ABDOMINAL
EXAMINATION
3
rd
year – General Medicine
Dr.Muayad Al-Qaisy
Department of Medicine

GASTROINTESTINAL EXAMINATION
General examination
◦
General inspection
◦
Hands and arms
◦
Face, eyes and mouth
◦
Neck
Abdominal examination
Inspection
Palpation
Percussion
Auscultation
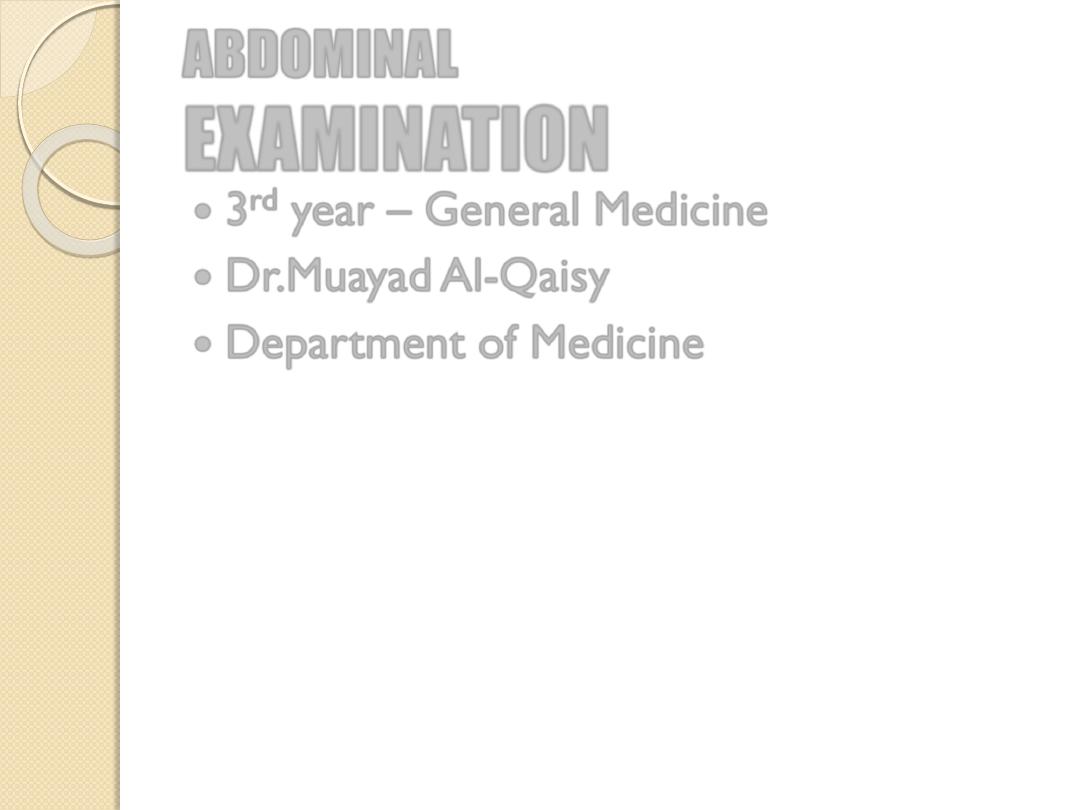
GENERAL INSPECTION
Nutritional state (wasting)
Pallor
Jaundice (liver disease)
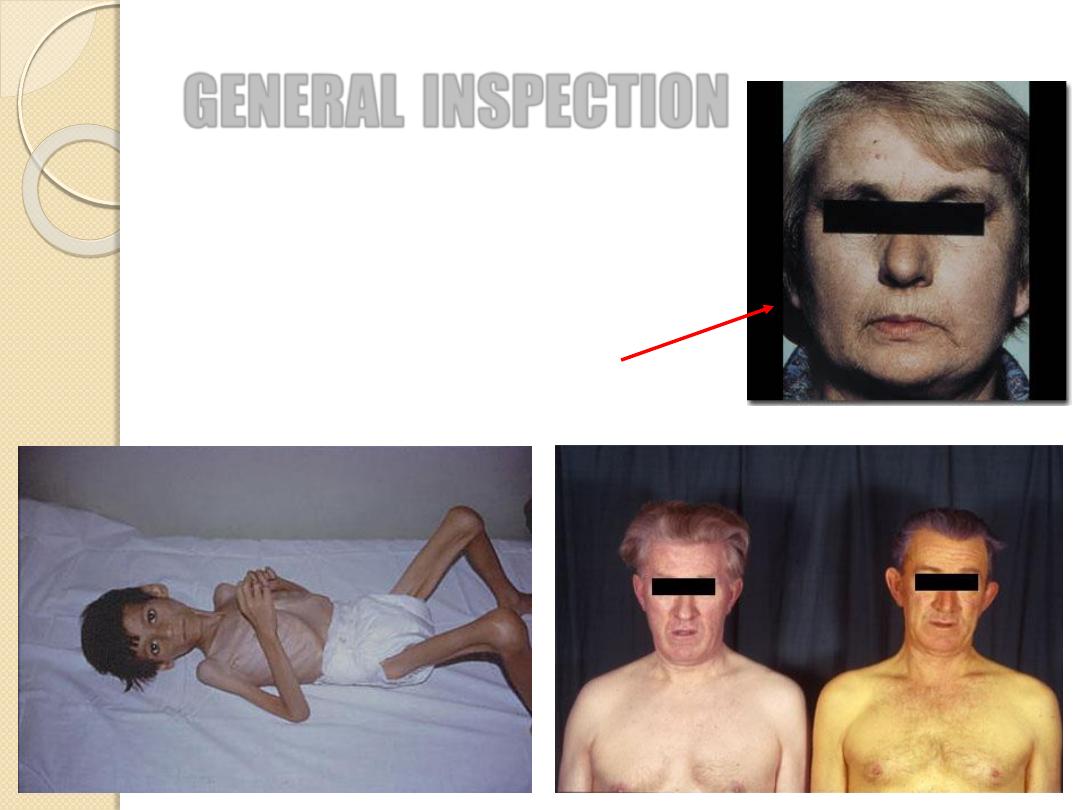
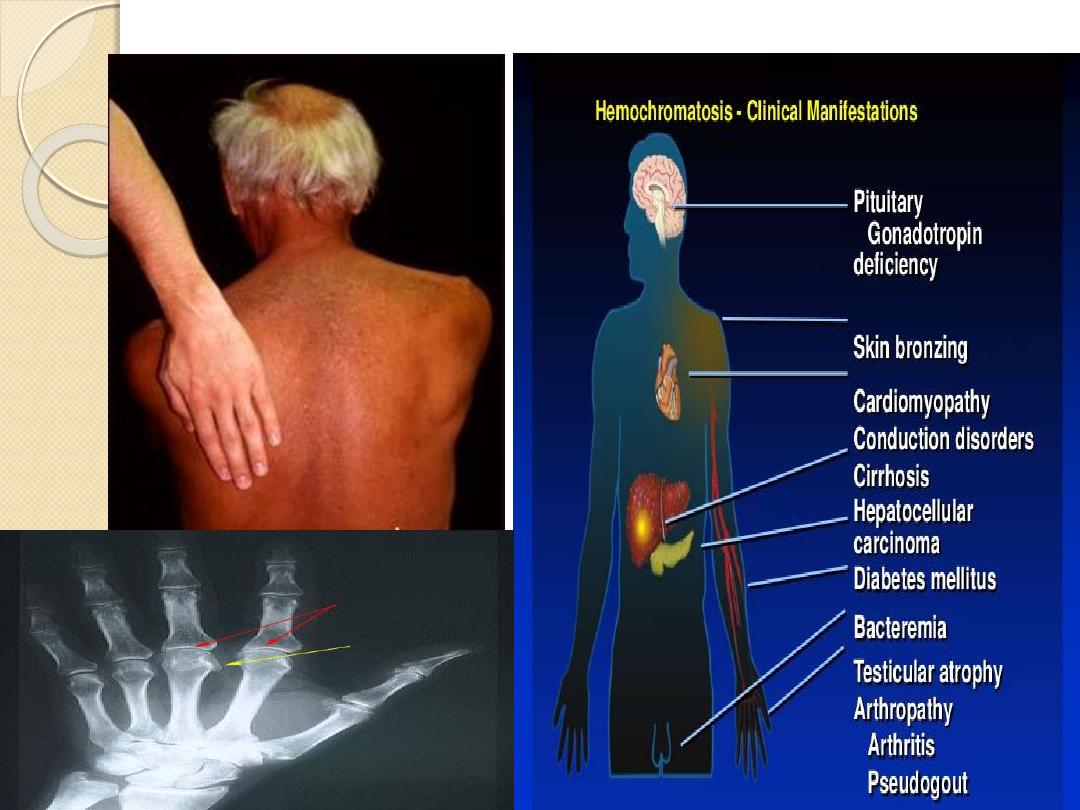
Pigmentation (hemochromatosis)
Mental state (encephalopathy)
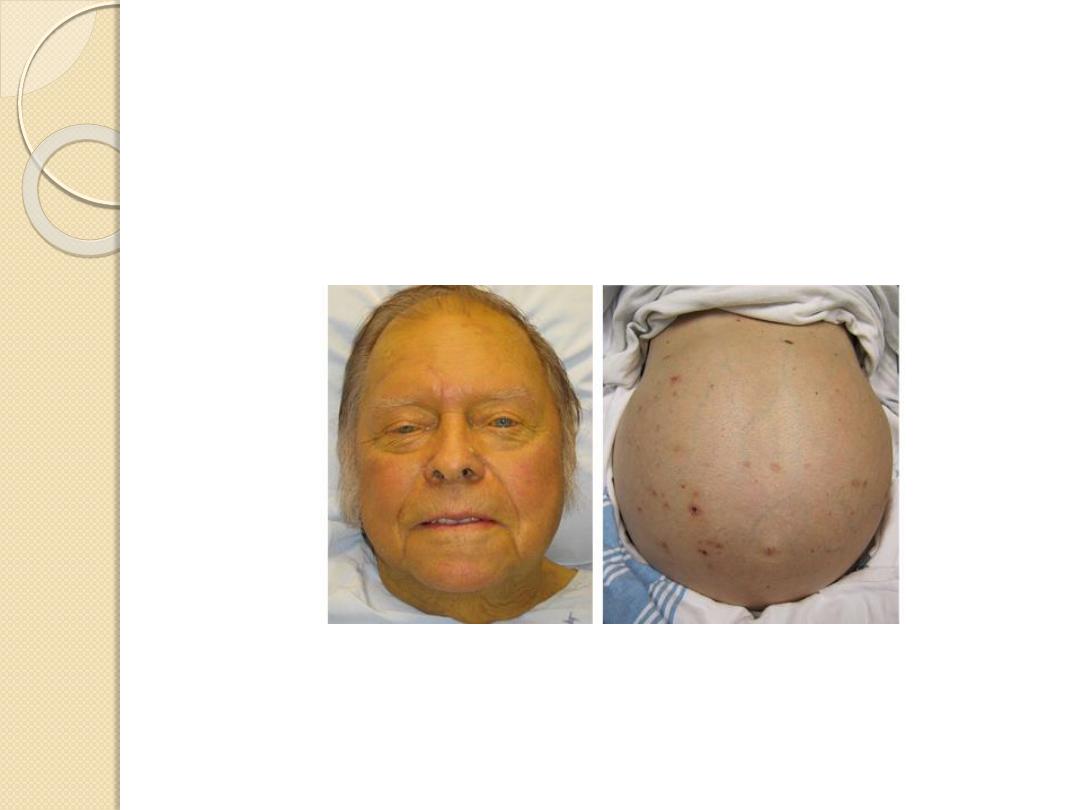
· The patient is a pigmented male over 30 years of age.
· Palmar erythema, spider naevi.
· Jaundice.
· Ascites, hepatomegaly (firm, regular).
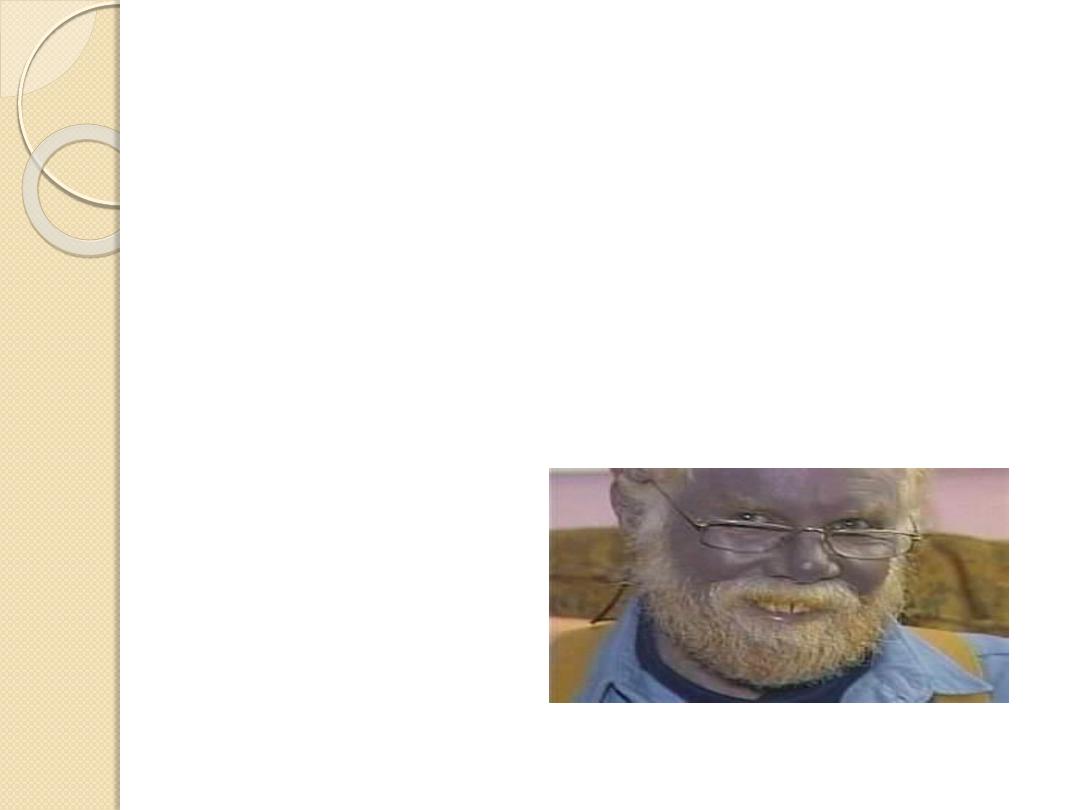
· Loss of secondary sexual hair.
Proceed as follows:
Tell the examiner that you would like to investigate as follows:
· Look for testicular atrophy (due to iron deposition affecting hypothalamo-pituitary function).
· Examine the heart for dilated cardiomyopathy, cardiac failure.
· Check urine for sugar, looking for evidence of diabetes mellitus (present in 80% of cases).Bronz Diabetes
Remember. Such patients develop cirrhosis and hepatocellular carcinoma.
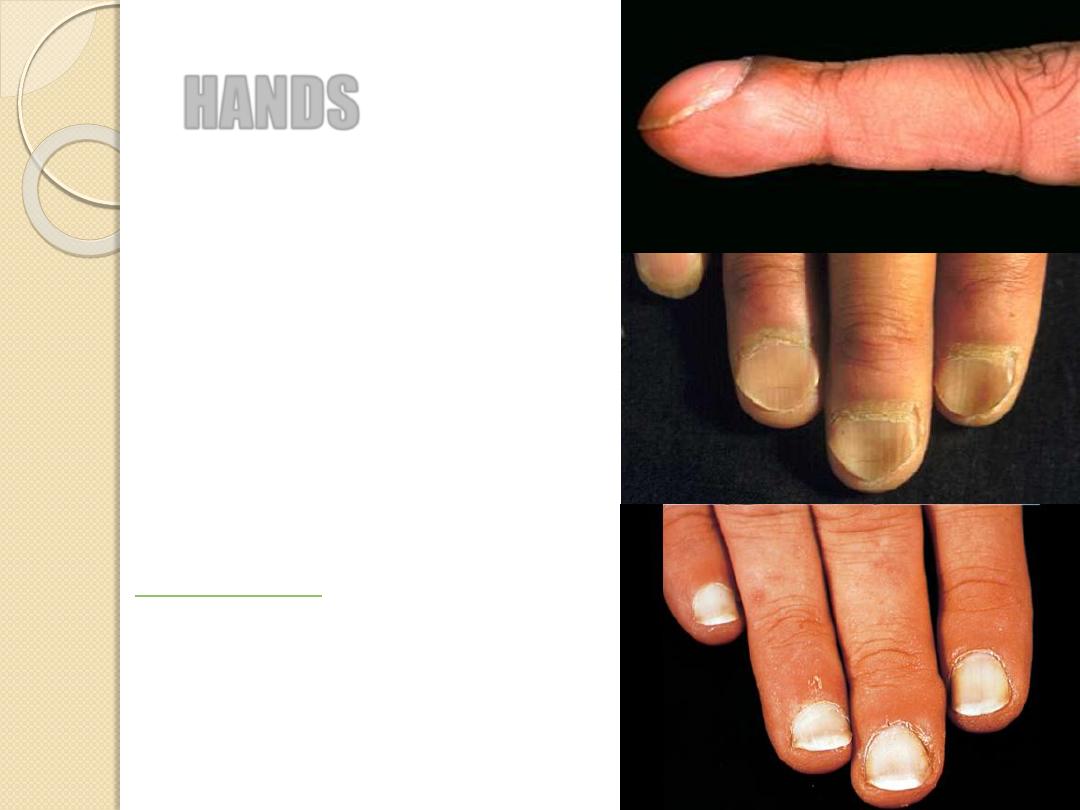
HANDS
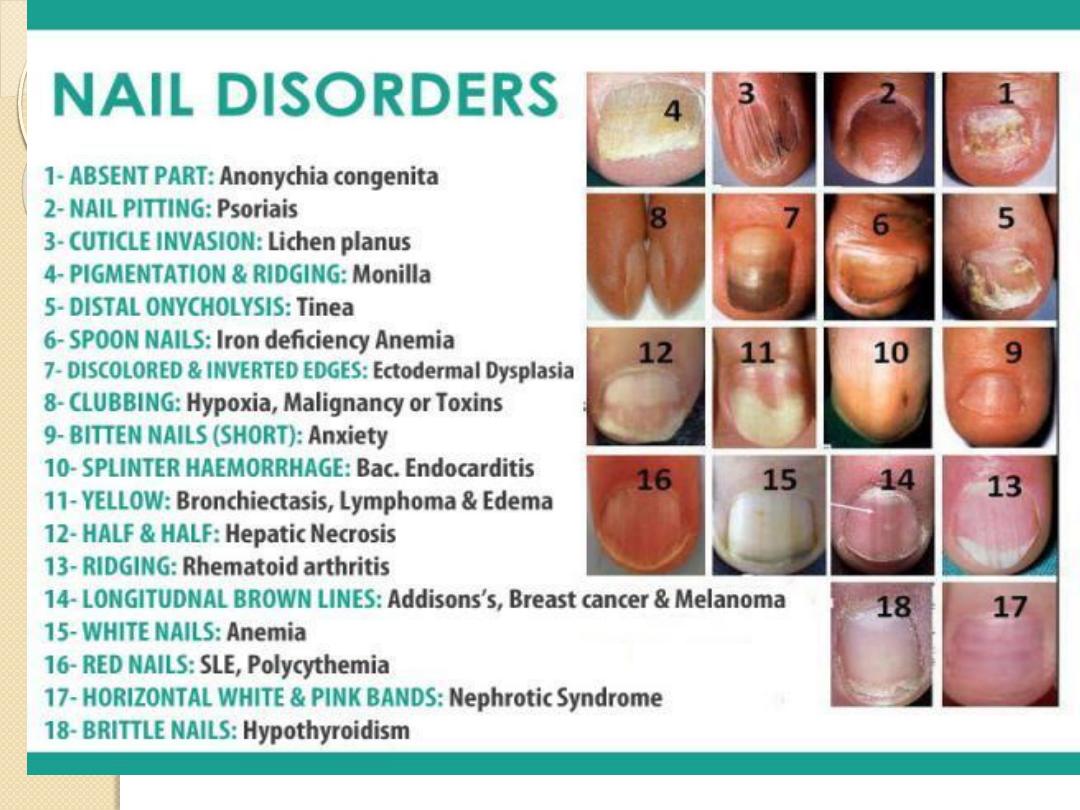
Nails
◦
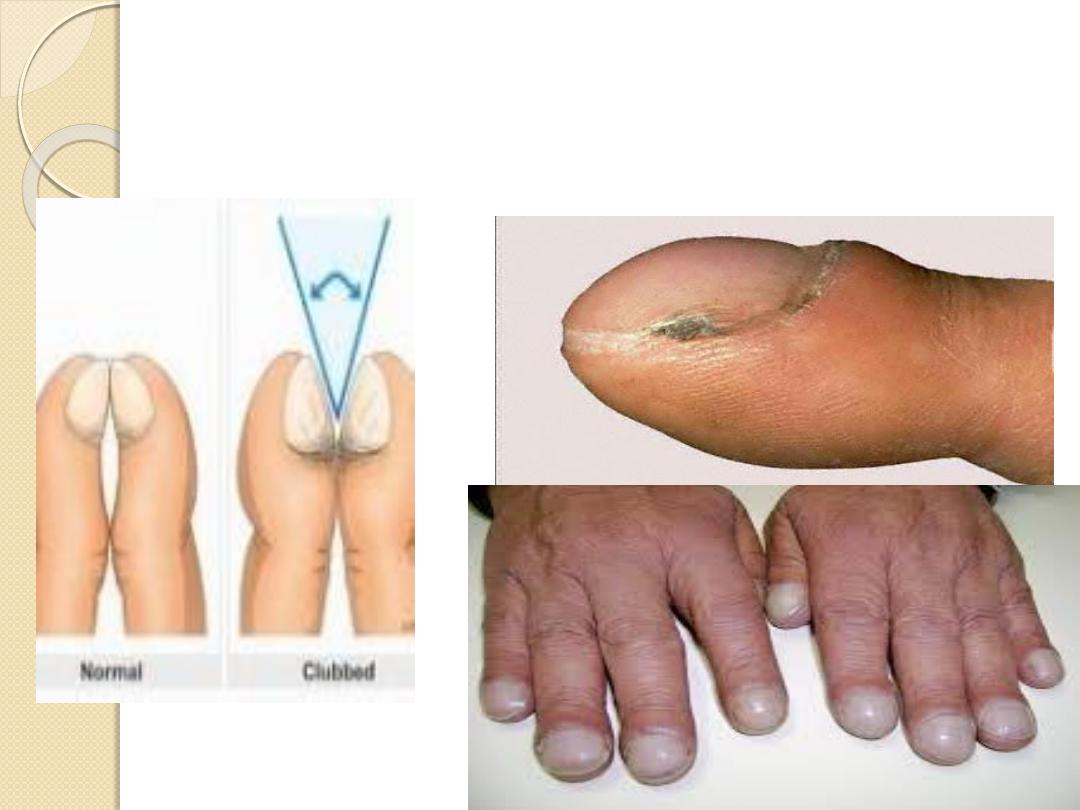
Clubbing
◦
Koilonychia
◦
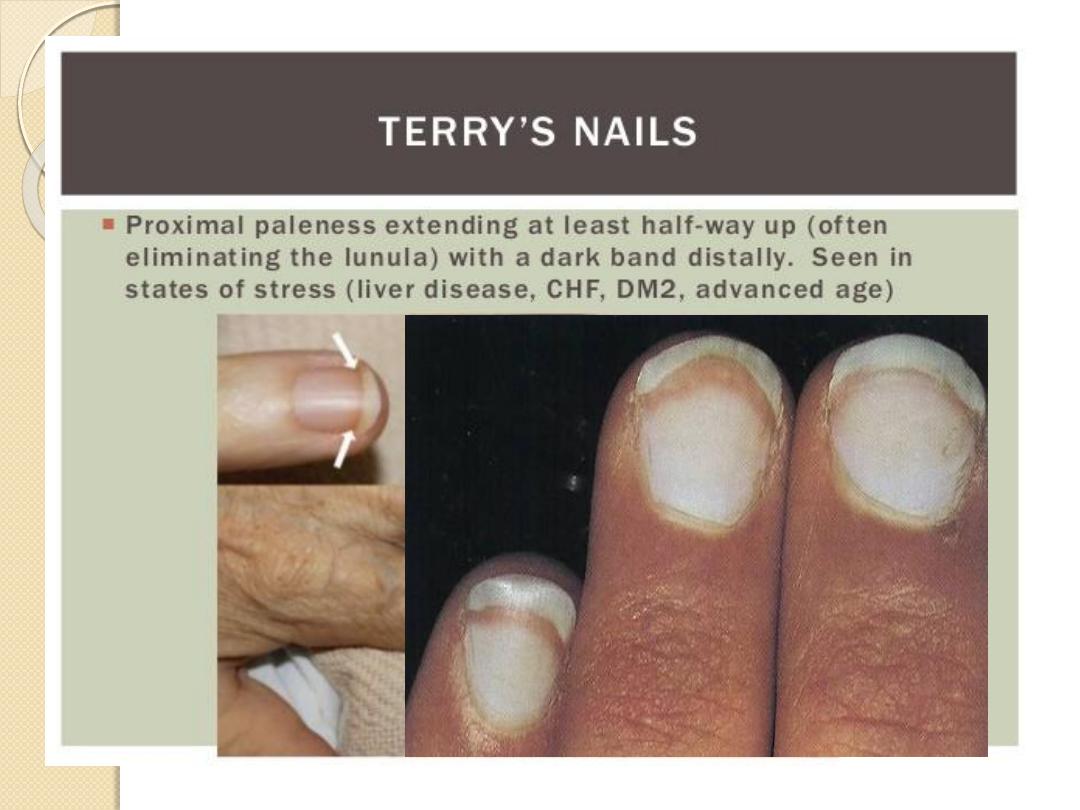
Leuconychia
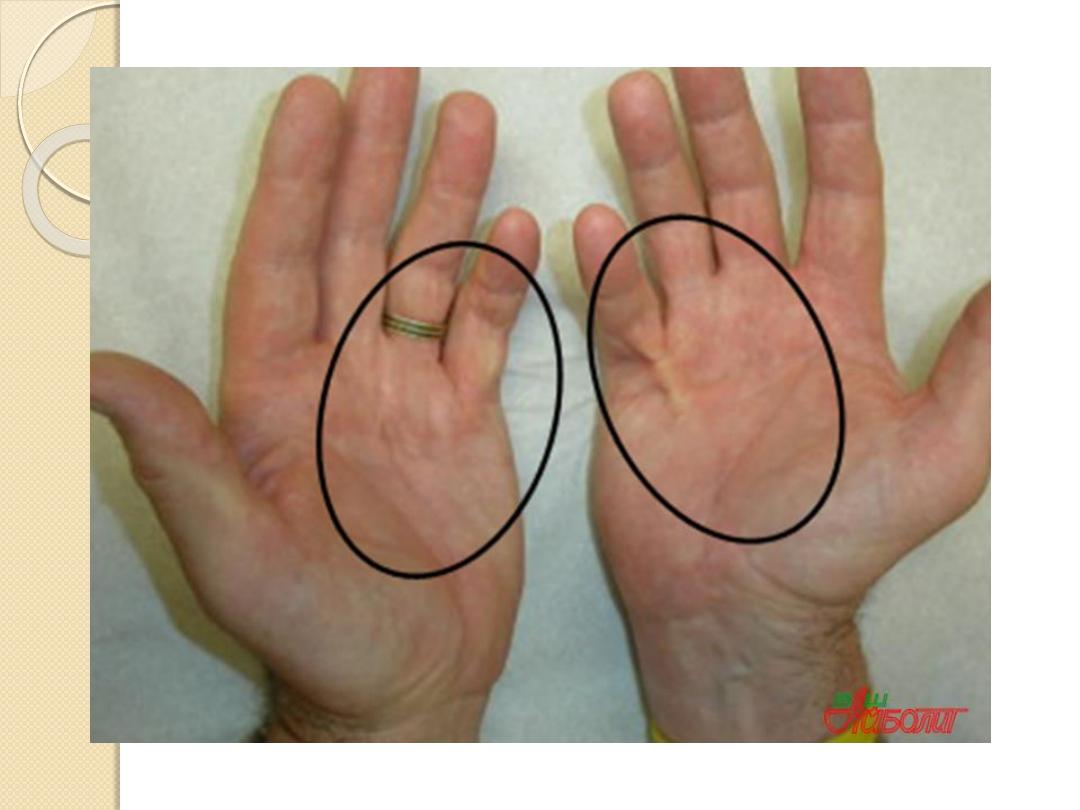
Palmar erythema
Dupuytren’s contractures
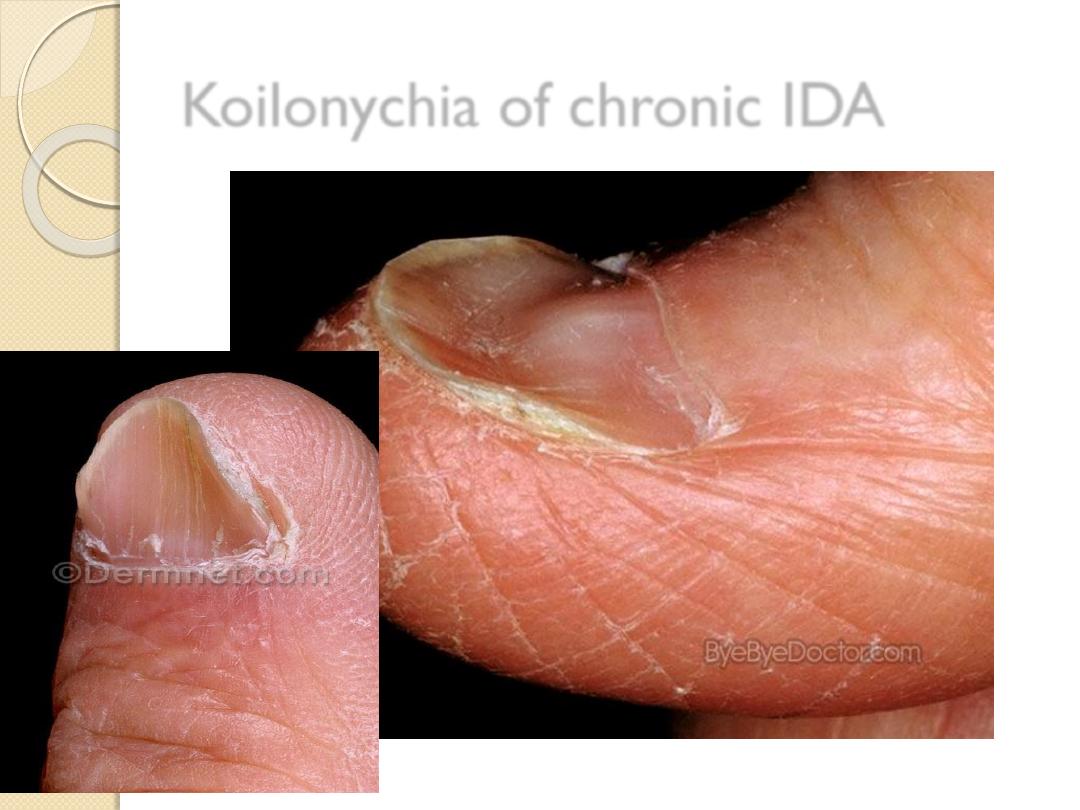
Koilonychia of chronic IDA
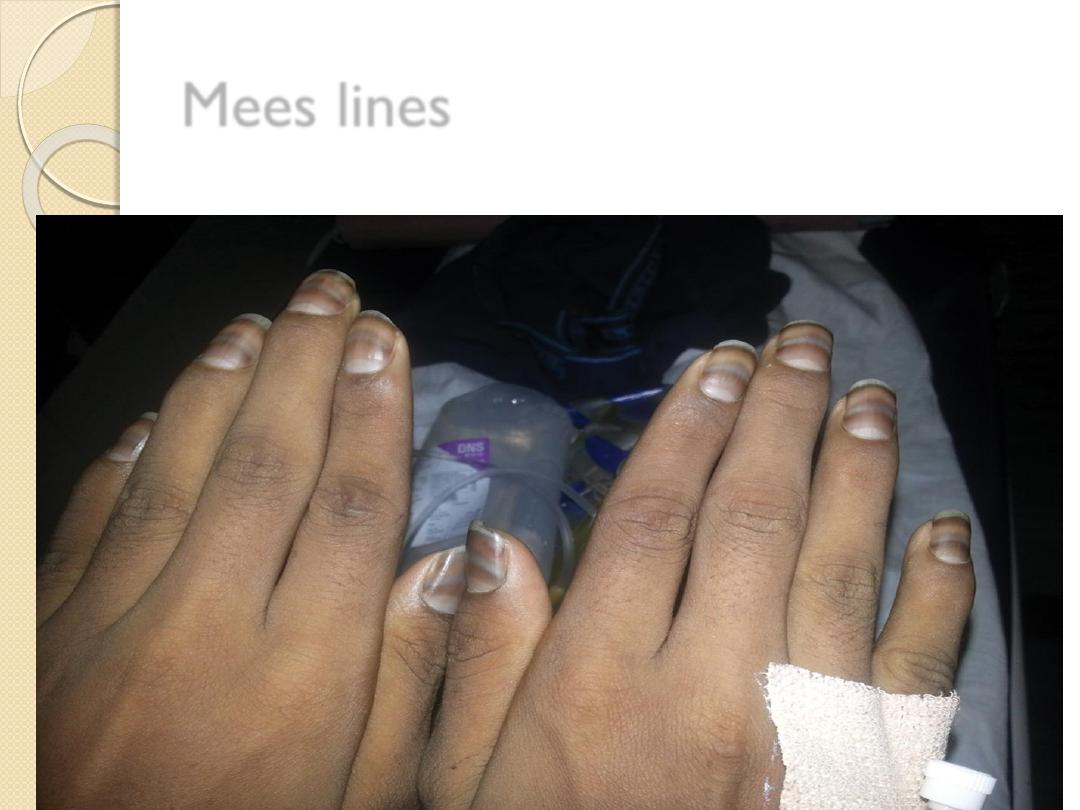
Mees lines
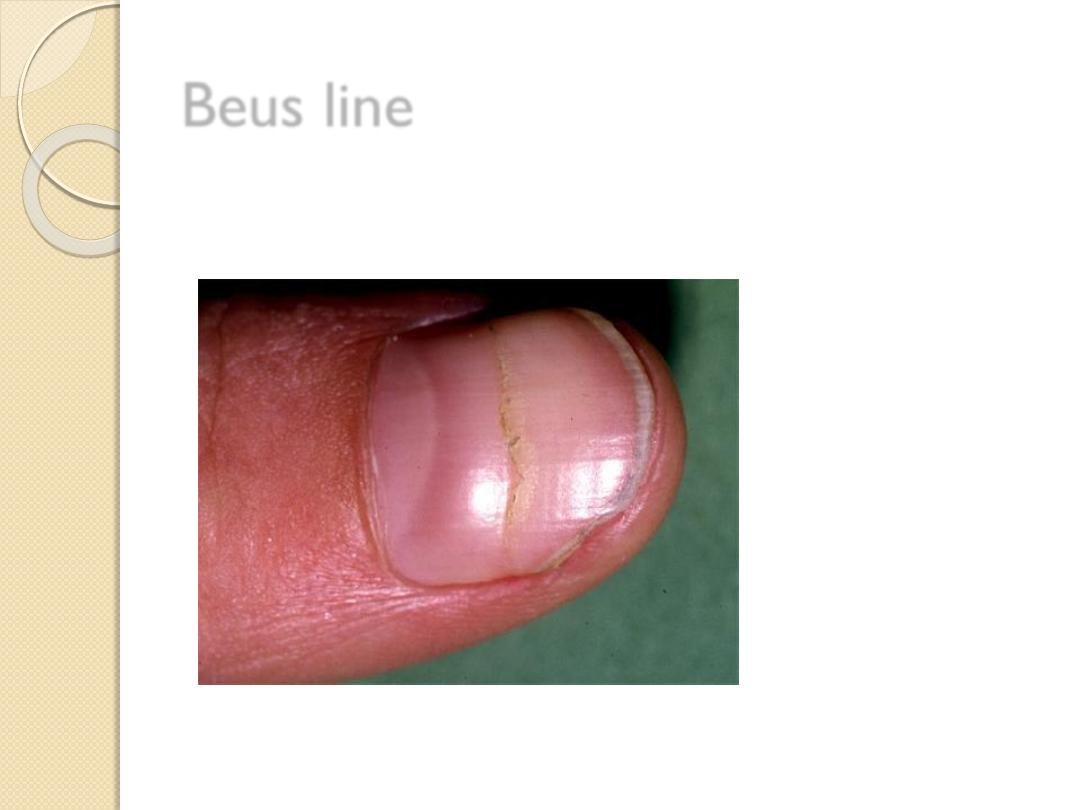
Beus line

HANDS
Palmar erythema
Dupuytren
’s contractures
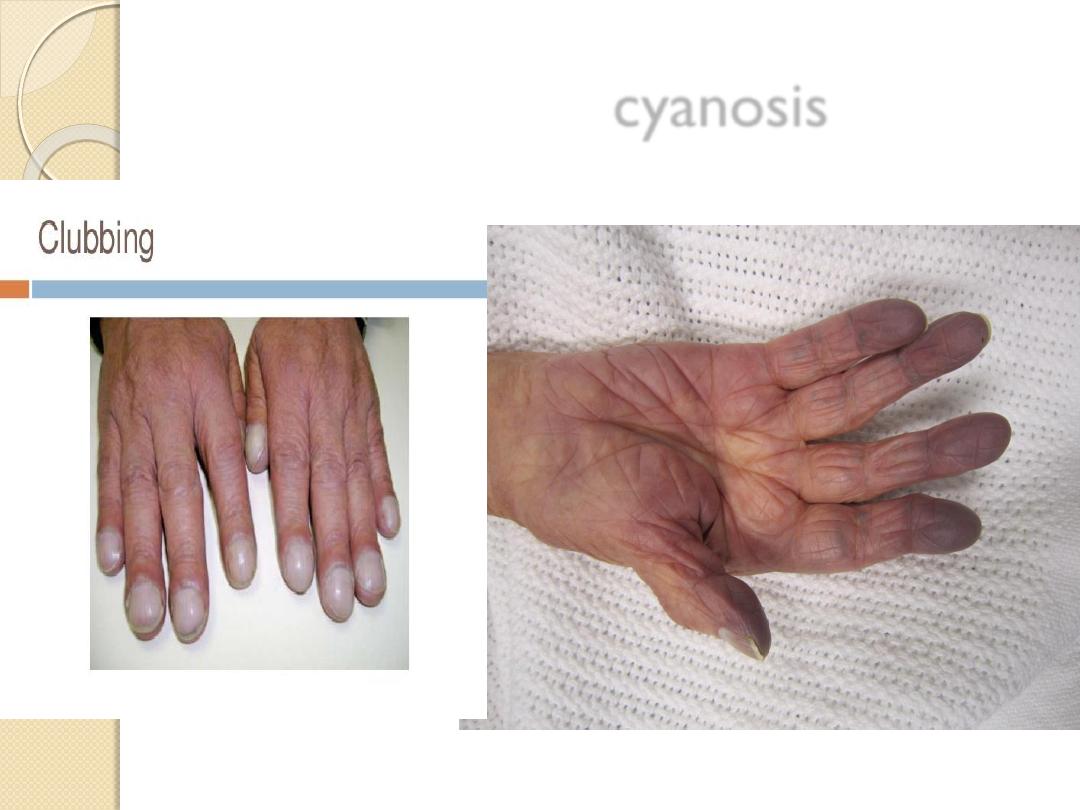
cyanosis
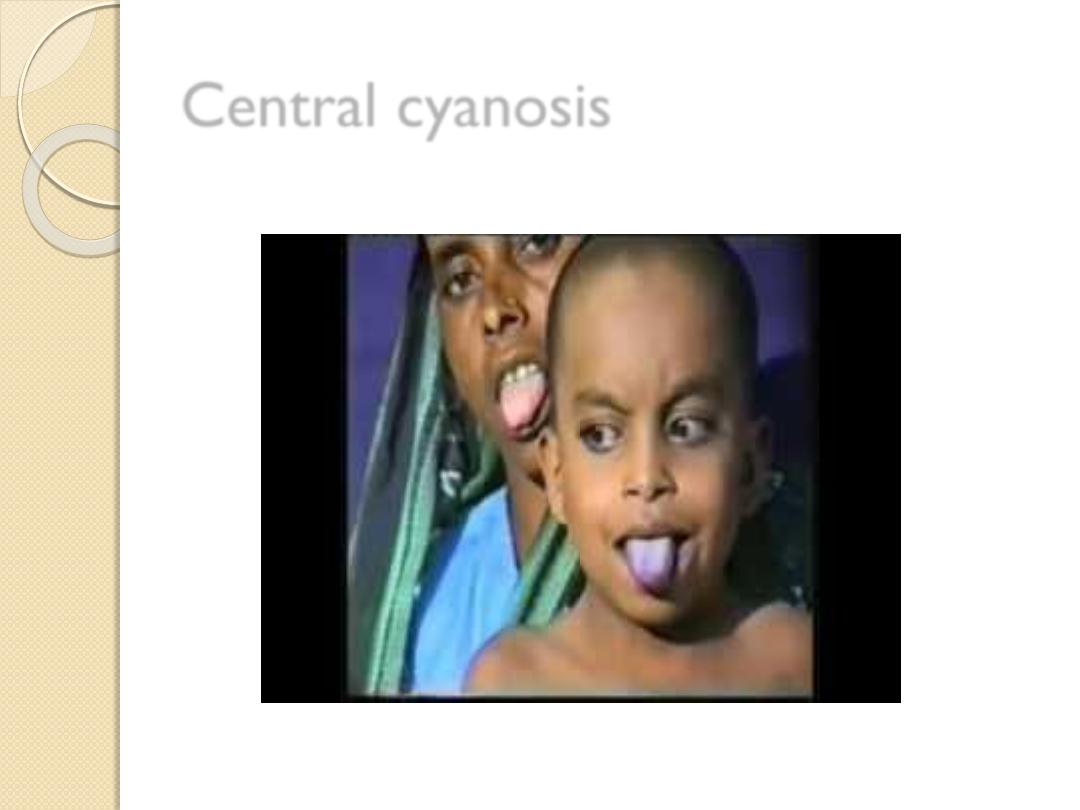
Central cyanosis

ARMS
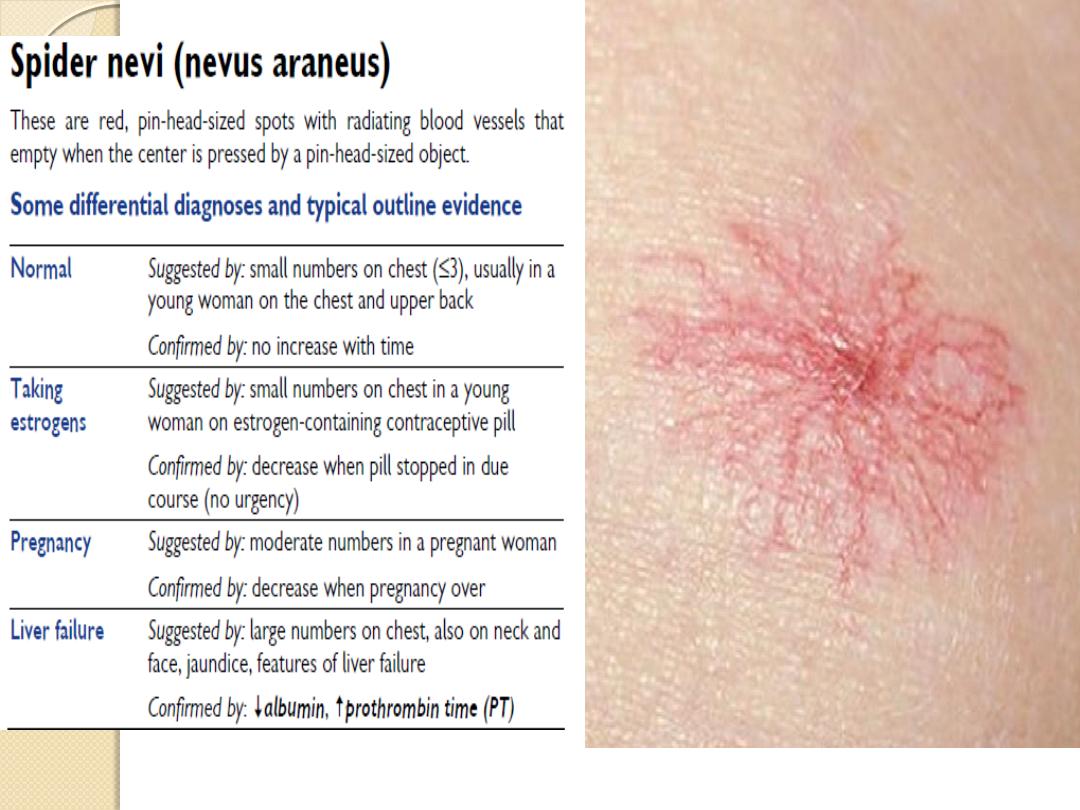
Spider naevi (telangiectatic lesions)
Bruising
Wasting
Scratch marks (chronic cholestasis)

FACE, EYES …
Conjuctival pallor (anaemia)
Sclera: jaundice, iritis
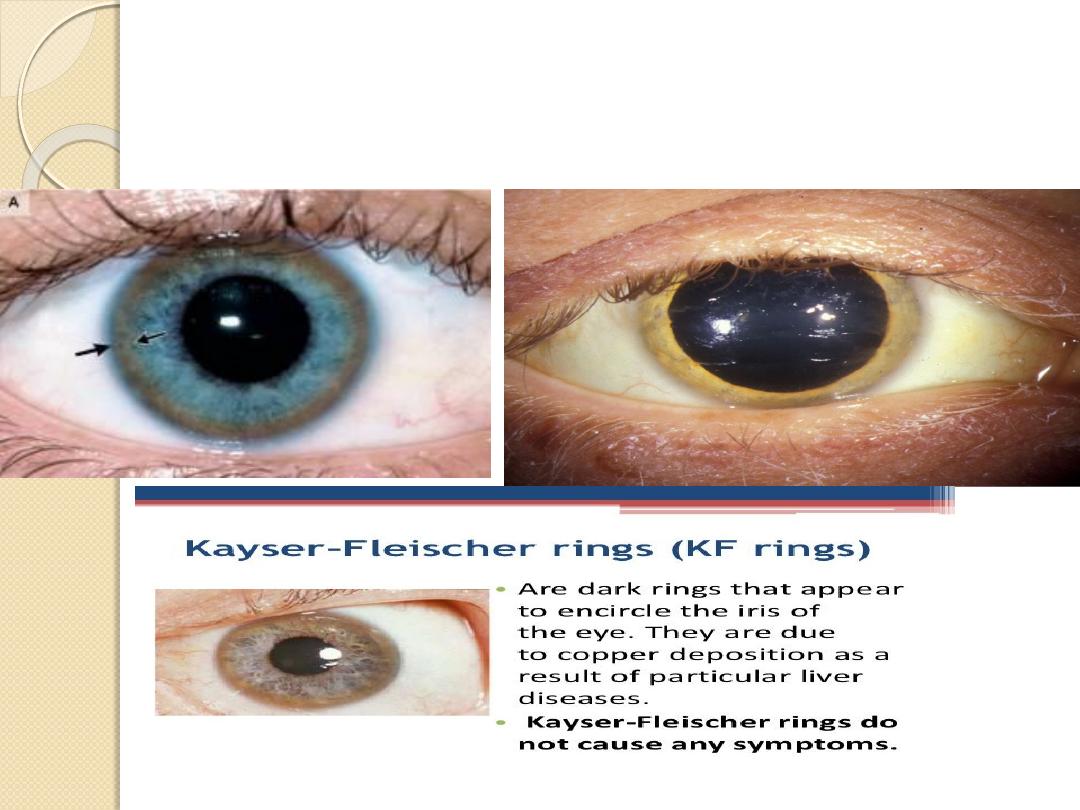
Cornea: Kaiser Fleischer’s rings (Wilson’s disease)
Xanthelasma (primary biliary cirrhosis)
Parotid enlargement (alcohol)
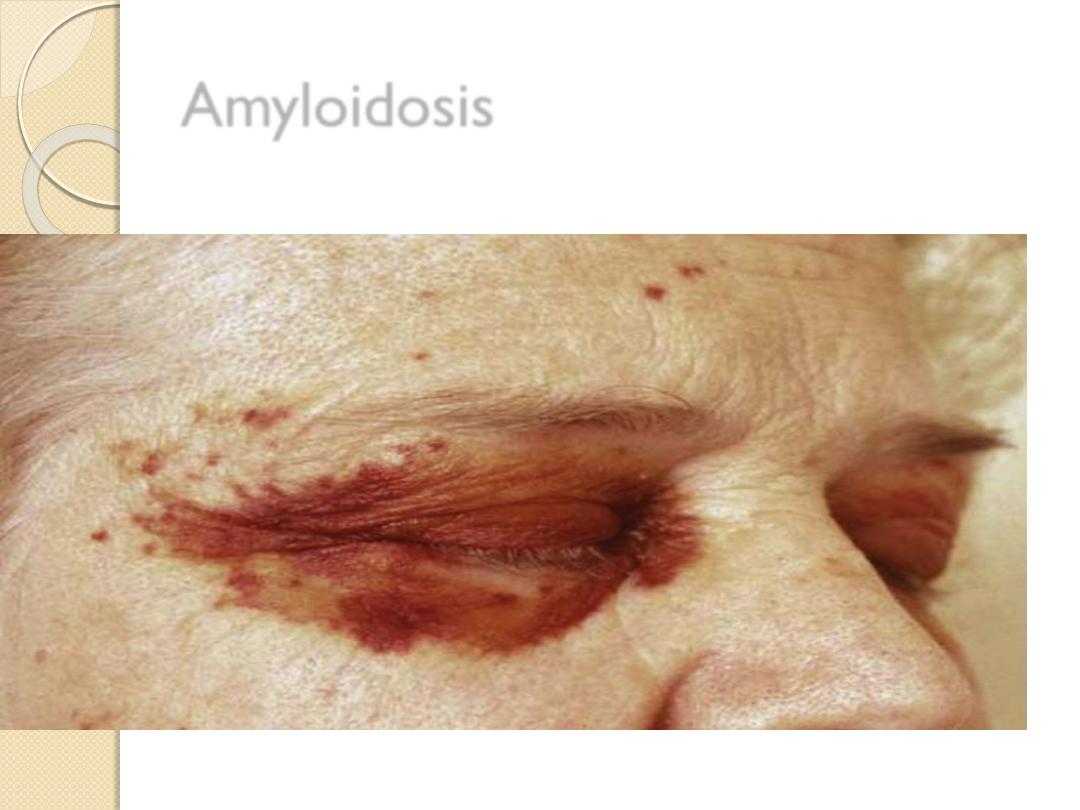
Amyloidosis

History
· History of consanguinity.
· In young adult or child - hepatitis, haemolytic anaemia, portal hypertension or
neuropsychiatric abnormalities.
· In adolescents - presents as liver disease.
· In adults <40 years of age consider chronic or fulminant hepatitis.
Examination
Greenish yellow to golden-brown pigmentation at the limbus of the cornea, called the
Kayser-Fleischer ring. The ring is most marked
at the superior and inferior poles of the cornea and is due to the deposition of copper
in Descemet's membrane in the cornea. It may be absent in patients with hepatic
manifestations only but is present in those
with neuropsychiatric disease.):
Look for the following:
· Jaundice (look at the sclera).
· Sunflower cataracts.
· Hepatomegaly.
· Signs of liver cell failure.
· Neurological manifestations - tremor, chorea, mask-like facies with a vacuous smile.
DIAGNOSIS
This patient has a classical Kayser-Fleischer ring with jaundice and hepatomegaly
(lesions) due to Wilson's disease (aetiology)and
does not have a hepatic flap (functional status).

Parotid enlargement
Xanthelasma
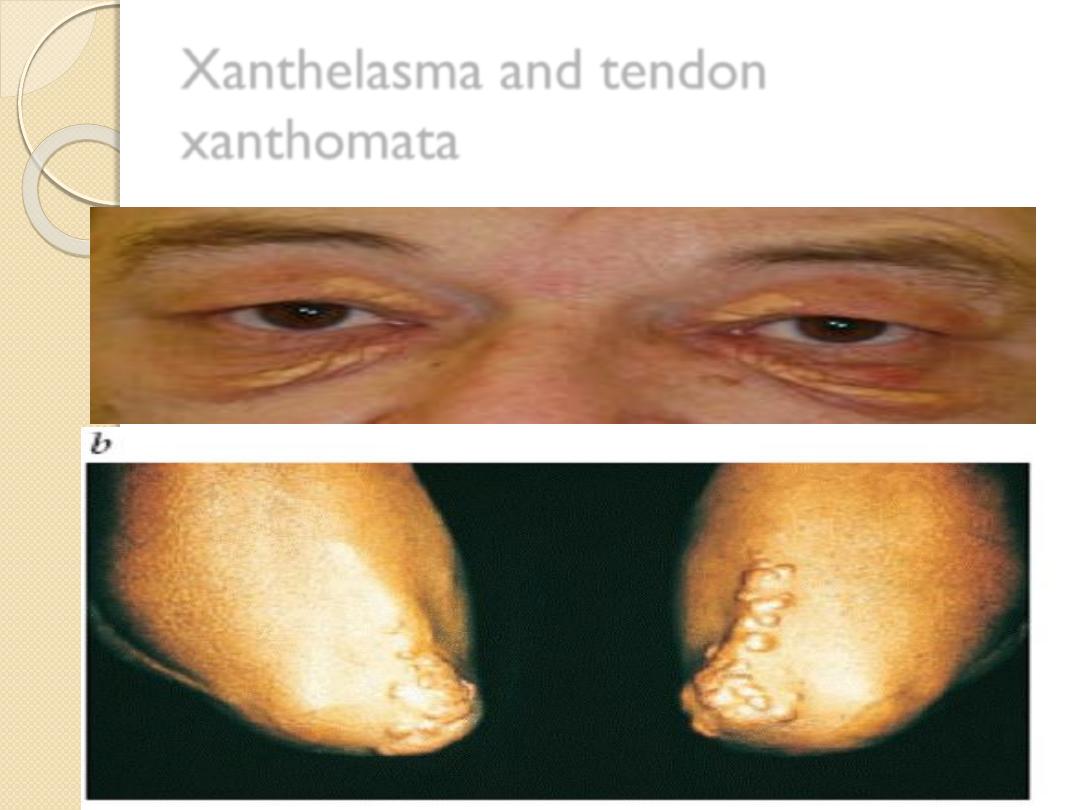
Xanthelasma and tendon
xanthomata
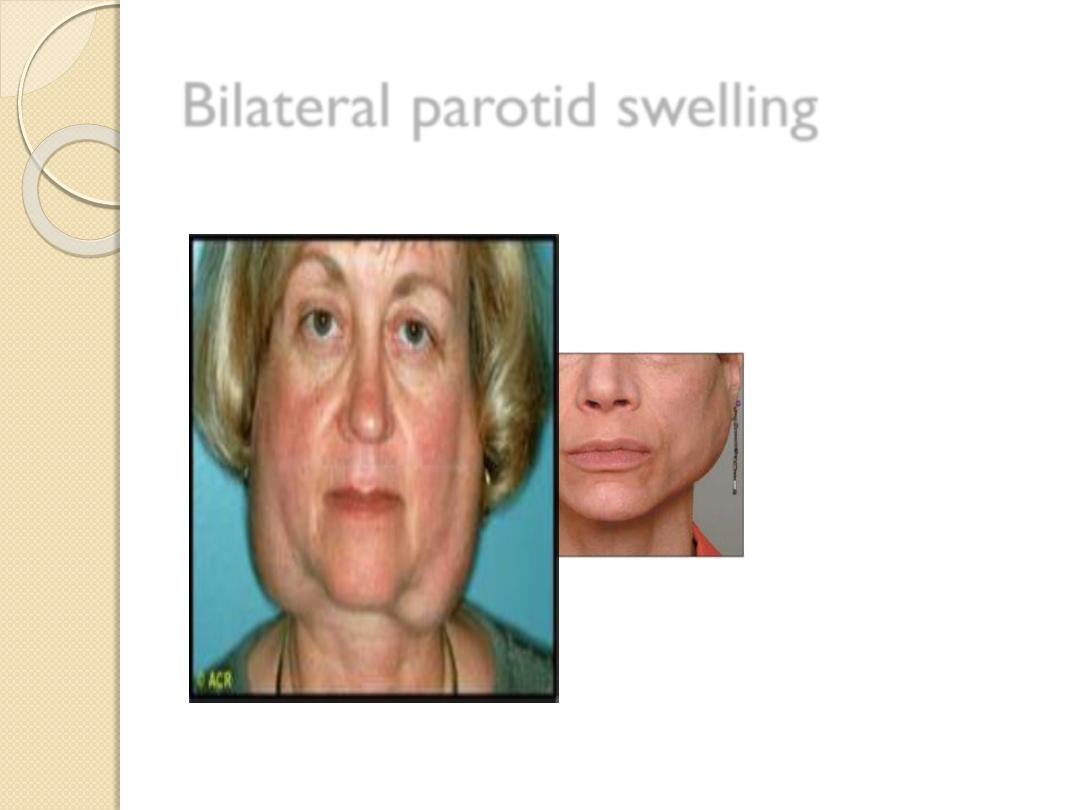
Bilateral parotid swelling
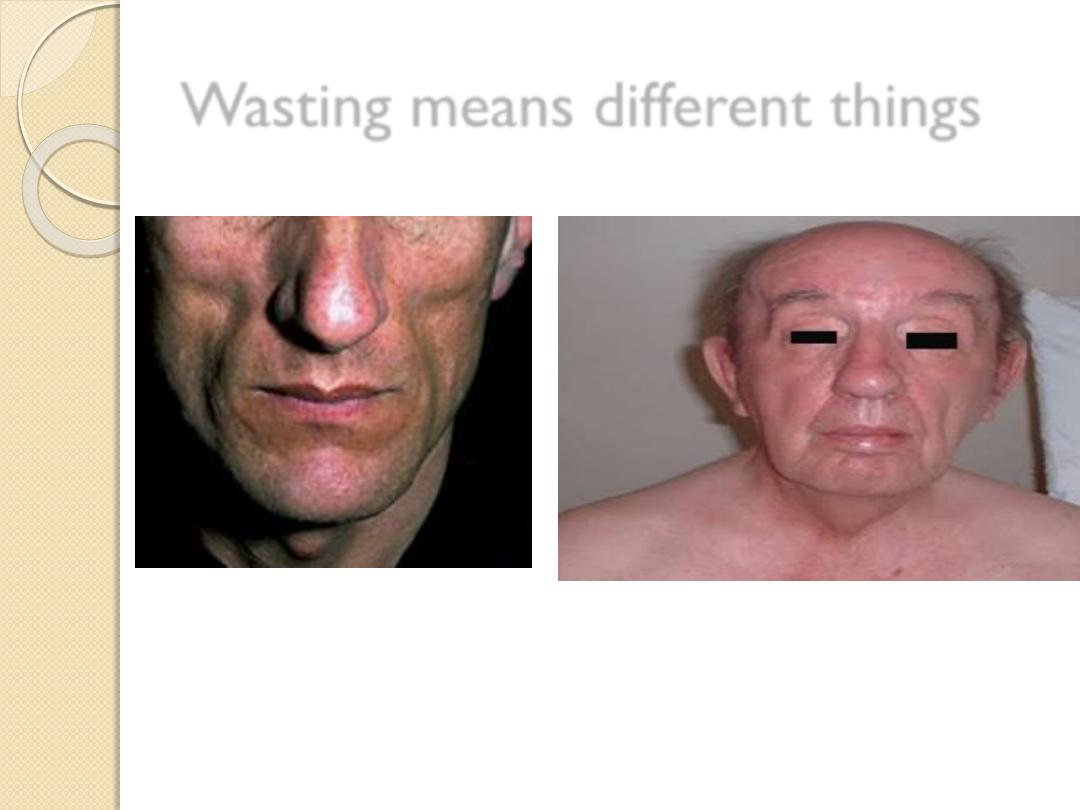
Wasting means different things
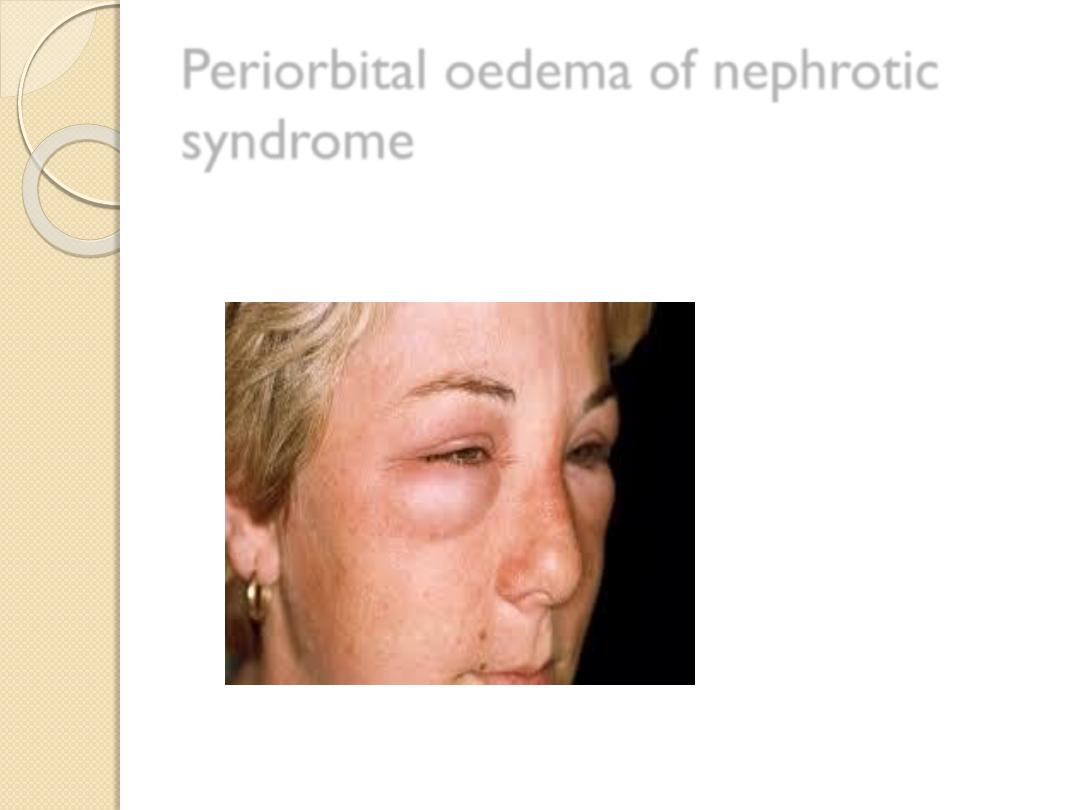
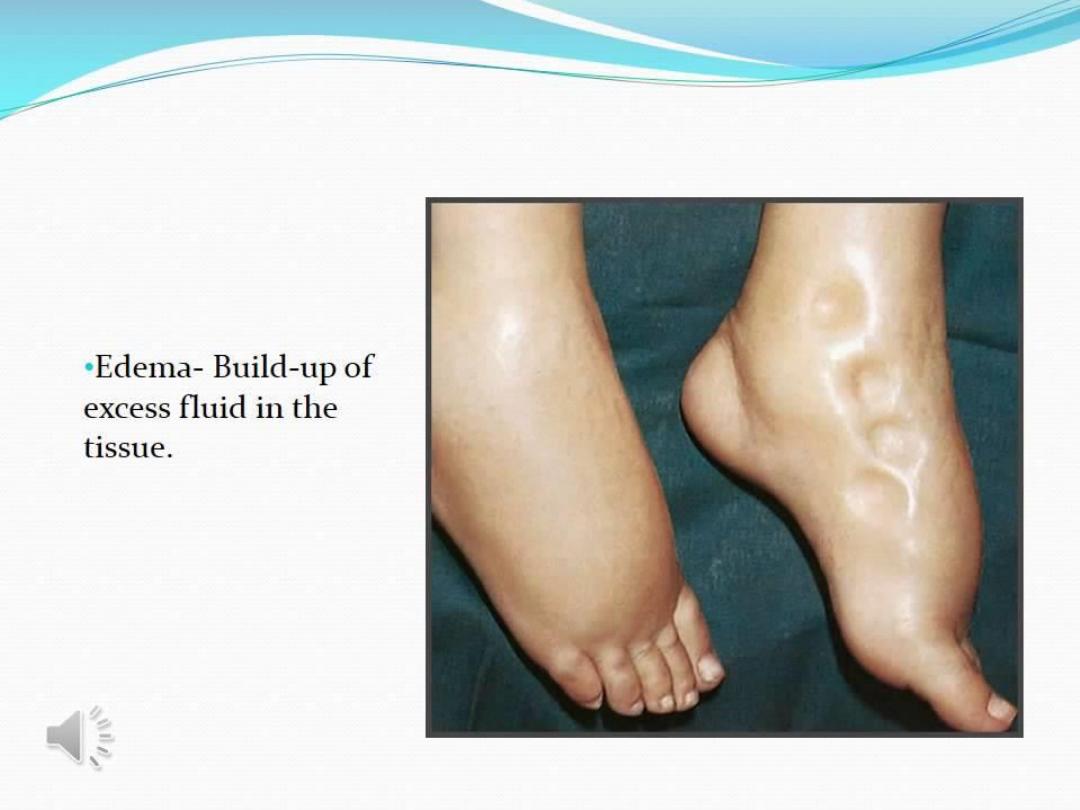
Periorbital oedema of nephrotic
syndrome

Dermatitis Herpetiformis
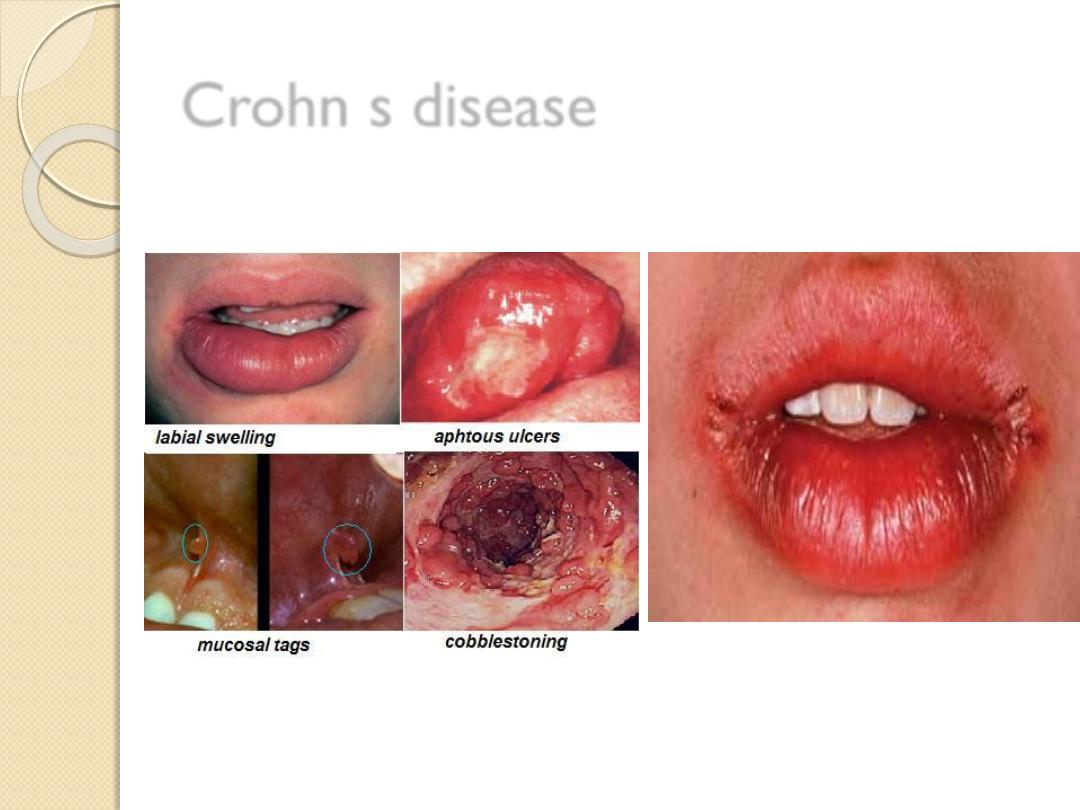
Crohn s disease
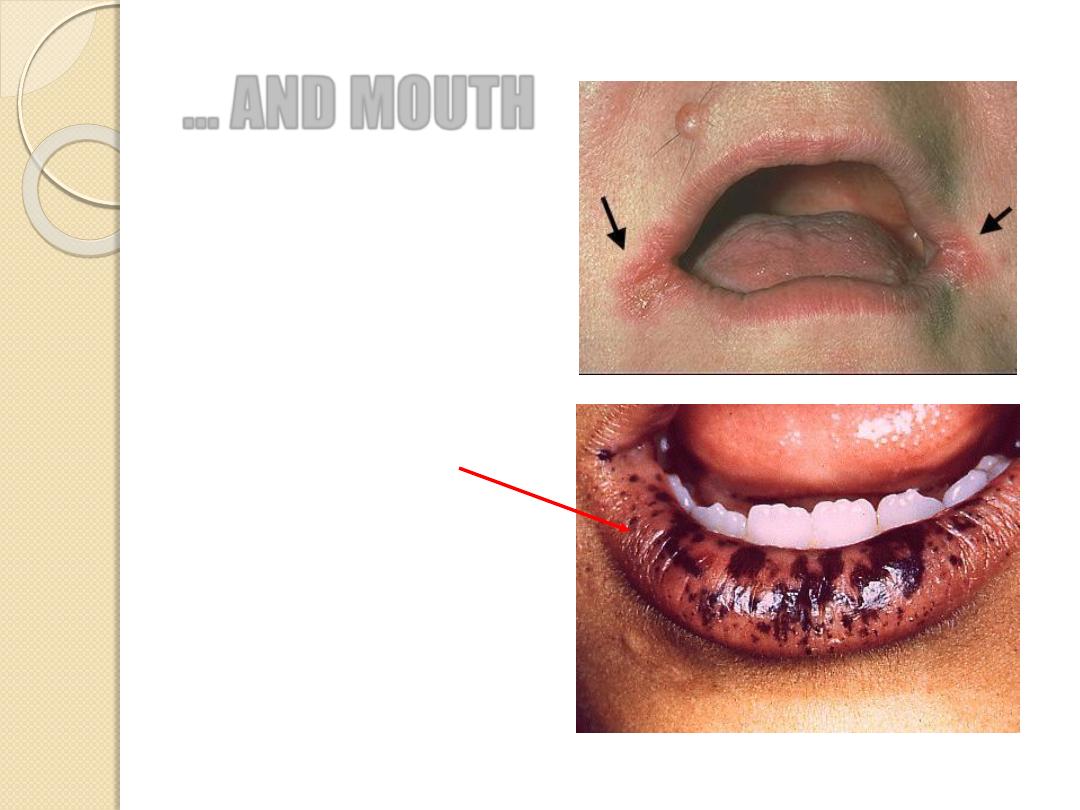
… AND MOUTH
Breath (fetor hepaticus)
Lips
◦
Angular stomatitis
◦
Cheilitis
◦
Ulceration
◦
Peutz-Jeghers syndrome
Gums
◦
Gingivitis, bleeding
◦
Candida albicans
◦
Pigmentation
Tongue
◦
Atrophic glossitis
◦
Leicoplakia
◦
Furring
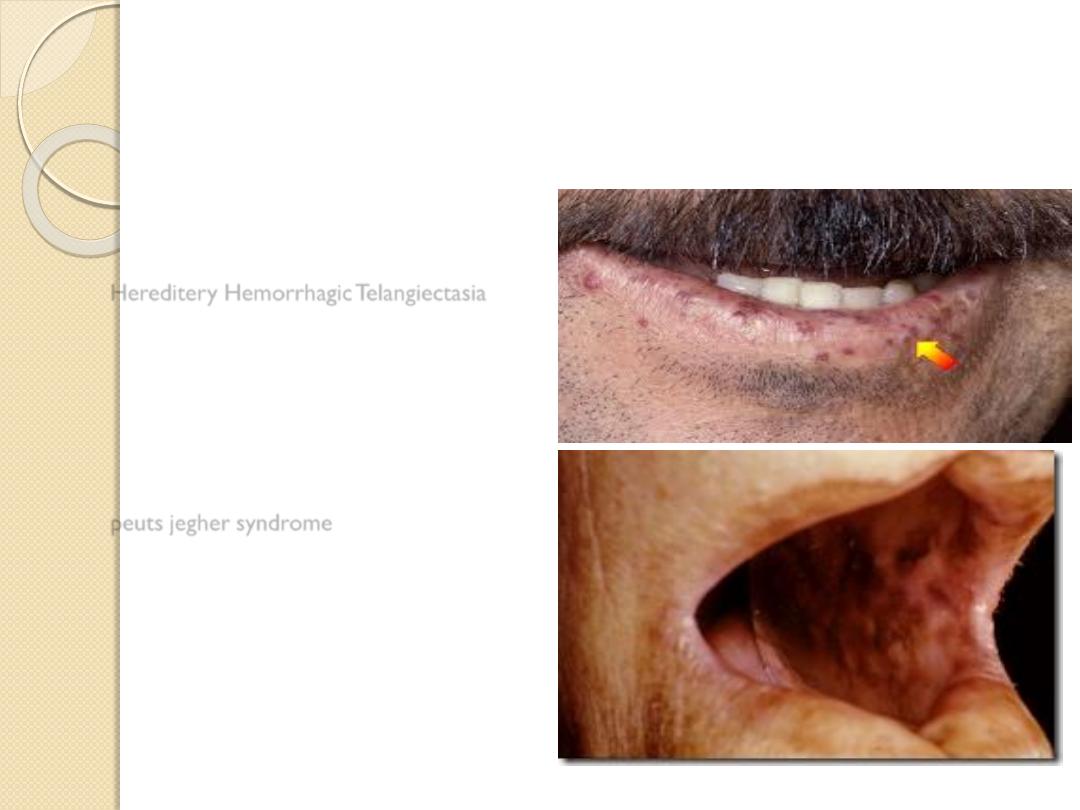
Hereditery Hemorrhagic Telangiectasia
peuts jegher syndrome

Atrophic glossitis
Thrush

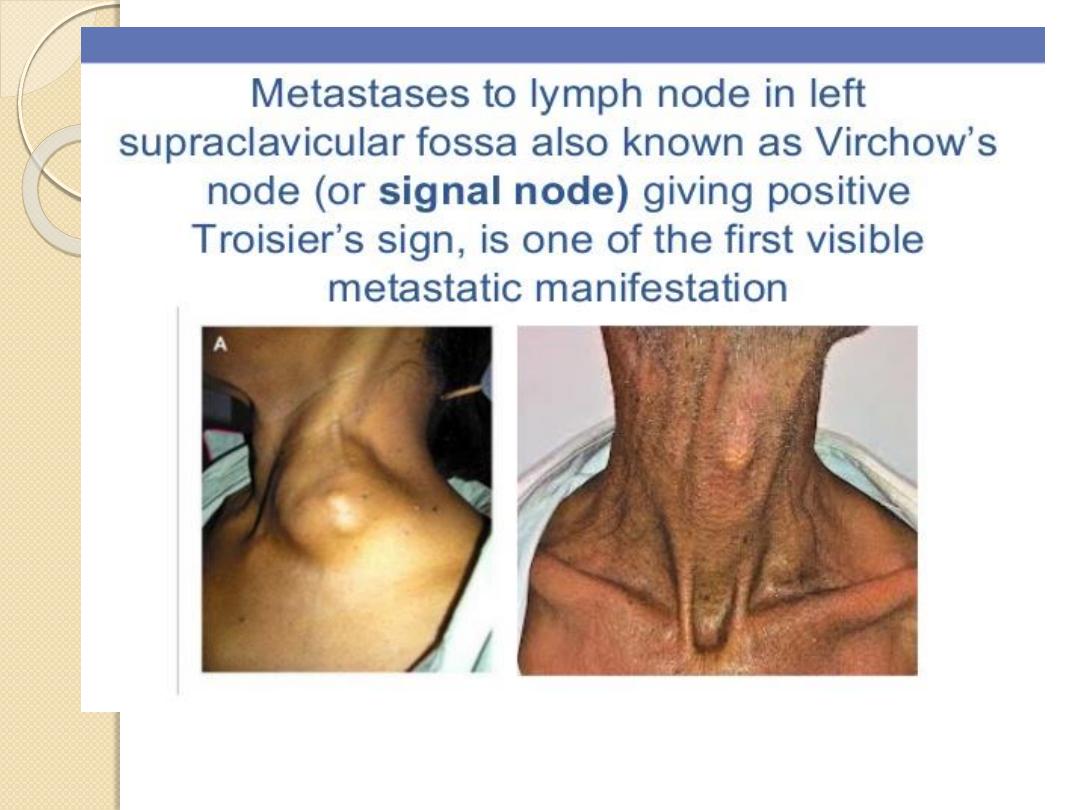
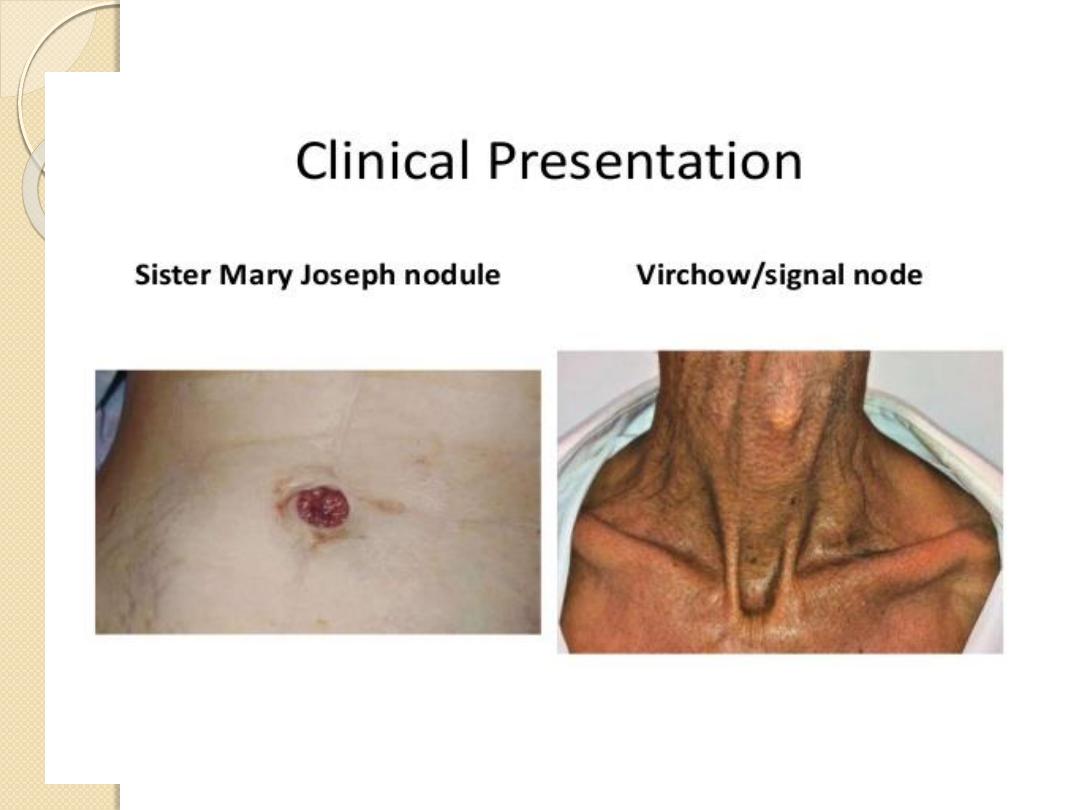
NECK AND CHEST
Cervical lymphadenopathy
Left supraclavicular fossa (Virchow’s node)
Gynaecomastia
Loss of hair


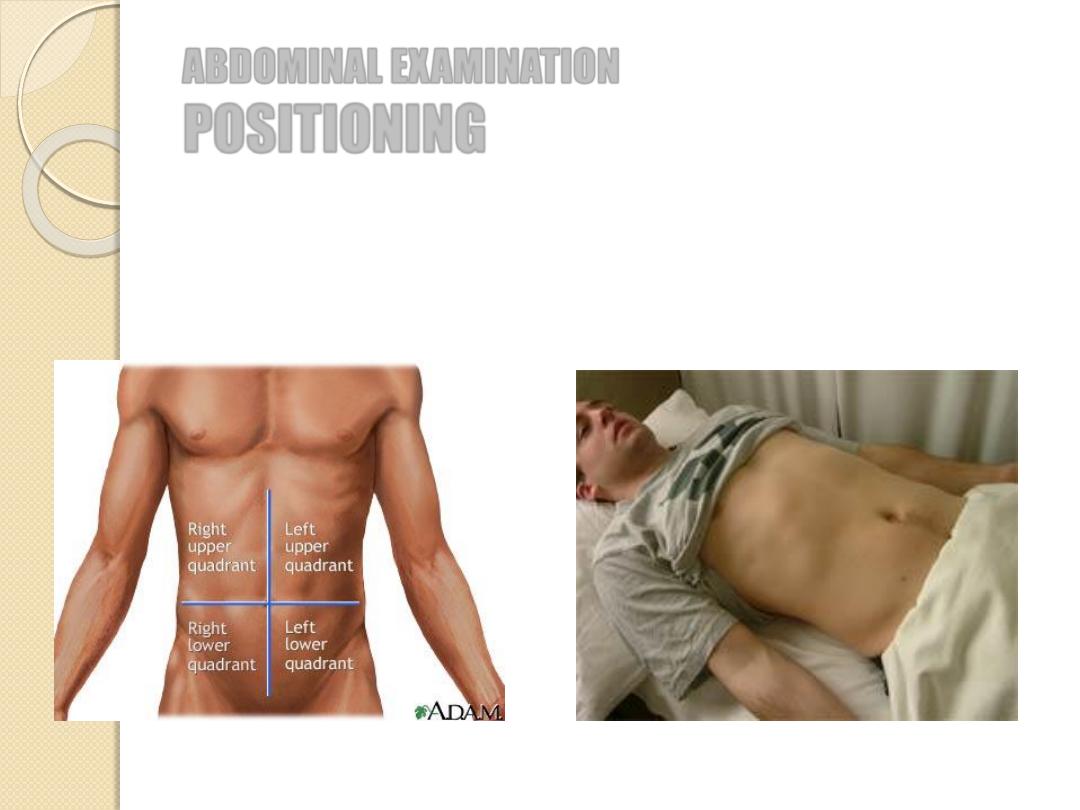
ABDOMINAL EXAMINATION
POSITIONING
Abdomen can be divided in four quadrants
Patient should be lying on supine position
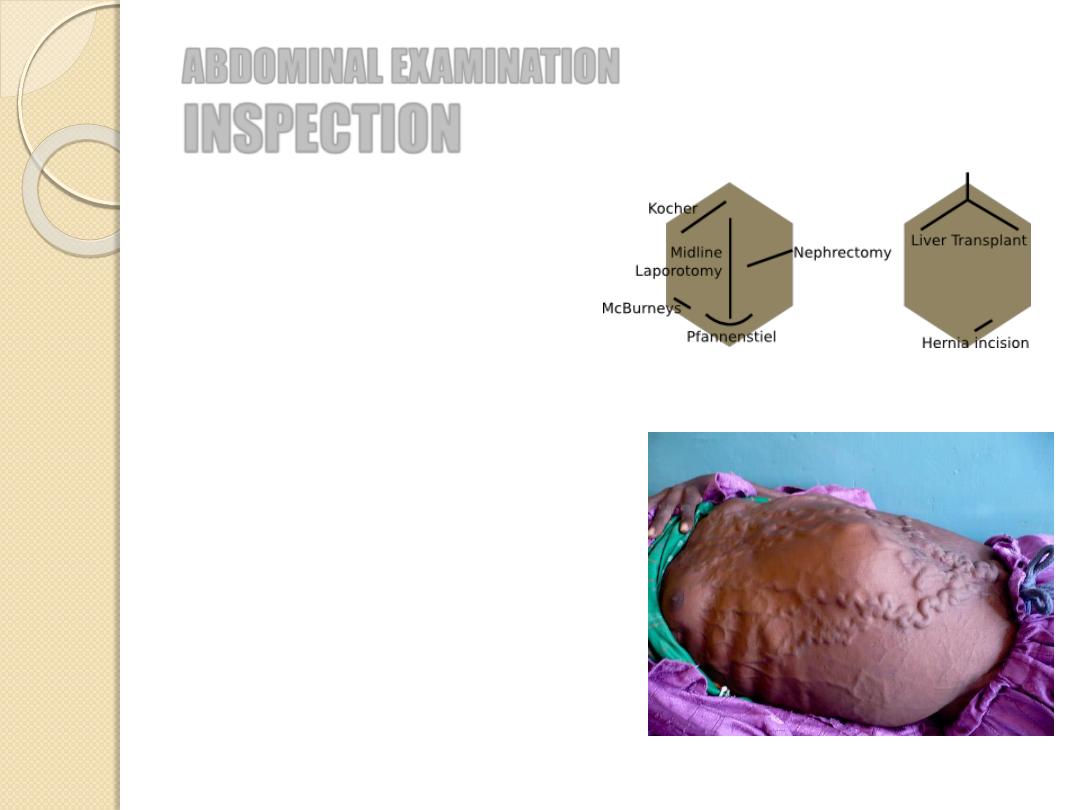
ABDOMINAL EXAMINATION
INSPECTION
Shape and movements
Scars
Distension
◦
Localised: mass, organomegaly
◦
Generalized: 5 F’s
Prominent veins (caput medusae)
Striae
Bruises
Pigmentation
Visible peristalsis

Tête de Méduse, by Peter Paul Rubens (1618)

Caput medosae in Cavernous sinus
thrombosis
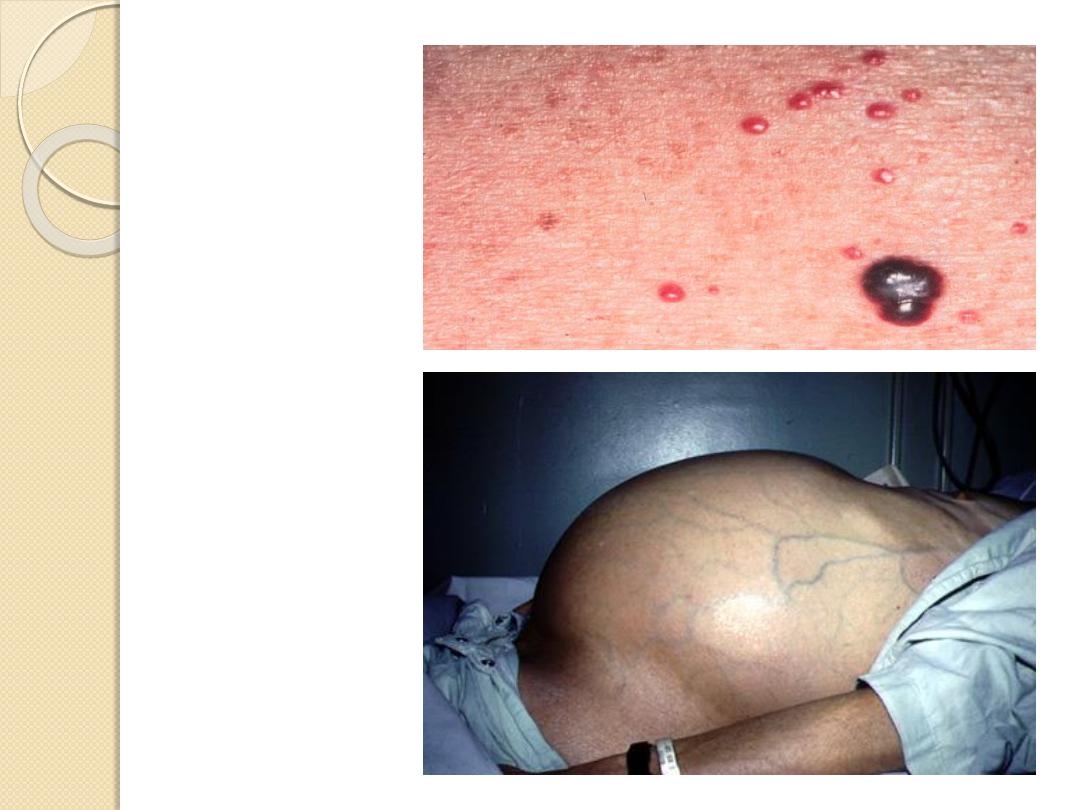
Campbell de
Morgan spots
Ascitic abdomen
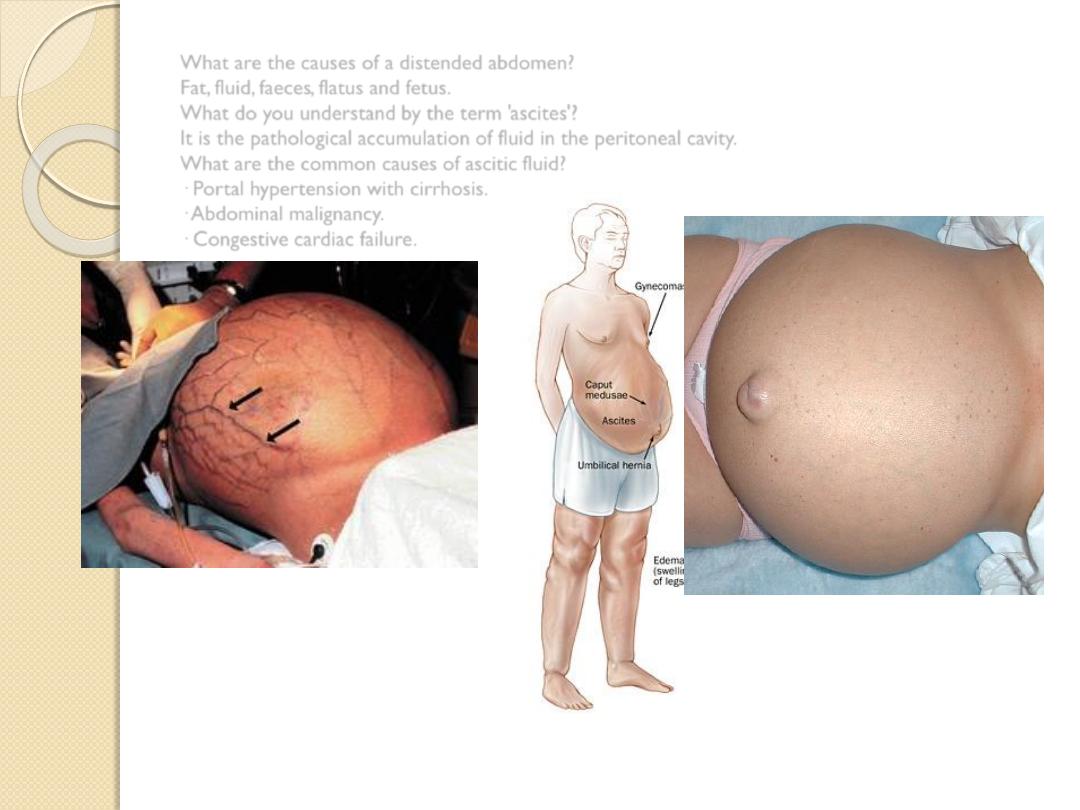
What are the causes of a distended abdomen?
Fat, fluid, faeces, flatus and fetus.
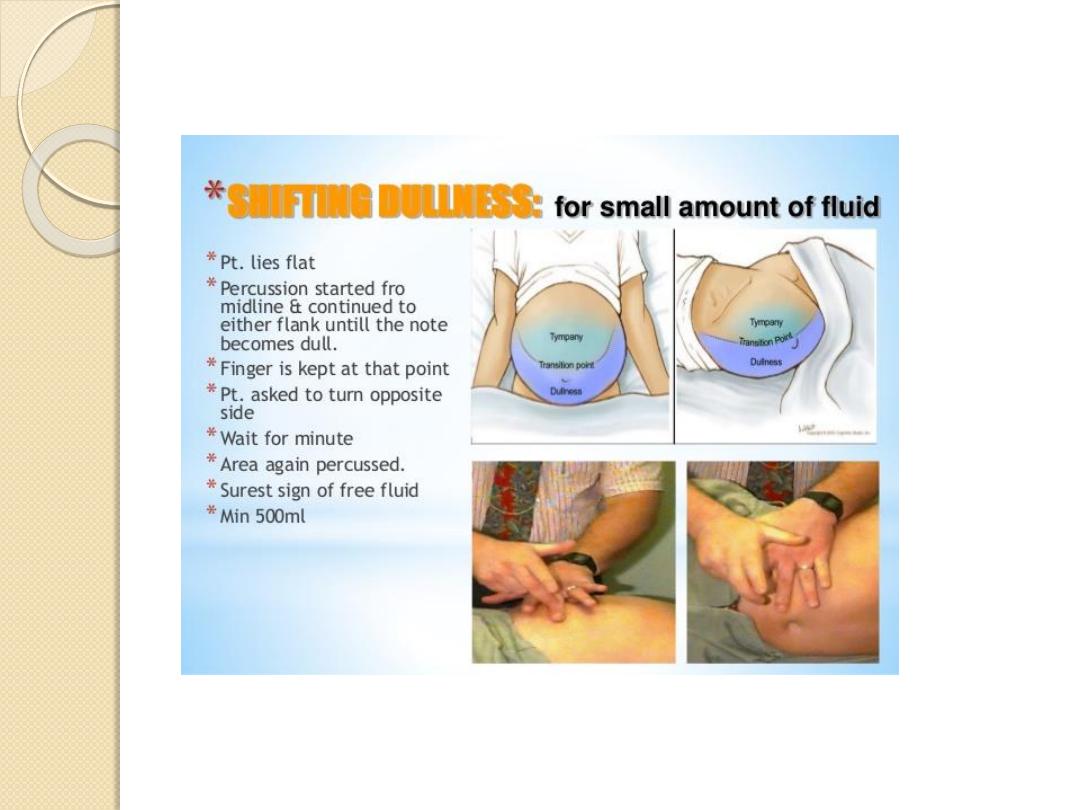
What do you understand by the term 'ascites'?
It is the pathological accumulation of fluid in the peritoneal cavity.
What are the common causes of ascitic fluid?
· Portal hypertension with cirrhosis.
· Abdominal malignancy.
· Congestive cardiac failure.
ABDOMINAL EXAMINATION
PALPATION
1.
Ensure that your hands are warm
2.
Stand on the patient’s right side
3.
Help to position the patient
4.
Ask whether the patient feels any pain before
you start
5.
Begin with superficial examination
6.
Move in a systematic manner through the
abdominal quadrants
7.
Repeat palpation deeply.
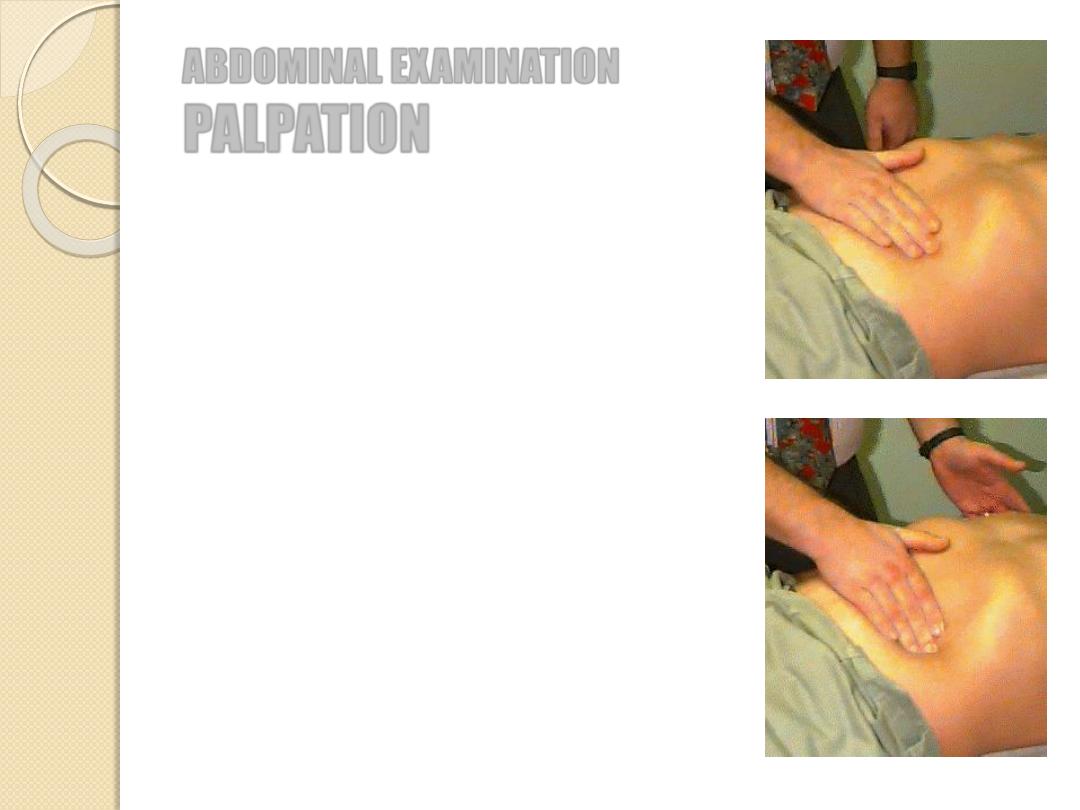
ABDOMINAL EXAMINATION
PALPATION
Tenderness: discomfort and resistance to palpation
Involuntary guarding: reflex contraction of the
abdominal muscles
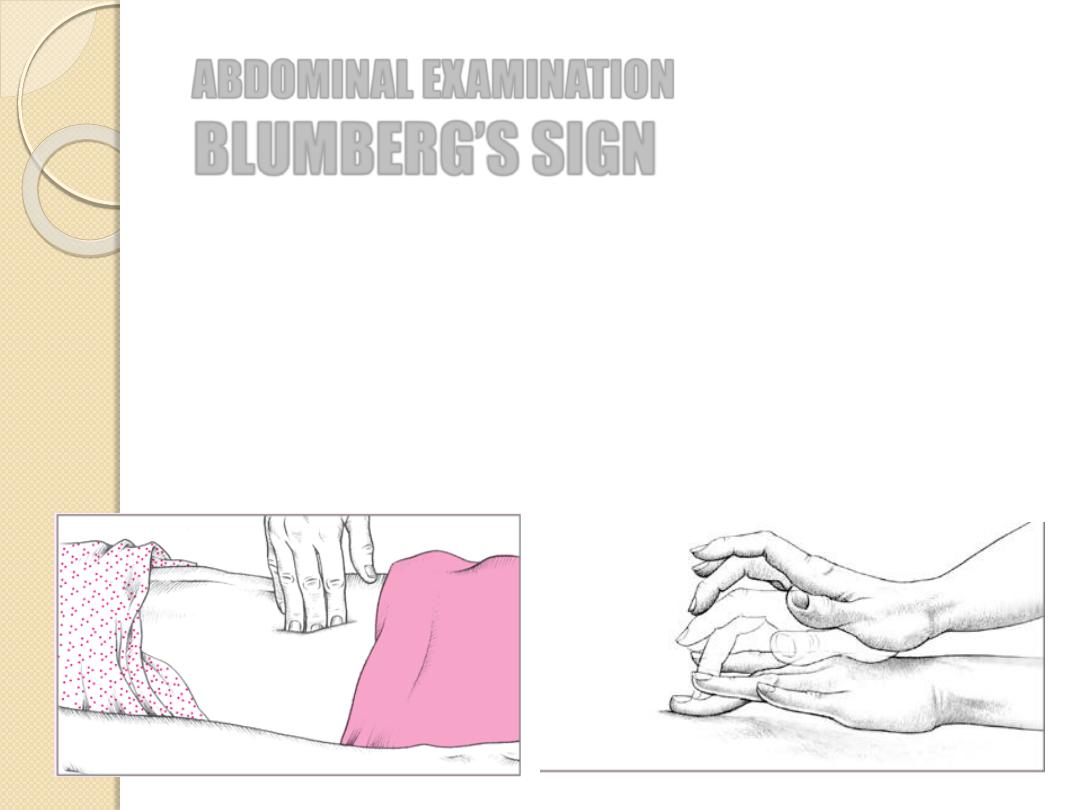
Rebound tenderness: patient feels pain when the
hand is released
Tenderness + rigidity: perforated viscus
Palpable mass (enlarged organ, faeces, tumour)
Aortic pulsation
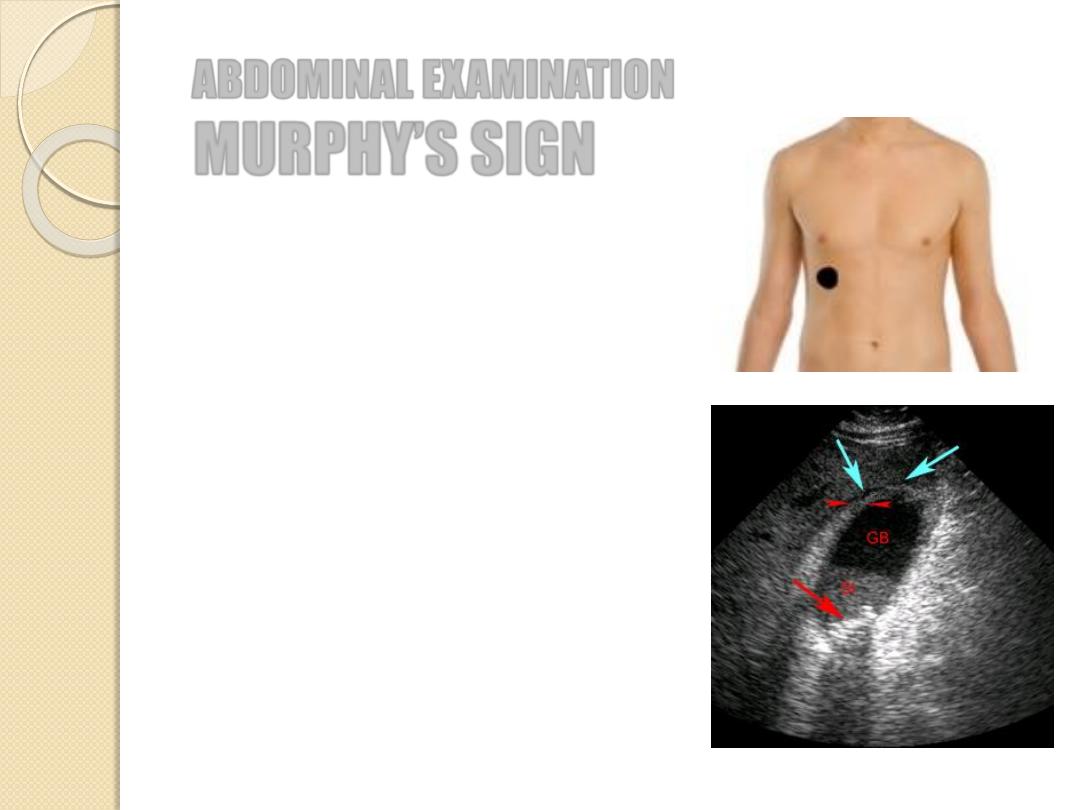
Pain in RUQ
Inflammation of gallbladder
(cholecystitis)
ABDOMINAL EXAMINATION
MURPHY’S SIGN
a.k.a. rebound tenderness
Pain upon removal of pressure rather than application
of pressure to the abdomen
Peritonitis and/ or appendicitis
ABDOMINAL EXAMINATION
BLUMBERG’S SIGN
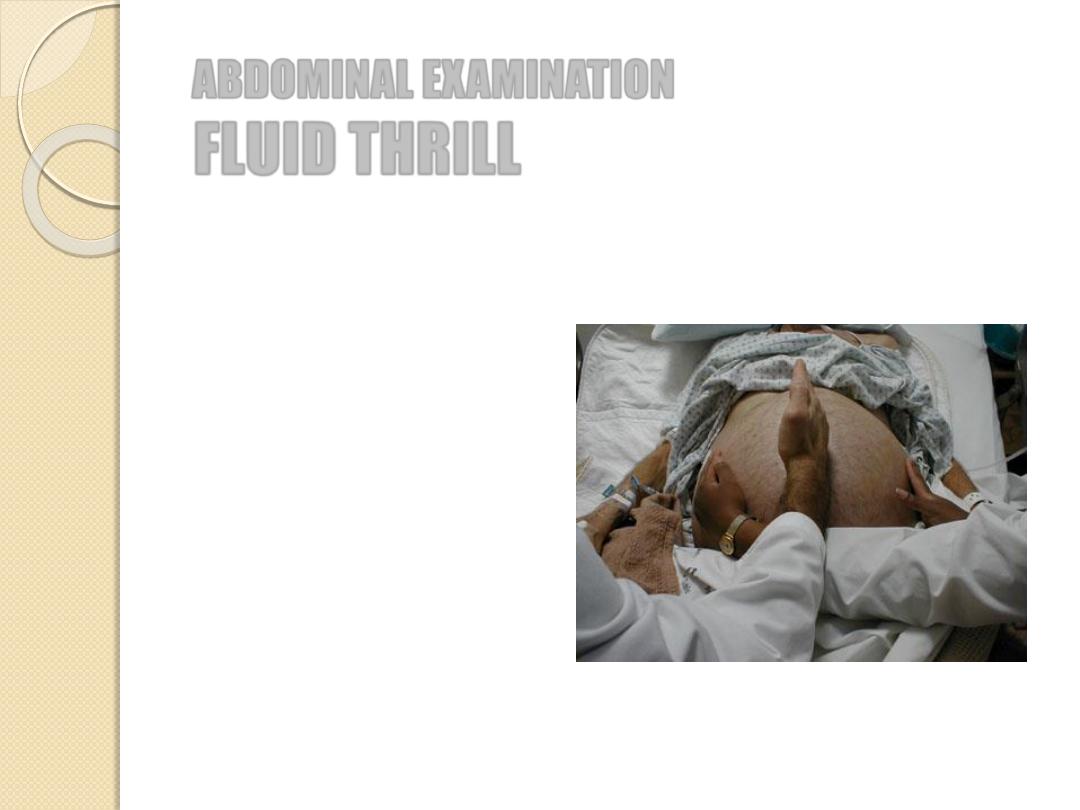
ABDOMINAL EXAMINATION
FLUID THRILL
Place the palm of your left
hand against the left side of the
abdomen
Flick a finger against the right
side of the abdomen
Ask the patient to put the edge
of a hand on the midline of
the abdomen
If a ripple is felt upon flicking
we call it a fluid thrill = ascites
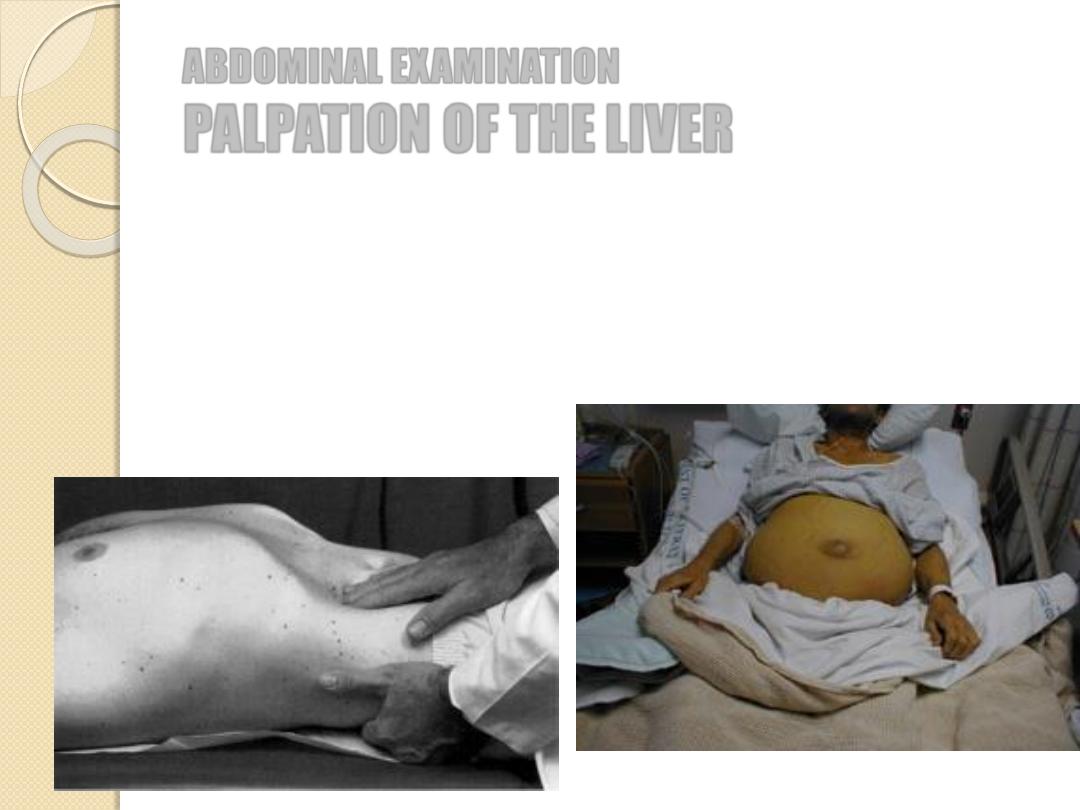
ABDOMINAL EXAMINATION
PALPATION OF THE
LIVER
1.
Start palpating in the right iliac fossa
2.
Ask the patient to take a deep breath in
3.
Move your hand progressively further up the abdomen
4.
Try to feel the liver edge

Note
,
By percussion, the mean liver size is 7 cm for women and
10.5 cm for men. A liver span 2-3 cm larger or smaller than these
values is considered abnormal.
History of fatigue, weight loss, jaundice.
History of alcohol abuse.
History of hepatitis B, intravenous blood products.
History of intravenous drug abuse.
Mental status changes (hepatic encephalopathy).
History of drugs (methyldopa, amiodarone, methotrexate).
History of Wilson's disease, alpha 1-antitrypsin deficiency.

In the hands
:
-Clubbing, leukonychia.
-Dupuytren's contracture (see Fig. 90), palmar
erythema.
Spider nevi tattoos, hepatic flap, pallor.
Scratch marks, generalized pigmentation.
Eyes and face
: icterus, cyanosis, parotid enlargement.
Ches
t: spider naevi, loss of axillary hair,
gynaecomastia.
Abdomen
:
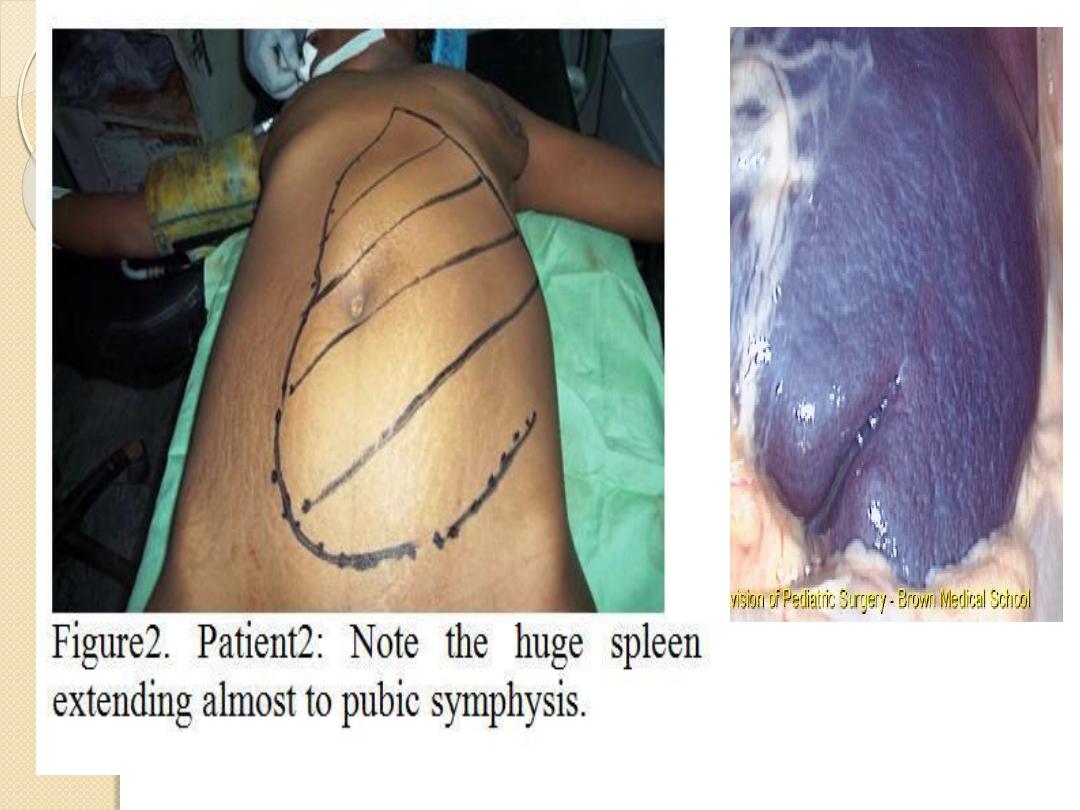
-Splenomegaly (seldom more than 5 cm below the
costal marg
Ascites.
- Hepatomegaly (particularly in alcoholic liver disease).
Loss of hair on the shins.
Leg oedema.
Tell the examiner that you would like to look for
testicular atrophy.
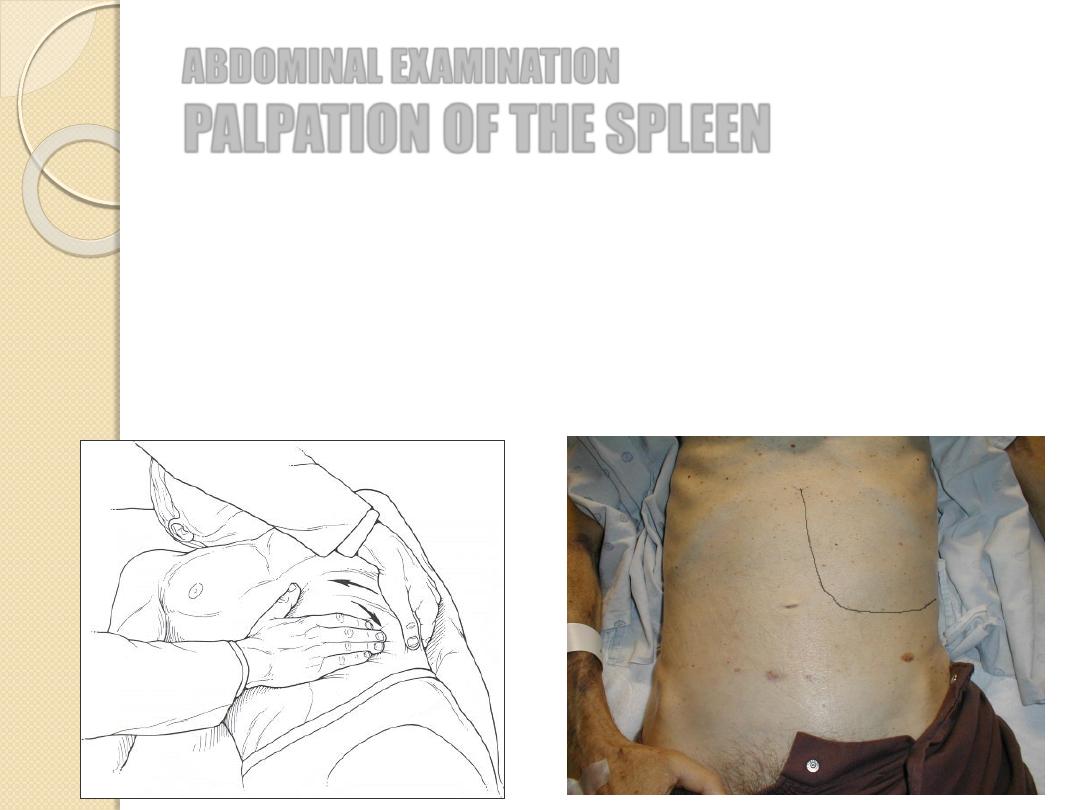
ABDOMINAL EXAMINATION
PALPATION OF THE
SPLEEN
1.
Roll the patient towards you
2.
Palpate with your left hand while using your left hand to press
forward on the patient’s lower ribs from behind
3.
Feel along the costal margin
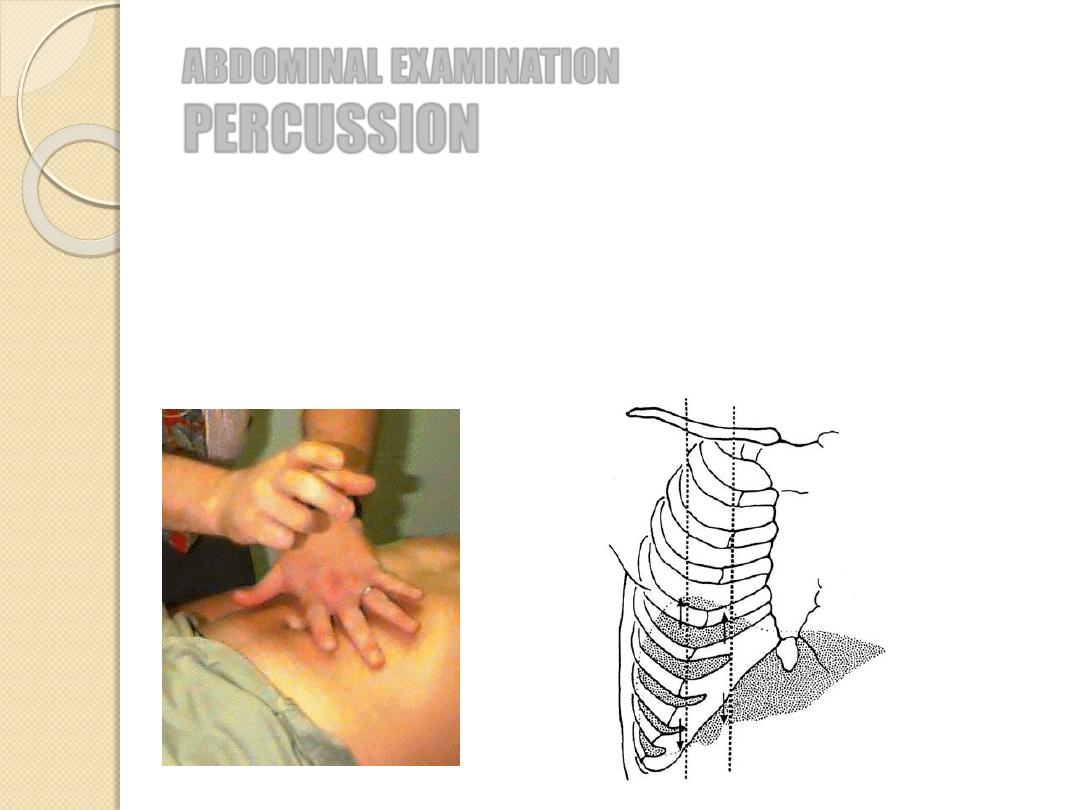
ABDOMINAL EXAMINATION
PERCUSSION
Dull sounds: solid or fluid-filled structures
Resonant sounds: structures containing air or gas
ABDOMINAL EXAMINATION
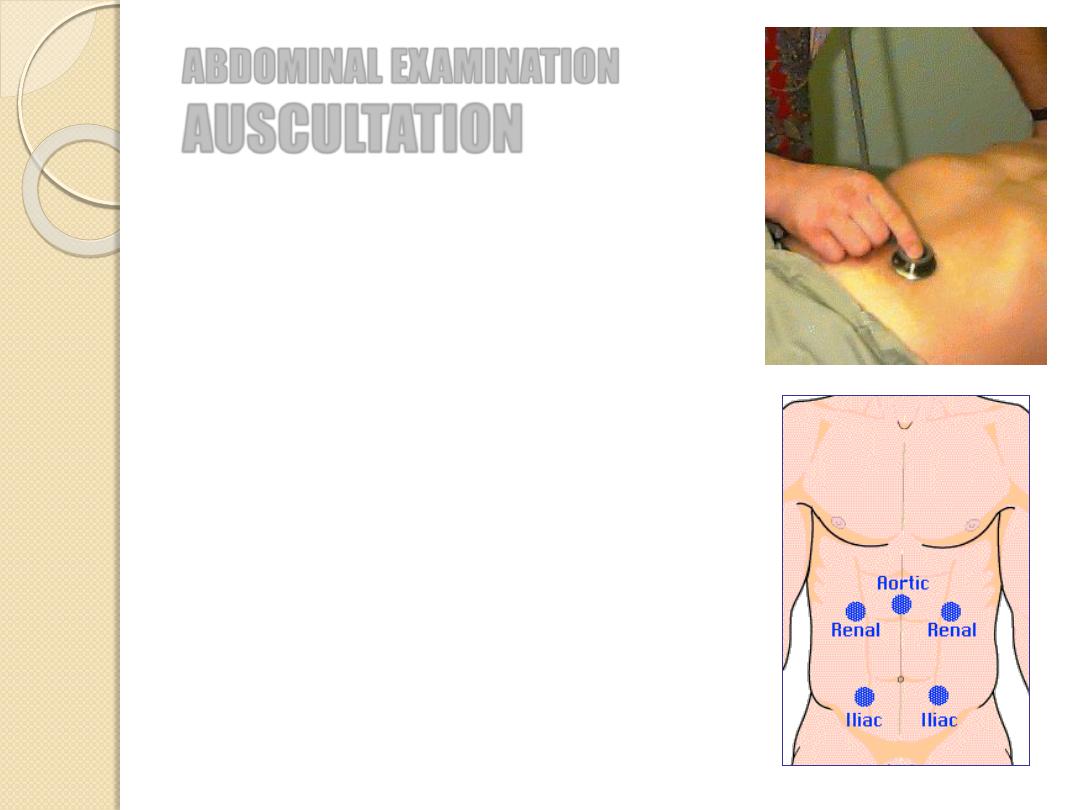
AUSCULTATION
Place the diaphragm of the stethoscope to
the right of the umbilicus
Bowel sounds (borborygmi) are caused by
peristaltic movements
Occur every 5-10 sec.
Absence of b.s.: paralytic ileus or peritonitis
Bruits over aorta and renal a. could be a
sign of an aneurysm and stenosis