
Chromoblastomycosis
Chromoblastomycosis is a specific type of cutaneous infection caused by
dematiaceous (pigmented) fungi. Symptoms are ulcerating nodules on exposed body
parts. Diagnosis is by appearance, histopathology, and culture. Treatment is with
itraconazole, another azole, or flucytosine and surgical excision.
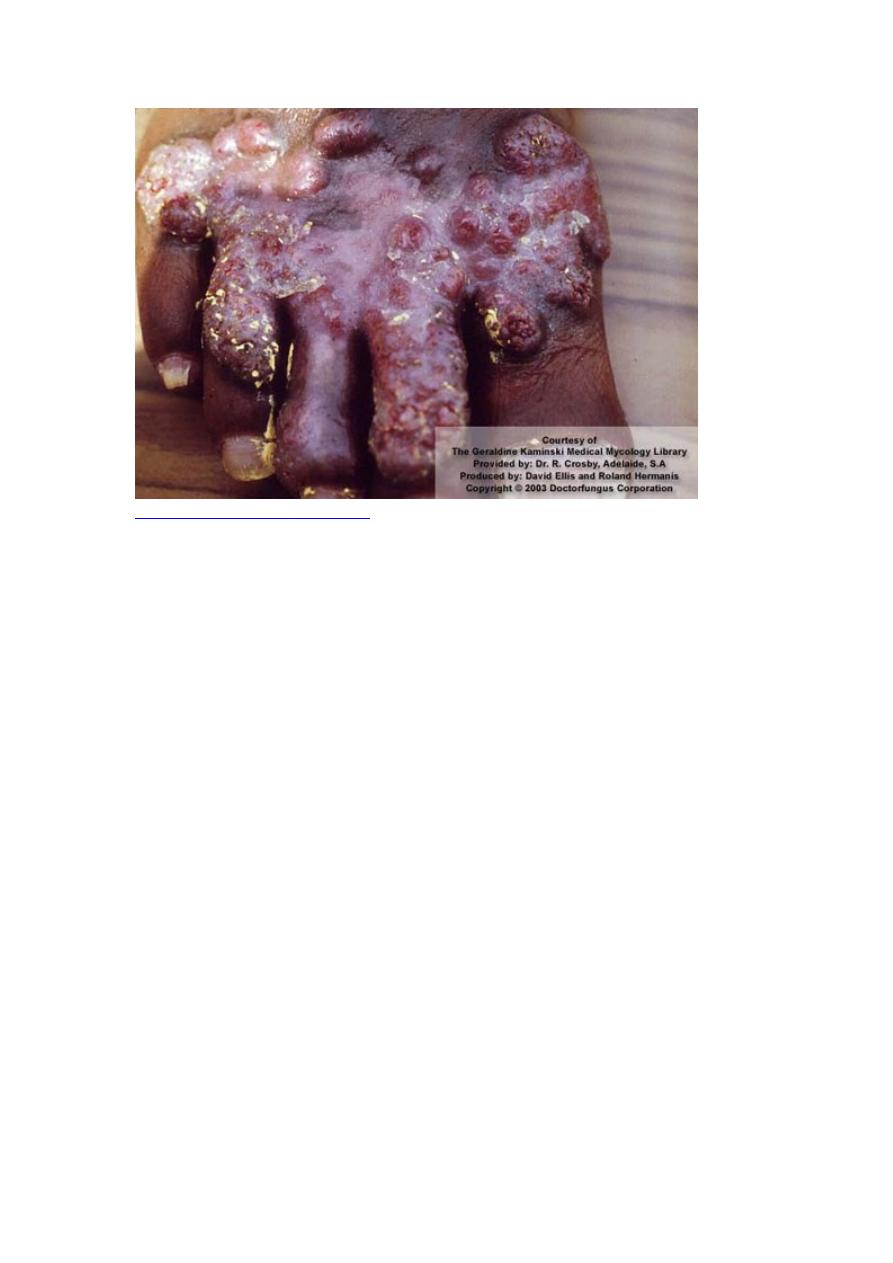
Chromoblastomycosis is a cutaneous infection affecting normal, immunocompetent
people mostly in tropical or subtropical areas; it is characterized by formation of
papillomatous nodules that tend to ulcerate.
Symptoms and Signs
Most infections begin on the foot or leg, but other exposed body parts may be
infected, especially where the skin is broken. Early small, itchy, enlarging papules
may resemble dermatophytosis (ringworm). These papules extend to form dull red or
violaceous, sharply demarcated patches with indurated bases. Several weeks or
months later, new lesions, projecting 1 to 2 mm above the skin, may appear along
paths of lymphatic drainage. Hard, dull red or grayish cauliflower-shaped nodular
projections may develop in the center of patches and, if the infection is untreated,
gradually extend to cover extremities over the course of many years. Lymphatics may
be obstructed, itching may persist, and secondary bacterial superinfections may
develop, causing ulcerations and occasionally septicemia.
Diagnosis
Histopathology
Culture
Late chromoblastomycosis lesions have a characteristic appearance, but early lesions
may be mistaken for dermatophytoses.
Fontana-Masson staining for melanin helps confirm the presence of the sclerotic
bodies (Medlar bodies), which are pathognomonic. Culture is needed to identify the
causative species.
Treatment
Itraconazole, sometimes with flucytosine
Often surgery or cryotherapy.
Itraconazole is the most effective drug, although not all patients respond. Flucytosine
is sometimes added to prevent relapse. Amphotericin B is ineffective. Anecdotal
reports suggest that posaconazole, voriconazole, or terbinafine may also be effective.
Adjunctive therapies such as cryotherapy are often helpful, although response is slow.
For localized lesions, surgical excision may be curative.