INFLAMM4444vbddATORY BOWEL DISEASE
4
th
stage lec: 5 GIT
.ا
.م
.د
ﺣ
ﺴ
ﻦ
ا
7
8
ﻤ
ﻴ;
<
Inflammatory bowel diseases
Ulcerative colitis and Crohn’s disease are chronic inflammatory bowel diseases with a protracted
relapsing and remitting course, usually extending over years. A crucial distinction is that ulcerative
colitis only involves the colon, while Crohn’s disease can involve any part of the gastrointestinal tract
from mouth to anus.
Pathophysiology
Genetic:
1-Both CD and UC common in Ashkenazi Jews
2- High concordance in identical twins (40–50% CD; 20–25% UC)
3- UC and CD both associated with genetic variants at HLA locus, and with multiple genes involved
with immune signalling (esp. IL-23 and IL-10 pathways)
4- HLA-DR 103 associated with severe UC
Environmental
• UC more common in non-smokers and ex-smokers
• CD more common in smokers
• CD associated with high-refined-sugar diet
• Commensal gut microbiota altered in CD and UC
• Appendicectomy protects against UC
Ulcerative colitis
-Proctitis 40–50% ,Left-sided colitis 30–40% and Extensive colitis 20%.
- In long-standing pancolitis, the bowel can become shortened and post-inflammatory ‘pseudopolyps’
-The inflammatory process is limited to the mucosa and spares the deeper layers of the bowel wall
,both acute and chronic inflammatory cells infiltrate the lamina propria and the crypts (‘cryptitis’).
Crypt abscesses are typical.
- Dysplasia, nuclear atypia and increased mitotic rate, may herald development of colon cancer.
Crohn’s disease
-The sites most commonly involved are, in order of frequency, the terminal ileum and right side of
colon, colon alone, terminal ileum alone, ileum and jejunum.
-The entire wall of the bowel is oedematous and thickened, and there are deep ulcers which often
appear as linear fissures; thus the mucosa between them is described as ‘cobblestone’. These may
penetrate through the bowel wall to initiate abscesses or fistulae involving the bowel, bladder,
uterus, vagina and skin of the perineum.
-The mesenteric lymph nodes are enlarged and the mesentery is thickened.
Clinical features
Ulcerative colitis:
-The cardinal symptoms are rectal bleeding with passage of mucus and bloody diarrhoea. The
presentation varies depending on the site and severity of the disease.
-Emotional stress, intercurrent infection, gastroenteritis, antibiotics or NSAID therapy may all
provoke a relapse. -
-Proctitis causes rectal bleeding and mucus discharge, accompanied by tenesmus.
-Some patients pass frequent, small volume fluid stools, while others pass pellety stools due to
constipation.
-assessment of severity depend on:
- Daily bowel frequency , Blood in stools , Stool volume , Pulse ,Temperature ,Haemoglobin , ESR &
C-reactive protein ,Serum albumin , Abdominal X-ray and Sigmoidoscopic finding.
The Truelove–Witts criteria for acute severe ulcerative colitis are ≥ 6 bloody stools/24 hrs plus one
or more of anaemia, fever, tachycardia and high inflammatory markers.
Crohn’s disease:
-The major symptoms are abdominal pain, diarrhoea watery and does not contain blood or mucus.
and weight loss.
-Ileal Crohn’s disease may cause subacute or even acute intestinal obstruction.
-Weight loss because they avoid food, since eating provokes pain also due to malabsorption, and
some patients present with features of fat, protein or vitamin deficiencies.
-Crohn’s presents in an identical manner to ulcerative colitis, but rectal sparing and the presence of
perianal disease are features which favour a diagnosis of Crohn’s disease.
-A few patients present with isolated perianal disease, vomiting from jejuna strictures or severe oral
ulceration.
- Perianal skin tags, fissures or fistulae are found in at least 50% of patients.
Differential diagnosis
1-Infective
-Bacterial • Salmonella • Shigella • Campylobacter jejuni • E. coli O157 • Pseudomembranous colitis
-Viral • Herpes simplex proctitis • Cytomegalovirus
Protozoal • Amoebiasis
Non-infective
• Ischaemic colitis • Radiation proctitis • Collagenous colitis
• Behçet’s disease • NSAIDs • Colonic carcinoma• Diverticulitis
Complications
1-Life-threatening colonic inflammation:
In the most extreme cases, the colon dilates (toxic megacolon) and bacterial toxins pass freely across
the diseased mucosa into the portal and then systemic circulation.
. An abdominal X-ray should be taken daily because, when the transverse colon is dilated to more
than 6 cm .there is a high risk of colonic perforation, this complication can also occur in the absence
of toxic megacolon.
2-Haemorrhage :due to erosion of a major artery.
3-Fistulae
These are specific to Crohn’s disease. Enteroenteric fistulae. Enterovesical fistulation causes
recurrent urinary infections and pneumaturia. An enterovaginal fistula causes a faeculent vaginal
discharge.
Fistulation from the bowel may also cause perianal or ischiorectal abscesses, fissures and fistulae.
4-Cancer
-The risk of dysplasia and cancer increases with the duration and extent of uncontrolled colonic
inflammation.
Thus patients who have long-standing, extensive colitis are at highest risk.
-Oral mesalazine therapy reduces the risk of dysplasia and neoplasia in ulcerative colitis. Azathioprine
also seems to reduce the risk of colorectal cancer in ulcerative colitis and Crohn’s colitis.
-Patients with long-standing colitis are therefore entered into surveillance programmes beginning 10
years after diagnosis. Targeted biopsies of areas that show abnormalities on staining with indigo
carmine or methylene blue increase the chance of detecting dysplasia and this technique (termed
pancolonic chromo-endoscopy) has replaced colonoscopy with random biopsies taken every 10 cm in
screening for malignancy. The procedure allows patients to be stratified into high-, medium- or low-
risk groups to determine the interval between surveillance procedures.
If high-grade dysplasia is found, panproctocolectomy is usually recommended because of the high
risk of colon cancer.
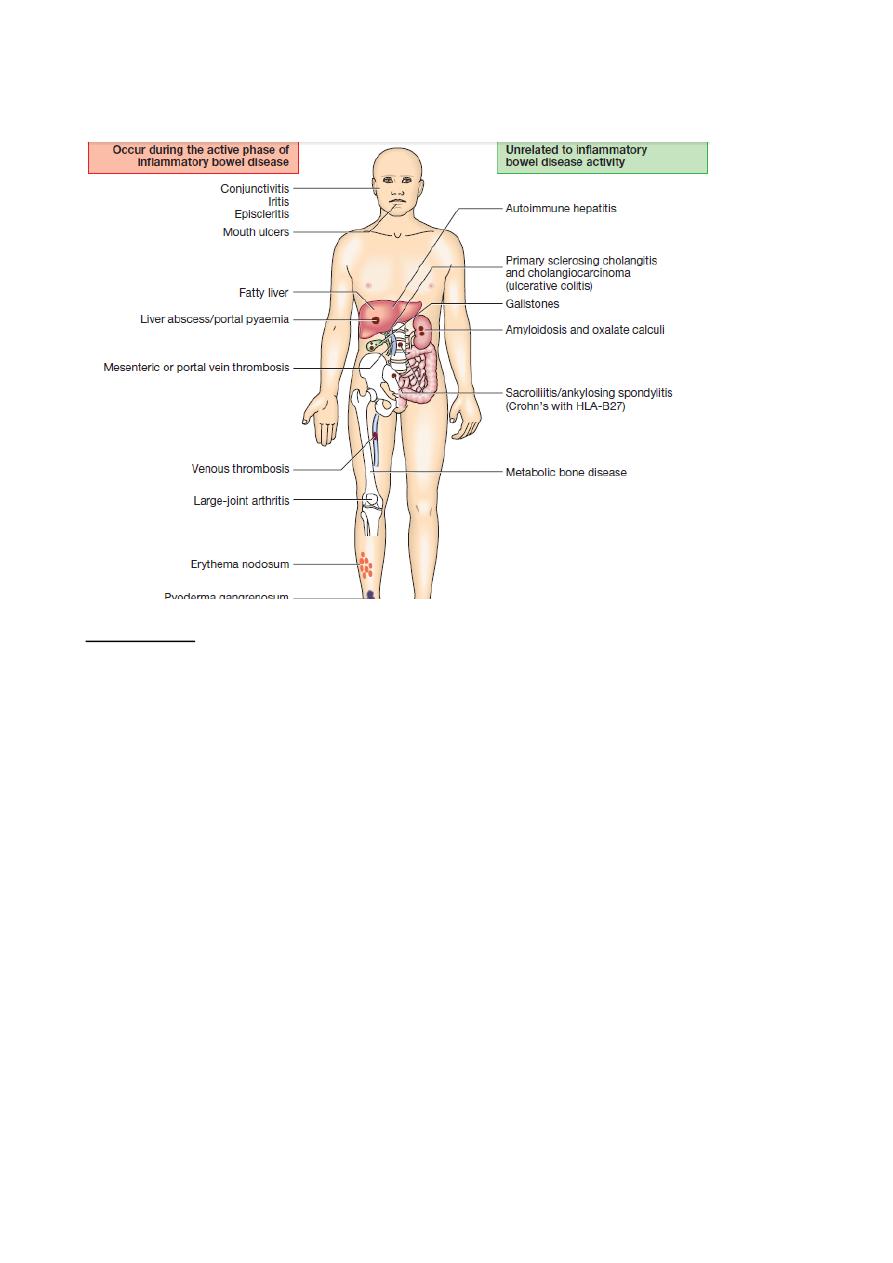
5-Extra-intestinal complication:
Investigations
▲
Blood:
1-Full blood count may show anaemia resulting from bleeding or malabsorption of iron, folic acid or
vitamin B12.
2-Serum albumin concentration falls as a consequence of protein-losing enteropathy, inflammatory
disease or poor nutrition.
3- The ESR and CRP are elevated in exacerbations and in response to abscess formation.
4-Faecal calproctectin has a high sensitivity for detecting gastrointestinal inflammation
▲
Bacteriology
-stool microscopy, culture and examination for Clostridium difficile toxin or for ova and cysts, blood
cultures and serological tests should be performed.
▲
Endoscopy
-Patients who present with diarrhoea plus raised inflammatory markers or alarm features, such as
weight loss,
bleeding and anaemia, should undergo ileocolonoscopy
-In ulcerative colitis, there is loss of vascular pattern, granularity, friability and contact bleeding,
with or without ulceration.
- In Crohn’s disease, patchy inflammation, with discrete, deep ulcers, strictures and perianal disease
(fissures, fistulae and skin tags), is typically observed, often with rectal sparing. In established disease,
colonoscopy may show active inflammation with pseudopolyps or a complicating carcinoma.
▲
Radiology
1-Barium enema is a less sensitive investigation than colonoscopy in patients with colitis and, where
colonoscopy
is incomplete, a CT colonogram is preferred.
2- Traditional contrast imaging by barium follow-through demonstrates affected areas of the bowel
as narrowed and ulcerated, often with multiple strictures . This has now largely been replaced
by MRI enterography
3- A plain abdominal X-ray is essential in the management of patients who present with severe active
disease. Dilatation of the colon, mucosal oedema (thumb-printing) or evidence of perforation may be
found. In small bowel Crohn’s disease, there may be evidence of intestinal obstruction or
displacement of bowel loops by a mass.
4-Ultrasound is a very powerful tool to detect small bowel inflammation and stricture formation
5-The role of CT is limited to screening for complications, such as perforation or abscess formation
Management
. The key aims of medical therapy are to:
• treat acute attacks (induce remission)
• prevent relapses (maintain remission)
• prevent bowel damage
• detect dysplasia and prevent carcinoma
• select appropriate patients for surgery.
♠
Ulcerative colitis
1-Active proctitis. suppository ± oral 5-aminosalicylate (5-ASA) therapy. resistant disease
→corticosteroids and immunosuppressants.
2-Active left-sided or extensive ulcerative colitis.
mild to moderate :
- combination of oral and a topical 5-ASA preparation is usually effective. The oral 5-ASA is continued
long-term to prevent relapse and minimise the risk of dysplasia.
-In patients who do not respond to this approach within 2–4 weeks, steroid indicated.
Corticosteroids should never be used for maintenance therapy. At the first signs of corticosteroid
resistance (lack of efficacy) or in patients who require high corticosteroid doses to maintain control→
immunosuppressive therapy with a thiopurine should be introduced.
Severe ulcerative colitis.
• Admit to hospital for intensive therapy and monitoring
• Intravenous fluids and correction of electrolyte imbalance
• Transfusion if haemoglobin < 10 g/dL
• IV methyl prednisolone (60 mg daily) or hydrocortisone (400 mg daily)
• Antibiotics until enteric infection excluded
• Nutritional support
• Subcutaneous low-molecular-weight heparin for prophylaxis of venous thromboembolism
• Avoidance of opiates and antidiarrhoeal agents
• Consider infliximab or ciclosporin in stable patients not responding to 3–5 days of corticosteroids
3-Maintenance of remission.
-Life-long maintenance therapy is recommended for all patients with left-sided or extensive disease
.Once-daily oral 5-aminosalicylates are the preferred first-line agents.
-Patients who frequently relapse despite aminosalicylate drugs should be treated with thiopurines.
♠
Crohn’s disease
A-Induction of remission.
1-Corticosteroids remain the mainstay of treatment for active Crohn’s disease
2-Calcium and vitamin D supplements should be co-prescribed in patients who are on corticosteroids,
to try to compensate for their inhibitory effect on intestinal calcium absorption.
3-enteral nutrition with either an elemental (constituent amino acids) or polymeric (liquid protein)
diet may induce remission.

4-Insevere ileal or panenteric disease, induction therapy with an anti-TNF agent (infliximab and
adalimumab) is appropriate, unless there is abscess.
- combination therapy with an anti-TNFantibody and a thiopurine is the most effective strategy
for inducing and maintaining remission in luminalCrohn’s patients. This strategy is more effective
than anti-TNF monotherapy,
B-Maintenance therapy.
-Immunosuppressive treatment with thiopurines (azathioprine and mercaptopurine) Or
methotrexate…note : methotrexate is teratogenic.
-Combination therapy with an immunosuppressant and an anti-TNF antibody is the most effective
strategy but costs are high and there is an increased risk of serious adverse effects.
- stop smoking.
C-Fistulae and perianal disease.
-Fistulae often associated with sepsis.treat:Sx
-Corticosteroids are ineffective.
- For simple perianal disease, metronidazole and/or ciprofloxacin are first-line therapies.
-Thiopurines can be used in chronic disease but do not usually result in fistula healing.
-Infliximab and adalimumab can heal fistulae and perianal disease in many patients and are indicated
when the measures described above have been ineffective.
Surgical treatment
♠
Ulcerative colitis:
Up to 60% of patients with extensive ulcerative colitis eventually require surgery. Indication of Sx:
1-Impaired quality of life
• Loss of occupation or education
• Disruption of family life
2-Failure of medical therapy
• Dependence on oral corticosteroids
• Complications of drug therapy
3-Fulminant colitis
4-Disease complications unresponsive to medical therapy • Arthritis • Pyoderma gangrenosum
5-Colon cancer or severe dysplasia
♠
Crohn’s disease:
-The indications for surgery are similar to those for ulcerative colitis.
-Operations are often necessary to deal with fistulae, abscesses and perianal disease, and relieve
small or large bowel obstruction.
- Incontrast to ulcerative colitis, surgery is not curative and disease recurrence is the rule.
-The only method that has consistently been shown to reduce post-operative recurrence is smoking
cessation.