Blood vesselspathology
Master And Board LecturesLecturer Dr. ZAHRAA MARWAN
LEC. 2Arterial Dissection
By comparison, a false aneurysm (pseudo- aneurysm) results when a wall defect leads to the formation of an extravascular hematoma that communicates with the intravascular space (“pulsating hematoma”). While, in arterial dissections, pressurized blood gains entry to the arterial wall through a surface defect and then pushes apart the underlying layers.Aortic Dissection
Affects 2 groups of patients:- Hypertensive men of 40-60yrs.
- Young people with systemic or localized abnormality of connective tissueMorphology
. Transverse or oblique intimal tear within 10cm of aortic valve 1-5cm in length
. Dissection extends proximally and distally
. The hematoma is between the middle and outer thirds of the wall
* Histology: cystic medial degeneration
Aortic dissection

Aortic dissection
VASCULITIS
Vasculitis : vessel wall inflammation.Pleural: VASCULITIDES
Clinical features:Are variable & largely depend on the vascular bed affected (e.g., CNS vs. heart vs. small bowel).
Constitutional symptoms such as fever, myalgia & arthralgia.
VASCULITIS
* Causes & pathogenesis
I- Direct microbiological infection:
eg. Pseudomonas , Aspergillus & Mucor
II - Immune-mediated:
• Immune complex deposition• Antineutrophil cytoplasmic antibodies
• Antiendothelial cell antibodies
• Autoreactive T cells
III-Others (Physical and chemical injury, including radiation, mechanical trauma, and toxins)
Immune Complex-Associated Vasculitis
• Autoantibody production and formation of immune complexes that deposit in vessels, eg.• SLE
• Drug hypersensitivity vasculitis ( penicillin)
• Vasculitis secondary to infections ( hepatitis B).
Anti-Neutrophil Cytoplasmic Antibodies
Circulating autoantibodies that react with neutrophil cytoplasmic antigens ( mainly enzymes), also called pauci immune.ANCAs are very useful diagnostic markers; their titers generally mirror clinical severity, and a rise in titers after periods of quiescence is predictive of disease recurrence.
Types:
• Antiproteinase-3 (PR3-ANCA), previously called c-ANCA. Eg. Wegener granulomatosis
• Anti-myeloperoxidase (MPO-ANCA), previously called p-ANCA. Eg. microscopic polyangiitis and Churg-Strauss syndrome.
Anti-Endothelial Cell Antibodies.
Antibodies to endothelial cells, eg. Kawasaki diseaseClassification
Some 20 primary forms of vasculitides are recognizedThe classification schemes attempt to group them according to:
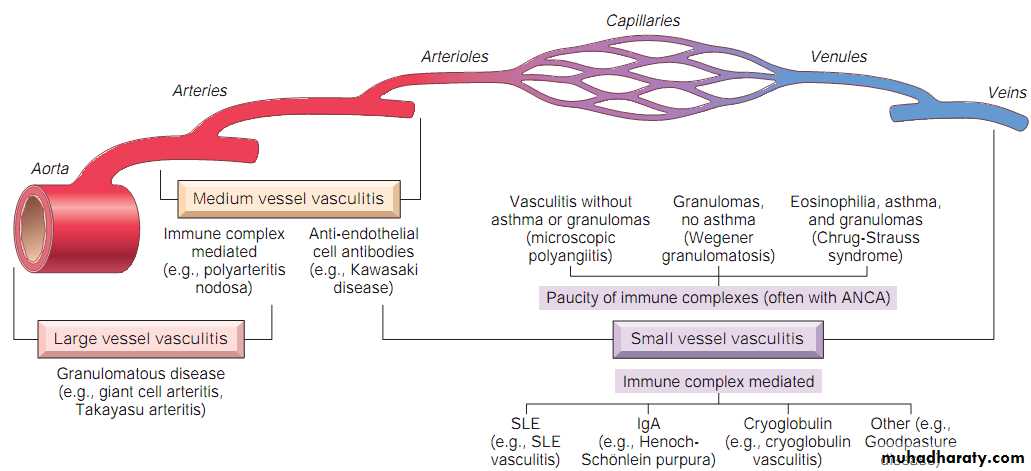
• Vessel diameter ( size),
• Role of immune complexes,
• Presence of specific autoantibodies,
• Histology & Granuloma formation,
• Organ specificity,
• Even population demographics
Vasculitis, types-sites relation
Giant Cell Arteritis
.The most common form of Vasculitis in elderly (older than 50yrs).
. Chronic, typically granulomatous inflammation of large to small size arteries.Most common arteries involved are:
(temporal, vertebral, ophthalmic, aorta ”giant cell aortitis”)
Pathogenesis:
- T cell mediated immune response to an as-yet uncharacterized vessel wall antigen.- Pro-inflammatory cytokines (especially TNF) and anti-endothelial cell antibodies also contribute.
* Clinical features
Temporal artery: headache & pain in artery courseOphthalmic artery: diplopia , loss of vision
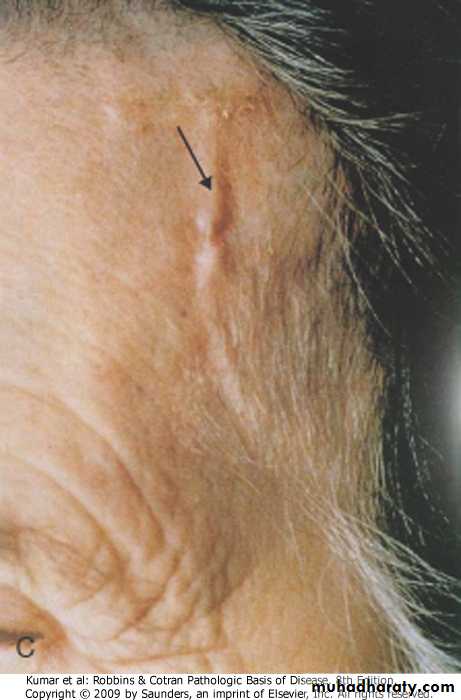
Temporal artery, giant cell arteritis
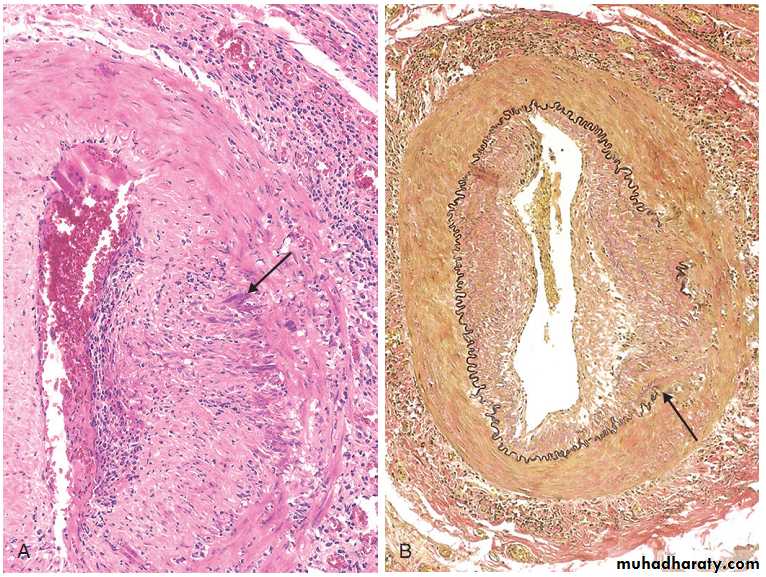
Morphology:segemental involvement of vessel
Giant cells arteritis:
Granulomatous inflammation within the inner media with multinucleate giant cellsFragmentation of the internal elastic laminas
Polyarteritis nodosa
Systemic vasculitis of small or medium-sized muscular arteriesTypically involves the renal and visceral vessels
Spares the pulmonary circulation.
There is no association with ANCAs
1/3 of cases have chronic hepatitis B infection
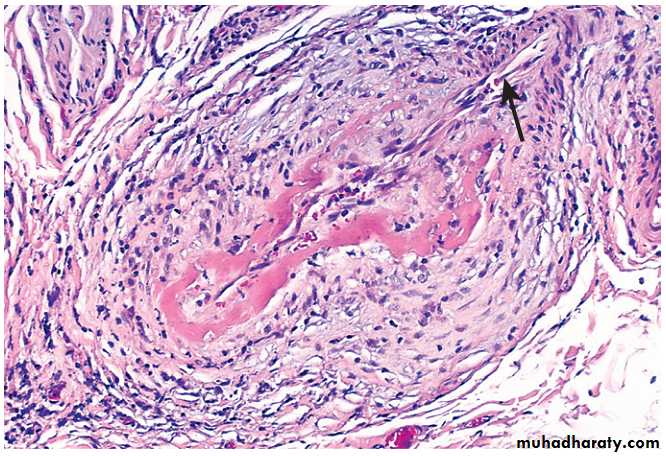
PAN: segmental transmural fibrinoid necrosis of small artery,
Kawasaki disease
acute, febrile, usually self-limited illness of infancy and childhood (80% < 4 years)
Mainly involve large to medium-sized vessels.
Coronary arteritis cause aneurysms that rupture or thrombose, resulting in myocardial infarction ( ! in children).
Also called mucocutaneous lymph node syndrome
Muco: conjunctival and oral erythema and blistering
Cutaneous: desquamative rash
LN: cervical lymph node enlargement
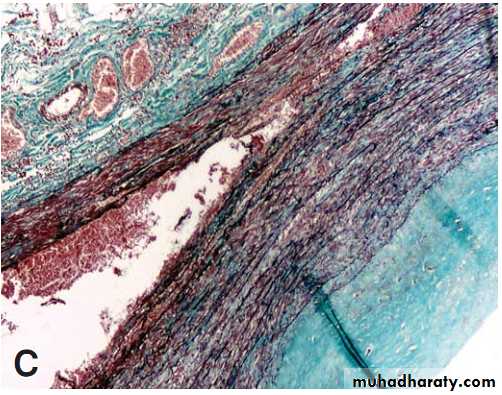
Thrombo Angiitis Obliterans (Buerger Disease)
Focal acute and chronic inflammation of medium-sized and small arteries ( especially tibial and radial arteries)Associated with thrombosis & frequently results in severe vascular insufficiency and gangrene of the extremities
Occasionally, secondary extension into adjacent veins and nerves
usually < 35 yrs.
Occurs almost exclusively in heavy tobacco smokers :
-direct toxicity
-hypersensitivity
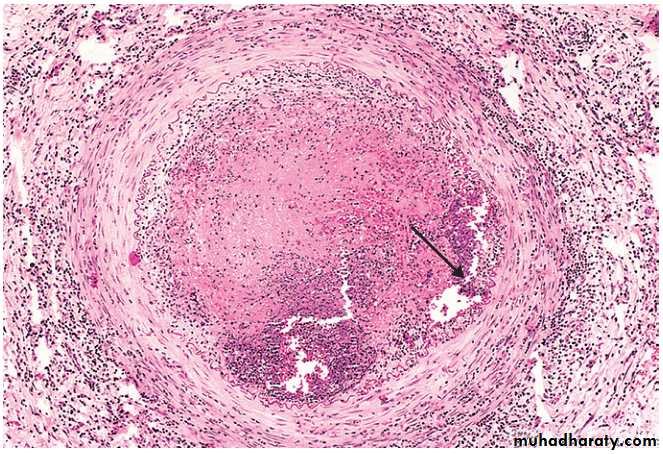
Thromboangiitis obliterans (Buerger disease). The lumen is occluded by thrombus containing abscesses (arrow) and the vessel wall is infiltrated with leukocytes.
Raynaud Phenomenon
Exaggerated vasoconstriction of arteries and arterioles in the extremities, particularly: fingers and toes, also nose, earlobes, or lips.Digits show “red - white - blue” color changes from most proximal to most distal, reflecting proximal vasodilation, central vasoconstriction, and more distal cyanosis, respectively.

Raynaud phenomenon
• Primary Raynaud PhenomenonCaused by exaggerated central and local vasomotor responses to cold or emotion
Affects 3% to 5% of population
Symmetrically affect the extremities
the severity and extent of involvement typically remains static over time.
• 2 . Secondary Raynaud Phenomenon .arterial insufficiency of the extremities caused by: -SLE -systemic sclerosis -atherosclerosis -Buerger disease
Asymmetric involvement of the extremities
Progressively worsens in extent and severity over time.
Varicose Veins
Abnormally dilated, tortuous veins, often
scarred with thrombosis, secondary to:
-prolonged high intraluminal pressure
-loss of vessel wall support
Mostly involve superficial veins of legs, causing leg edema, the most disabling sequelae include persistent edema in the extremity and secondary ischemic skin changes, including stasis dermatitis and ulcerations. The latter can become chronic varicose ulcers as a consequence of poor wound healing and superimposed infections.
Varicose Veins
People at risk:-long period of standing
-older than 50 years
-obese
-women with multiple pregnancies
-familial tendency, (weakness of wall)
Varicose veins

Varicose vein of legs

Apart from legs, varices occur also at :
-The lower end of esophagus -Ano-rectum, (hemorrhoids) -Scrotum, (varicocele)Vascular Tumors
Vascular neoplasms arise either from:Endothelium (e.g., hemangioma, lymphangioma, angiosarcoma)
Cells that support or surround blood vessels (e.g., glomus tumor).
In general, benign and malignant vascular neoplasms are distinguished by the following features:
Benign tumors usually are composed of vascular channels filled with blood cells or lymph that are lined by a monolayer of normal appearing ECs.
Malignant tumors are more cellular, show cytologic atypia, are proliferative, and usually do not form well-organized vessels.
Classification of Vascular Tumors and Tumor-like Conditions
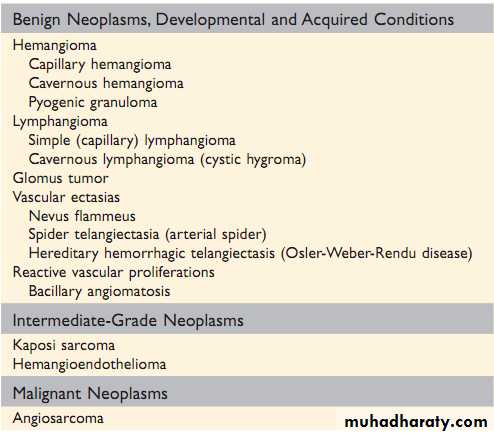
Hemangiomas
Very common tumors composed of blood-filled vessels.Constitute 7% of all benign tumors of infancy and childhood;
Capillary hemangiomas
Most common type
Occur in the skin, subcutaneous tissues, and mucous membranes of the oral cavities and lips, as well as in the liver, spleen, and kidneys
Histologically: thin-walled capillaries with scant stroma
Cavernous hemangiomas
Composed of large, dilated vascular channels.
Frequently involve deep structures
Not spontaneously regress.
Pyogenic granulomas
are capillary hemangiomas that manifest as rapidly growing red pedunculated lesions on the skin, gingival, or oral mucosa.
Microscopically they resemble exuberant granulation tissue.
They bleed easily and often ulcerate.
Roughly one fourth of the lesions develop after trauma, reaching a size of 1 to 2 cm within a few weeks.
Curettage and cautery usually are curative.
Hemangioma
(A) Hemangioma of the tongue. (B) Histologic appearance in juvenile capillary hemangioma. (C) Histologic appearance in cavernous hemangioma. (D) Pyogenic granuloma of the lip.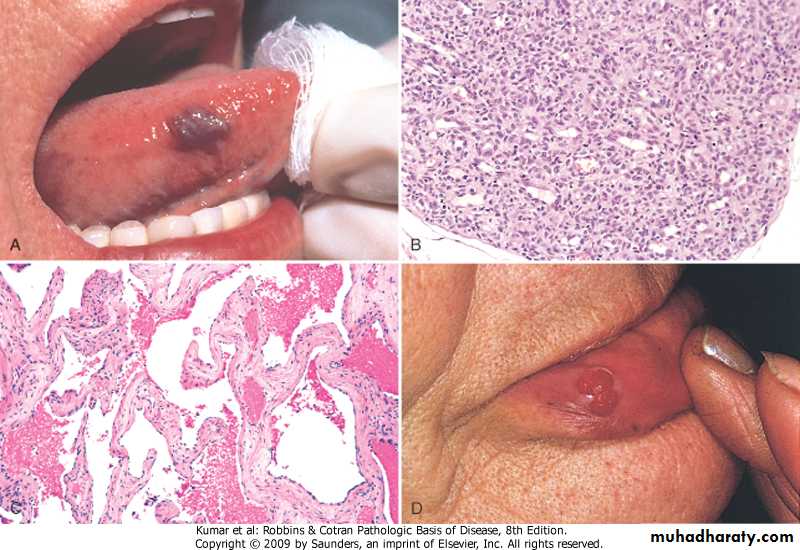
Lymphangiomas
Benign lymphatic counterpart of hemangiomas.Simple (capillary) lymphangiomas
occur predominantly in the head, neck, and axillary subcutaneous tissues.
Histologically: networks of endothelium-lined spaces
Cavernous lymphangiomas (cystic hygromas)
Typically neck or axilla of children
Common in Turner syndrome.
Massively dilated lymphatic spaces lined by endothelial cells + lymphoid aggregates.
Kaposi Sarcoma
Vascular neoplasm caused by Kaposi sarcoma herpes virus (KSHV, also known as human herpes-virus-8, or HHV-8).
Four forms of KS:
Classic KS; Endemic African KS; Transplant-associated KS; AIDS-associated (epidemic) KS
Three stages: patch, plaque, nodule.
Histologically: proliferating spindle cells, slit like vessels, extravasated RBC
kaposi sarcoma

Kaposi Sarcoma
coalescent cutaneous red-purple macules and plaquesKaposi sarcoma
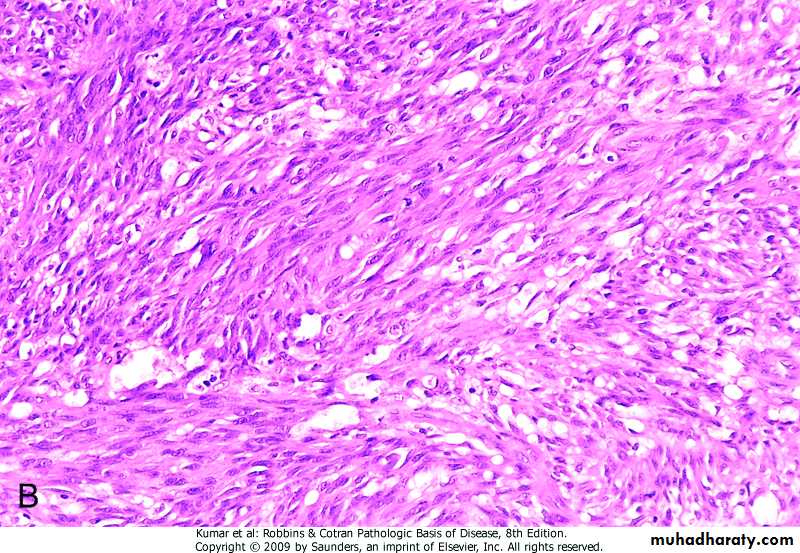
nodular stage, demonstrating sheets of plump, proliferating spindle cells and slit like vascular spaces.
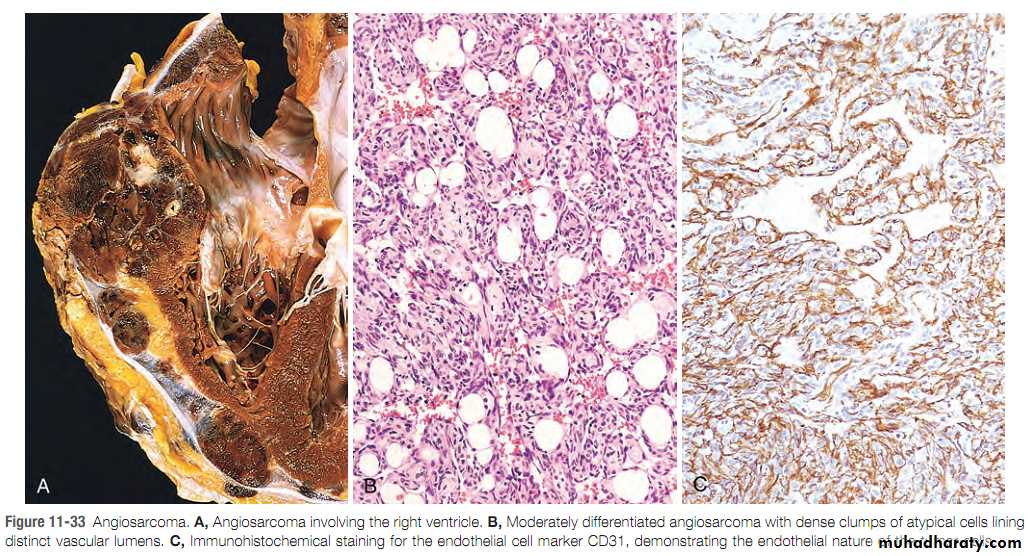
Angiosarcoma
Malignant endothelial neoplasm that primarily affects older adults.Most often involves skin, soft tissue, breast, and liver.
Heart, angiosarcoma, moderately differentiated, endothelial cell marker (CD31)