Fifth Stage
Gynecology
Dr. Sumaya – Lecture 1
1
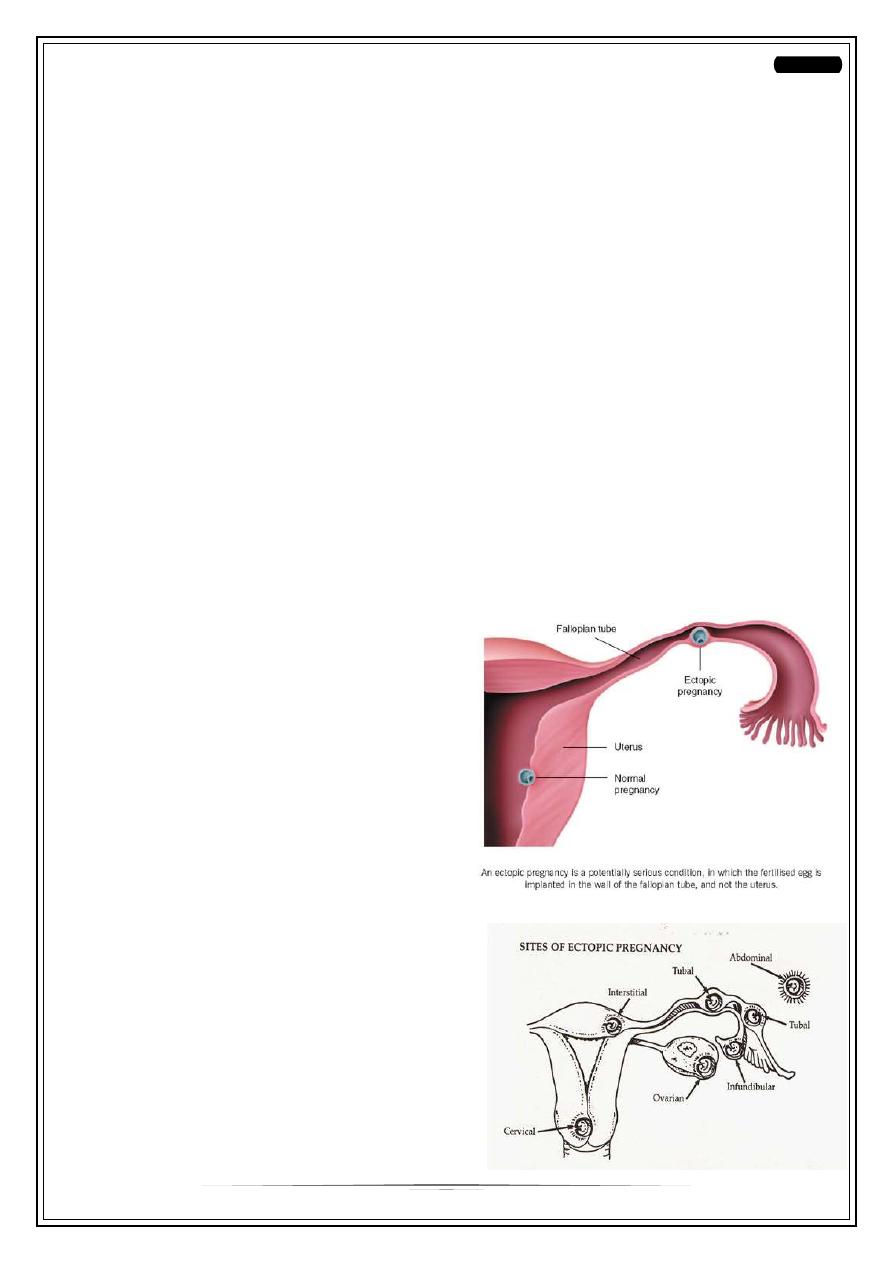
Ectopic Pregnancy
Definition:
Implantation of coceptus outside uterine cavity
Incidence; The incidence of ectopic pregnancy is11/1000pregnancies and the
mortality rate is around10/100 000. Approximately 11 000 cases of ectopic
pregnancies are diagnosed each year
The rising incidence of ectopic pregnancy :
1-early diagnosis of pregnancy can be made with the use of b-human chorionic
gonadotrophin (bHCG)
2-ultrasound scans to identify the location of an early pregnancy
Heterotopic pregnancy
Is the simultaneous development of a pregnancy within and outside the uterine
cavity. Although the incidence of a heterotopic pregnancy in the general population is
low (1:25 000– 30 000), the incidence is significantly higher after in vitro fertilization
(IVF) treatment (1 per cent).
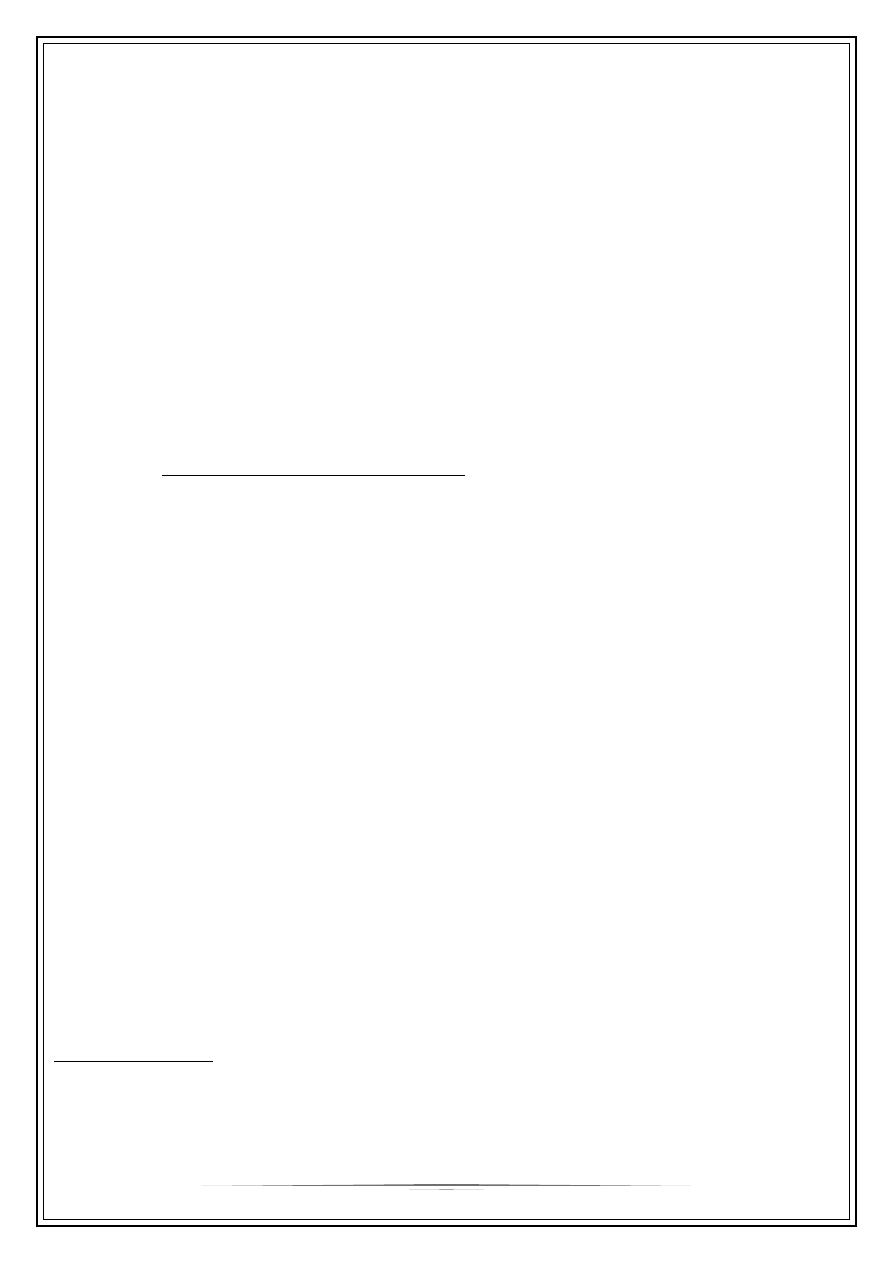
Common sites of implantation
Fallopian tubes (95 per cent)
ovaries (3 per cent)
peritoneal cavity (1 percent).
In the Fallopian tubes, the distribution of
sites:
the ampulla (74 per cent)
isthmus (12 per cent)
fimbrial end of the tube (12 per cent)
interstitium (2 per cent).
-
any mechanical or functional factors that
prevent or interfere with the passage of
the fertilized egg to the uterine cavity
may be aetiological factors for an ectopic
pregnancy.
2
Risk Factor for Ectopic Pregnancy
Previous PID – chlamydia infection 40%
Previous ectopic pregnancy
Tubal ligation
Previous tubal surgery
Intrauterine device
THE OUTCOME OF ECTOPIC PREGNANCY
The muscle wall of the tube has not the capacity of uterine muscles for
hypertrophy and distention and tubal pregnancy nearly always end in
rupture or death.
Tubal abortion – usually in ampullary about 8 weeks – forming pelvic
haematocele
Rupture into the peritoneal cavity:
Occur mainly from the narrow isthmus before 8 weeks or later from
the interstitial portion of the tube. Haemorrhage is likely to be
severe.
Sometimes rupture is extraperitoneal between the leaves of the broad
ligament – Broad ligament haematoma.
A high proportion of women with a tubal pregnancy miscarry during the early
stages of gestation.
The products of conception may persist for a considerable period of time within
the tube as one form of 'chronic ectopic pregnancy', or they may be gradually
absorbed.
Tubal pregnancy – effect on uterus
The uterus enlarge in first 3 months as if the implantation were normal,
reach the size of a gravid uterus of the same maturity.
Uterine decidua grows abundantly(Arias-Stella reaction). and when the embryo
dies bleeding occurs as the decidua degenerates due to effect of oestrogen
withdrawal.
Clinical Finding:
Variable - Early diagnosis
- location of the implantation
- Whether rupture has occurred
3
Classic symptom trait with unruptured ectopic pregnancy(subacute):
Amenorrhoea, abdominal pain, abnromal vagina bleeding(dark blood
indicate old blood)
Classic signs – adnexal or cervical motion tenderness.
With ruptured ectopic pregnancy(acute) finding parallel with the degree of
internal bleeding and hypovolemia – abdominal guarding and rigidity, shoulder
pain and fainting attacks and shock.
Pain – constant
- Cramp-like
-
It may be referred to the shoulder if blood tracks to the diaphragm
and stimulate the phernic nerve and it may be severe as to cause
fainting.
-
The pain caused by the distension of the gravid tube by its effort to
contract and expel the conceptus and by irritation of the peritoneum,
by leakage of blood.
-
Vaginal bleeding – occur usually after death of the fetus and is an
effect of oestrogen withdrawal. It is dark, scanty and its irregularity
may lead the patient to confuse it with the menstrual flow and give
misleading history.
25% of cases presents without any vaginal bleeding
-
Internal blood loss – severe and rapid. The usual sign of collapse and shock
and it is less common than the condition presenting by slow trickle of blood
into the pelvic cavity.
-
Peritoneal irritation: – muscle guarding
- frequency of micturation
- fever
-
Pelvic examination: – extreme tenderness
- cystic mass may be felt
-
Abdominal: -Tenderness in one or other fossa.
-General tenderness and resistance to palpation over whole
abdomen.
4
Differential diagnosis:
1. Salpingitis
2. Abortion
3. Appendecitis
4. Torsion of pedicle of ovarian cyst
5. Rupture of corpus luteum or follicular cyst
6. Perforation of peptic ulcer.
Diagnosis:
-Careful history about LMP its timing and appearance.
-Always think of tubal pregnancy women with lower abdomen pain in whom there
is possibility of pregnancy should be regarded as having an ectopic until proved
otherwise.
-Pregnancy test nearly always be found by the time of clinical presentation.
Investigation
• Observations: BP, pulse, temperature
• Laboratory investigations:
Haemoglobin, group and save (or crossmatch if patient is severely compromised)
HCG :This hormone is a glycoprotein produced by the placenta. It has a half-life of
up to 24 hours and peaks at around ten weeks. Pregnancy tests measure the b-
subunit of HCG.
A bHCG level of less than 5 mIU/mL is considered negative for pregnancy, and
anything above 25 mIU/ mL is considered positive for pregnancy. In 85 per cent of
pregnancies, the bHCG levels almost double every 48 hours in a normally
developing pregnancy.
In patients with ectopic pregnancies, the rise of bHCG is often suboptimal. However
bHCG levels can vary widely in individuals and thus often multiple readings are required
for comparison purposes.
Transvaginal ultrasound scan (TVS): An intrauterine gestational sac should be
visualized at about 4.5 weeks of gestation. The corresponding bHCG at that gestation is
around 1500 mIU/ mL. By the time a gestational sac with fetal heart pulsation is
detected (at around 5 weeks gestation), bHCG level should be around 3000 mIU/mL.
Hence, the interpretation of bHCG must be done in context with the clinical picture
and ultrasound findings.
5
Thus, if there were discrepancy between the bHCG concentrations and that seen on
ultrasound scan (e.g. a high bHCG with no intrauterine pregnancy on ultrasound scan),
the differential diagnosis of an ectopic pregnancymust be made.
Identification of an intrauterine pregnancy (gestation sac, yolk sac along with fetal
pole) on TVS effectively excludes the possibilityof an ectopic pregnancy in most patients
except in those patients with rare heterotopic pregnancy.
The presence of free fluid during TVS is suggestive of a ruptured ectopic pregnancy.
Laparoscopy: this can be used to diagnose and treat ectopic pregnancy.
Management
Ectopic pregnancy can be managed using an expectant, medical or a surgical
approach, depending on clinical presentation and patient choice.
Expectant
Expectant management is based on the assumption that a significant proportion
of all tubal pregnancies will resolve through regression or a tubal abortion without
any treatment.
This option is suitable for patients who are haemodynamically stable and
asymptomatic. This entails serial bHCG measurements and ultrasonography.
If haemorrhage and shock present
Restore blood volume by the transfusion of red cells or volume expander
Proceed with Laparotomy
Medical Managment
Methotrexate.
Indications:
Haemodynamically stable, no active bleeding, No haemoperitneum, minimal
bleeding and no pain
No contra indication to methotrexate
General anaesthesia poses a significant risk
cornual pregnancy;
patient with one Fallopian tube and fertility desired
treatment of ectopic pregnancy where trophoblast is adherent to bowel or blood
vessel.
6
Medical treatment should be offered only if facilities are present for regular follow-
up visits.
Systemic methotrexate is a treatment option for a carefully selected subgroup of
patients.
Methotrexate, a folic acid antagonist, inhibits DNA synthesis in trophoblastic cells.
It can be administered as a single intramuscular injection or in a multiple fixed
dose regimen.
The dose is calculated based on the patient’s body surface area and is 50 mg/m2.
Contraindications:
Breastfeeding
Immunodeficiency / active infection
Chronic liver disease
Active pulmonary disease
Active peptic ulcer or colitis
Blood disorder
Hepatic, Renal or Haematological dysfunction
Side Effects:
Nausea & Vomiting
Stomatitis
Diarrhea, abdominal pain
Photosensitivity skin reaction
Impaired liver function, reversible
Pneumonia
Severe neutropenia
Reversible alopecia
Haematosalpinx and haematoceles
Treatment failure and tubal rupture:
Significantly worsening abdominal pain, regardless of change in serum HCG
(Check CBC)
Haemodynamic instability
Level of HCG do not decline by at least 15% between Day 4 & 7 post
treatment
7
or plateauing HCG level after first week of treatment
Follow-Up:
Repeat HCG on Day 5 post injection if <15 % decrease – consider repeat
dose
If BHCG >15 recheck weekly until <25 ul/l
Surgery should also considered in all women presenting with pain in the first
few days after methotrexate and careful clinical assessment is required. If
these is significant doubt surgery is the safest option
SURGICAL MANAGEMENT:
Surgical treatment can be by laparoscopy or laparotomy.
Laparoscopic surgery is the mainstay of management
The laparoscopic approach offers significant advantage when compared to
laparotomy as it results in
less blood loss,
shorter operating time,
less analgesia requirement,
a shorter hospital stay and a
shorter convalescence than laparotomy..
Laparotomy
Is mainly reserved for
severely compromised patients
The lack of endoscopic facilities
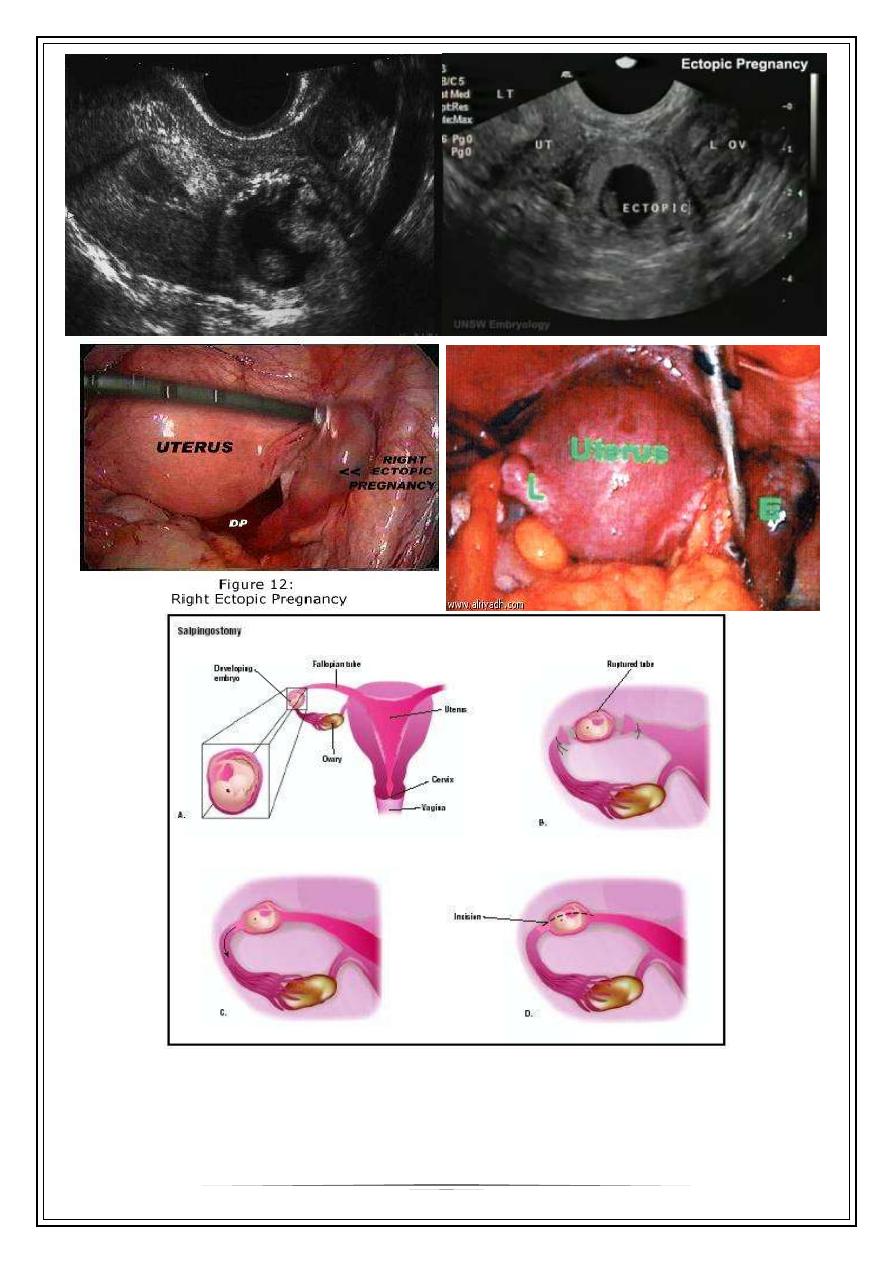
During surgery, the Fallopian tube can either be removed (salpingectomy) or
a small opening can be made at the site of the ectopic pregnancy and the
trophoblastic tissue extracted via the opening (salpingotomy).
In general, if the patient has a normal remaining tube, salpingectomy is the
treatment of choice.
Salpingotomy is thought to be associated with a higher rate of subsequent
ectopic pregnancy.
8
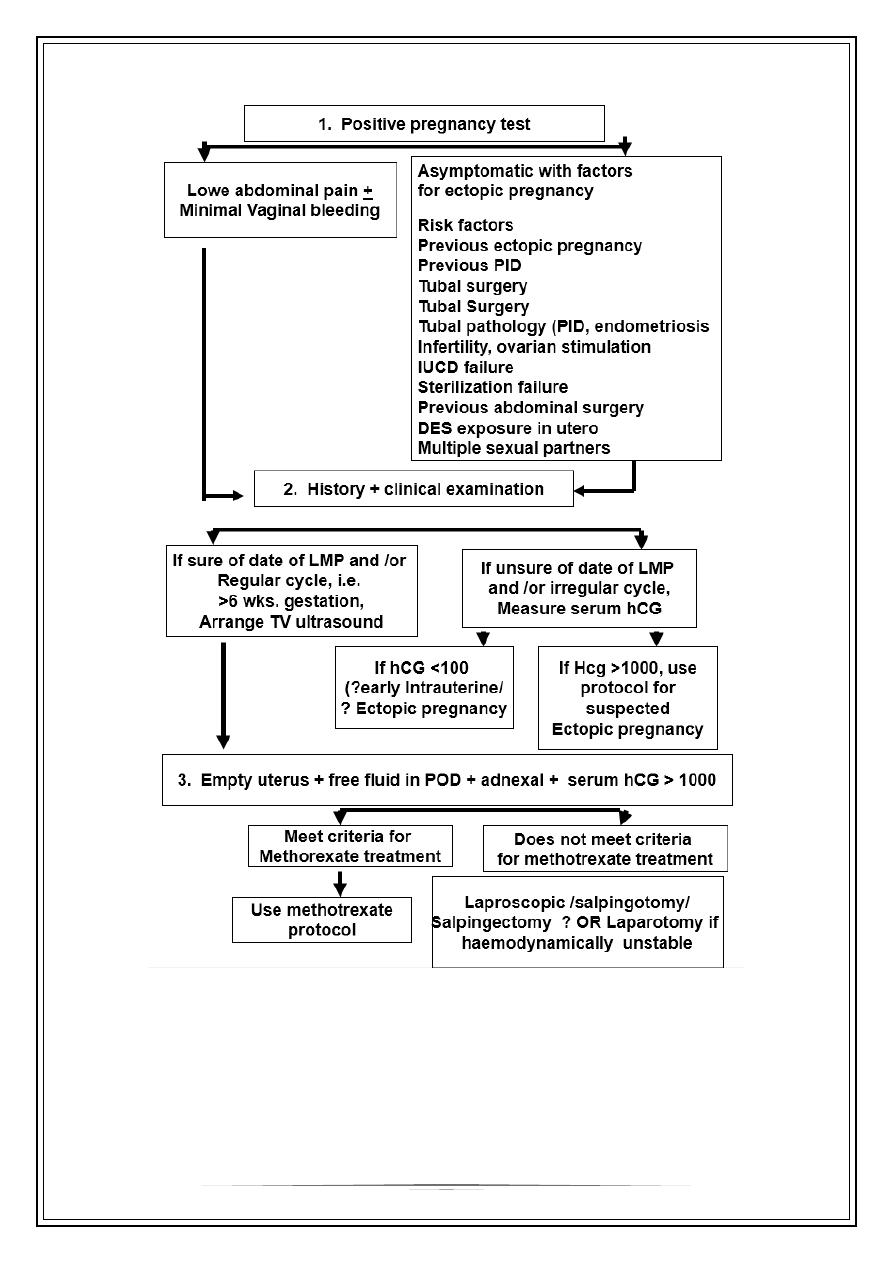
MANAGEMENT OF ECTOPIC PREGNANCY
9
In a woman of child bearing age with pelvi-abdominal pain and/ or vaginal
bleeding …… ALWAYS….think : -> Ectopic Pregnancy
Thank you,,,