
1
WARFARE INJURIES
Penetrating missile wounds, injury from blast phenomena & burn are the typical
feature of modern war.
Hallmark of modern war injury;
*Multiple injuries to different body systems.
*The aim of warfare is to maim not to kill.
*Fragments are the commonest wounding agents.
*No characteristic war wound.
*Variety of injuries requires intuitive care.
MECHANISM OF INJURY
As a missile traverse the body it cause injury by transferring some or all of its
available energy ,and this is manifested by lacerating &crushing tissues in its path
&in some cases, injury remote from missile path .The amount of energy
transferred may be expressed by the formula
KE"available energy" =1/2M"mass"(V1-V2)2velosity at entrance &exit
respectively.
In general, bullets fired from handguns & most modern fragments munitions are
propelled at low velocity &have low available energy (100-500 J) &result in "low
energy transfer wounds". Missile with high available energy (2000_3000J) have
potential to cause "high-energy transfer wounds".
*Low_energy transfer wounds are characterized by injury confined to the wound
track.
*High-energy transfer wounds also cause local laceration &crush injury, but have
in addition, the potential to cause injury remote from the wound rack associated
with the phenomenon known as temporary cavitation.
This cavitation extent depends upon the density &elasticity of the target organ or
structures &, in certain circumstances is associated with injury many centimeters
away from the missile wound track.
Cavitation within solid organs such as the liver ,spleen &kidney results in
shattering with high morbidity &mortality .The extent of injury to bowel is variable
.In general ,small bowel fares better than the colon particularly if the latter is
loaded with faeces.
A similar event in an elastic tissue such as the lung may result in quite modest
injury .In the limb the position is more complex &controversial. While voluntary
muscle may merely stretch if injured in isolation, bone fares badly. As a rule, bone
involvement result in severe injury due to high energy transfer with disruption of
missile &involved bone, with generation of secondary missiles. Extensive
devitalisation of muscle is a typical finding. Devitalized muscle in the depths of the
wound provides perfect culture medium for growth of pathogenic bacteria. Nerves
&blood vessels respond unpredictably with injury, ranging from minimal bruising
to complete disruption. Within closed skull there is, in addition, a rapid _pressure
shock wave causing widespread disruption &injury at distance .Thus vital centres
at the base of the brain may be injured by a wound of the cranium

2
MANAGEMENT OF MISSILE INJURIES
MISSILE WOUNDS OF SOFT TISSUE
The full extent of injuries sustained can be detected only by complete exploration
.In limb wounds ,exploration is followed by thorough wound excision after which
,with very few exceptions ,the wound should be left open .Delay primary closure
should follow within 4-7 days after in jury
Principles of missile injury surgery
*Preserve skin.
*Divided fascia.
*Repair vessels not nerves (tendons should not perform at this initial procedure).
Remove dead tissue (4Cs"color, contractility, consistency, cap. bleeding).
*
*Stabilize bone with external fixation (immobilization).
*Clean&close joint cavities.
*Leave wounds open (antibiotics cover).
MISSILE WOUNDS OF THE ABDOMEN
Every penetrating &perforating missile wounds of the abdomen should be
explored by laparotomy.Before surgery ,a nasogastric tube should be passed into
the stomach &a urinary catheter into bladder .Bladder catheterization must be
preceded by digital rectal examination .Timing of exploration will vary. In some
cases operation will be undertaken as part of resuscitation ,in other pre operative
stabilization is possible .A full midline incisions recommended .Hemorrhage must
be controlled &careful examination is then made of all the abdominal content .
*Stomach inspects the lesser sac.
*Retroperitoneal hematoma in the region of (duodenum, colon, kidney)
*Colon (RT &Lf).
*Rectal injury.
RENAL INJURY
Renal injury best treated conservatively if this possible .Fortunately, immediate
nephrectomy is rarely indicated .A divided ureter may be brought to surface or
may be repair over a"pigtail"stent.
.
BLADDER &URETHRAL INJURIES
Bladder &urethral injuries are treated by suprapubic cystostmy with placement of
a suprapubic drain after wound excision.
LIVER INJURY
In 50%of patients with hepatic injury who survive to reach a surgical centre
bleeding has stopped ¬ a problem at laparotomy.If bleeding is still occurring,
damage control technique are particularly appropriate in a warfare setting.

3
DAMAGE TO SPLEEN & PANCREAS
Damage to the spleen &pancreatic tail may require resection, although in some
cases splenorrhaphy may be feasible. Missile injury of the head of the pancreas
&surrounding structures is usually fatal.
PERITONEAL TOILET
Using warm saline, it is important to assist the removal of all spilled bowel content
&blood clot
.
CLOSURE
The laparotomy wound is closed using mass closure technique .The missile
entrance & exit wound should be excised & left open initially with view to delay
primary closure at 4-6 days.
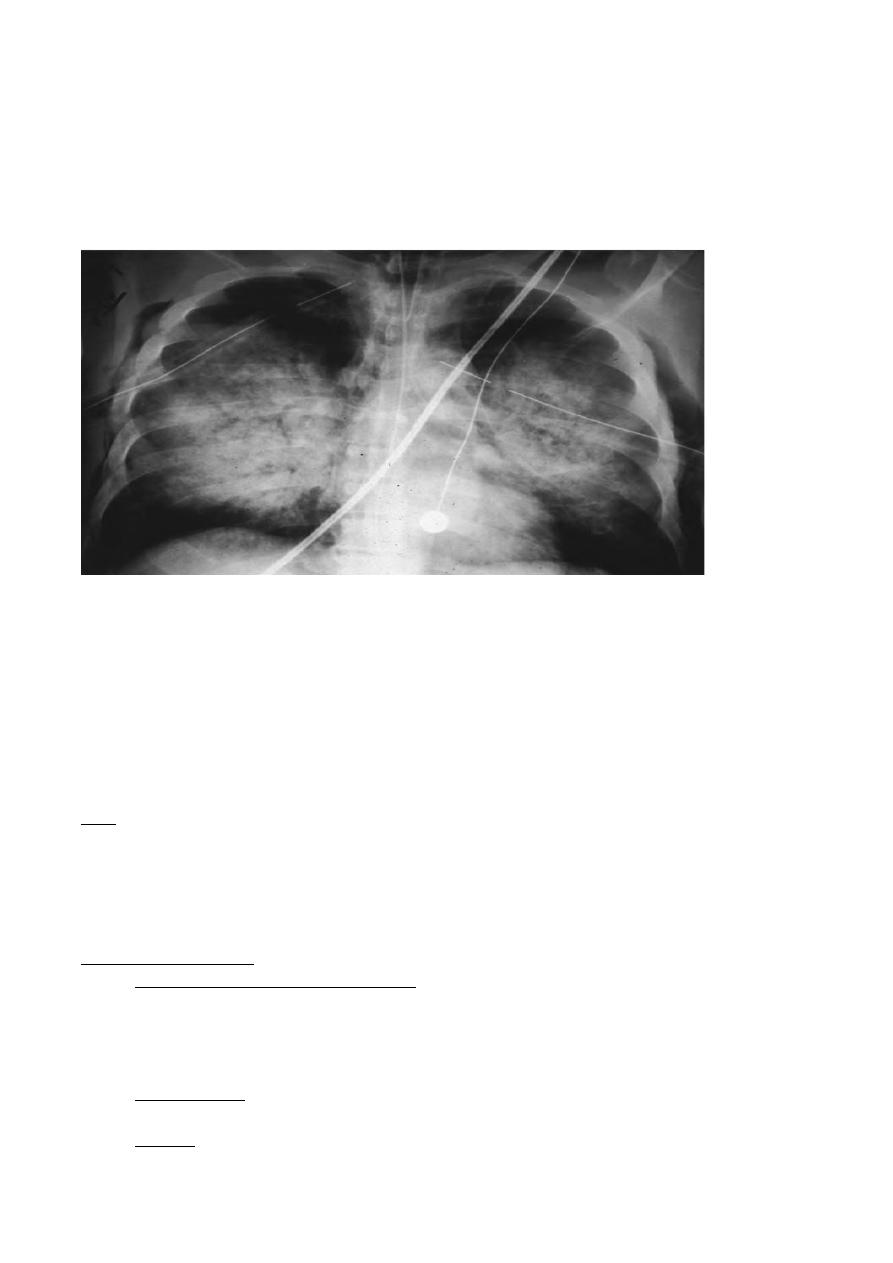
MISSILE WOUNDS OF THE CHEST
Penetrating missile wound of the chest are common in war &are associated with
high mortality if simple life _saving measures are neglected. Its important to
secure an airtight seal of open wounds of the chest to prevent a potentially fatal
open pneumothorax.This is immediately followed by tube thoracostomy"done
during primary survey".
All penetrating wounds of the chest require adequate venting of the pleura by
formal tube thoracostomy .Once pulmonary function has been stabilized missile
entry & exit wounds are excised.
*Remove any retained foreign materials.
*Arrest haemorrhage"usually from I.C. &I. mammary V.".
*Oversaw or staple hole in adjacent lung.
*Pleural opening must be sealed either by direct pleural closure or by overlying
healthy soft tissues.
*Wounds left open for subsequent delay closure.
These simple measures will suffice for more than 80%of chest wounds.
Indications for formal thoracotomy
*More than 1.5 L. initial blood loss.
*Continuing blood loss of >200 ml /hr/
*Cardiac tamponade.
*Other mediastinal injuries.
*Persistent air leak.
*Relative foreign bodies >1.5 cm.
In thoracoabdominal injuries, thoracic component is treated by tube thoracostomy
& abdominal component by laparotomy through midline incision. Formal
thoracoabdominal incision has risk contaminations of the chest cavity by faces
&should be avoided.

4
MISSILE OF THE HEAD
The penetrating high energy transfer missile wounds of the head are usually
lethal. Successful management of penetrating low energy transfer & tangential
wounds depends initially on measures such as protected air way, adequate
ventilation & maintenance of blood pressure & perfusion pressure to permit
oxygenation of the brain. Good radiographs are mandatory to localize foreign
bodies & bone fragments .CT scan images are invaluable in planning surgical
exploration .Wound excision should be carried out using gentle irrigation & suction
to remove devitalized brain & boney fragments .Every effort, including the use of
temporal is fascia or fascia lata, should be made to close overlying dura .The skin
overlying the head & face, allowing primary closure due to its excellent blood
supply.IPPV assist in the reduction of intracranial pressure by reducing brain
swelling.
SHOTGUN INJURIES
Accident from large_bore shotgun is common & often lethal when injury sustained
at close range. It's never possible to retrieve all the shot & indeed, to do so would
result in unacceptable damage to uninjured soft tissues. Wound excision should
be carried out on the major wound; particularly looking for in driven wadding &
plugs of clothing .The retention of lead shot in the body can result in a
dangerously high lead concentration, which should be monitored.
BLAST INJURIES
Terrorism is now a global phenomenon.
Both civilian, as well as military, surgeons will be exposed to patients injured in
explosion
Blast injuries in civilian populations occur asresult of
fireworks,
household explosions, or
industrial accidents.
Terrorist tactics may take the form of
letter bombs,
suitcase bombs,
vehicle bombs, and
suicide bombers.
Types of Blasts
High order explosive
• Explosion is supersonic
• Blast contains a over-pressurized wave
5
A wave where the air is compressed to a point where it can itself be dangerous
Followed by under-pressure as the air pressure drops before returning to
normal
Low order explosive
• Explosion is not as fast as the speed of sound
• No over-pressurization wave
# Blast pr. wave "known as dynamic over pr."with positive & negative phase
.
#Mass movement of air "blast wind".
* The positive pr. phase of blast wave last for only few milliseconds, but
close to explosion it may rise to over 7000KN/M.
* Blast pr. wave flow over & around an obstruction & affect anyone
sheltering behind a wall or in trench "known as incident pr.".
* Also any person standing in front of a wall or other vertical surface facing
an explosion is subjected to added effect of a reflected pr.
Negative effect of pr. wave is of low amplitude, last longer than positive pr.
& is doubtfully clinical significance.
A mass movement of air ort dynamic pr. result from the rapid expansion of
gases at the center of explosion, which displace air at suprasonic speed "
This results in injury patterns ranging from traumatic amputation to total
body disruption.
In water, velocity & distance are greater & the inj.tend to be more complex
& severe.
In water, the wave exert (water hammer) effect with significant rates of GIT
perforations.
When body is impacted by blast pr. wave, it couples into body & set upas a
series or stress waves which are capable of inj., particularly at air-fluid
interface .
This inj. to the ear, lungs, heart & to lesser extent GIT.
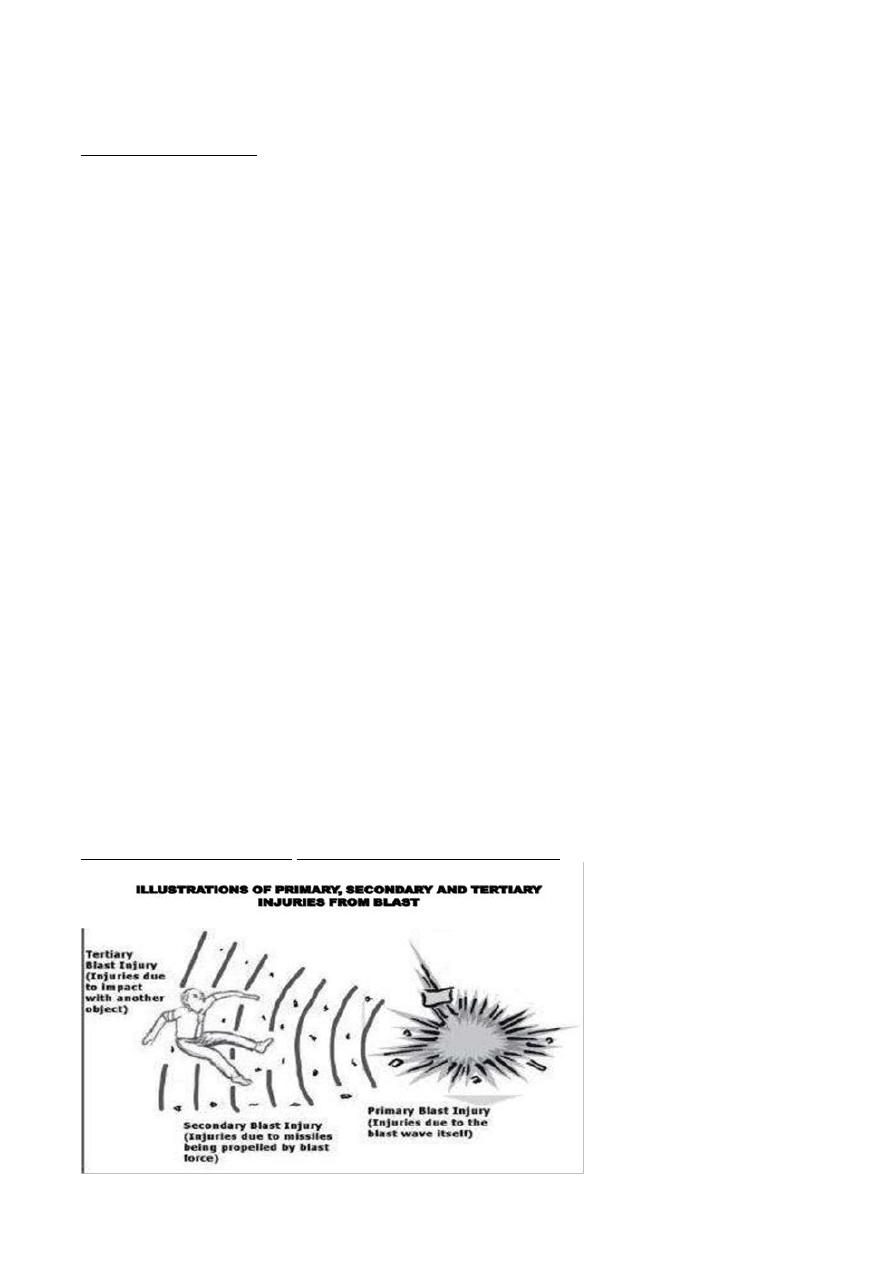
Mechanisms of injury following bombing attacks
6
Primary blast injury (PBI)
occurs as a direct effect of changes in atmospheric pressure caused by the blast
wave.
Injury to gas-containing organs such as perforation of the middle ear and BLI are
most common followed by the hollow organs of the gastrointestinal tract.
Gastrointestinal injuries may present after a delay of hours or even days. Injury
from blast overpressure is a pressure and time dependent function. By increasing
the pressure or its duration, the severity of injury will also increase.
In general, primary blast injuries are characterized by the absence of external
injuries; thus internal injuries are frequently unrecognized and their severity
underestimated.
Secondary blast injury
Secondary injuries are caused by fragmentation and other objects propelled by
the explosion.
These injuries may affect any part of the body and sometimes result in
penetrating trauma with visible bleeding.
At times the propelled object may become embedded in the body, obstructing
the loss of blood to the outside. However, there may be extensive blood loss
within the body cavities.
Fragmentation wounds may be lethal and therefore many anti-personnel bombs
are designed to generate fragments
Most casualties are caused by secondary injuries as generally a larger
geographic area is affected by this form of injury than the primary blast site as
debris can easily be propelled for hundreds to thousands of meters.
Some explosives, such as nail bombs, are deliberately designed to increase the
likelihood of secondary injuries.
In other instances, the target provides the raw material for the objects thrown
into people, e.g., shattered glass from a blasted-out window or the glass facade of
a building.
Tertiary blast injury
Displacement of air by the explosion creates a blast wind that can throw victims
against solid objects.
Injuries resulting from this type of traumatic impact are referred to as tertiary
blast injuries.
Tertiary injuries may present as some combination of blunt and penetrating
trauma, including bone fractures and coup contre-coup injuries.
Children are at a particularly higher risk of tertiary injury due to their relatively
smaller body weight.
Quaternary injuries
quaternary injuries, or other miscellaneous named injuries, are all other injuries
not included in the first three classes. These include flash burns, crush injuries,
and respiratory injuries.
7
Traumatic amputations quickly result in death, and are thus rare in survivors,
and are often accompanied by significant other injuries .
The rate of eye injury may depend on the type of blast.
Psychiatric injury, some of which may be caused by neurological damage
incurred during the blast, is the most common quaternary injury, and post-
traumatic stress disorder may affect people who are otherwise completely
uninjured.
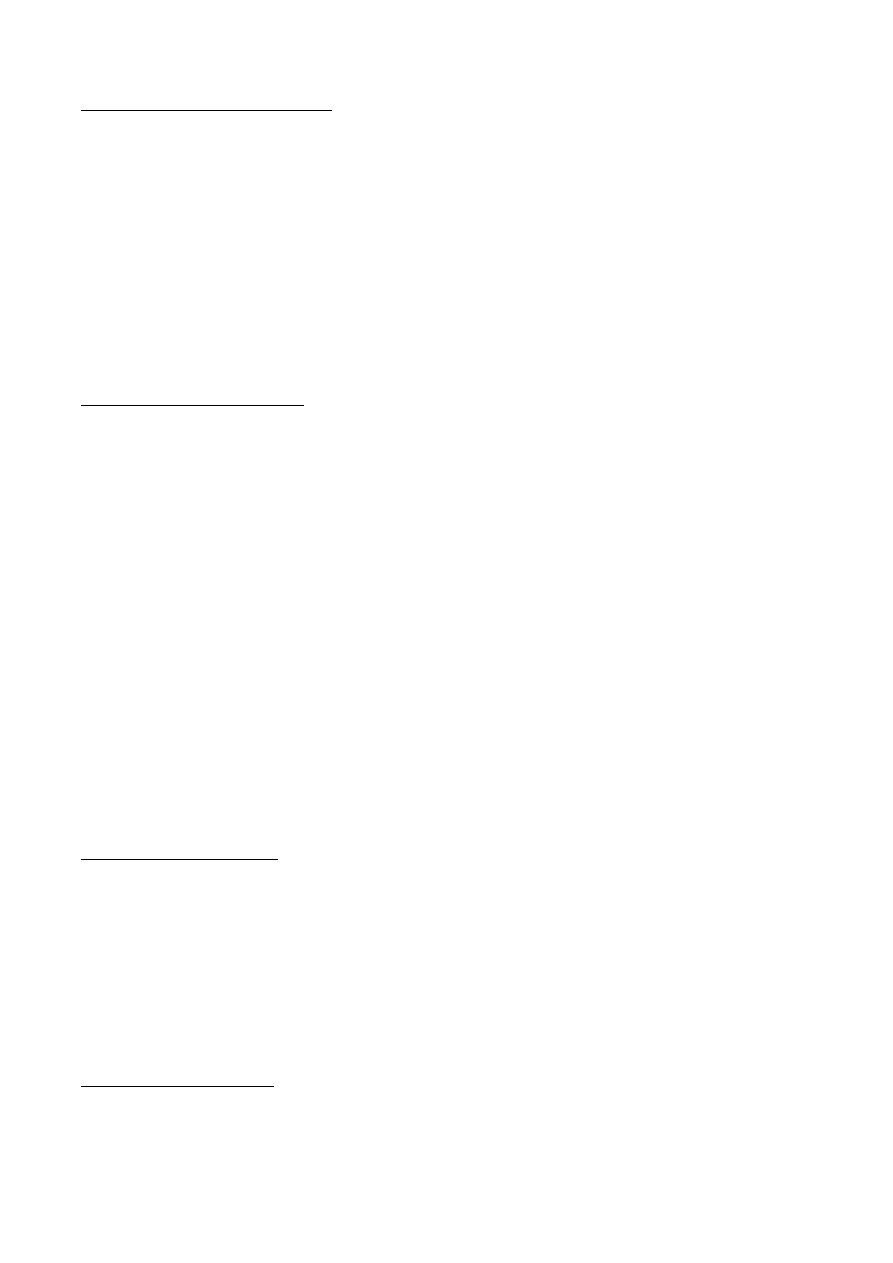
Category
Characteristics
Body Part
Affected
Types of Injuries
Primary
Results from the
impact of the over-
pressurization
wave with body
surfaces.
Gas filled
structures
lungs, GI
tract, and
middle ear.
Blast lung injury
TM rupture and
middle ear damage
Abdominal hge and
perforation
Concussion (TBI)
Secondary
Results from flying
debris and bomb
fragments
Any body
part may
be
affected.
Penetrating
blunt injuries
Eye penetration
Tertiary
Results from
individuals being
thrown by the blast
wind.
Any body
part may
be
affected
Fracture and
traumatic amputation
Closed and open brain
injury
Quaternary
All explosion-related
injuries, illnesses, or
diseases not due to
primary,secondary,
or tertiary
mechanisms
Any body
part may
be
affected
Burns
Crush injuries
Closed and open brain
injury
breathing problems
from dust, smoke, or
toxic fumes
GENERAL MANAGEMENT OF BLAST INJURIES
The structures inj. by primary blast wave in order of prevalence, are the
middle ear, lungs, & bowel.
However ,the most common urgent clinical problem in survivors is
usu.penetrating inj. caused by blast-energised debris & fragments from a
casing of exploding device .
Many of those exposed will have blunt ,blast ,& thermal inj. ,in addition to
more obvious penetrating wounds "combined inj.".
8
The deafness of the victim makes communication with them difficult &
may complicate early assessment & management.
The soft tissue wound are usu. heavily contaminated, some cases are
associated with multiple wounds of varying severity affecting a limb.
It may not always to practical to explore every wounds at first surgery. The
larger & deeper wounds should have priority of management owing to the
more serious consequences of infection.
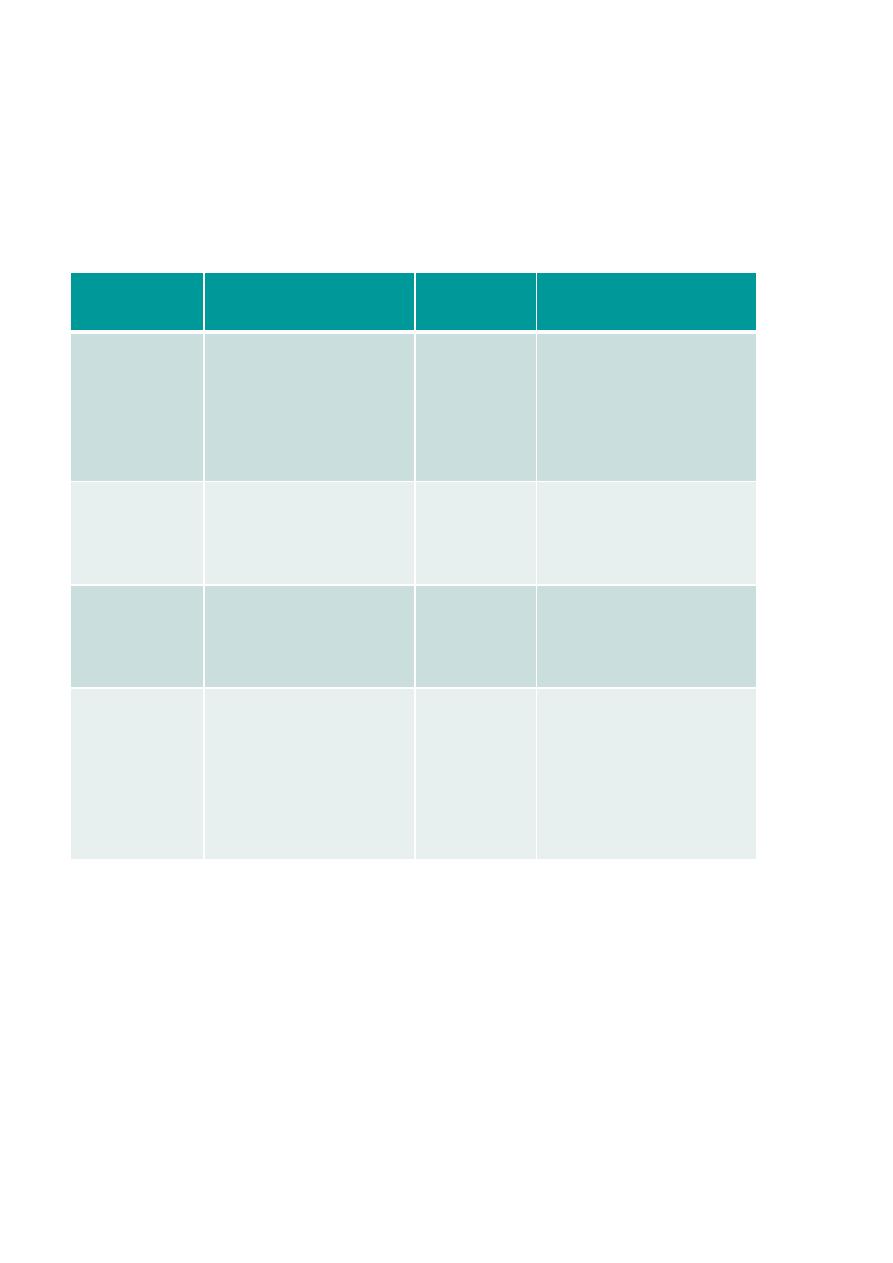
REGIONAL MANAGEMENT OF BLAST INJURIES
*Auditory system
Damage of hearing by three ways
-rupture of tympanic membrane.
-dislocation of ossicles.
-or widespread disruption of the inner ear.
Although deafness is certain indicator of exposure to significant blast
loading, its absence does not imply the absence of the blast inj.to other
systems
The ear is the most sensitive organ to blast injury, and auditory injury has
been reported in up to 41% of survivors following bombing attacks.
Immediate otoscopic examination for TM rupture should be performed by an
otolaryngologist in all cases. Treatment consists of removal of debris from the
external canal by suction under microscope and keeping the ears dry.
Respiratory system
# Primary blast wave may cause rapid inward movement of the chest wall
& result in underlying pulmonary contusion .
# Also initial blast wave couple into the chest , resulting in"stress waves "
which spread out , reflect & reinforce at tissue interface .
At air-fluid interface they may result in considerable disruption lead to cap.
leakage resulting in spreading hemorrhagic alveolar contamination.
An inflammatory cascade now ensure resulting in post blast respiratory
insufficiency "PBRI"which is virtually indistinguishable from ARDS .
PBRI varies from mild & localized area of pul.contusion to fulminating &
rapidly fatal condition involving both lungs.
9
In severe cases resp. insufficiency may further precipitated by over
transfusion with electrolyte fl.
# The clinical picture is the pat. develop cough with frothy bl. stained
sputum, dyspnea & feeling of apprehension .
# Bl. gases analysis confirm art. hypoxia & raised PCO2
# Chest radiographs in initial stages show localized contusion inj. but later the
evidence of bilat. fluffy infiltrates spreading out from the hilum of both lungs
Post blast respiratory insufficiency management
*Work within ABCDE system of the ATLAS program.
*Avoid over hydration.
*Administer high flow oxyg. with mask & re breathing bag.
*Art.bl. Analysis to asses the need for further measures.
*Resort to mechanical ventilation early to ensure adequate
ventilation.
*Corticosteroid should be avoided.
GIT
Inj.to gas-filled viscera is more common in under water explosions than in
air blast .
Perforation of stomach ,S.I., & caecum is most common .
In presence of clear physical sign urgent laparotomy is indicated .
Blast Abdomen
Delayed onset > 8-36 hours –
a. Intestinal intra-wall hemorrhages
b. Shearing of local mesenteric vessels
c. Sub-capsular and retroperitoneal hematomas,
d. Rupture of liver and spleen, and testicular rupture
Symptoms –abdominal pain, nausea, vomiting,
hematemesis (rare), rectal or testicular pain and tenesmus
Signs – abdominal tenderness, rebound, guarding, absent bowel sounds,
signs of hypovolemia
10
Management – Resect small bowel contusions > 15 mm, and large bowel
contusions > 20 mm
EYE
The eye should be examined in both primary & secondary surveys, yet inj.
is missed easily .
Conjunctival hemorrhage following blast exposure may herald a more
serious underlying problem of penetrating of globe by blast energised debris
or fragments.
Conclusions
n Terror-related blast generated by suicide
bombing attacks results injury, which is a combination of blast, penetrating
wounds, and burns.
n Victims of indoor attacks sustain more BLI and burns.
n The work-up and management of these
victims includes extensive utilization of
imaging modalities and a multi-disciplinary approach.