Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
1
Bone imaging
Aims of our lecture:
To know the different radiological techniques used in bone imaging, and what are
their advantages and disadvantages.
To know different bone pathologies.
To differentiate benign from malignant nature of a bony lesion.
See some examples of bony lesions
I) Radiological techniques used in bony imaging:
Plain X ray
Ultrasonography
CT scan
MRI
Radionuclide bone scanning
Plain X ray
•
Advantages:
•
Disadvantages:
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
2
The signs of bone disease on plain X ray
Decrease in bone density, which may be focal or generalized. Focal reduction in
density is usually referred to as a ‘lytic area’ or an area of ‘bone destruction’.
When generalized, decrease in bone density is best referred to as ‘osteopenia’
Increase in bone density (sclerosis), which may also be focal or generalized.
Periosteal reaction. The periosteum is not normally visible on a radiograph. The
term ‘periosteal reaction’ refers to excess bone produced by the periosteum,
which occurs in response to such conditions as neoplasm, inflammation or trauma.
Alteration in trabecular pattern is a complex response usually involving a
reduction in the number of trabeculae with an alteration in the remaining
trabeculae, e.g. in osteoporosis and Paget’s disease
Alteration in the shape of a bone is another complex response with many causes.
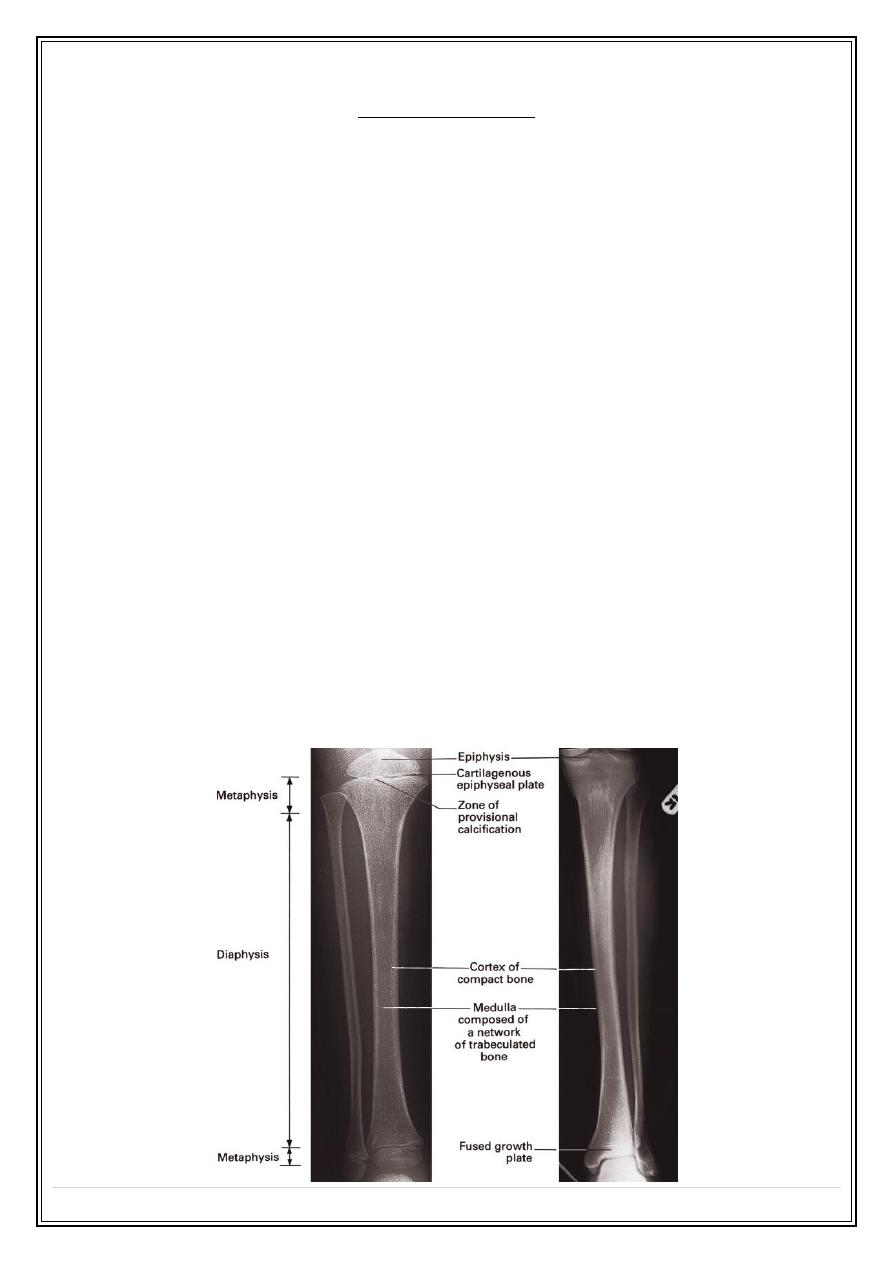
Alteration in bone age. The time of appearance of the various epiphyseal centers
and their time of fusion depends on the age of the child.
Generalized alteration of bone density:
Osteoporosis
Normal
Osteopetrosis
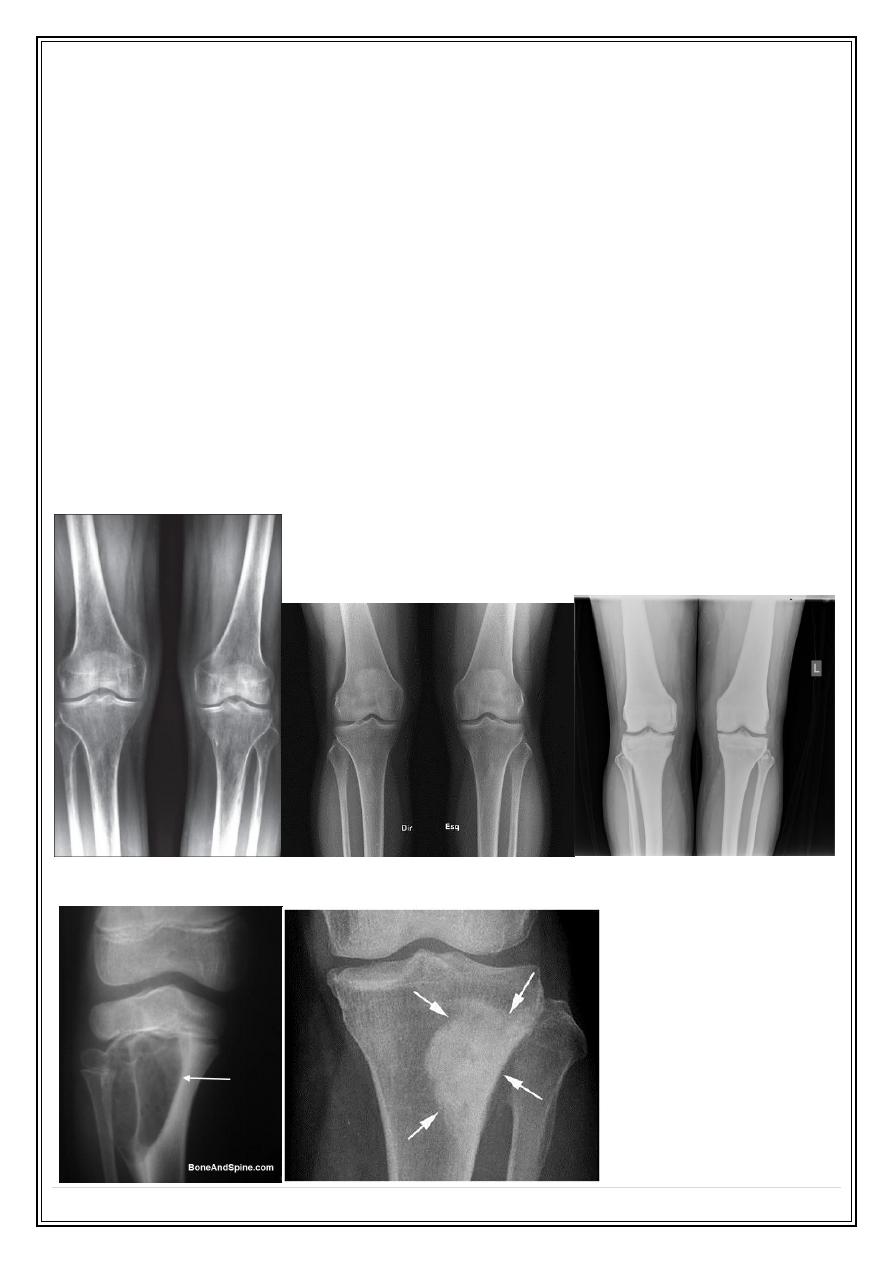
Focal alteration of bone density:
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
3
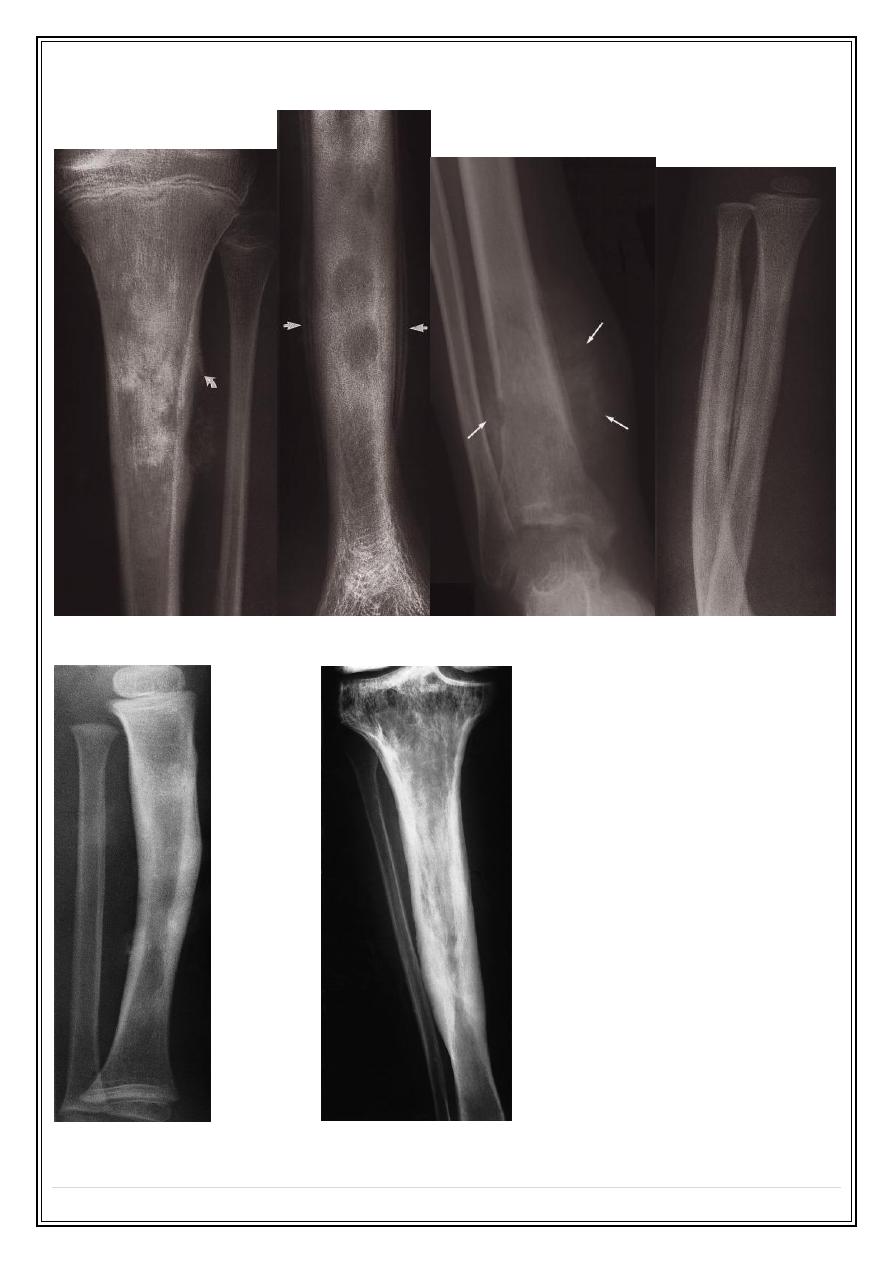
Periosteal reaction:
Codman’s triangle
Onion skin
Spiculated (sunray) Smooth lamellar
Cortical thickening
Alteration of trabecular pattern in Paget’s disease
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
4
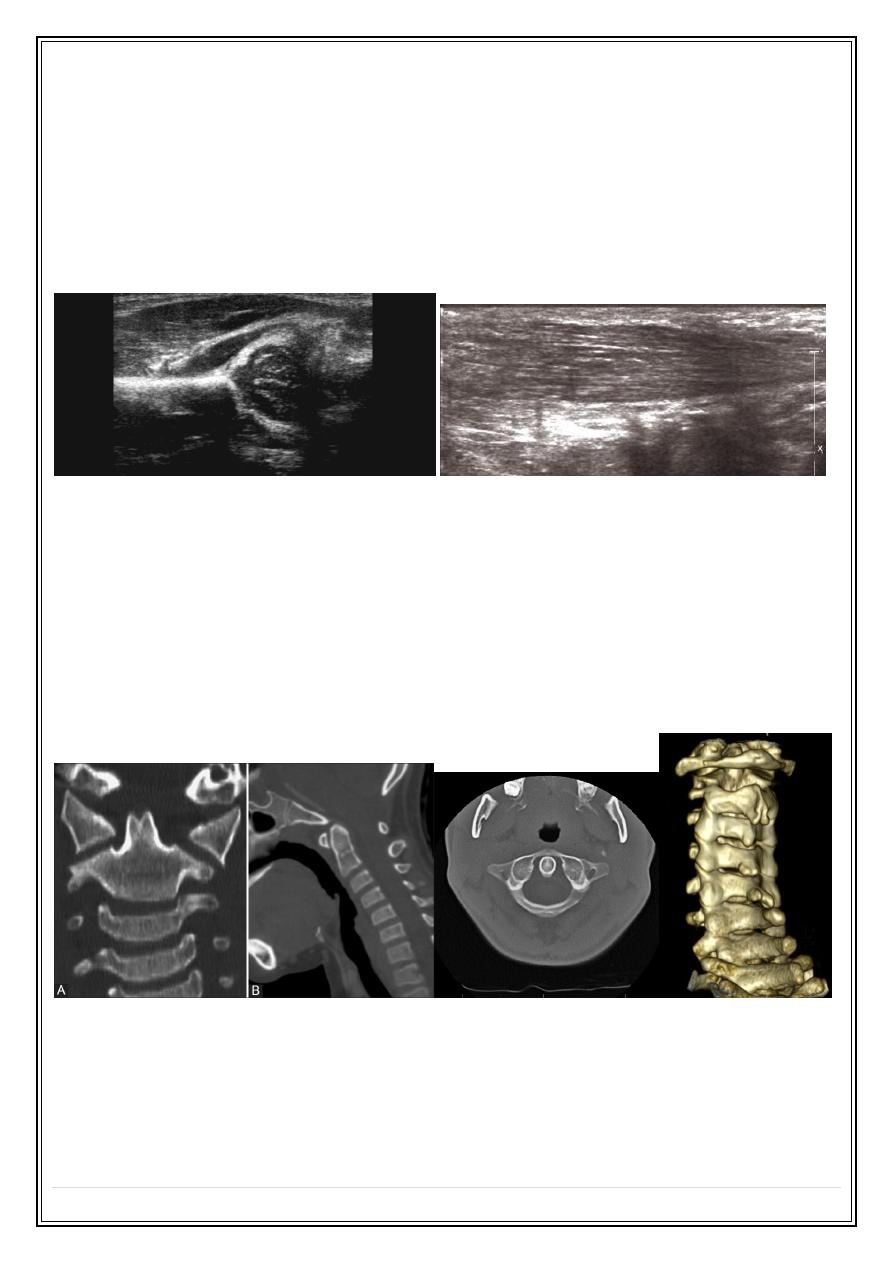
Ultrasonography:
Ultrasound cannot demonstrate bone pathology
Detecting tenosynovitis, tendon tears and rupture
Diagnosis of DDH in infants.
Diagnosis of osteomyelitis.
Soft tissue lesions or calcification
Computed tomography
Demonstrating abnormalities in the spine, pelvis and Hips. Three-dimensional
reconstructions can be made
Demonstrating the extent and characterization of bone lesion
As a guide for bone biopsy.
❖
Advantages:
❖
Disadvantages:
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
5
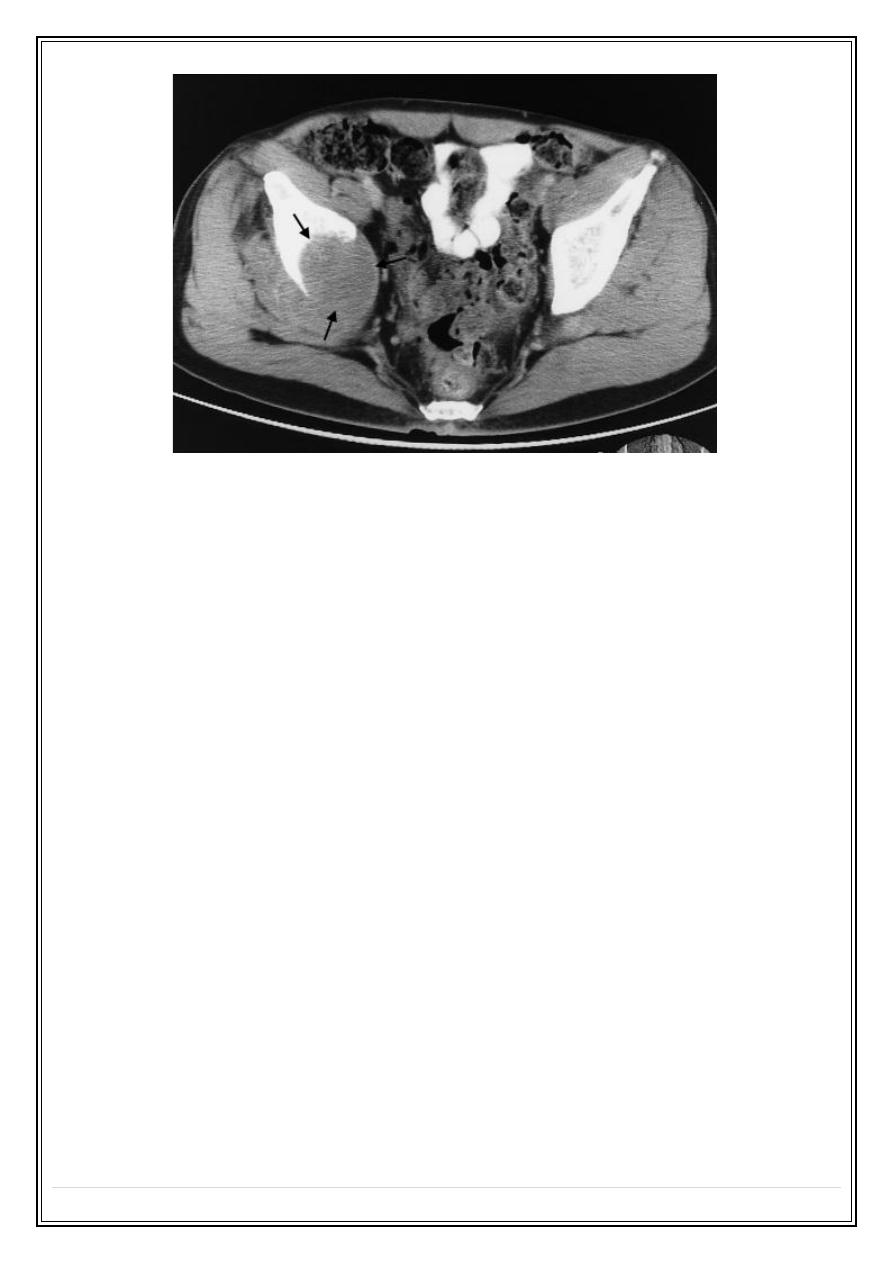
CT scan of pelvis showing a large mass (arrows) due to a metastasis destroying the
medial half of the right iliac bone with extension into the adjacent soft tissues
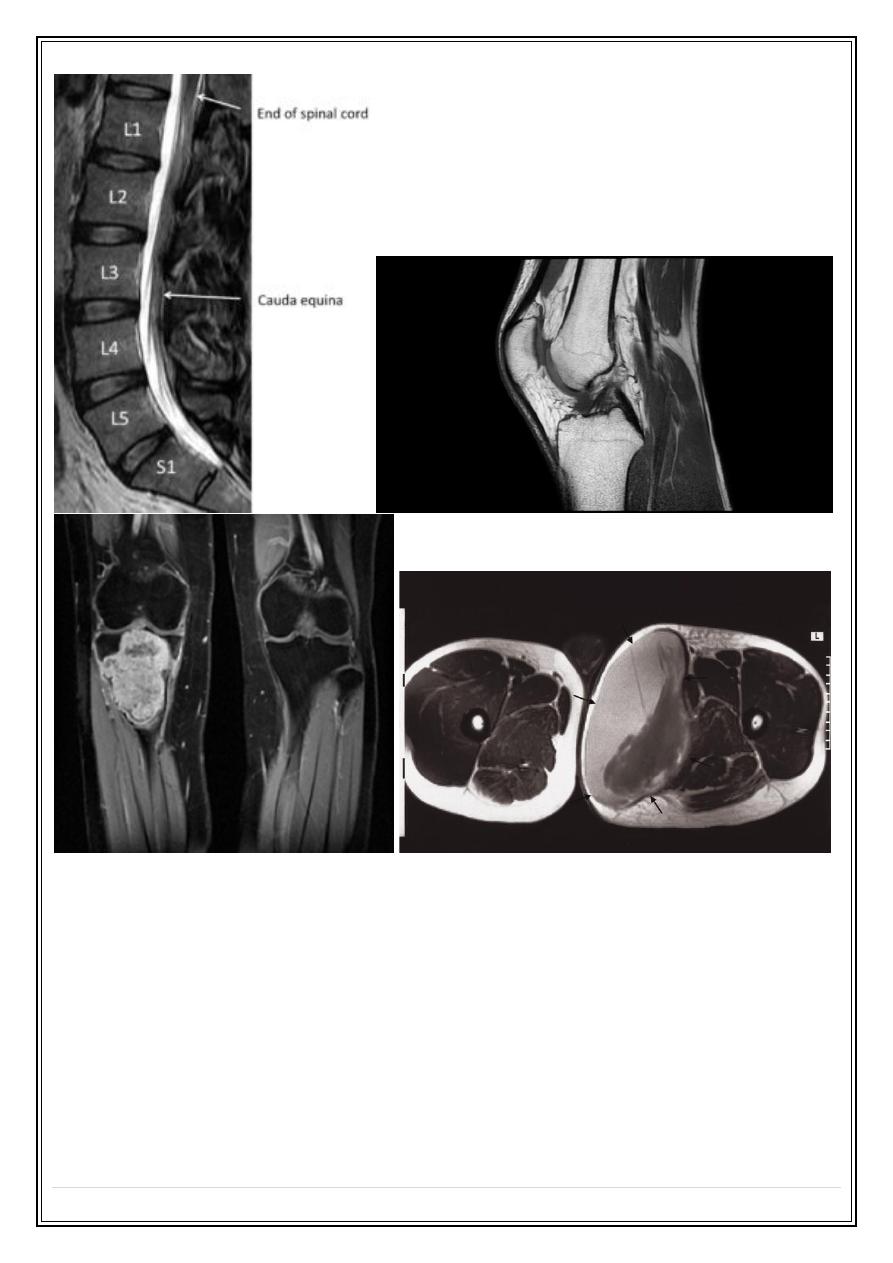
Magnetic resonance imaging
ž
Calcified tissues such as bone produce no signal with MRI, but MRI can
demonstrate the bone marrow directly
ž
The major indications for musculoskeletal MRI are:
To demonstrate disc herniation and spinal cord or nerve root compression
To diagnose bone metastases
To show the extent of primary bone tumors
To image soft tissue masses
To diagnose osteomyelitis and show any soft tissue abscess
To diagnose avascular necrosis and other joint pathologies and to image
both acute and chronic injury to joint cartilages, ligaments and other intra-
articular soft tissues
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
6
Radionuclide bone scanning
ž
Using Technetium-99m (99mTc)-labelled phosphate complexes given as an
intravenous injection. They are taken up selectively by the bones and excreted in
the urine.
ž
Indications for radionuclide bone scanning are:
Detection of metastases
Detection of osteomyelitis.
Determination of whether a lesion is solitary or multifocal
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
7
Investigation of a clinically suspected bone lesion despite a normal
radiograph osteomyelitis
Determination, in equivocal cases, of whether an abnormality seen on the
radiograph is significant or not
Investigation of painful joint prostheses.
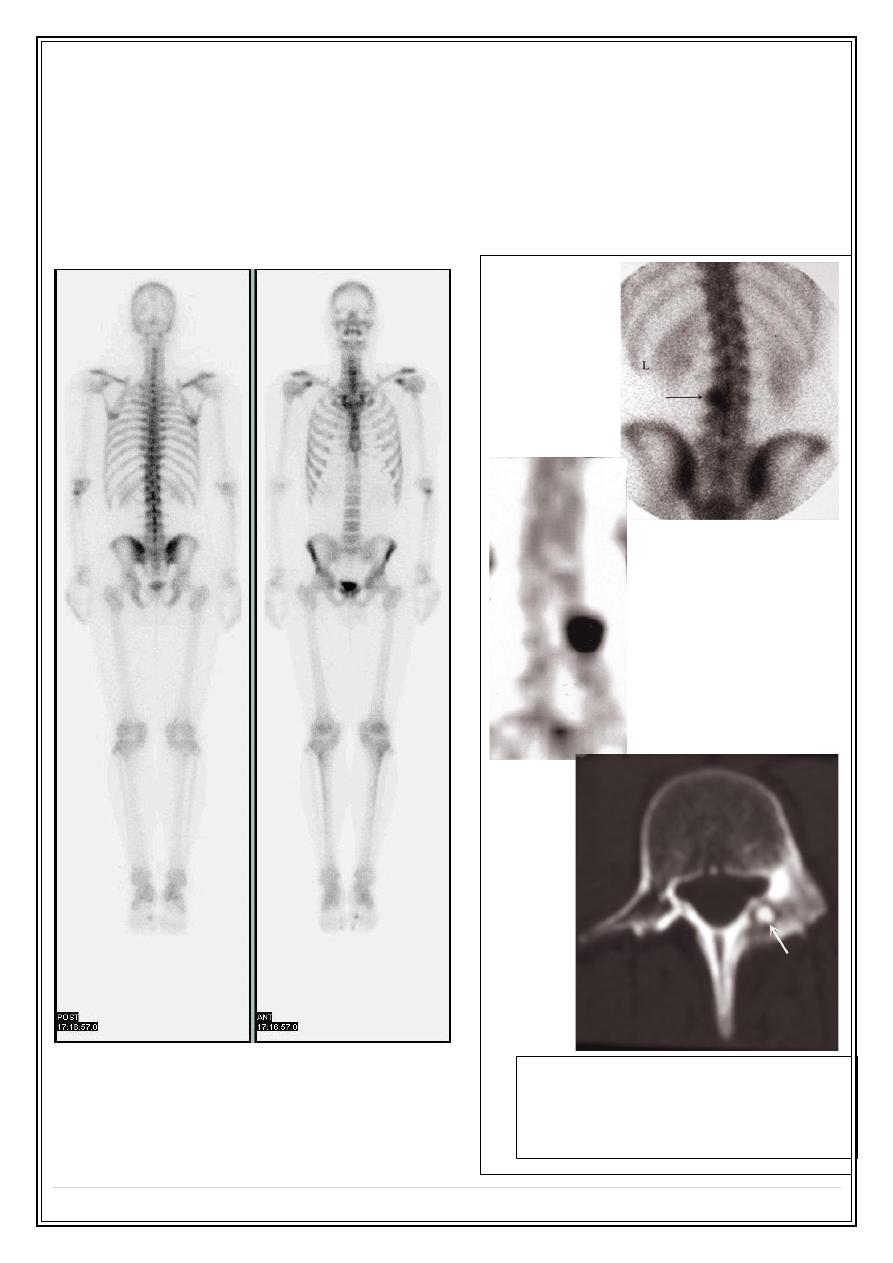
Radionuclide bone scanning:
Osteoid osteoma
Bone scan (posterior view) showing a focal
area of intense increased uptake in L3
CT demonstrates the tumor arising in the
pedicle.
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
8
II) Bone pathology:
Solitary lytic or sclerotic lesions
Multiple focal lesions, i.e. several discrete lytic or sclerotic lesions in one or more
bones
Generalized increase or decrease in bone density
Alteration of the trabecular pattern or change its shape
Solitary bone lesion
➢
Lytic
➢
Sclerotic
➢
Mixed
o
bone tumors (a) malignant (primary or secondary) (b) benign
o
osteomyelitis
o
bone cysts, fibrous dysplasia or other non-neoplastic defects of bone
o
conditions of uncertain nature such as Langerhans histiocytosis and osteoid
osteoma
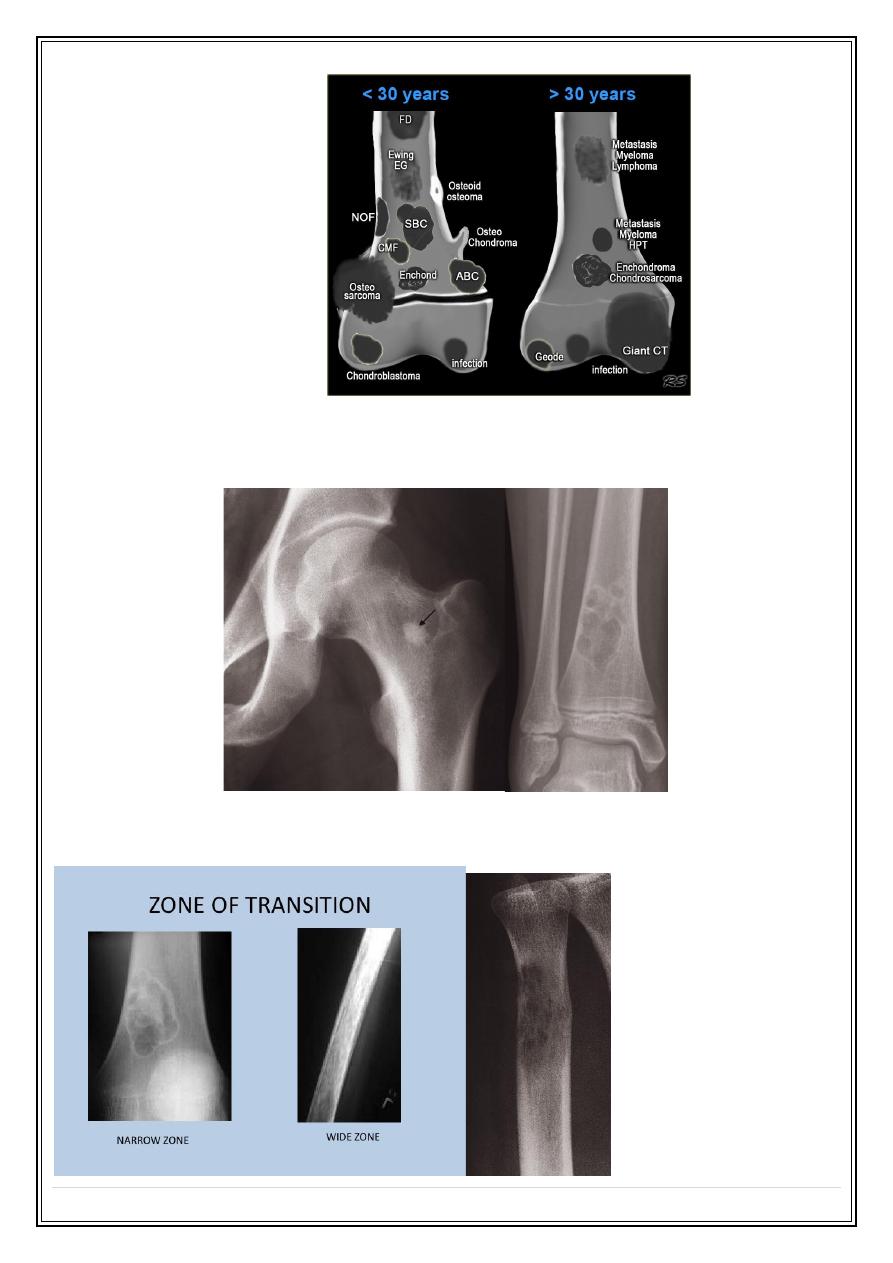
How to determine the nature of the lesion?
Age of the patient
Site of the lesion
Zone of transition
The adjacent cortex
Expansion
Periosteal reaction
Calcific densities within the lesion
Soft tissue swelling
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
9
1- Age of the patient
2- Site of the lesion
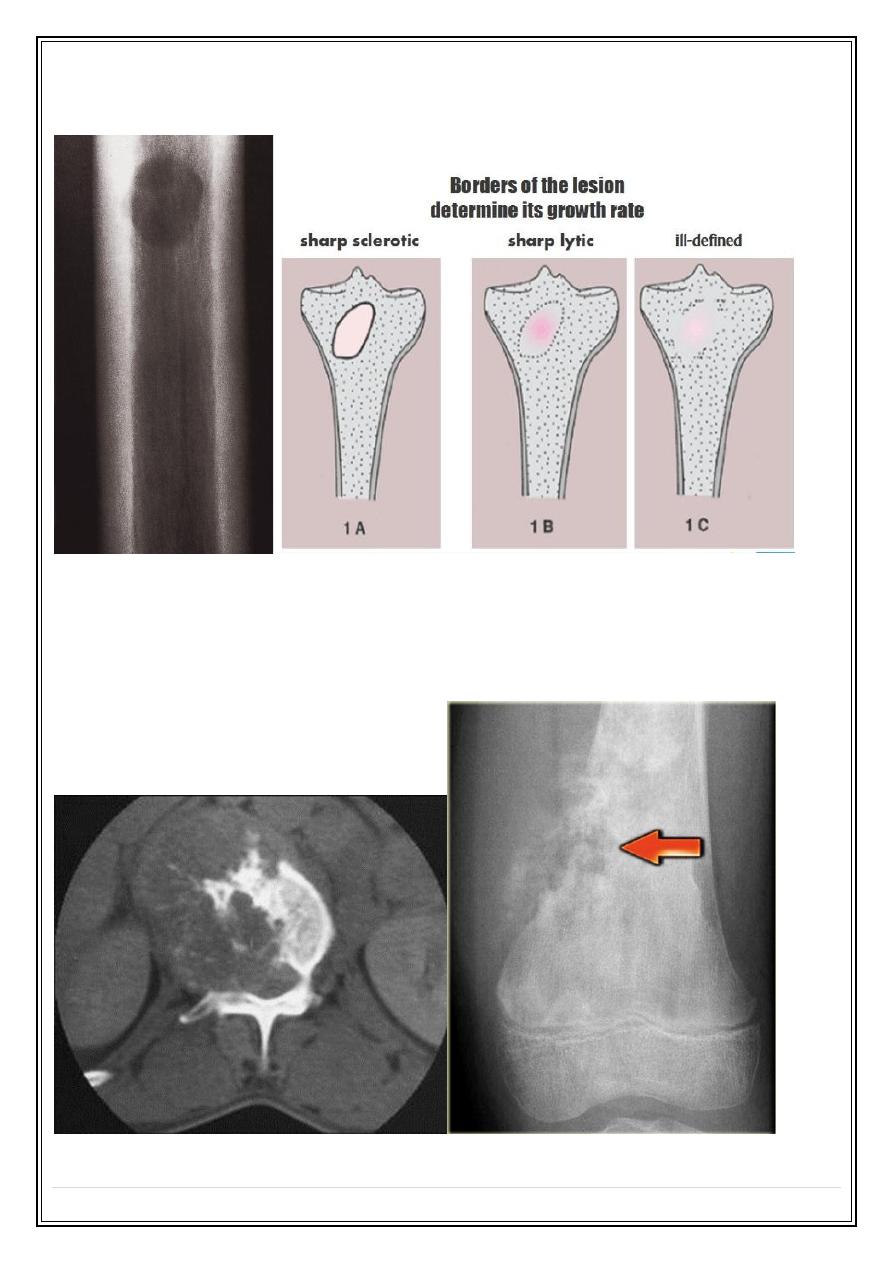
3- Zone of transition
❖
A lesion with a well-defined sclerotic edge is almost certainly benign, e.g. a fibrous
cortical defect or a bone island
❖
A lytic area with an ill-defined edge is likely to be aggressive. E.g. malignant
tumor and infection
Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
10
❖
A lytic area with no sclerotic rim, which may be a benign or malignant lesion. E.g.
metastases and myeloma
4- The adjacent cortex
Any destruction of the adjacent cortex indicates an aggressive lesion such as a
malignant tumor or osteomyelitis.

Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
11
5- Expansion
Bone expansion with an intact well-formed cortex usually indicates a slow-growing
lesion such as an enchondroma or fibrous dysplasia
6- Periosteal reaction
The causes of localized periosteal reactions adjacent to a lytic or sclerotic lesion are:
❖
Osteomyelitis
❖
Trauma
❖
Malignant bone
tumor,
particularly
Ewing’s sarcoma
and
osteosarcoma
❖
occasionally
metastasis,
particularly
neuroblastoma
❖
Langerhans histiocytosis.

Fifth Stage
Diagnostic Imaging
Dr. Firas A. – Lecture 1
P a g e
12
7- Calcific densities within the lesion
Calcification within an area of bone destruction occurs in specific conditions; for
example, patchy calcification of a popcorn type usually indicates a cartilage tumor,
whereas diffuse ill-defined calcification suggests osteoid formation and indicates an
osteosarcoma
8- Soft tissue swelling
The presence of a soft tissue mass suggests an aggressive lesion
To be continued ,,,