The Heart
DR KHALID WISSAMPathology Department
Mosul Medical college
Lec 2
CONGENITAL HEART DISEASES
Most common types of heart diseases among childrenOccur in about 1% of live births.
Etiology and pathogenesis
I. Most are developmental anomalies during gestational 3-8 weeks
II. Multiple factors account for most cases:
1. Genes involved have been identified in only a minority of conditions, trisomy 21 is the most common
2. In utero rubella and syphilitic infections of the fetus
Clinical Features
-Left to right shunt
-Right to left shunt
-Flow obstruction
Shunt : is an abnormal communication between chambers or blood vessels.
Left to right shunt
Cyanosis is no an early feature
examples:
Ventricular septal defect (VSD)
- Atrial septal defect (ASD)
- Patent ductus arteriosus (PDA)
- Atrioventricular septal defect
Ventricular septal defect (VSD)
the most common congenital cardiac anomaly at birth— Incomplete closures of the ventricular septum
— Most VSDs are single, but those in the muscular septum may be multiple.
— Approximately 50% of small muscular VSDs close spontaneously.
Atrial septal defect (ASD)
— Abnormal, fixed openings in the atrial septum— Usually asymptomatic until adulthood
Right to left shunt (cyanotic congenital heart diseases)
- Cyanosis is early,examples:
Tetralogy of Fallot .
Transposition of the great arteries .
Persistent truncus arteriosus .
Tricuspid atresia
Total anomalous pulmonary venous connection
Tetralogy of Fallot:
is the most common cause of cyanotic congenital heart disease
1) VSD
2) Subpulmonary stenosis
3) Aorta overrides the VSD
4) Right ventricular hypertrophy
— The heart is typically enlarged and is classically “boot-shaped” due to marked right ventricular Hypertrophy.
— 10% of untreated patients are alive at 20 years
RHEUMATIC FEVER
RHEUMATIC FEVER is an acute immunologically mediated multi-system inflammatory disease occur few weeks after pharyngitis caused by group A beta hemolytic streptococci.most often affects children of 5-15 years of age
Rheumatic heart disease is the cardiac manifestation of rheumatic fever. It is associated with inflammation of all parts of the heart
Chronic rheumatic carditis occurs years or even decades after acute RF
Rheumatic heart disease, acute, chronic
Pathogenesis- Hypersensitivity reaction induced by streptococci in genetically susceptible individual (3%)
- 2 Mechanisms are involved:
1 . Antibodies directed against M proteins of certain strains of streptococci cross-react with glycoprotein antigens in various tissues
2 . CD4+ T cells cross-react with host antigens and elicit cytokine-mediated inflammatory responses.
Morphology
Acute RHD
is characterized by inflammatory lesions—called Aschoff bodies —are pathognomonic for rheumatic fever ; these are collections of lymphocytes , scattered plasma cells, and plump activated macrophages called Anitschkow cells associated with zones of fibrinoid necrosis.
Chronic RHD is characterized by, organization of the acute inflammation, fibrosis, and deformity of involved valves (fish- mouth or ―buttonhole stenosis).
Aschoff bodies
fish- mouth or ―buttonhole stenosisRHEUMATIC FEVERClinical features:
- Major manifestations1. Migratory polyarthritis of large joints
2. Carditis (RHD)
3. Subcutaneous nodules
4. Erythema marginatum
5. Sydenham chorea
- Minor manifestations
• Fever
• Arthralgia
• Elevated blood levels of acute phase reactants
RHEUMATIC FEVER Diagnosis:
Established by Jones criteriaEvidence of streptococcal infection, plus
Presence of 2 major manifestations OR
one major and 2 minor manifestations
INFECTIVE ENDOCARDITIS
Characterized by:
- Microbial infection of the heart valves or the mural endocardium
- Formation of friable vegetations (thrombotic debris & organism)
- Destruction of the underlying cardiac tissues
Causes:
- Bacteria (most cases) inclduing: S. viridans, S. aureus, enterococci, HACEK group, S epidermidis
- Fungi
- Rickettsia
- Chlamydia
Classification
- Acute, occurs in previously normal heart valve, caused by highly virulent microbe (eg. S aureus).- Subacute, occurs in a previously abnormal valve, caused by low virulent microbe ( eg. S viridans).
Etiology and pathogenesis
- Predisposing cardiac conditionsRheumatic heart disease
mitral valve prolapse
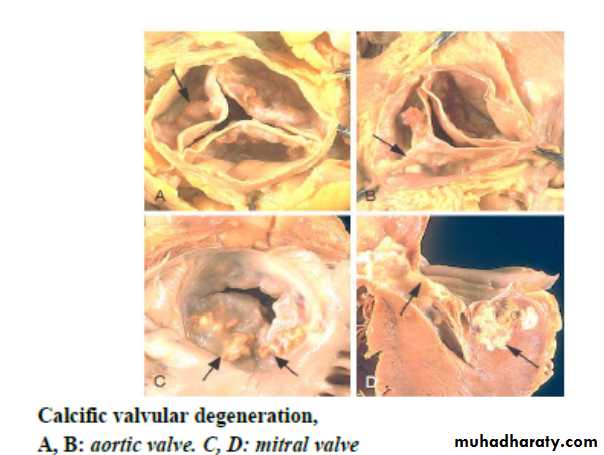
Degenerative calcific valve
Bicuspid aortic valve
Artificial valves
- Host factors
Immunodeficiency
Malignancy
Diabetes mellitus
Intravenous drug and alcohol abuse
The most important factor predisposing to endocarditis is seeding of the blood with microbes.
The mechanism or portal of entry of the agent into the bloodstream may be:
an obvious infection elsewhere,
a dental or surgical procedure that causes a transient bacteremia,
injection of contaminated material directly into the bloodstream by intravenous drug abusers,
an occult source from the gut, or oral cavity, or trivial injuries.
Morphology:
- Single or multiple friable, bulky and destructive vegetations containing inflammatory cells, fibrin, and microbes on the heart valves
- Aortic and mitral valves are most commonly involved
Infective bacterial endomcarditis
A. large friable vegetations.
B. congenitally bicuspid aortic valve with extensive cuspal destruction and ring abscess
Clinical features
- feverfatigue
- loss of weight
Murmur
Petechia in nail bed (splinter) hemorrhages, retinal hemorrhages (Roth spots), painless palm or sole erythematous lesions (Janeway lesions), or painful fingertip nodules (Osler nodes).
Complications
- Ring abscess- Systemic emboli causing septic infarcts and mycotic aneurysms
VALVULAR HEART DISEASE
Types:- Stenosis (failure of a valve to open completely)
Insufficiency (Regurgitation) (failure of a valve to close completely)
Valvular abnormalities may be congenital
or acquired, are either pure or combined.
Examples: Aortic Stenosis,Aortic Insufficiency, Mitral Valve Stenosis,Mitral Valve Insufficiency
Mitral Valve Prolapse
- Affects 3% of mostly young women
- Myxomatous change in the valve leaflets probably due to underlying genetic defect of connective tissue.
TUMORS OF THE HEART
Primary tumors:- Myxoma
- Lipoma
- Papillary fibroelastoma
- Angiosarcoma
Secondary tumors (Metastasis)
MyxomaMost common primary tumor
Benign
Mostly (90%) located in the atria as solitary sessile or pedunculated mass of 1-10cm
Histology: stellate, frequently multinucleated myxoma cells embedded in an abundant acid mucopolysaccharide ground substance
Left atrial myxoma, A large pedunculated mass in fossa ovalis and extends into the mitral valve orifice. B, Abundant amorphous extracellular matrix contains scattered multinucleate myxoma cells (arrowheads) in various groupings, including abnormal vascular formations (arrow).