1
L16
Neck mass
D. Mushtaq
Anatomical Considerations
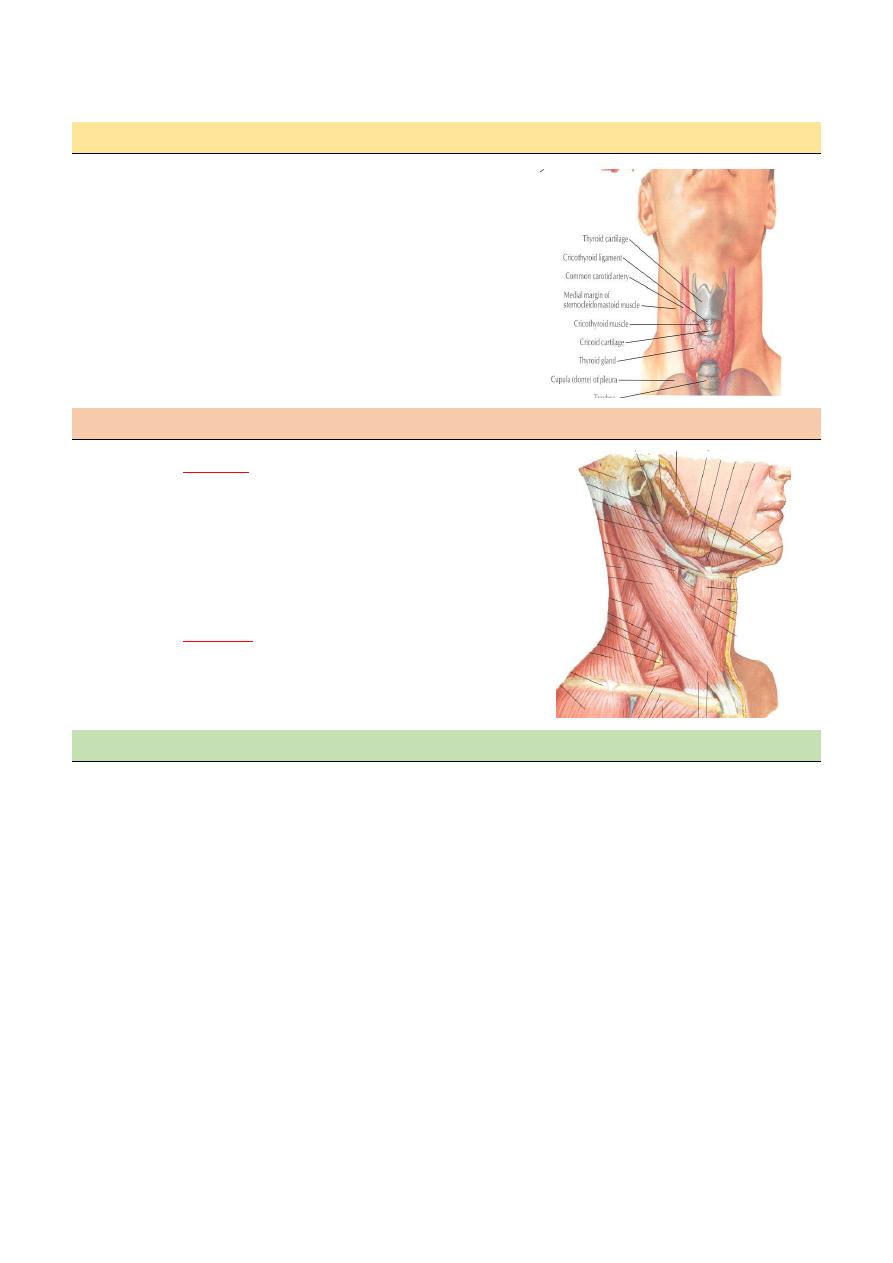
Prominent landmarks
o Hyoid bone
o Thyroid cartilage (men)
o Cricoid cartilage (women)
o Trachea
o Sternocleidomastoid muscle
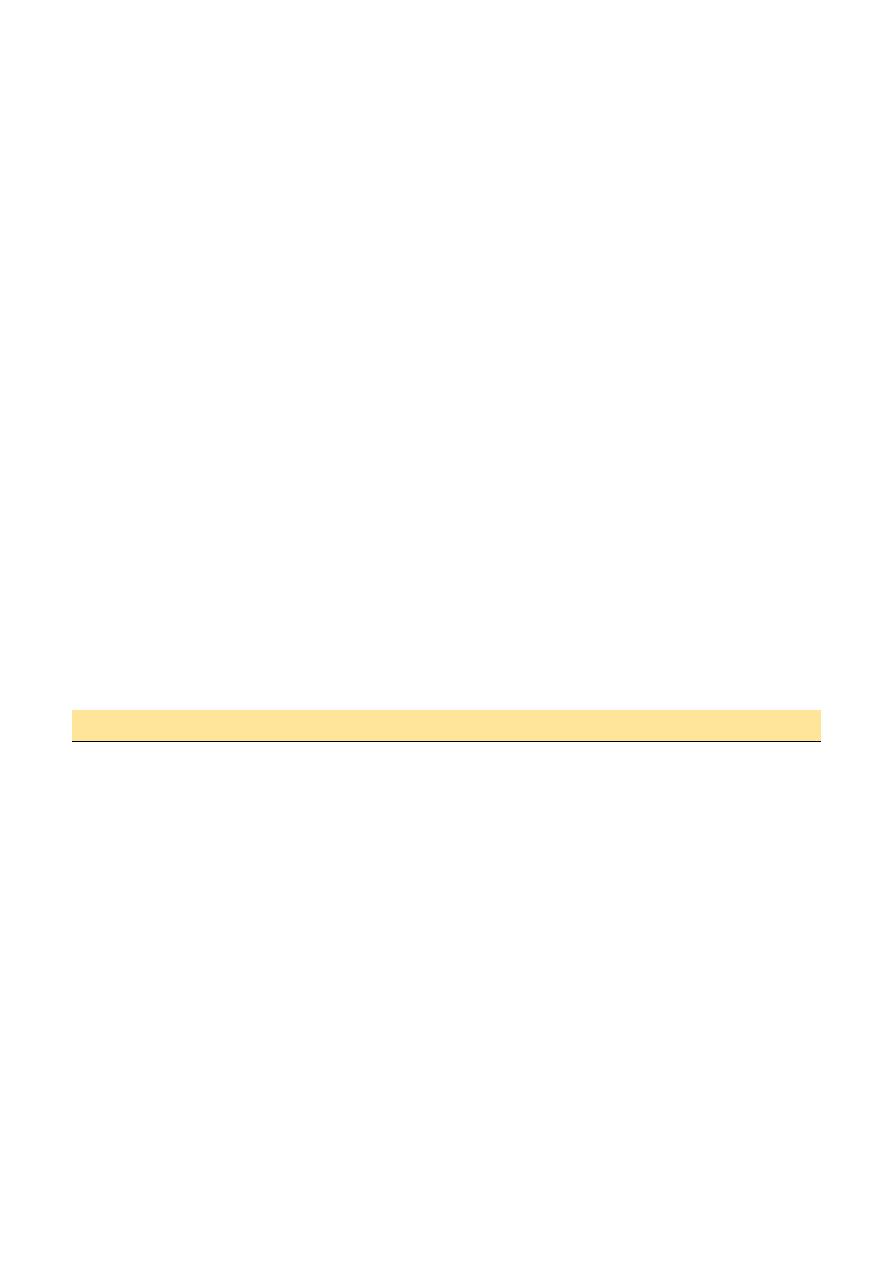
Triangles of the neck
o Anterior
Anterior border of the SCM,
midline, lower border of the
mandible
Subdivisions: inferior carotid,
superior carotid, submandibular,
submental
o Posterior
Posterior border of SCM, clavicle,
anterior border of trapezius
Subdivisions: subclavian, occipital
Differential diagnosis
A. Middle neck mass
1. Congenital
thyroglossal cyst
dermoid cyst
thymic tumor
2. Cx. Lymph adenopathy:
- inflammatory
- neoplastic( metastasis)
3. Neoplasm:
Benign: - lipoma, chondroma, isthmus swelling
Malignant:
Thyroid ca.
4. Inflammations:
- thyroiditis,
- infected thyroglossal cyst
2
B. Lateral neck mass
1. Cong. :
lymphangioma
lat. Thyroglossal cyst
2. Developmental:
- branchial cyst
- laryngocoele
- pharyngeal pouch cyst
3. swelling related to the gland :
submandibular
o = sialadenitis
o = stone
o = tumor
thyroid gland - goiter ,
- tumor.
4. Parapharyngeal tumors
parotid tail, carotid body tumor
5. soft tissue swelling (ludwig`s angina)
6. cx. Lymphadinitis
- -acute( URTI)
- -chronic( tb, syph. AIDS)
7. cx. Ln . Tumor
- 1-lymphoma
- 2-metastatic
8. sternoclidomastoid muscle tumor
9. cx. rib
Clinical evaluations
HISTORY:
- age
- chronicity
- associated symptoms/ dysphagia,
- Otalgia, hoarsness…
- Concurrent illnesses & past h.
- med / surg / drugs/ dxt
- exposure to infections
- smoking
Examinations
- General
- Characters of the Mass ;
Site, size, shape, surface, consistency, mobility &relation
ASSOCIATED SIGNS;
wt.loss,fever,pallor
3
Investigations
1. LAB. :
CBP, ESR ,B.FILM
a. -throat swab for c/s
b. -tub.t
c. -serologic tests for HIV,CMV, EBV.
2. RAD: - CXR u/ss ,MRI, Ct scan ,isotop
3. Thyroid function tests
4. F.N.A C, AFB, culture aerobic &anaerobic)
5. EXCISIONAL BIOPSY
Fine Needle Aspiration Biopsy
Standard of diagnosis
Indications
Any neck mass that is not an obvious abscess
Persistence after a 2 week course of antibiotics
Excisional Biopsy
1. Present of signs& symptoms of malignancy
2. Persist lymphadenopathy
3. DX. Remain in doubt.
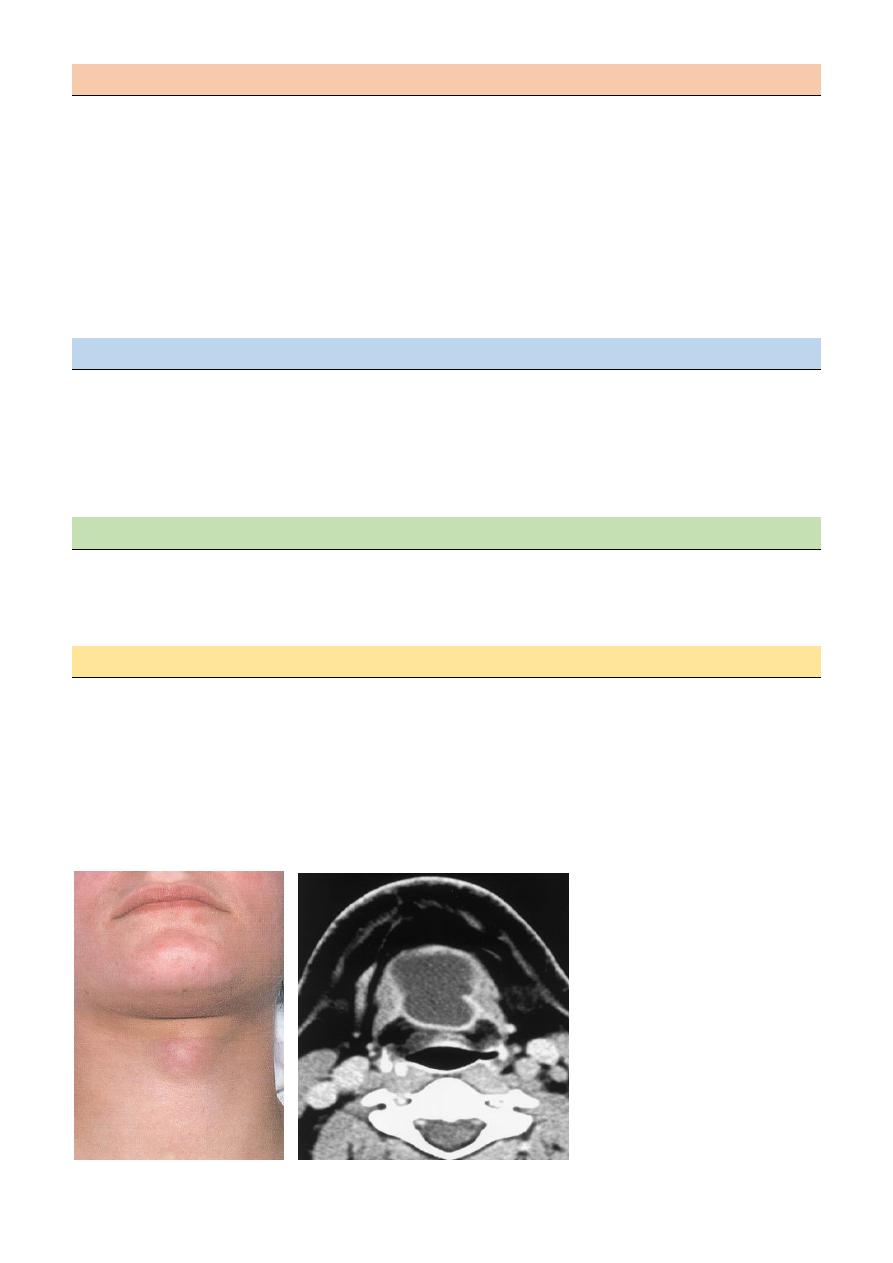
Thyroglossal Duct Cyst
Most common congenital neck mass (70%)
50% present before age 20
Midline (90%).
Usually just inferior to hyoid bone (65%)
Painless unless infected.
Elevates on swallowing/protrusion of tongue
Treatment is surgical removal (Sis trunk) after resolution of any infection
4
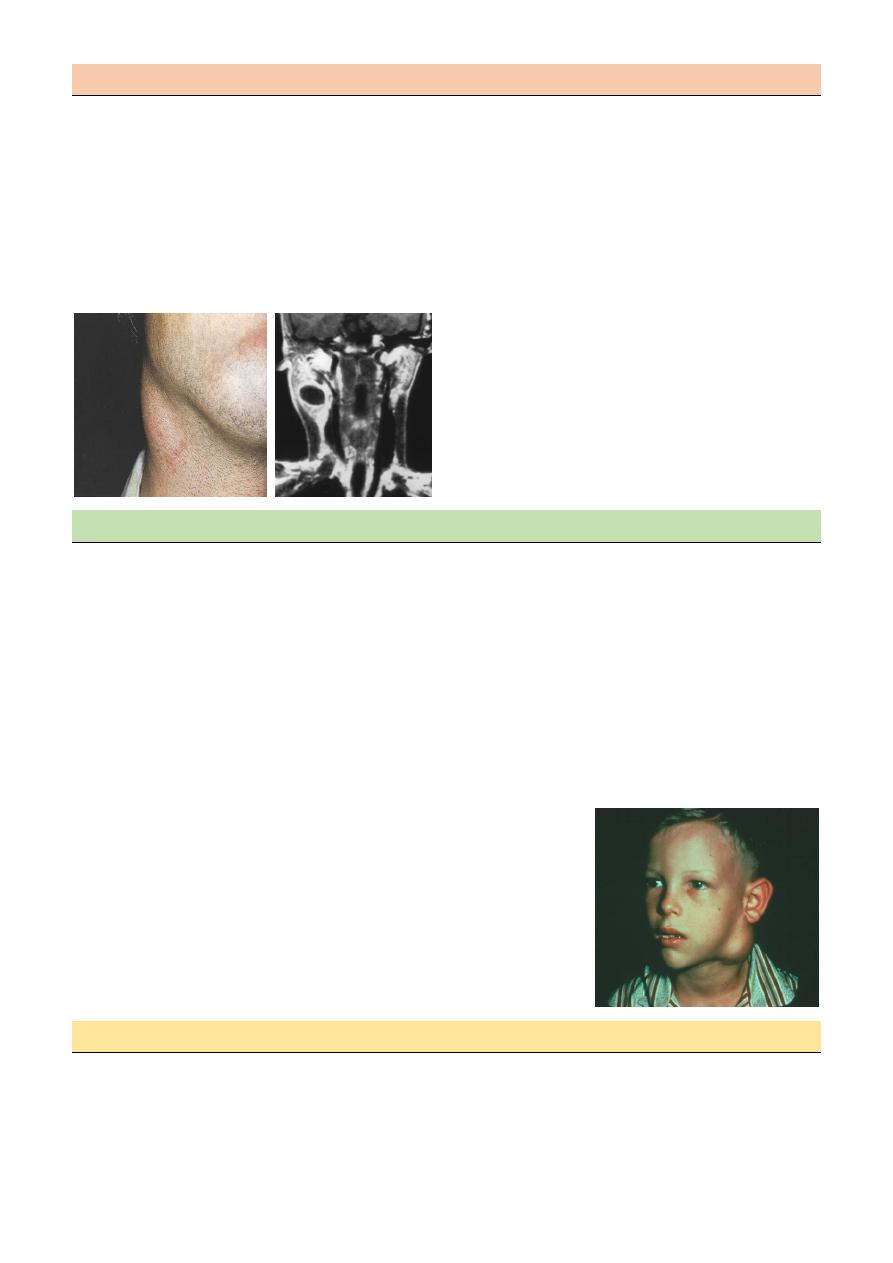
Branchial Cleft Cysts
Branchial cleft anomalies
2
nd
cleft most common (95%)
tracts between internal and external carotids
Most common as smooth, fluctuant mass underlying the SCM
Skin erythema and tenderness if infected
Treatment
o Initial control of infection
o Surgical excision, including tract
Lymphoma
More common in children and young adults
Up to 80% of children with Hodgkin’s have a neck mass
Signs and symptoms
o Lateral neck mass only (discrete, rubbery, non tender)
o Hepatosplenomegaly
Diffuse lymphadenopathy
FNAB – first line diagnostic test
If suggestive of lymphoma – open biopsy
Full workup – CT scans of chest, abdomen, head and neck; bone marrow
biopsy & full blood count.
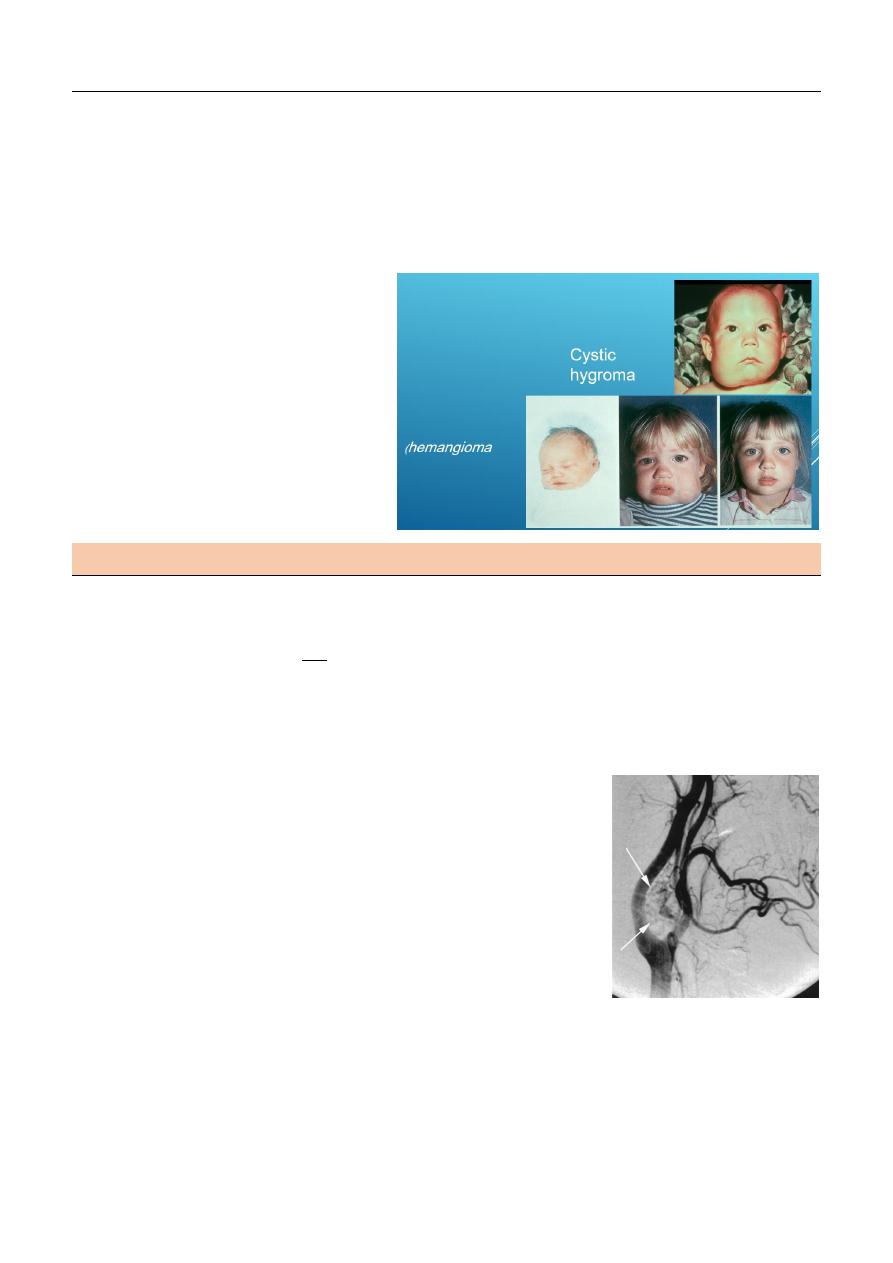
Vascular Tumors
Lymphangiomas and hemangiomas
Hemangiomas often resolve spontaneously, while lymphangiomas remain unchanged
CT/MRI may help define extent of disease
5
Treatment
Lymphangioma – surgical excision for;
- easily accessible
- lesions affecting vital functions
- Hemangiomas – surgical excision for
- rapid growth involving vital structures
- associated thrombocytopenia that fails medical therapy (steroids, interferon)
Carotid Body Tumor
Rare in children
Pulsatile, compressible mass
Mobile medial/lateral not superior/inferior
Clinical diagnosis, confirmed by angiogram or CT
Treatment
o Irradiation or close observation in the elderly
o Surgical resection for small tumors in young patients
Mubark A. Wilkins