Connective tissue diseases
Dr. Ahmed Abdulhussein AL-HuchamiConnective Tissue diseases:
Are groups of clinico pathological conditions involve connective tissue of most systems of the body, include mainly LE, scleroderma, systemic sclerosis, dermatomyositis, MCTD &others…



Pathogenesis
Infectious agent e.g viral cross react with self-antigen in person with genetic backgroundPerpetuating factors:
Ultraviolet lightSex hormones
Stress
SLE criteria(4 out of 11)
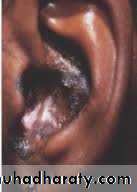
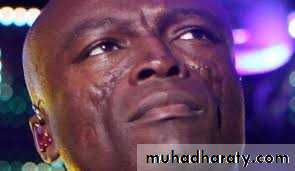
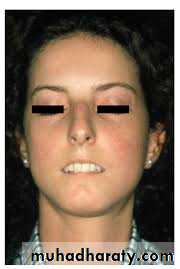
Malar(butterfly) rashDiscoid lesions
Photosensitivity
Oral ulcer
Arithritis
Serositis e.g. pleuritis, pericarditis
Renal: proteinuria, casts
Neurological: psychosis, seizure
Hematological: decreased platelets, WBC or RBC
Immunological: anti-DNA, anti-Sm, antiphospholipid antibodies
ANA
Drug-induced SLE
It is different from idiopathic SLE by (1) presence of anti-histone antibodies instead of ANA
Most commonly implicated drugs:
ProcainamideHydralazine
Minocycline
INH
Penicillamine
TNF- inhibitors
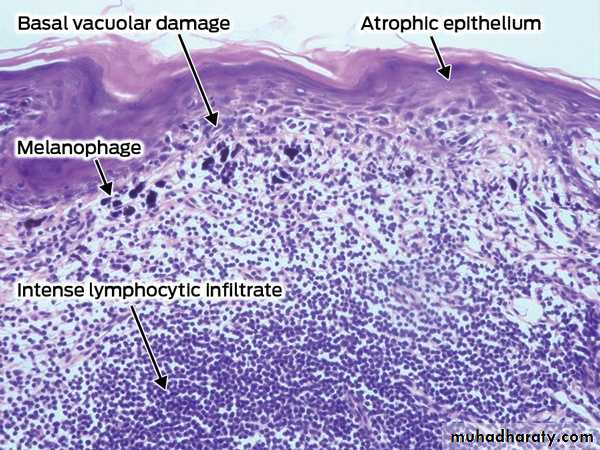
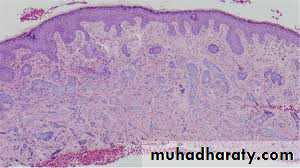
Pathology
Colloid bodies (damaged keratinocytes)Vacuolar changes in basal layer
Epidermal atrophy
Thickenening of basement membrane
Peri-adnexal, upper and lower dermal lymphocytic infiltrate
Mucin deposition
DIF (direct immunofluorescence) show granular deposit at DE junction (lupus band)a and around adnexa
Treatment
General: avoidance of sun and ppt factorSpecific :
Topical: Sun protection, topical and intralesional steroids
Systemic: Antimalarial e.g. hydroxychloroquine, chloroquine
Others: retinoids, thalidomide, dapsone
Morphea
Affect female more than maleDoes not affect survival but can cause a disability especially the linear type
Fibroblast isolated from morphea lesion produce increased amount of collagen and this is thought to be due to production of IL-4 and TGF-β by T-cells
Some believes that Borrelia plays a role
Types
1. Plaque-type : present as white indurated plaque surrounded by lilac border2. Deep morphea: invlove deep dermis, subcutis +/- fascia
3. Generalized morphea: plaques coaleasce affecting the entire trunk except nipple, can involves the extremities, it is disabiling causing difficulty in breathing,




4. Linear morphea: Mostly affect children
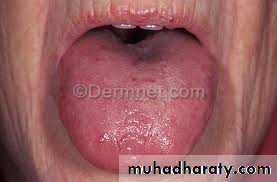
Variants:En coup de sabre type linear morphea of head, can involve muscle, bone
Parry-Romberg syndrome: hemifacial atrophy including eyes and tongue(the most severe form)



Diagnosis
Autoantibodies: ANA and anti-ssDNA are commonly seen in linear and generalized typesPathology: hyalinized and eosinophilic collagen bundles with a little space in between and atrophy of hair follicles and sweat glands
Treatment
Topical :Vit D analogues e.g. calcipotriol
Systemic treatment:
Glucocorticoids, methotrexate ,PUVA (psoralen plus UVA) and UVA1
Others: penicillin, penicillamine, acitretin , calcitriol and IFN-γ



Dermatomyositis
Classification (1):Juveile type: not associated with malignancy but associated with more calcinosis and vasculitis
Adult type: associated with malignancy especially ovarian, lung and breast
• Classification (2):
• Polymyositis (muscle only)
• Amyopathicdermatomyositis( skin only)
• Dermatomysitis (skin and muscle)
Clinical features
Cutaneous:
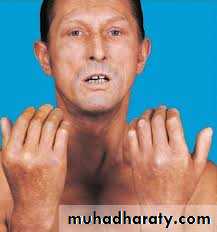
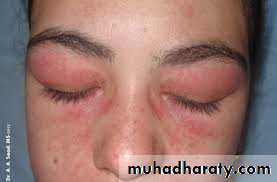
Heliotrop rash(violaceous patch and edema around eyes)
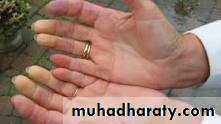
Gottron papules: flat-topped violaceous papules on knuckles
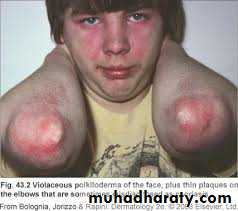
Gottron sign: violaceous discoloration of knuckles, elbows and knee
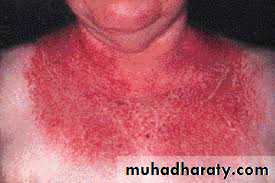
Photodistribution of skin manifestations(shawl)
Nail fold telengictasia





Systemic :
Proximal myopathy: inability to comb, to walk upstair or to stand from sitting positionLung: interstitial lung disease( restrictive lung disease)