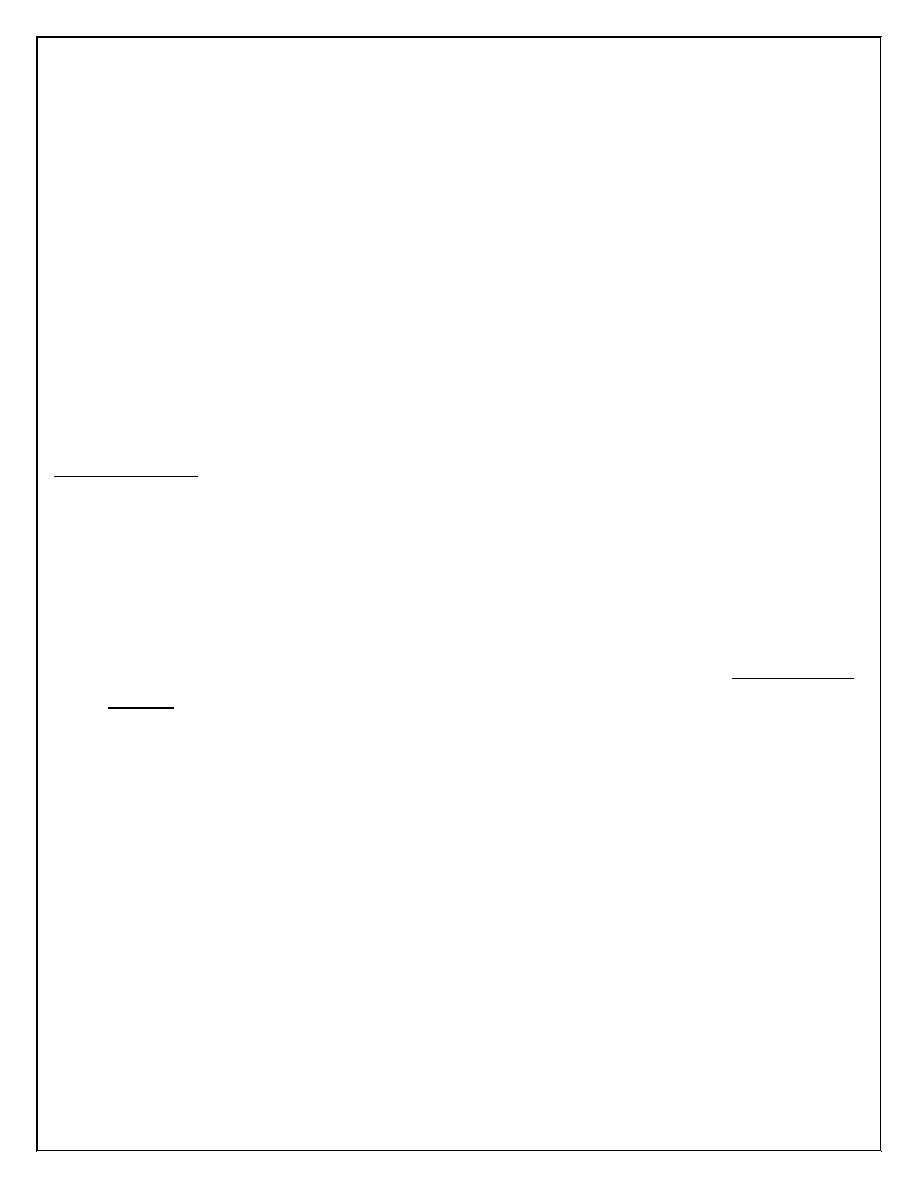
EXRTA ARTICULAR FEATURES :
1- circinate balanitis; 20-50% , starts as vesicles rupture to form superficial
erosions on the prepuce & glans penis. These lesions are painless.
2- keratoderma blenorrhagica 15%; waxy yellow –brown vesicopapules that may
coalesce to form large crusty plaques. Palms, soles & scrotum are typical sites.
Chronic or recurrent disease develops in 60% of patients & not necessarily related
to further infection.
KB: keratoderma-blenorrhagicum
8
Low back pain & stiffness due to sacroiliitis can occur together with cardiac& CNS
abnormalities similar to AS.
Other joints like ankles, midtarsal & MCP joints are involved in chronic reactive
arthritis.
INVESTIGATIONS:
acute phase responses are positive, Anemia of normochromic normocytic type
are clearly evident findings. Synovial fluid reveals inflammatory findings- low
viscosity& turbid , with giant macrophages(Reiter's cells).
GUE for mucoid threads(urethritis), vaginal swab for Chlamydia & GSE for
dysentery together with radiological changes are other clues for diagnosis.
MANAGEMENT
In the first attacks , symptomatic treatment with analgesics & NSAIDs is helpful
together with intra articular steroid injections. Systemic steroids are rarely
needed. In sever disease& intractable keratoderma blenorrhagica anti- rheumatic
drugs like methotrexate & azathioprine are warranted.
Chlamydial infections should be treated with short course tetracycline. Anterior
uveitis requires systemic steroids. TNF is an inflammatory cytokine& TNF blocking
agents like etanercept& infliximab have a rule in treatment of reactive arthritis.
Thank you,,,