
Refractive Errors (Ammetropia)
Introduction:
- Axial diameter: is the distance from tip of cornea to the center of macula,
which is normally 24mm.
- The most important two refractive surfaces are cornea and lens.
- The power of cornea and the lens depends on curvature of their surfaces, so
if we consider the cornea as a part of a sphere, it has a diameter of 7.8mm.
- The radius of curvature of anterior capsule of lens is 10 mm.
- The radius of curvature of posterior capsule of lens is 6 mm.
- If the curvature of cornea or lens is increased, or in other word, the radius
of cornea or lens is decreased, then there is increase in refractive power of
these structures and vice versa.
- For rays to come parallel, their source must be at distance of six meters and
more from the eye, and if the source of rays is at distance less than 6 meters,
then the rays will come divergent. The more close the source of rays to the
eye, the more divergent they are.
Emmetropia (normal refraction):
It is an eye in which parallel rays (i.e. from infinity, 6 meters or more) of
light come to a focus directly on the retina when the eye is at rest {i.e.
without accommodation = the eye is using its normal power (60D) only}.
- Accommodation: contraction of Ciliary muscle in order to increase
curvature of lens (and so increase its refractive power more than 17D) to
visualize objects closer than 6 meters (near objects).
- In order to see near objects, there will be contraction of Ciliary muscles
which lead to decrease the tone of Zonule and their will be increase in the
curvature of lens and increasing in the refractive power of lens (>60D).
- Amplitude of accommodation (difference between maximum contraction
and complete relaxation, which depends on contraction power of Ciliary
muscles and elasticity of capsule, and both of them decrease with advancing
in age). Amplitude of accommodation decrease with advancing age as the
following:
* Early in life: it is 14D, so children can focus on objects 7cm away from
their eyes, so the range of lens refractive power can be increase from 17D
to 31D.
* At age of 36y: due to atrophy of muscles and loss of lens elasticity
(sclerosis), amplitude of accommodation will be 6D only, so the nearest
object to the person which can be focused is at a distance of about 15cm
away from eye.
* At age of 45y: amplitude of accommodation is 4D only, and the nearest
focus point is 25cm away from eye.
* At age of 60y: amplitude of accommodation is 1D only, and the nearest
focus point is 1m.
Ammetropia: → Hypermetropia
→ Myopia
→ Astigmatism
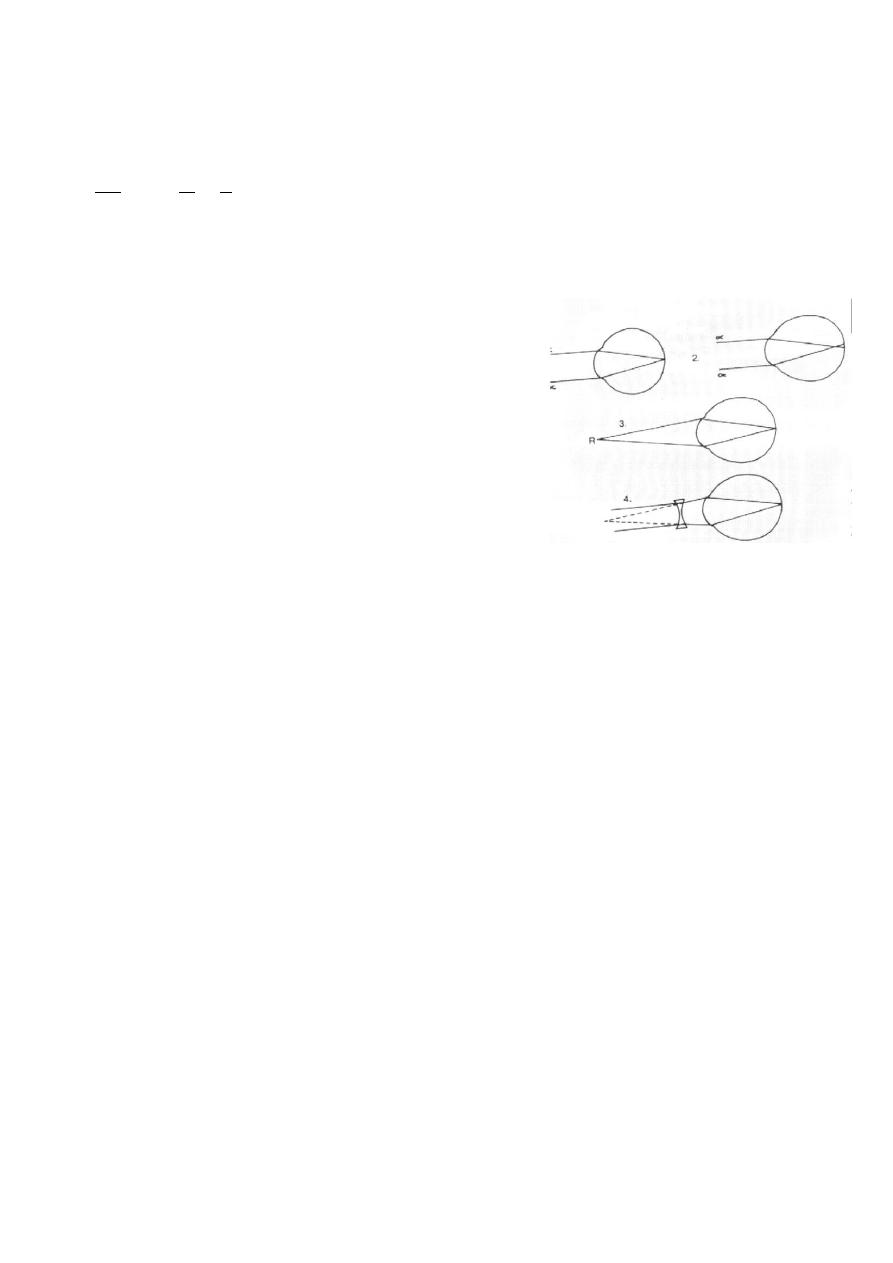
Hypermetropia (hyperopia), far-sightedness:
Is a type of refractive errors in which parallel rays
of light are brought to a focus some distance behind
the retina when the eye is at rest.
Etiological classification:
1- Axial Hypermetropia: shorter antero-posterior
axial length, i.e. the eye has normal converging
power (60D) but its axial length is less than 24 mm.
2- Curvature Hypermetropia: due to decreased
curvature (flattening) of the cornea congenitally or as a result of trauma or
disease e.g. corneal ulcer, microbial keratitis.
3- Index Hypermetropia: decrease in effective refractivity of the lens.
* power of lens depends on difference between refractive indices of the
nucleus and cortex, so the more the difference the more converging power
and vise versa. In index Hypermetropia, there is decrement of the difference.
Clinical classification:
1- Facultative hypermetropia: hypermetropia corrected by accommodation
(depends on age and degree of refractive error).
2- Absolute hypermetropia: hypermetropia out of amplitude of
accommodation and corrected by glasses.
3- Manifest hypermetropia: maximum hypermetropia that can be corrected
with a convex lens with accommodation active, i.e. = Facultative + Absolute.
4- Latent hypermetropia: hypermetropia hidden behind ciliary body tone
which equal to the difference between total and manifest hypermetropia. The
refractive power of the ciliary body is about 1-1.5D (usually it considered as

part of the refractive power of lens, i.e. 17D of lens = 16D + 1D (of the
ciliary body tone), it also decreases with age.
5- Total hypermetropia: amount of hypermetropia present with all
accommodation
suspended
(with
cycloplegic
drugs,
to
exclude
accommodation and tone of ciliary body) Manifest + Latent.
* With advancing in age, the facultative will decrease and the manifest
will be represented by absolute only, and at the same time, the latent will
also decrease and the total will be represented by manifest only, so in old
people the total is made of the absolute only.
Diopter: the reciprocal of the distance in meters from the reference light
source in air or vacuum, such that D= 1/(distance in meters).
Symptoms:
1- Blurred vision: for near work (as it needs more power) and even far vision
if the degree (of hypermetropia) beyond amplitude of accommodation.
2- Eye strain: headache due to excessive accommodation and dissociation
between Accommodative Convergence and Accommodation "AC/A:
Accommodative Convergence to Accommodation ratio" (due to continuous
contraction of ciliary muscle without interruption).
* To see the near objects, the eye will show the near reflex, which consists
of accommodation, convergence and miosis. When one of these processes
occurs, it will stimulate the other two. Here we are concerned with
accommodation
and
convergence.
Normally,
for
each
1D
of
accommodation, there will be associating 4 prism D convergence (i.e.
AC/A=4 prism D/1D). Therefore, in hypermetropia where we have
dissociation or disorganization between accommodation and convergence
causing headache and eye strain as in the following example:
A normal eye to see an object at distance of 50 cm needs 2D and this in
turn will produce 8 prism D convergence, while an eye with 7D
hypermetropia has at rest 28 prism D convergence, so to see an object at
50cm distance the 2D needed will produce 8 prism D more, so totally we
have 36 prism D.
3- General symptoms like nausea and fatigue.
Treatment:
- Convex lens in spectacles (+ve lenses to increase refractive power).
- Contact lenses.
- Excimer laser photorefractive keratectomy: reshaping of the cornea to
increase the refractive power, each 1mm decrease in radius of curvature
increases the refractive power about 6D.
- Laser in situ keratomileusis (Lasik).
- Non-contact laser thermal keratoplasty (Holmium laser spots): to change
the coneal curvature.
- Phakic intraocular lens (IOL).
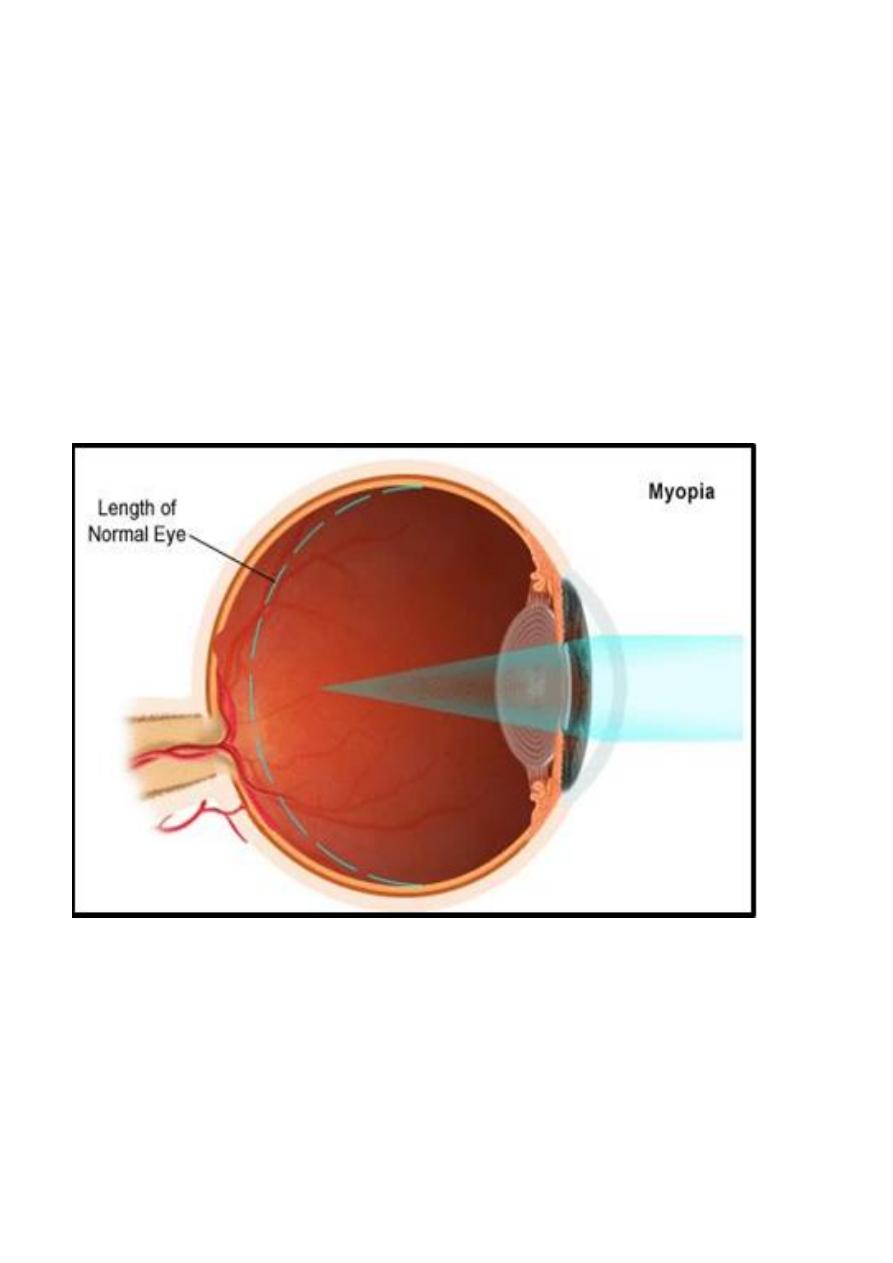
Myopia or short-sightedness:
That form of a refractive error where parallel
rays of light come to a focus in front of the
retina when the eye is at rest.
- As there is increase in the refractive power
of the eye, the near objects (closer than 6m)
will be seen normally, while far objects (whom
rays come parallel) will be focused in front of
retina.
Aetiological classification:
1- Axial myopia: anteroposterior length is longer than normal.
2- Curvature myopia: increased curvature of cornea, or one or both
surfaces of lens.
3- Index myopia: increased refractivity of lens, e.g. nuclear sclerosis (stage
before nuclear cataract), due increase the difference between refractive
indices of nucleus and cortex.
Clinical classification:
1- Simple (stationary): <6D, after the age of 4y, stationary (stops before
20y), normal physiological process and can be corrected.
2- Pathological (progressive): >6D, before the age of 4y, progress even
after age of 20y, real pathological process and cannot be corrected as the
real pathological process still found (if the patient has myopia of 20D, then
even if we give glasses with -20D, he will still having refractive error).
Symptoms:
1- Distance object "Blurred", near objects clear.
2- Headache due to sustained contraction of occipito-frontalis muscle, eye
strain due to dissociation of AC/A.
* A normal eye to see an object at distance of 50 cm needs 2D
(1/0.5m=2D) and this in turn will produce 8 prism D convergence, while a
eye with 2D myopia will not need any accommodation to see this object, but
there will convergence 8 prism D to see this near object. Thus is in turn will
produce 2 D accommodation which is not needed by myopic patient. So any
myopic should wear glasses for near to create normal relation between
accommodative convergence and accommodation.
3- general symptoms like fatigue and nausea.

6
Treatment:
- Concave lenses in spectacles.
- Contact lens
- Radial keratotomy
- Excimer laser photorefractive keratectomy.
- Lasik.
- Pkakic IOL.
- Normal Lens extraction:
Astigmatism
Astigmatism is that condition of refraction in which a point of focus of
light cannot be formed upon the retina. The optical condition is that
instead of a single focal point, there are two or more focal lines (depending
on the type of astigmatism), separated from each other by a focal interval.
Etiological classification:
1- Curvature astigmatism: Most commonly, it is corneal, where vertical
curvature is more than horizontal curvature (due to pressure of the upper
eyelid), less commonly it is lenticular (induced by lens).
2- Decentering astigmatism: subluxation of lens.
3- Index astigmatism: due to cataract in one meridian.
Clinical classification:
1- Regular: two principle meridians at right angle are involved (i.e. there
is difference in the refractive power of two meridians 90° in between):
a- Simple astigmatism: myopic or hypermetropic; one of the foci falls
on retina, other in front or behind it.
b- Compound astigmatism: neither of the two foci lies upon retina, but
are both placed in front or behind retina (myopic or hypermetropic
respectively).
c- Mixed astigmatism: one focus in front and other behind retina.
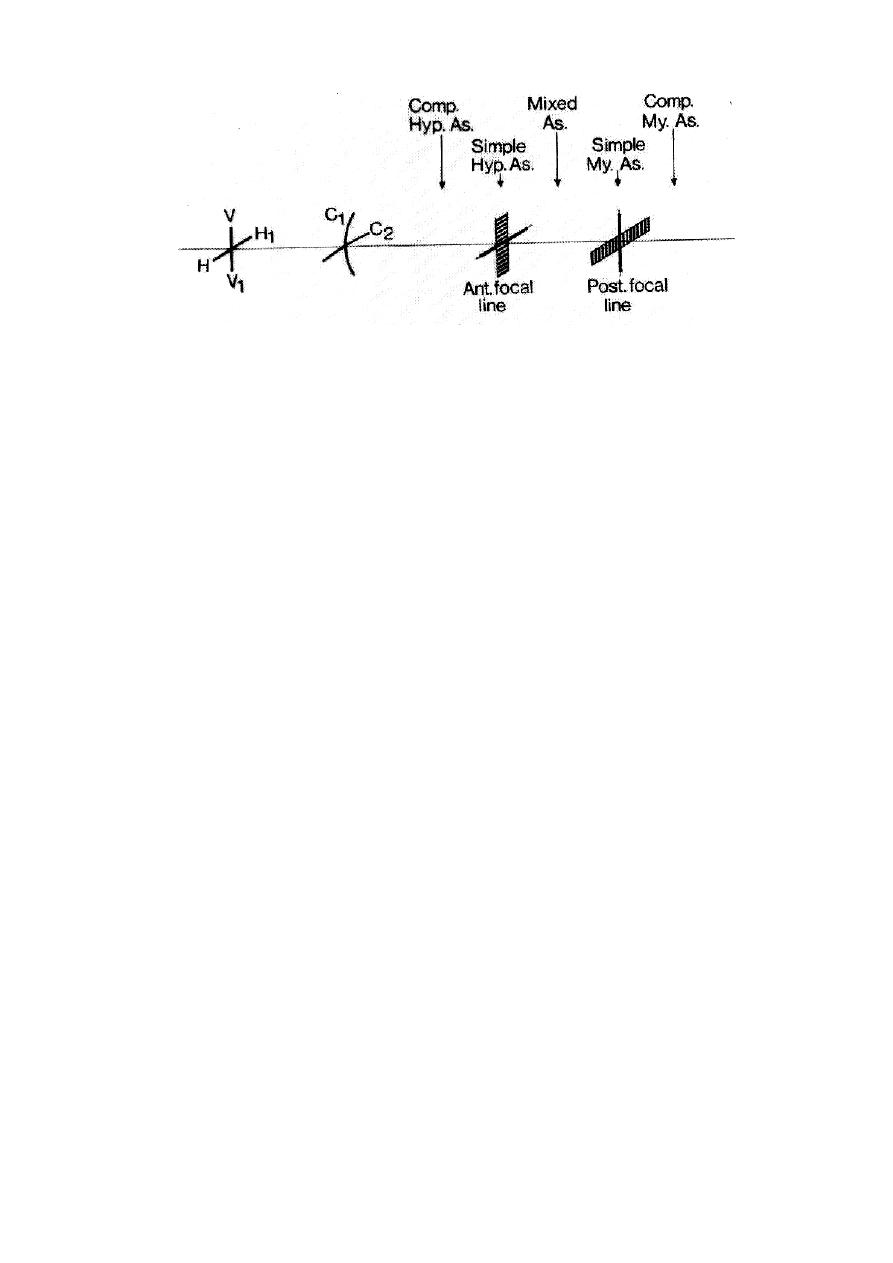
7
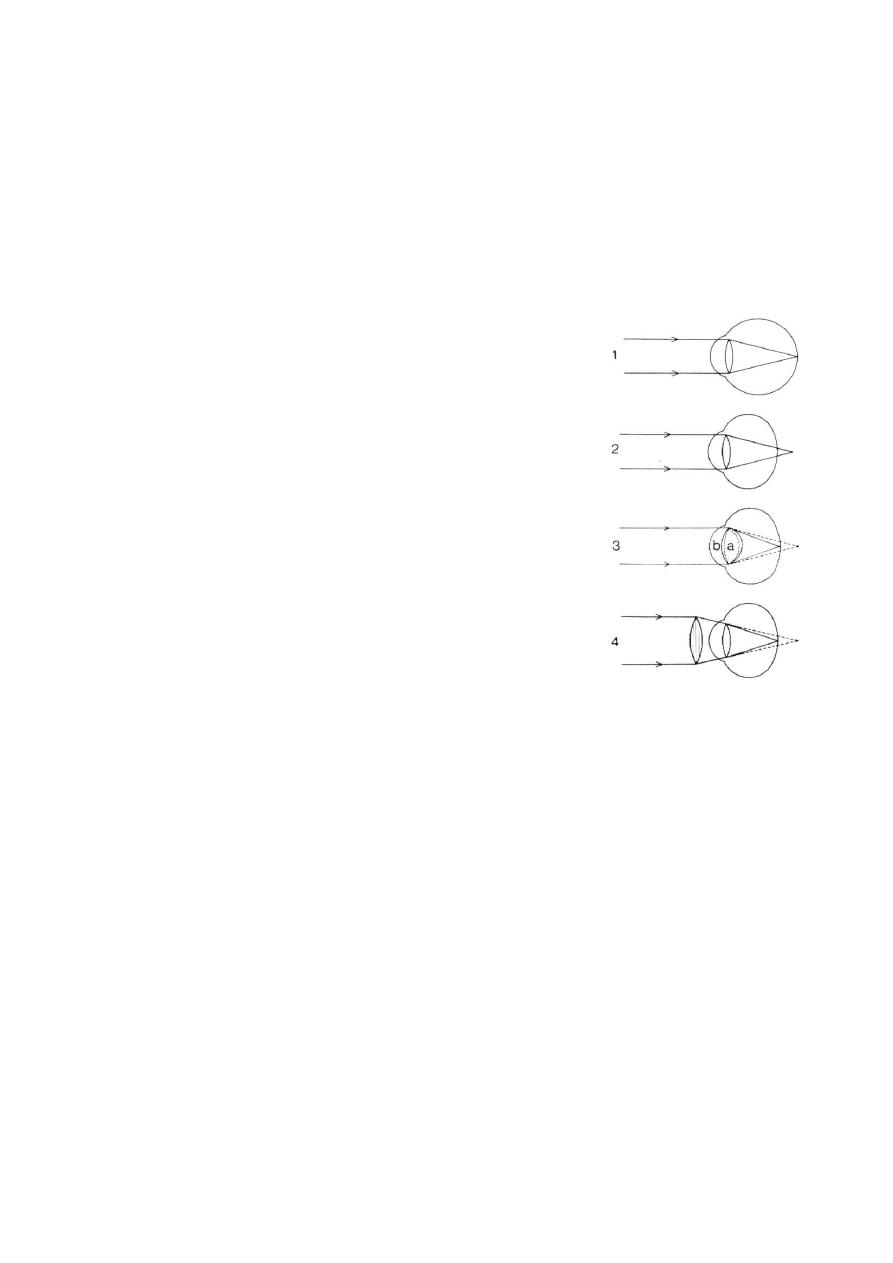
* This figure represents the appearance of the image in astigmatism
(regular), we have two perpendicular meridians; vertical (V-V
1
) and
horizontal (H-H
1
), we see that the refractive power of the vertical
meridian is larger than that of horizontal one as the curvature of the
vertical meridian (C
1
) is larger than the curvature of the horizontal
meridian (C
2
).
So as we see in (1), the image of vertical meridian is focused as (A
1
)
line on the retina (normal), while the horizontal meridian image focused
behind the retina (hypermetropic) and blurred on retina as (B
1
) line, so it
is called "Simple hypermetropic astigmatism". In (2), vertical
meridian image is focused in front of the retina (myopic) and its image
on retina is blurred (A
2
), while horizontal meridian image (B
2
) is focused
on the retina (normal), so it is called "Simple myopic astigmatism". In
(3) and (4) both image are focused behind or in front of retina
respectively and called "Compound hypermetropic or myopic
astigmatism". While in (5), one image focused in front of and the other
behind the retina and so it is called "Mixed astigmatism".
Treatment:
- Cylindrical lenses in spectacles: only for simple astigmatism.
-Contact lenses: used for compound and mixed astigmatism, where we
correct one of the meridians by them, and then correct the other meridian
by cylindrical lenses (i.e. we switch it to simple and correct it
accordingly).
- Photorefractive Excimer laser surgery: Also we correct one meridian.
-LASIK: like photorefractive Excimer laser surgery, but used for higher
refractive error.
- Phakic Toric IOL.
3 1 5 2 4
A
1
A
2
B
1
B
2

8
2- Irregular astigmatism: refraction in different meridians is quite
irregular. Found in pathological condition of cornea; irregular healing
after trauma or inflammations or keratoconus.
Treatment:
Rigid contact lenses to convert the irregular anterior surface into a
regular one.
Penetrating keratoplasty can be done if vision does not improve
with rigid contact lens.
PRESBYOPIA
Definition
Presbyopia is recession of the near point, due loss of accommodation
with ageing making near vision uncomfortable.
Mechanism
The crystalline lens become hard with age and loses its ability to change
its shape.
Symptoms
Difficult near vision usually occurs around the age of 45 in a previously
emmetropic eye
Correction of presbyopia
1. Eyeglasses: plus lenses (added to the far correction) are used
compensate for the lost automatic focusing power of the crystalline lens.
The near correction may occupy the whole spectacle frame, to be used
only for reading.
The near correction may occupy only the lower half of a bifocal spectacle
so that it can be used for both near and far vision (the upper part for far,
the lower part for near).
A multifocal spectacle contains progressive lenses that correct for all
distances by gradual change of power from furthest to nearest towards the
lower segment of the lens.
2. Multifocal contact lenses have been tried with limited success.
3. Multifocal intraocular lenses may used during cataract extraction.
4. Surgical correction of presbyopia(refractive surgery).

9
REFRACTIVE SURGERY
Definition:
Refractive surgery is the modification of refraction of the eye by surgical
interference.
Indications:
It is only indicated when glasses and contact lenses cannot be used due to:
Optical reasons as anisometropic with intolerance to contact lenses.
Mechanical reasons as nose and orbit configuration difficult to fit
spectacles with intolerable contact lenses.
Cosmetic and job reasons as people working in the media and sport
fields and contact lens intolerance.
Classification
A- Extra ocular surgery which may be :
Corneal
1. Radial keratotomy, where radial incisions were done to weaken the
cornea and make it flatter by the effect of IOP to correct low myopia.
The procedure is rarely used nowadays and only for mild myopia of
< -4.00D.
Astigmatic keratotomy where corneal incisions are done to flatten the
steep meridian.
2. Excimer laser ablation of the anterior corneal surface either by PRK
(Photorefractive Keratectomy) or LASIk (laser in Situ
Keratomileusis) can correct low and moderate myopia, astigmatism,
and low hyperopia.
In PRK, the laser ablation is done on the surface of the cornea after
removing the overlying epithelium. It can be used in low myopia < -5.00D
In LASIK, a corneal flap is made using a special microkeratome under
local anesthesia. The excimer laser is directed to the center of the cornea,
ablating (removing) part of the corneal thickness in a calculated manner.
The flap is returned.

10
This method has been successfully used in errors up to -10 D in myopia in
addition to astigmatism and low hyperopia.
3. Laser thermokeratoplasty (LTK) can be used to treat low hyperopia.
4. Corneal rings are used in keratoconus or low myopia.
B- Inraocular surgery which may be:
1. ICL (Implantable contact lens)
2. Phakic IOL