
Ophthous ulcer Pharmacology 3
rd
-stage
1 |
P a g e
Treatment of ophthous ulcer or ulcerative stomatitis:-
Non-specific ulceration of unknown etiology & consist of acute painful ulcer
on the movable oral mucosa occur as single or in group , aim of our
treatment to protect the ulcer to enable their healing , relief the pain(sever)
& to reduce the inflammation .
Drugs used for such purpose:-
1-carmellose gelatin(orabase =carmellose sodium +gelatin+ pectin all as
16.58% + plastibase 30gm use after meal as thin layer ) as mechanical
protective mean .
2-triamcinolone (kenalog 0.1% use after meal as thin layer 2-4 times a day)
as oral paste to reduce the discomfort.
3-local anesthesia to relief the pain, anesthesia of pharynx before meal
may cause suffocation.
4-tetracycline mouth wash, use for multiple lesion condition & for
recurrent attach, use as 2-3 times/day for three days. To be repeated at
interval not less than 3 days to avoid development of oral thrush.
5- Prednisolone gargle (5mg in 30 ml water) used in severe cases.
6-antibiotic for secondary bacterial infection, since infection causing
discomfort & delay healing.
7-chlorhexidine mouth wash it is a useful anti-septic agent, accelerate
healing if a recurrent attach occur.
8-hydrocortisone in dose of 2-5 mg three times a day.
9-anginovage as spray[aerosol of bisdequaliium chloride 100mg +B-
glycerbitinic acid 60mg+hydrocortisone acetate 60mg +tyrothricin 400mg+
lidpcaine 100mg ]/ (10ml ).

Ophthous ulcer Pharmacology 3
rd
-stage
2 |
P a g e
10-sus it is a lozenge of liquorice dry extract 30mg +benzalkonium chloride
solution 50% used in following condition symptomatic relief of sore throat
& pharyngitis, as local treatment of mouth condition like aphthous ulcer
gingivitis & denture irritation use as one lozenge every 4-6 hours for 2-4
days , to be avoid in heart failure & renal failure , their side effects are
(sodium& water retension + hypokalemia )
…………………………………………………
Treatment of oral moniliasis (thrush) ; as creasy white patch of exudates
that can be scraped off on inflamed tongue or buccal cavity mucosa more
common in infants , elderly , malnutrition patients & in poor oral hygiene
or who use corticosteroid , immune-suppressive , antibiotic or anti-
neoplastic agents . Treated by:
1-nystatine 100000 unit/ml suspension 1 ml apply in mouth after meal four
times a day, up to 48 hours after healing.
2-amphotericin as lozenger dissolve 1 lozenge slowly in mouth four times a
day.
3-gention violate not longer recommended to be apply four times a day.
……………………………………………………
Mouth washes & gargles as for oral hygiene:-
1-chlorhexidine as mouth washer in oral infection & when tooth brushing is
not possible (corsodyl it is chlorhexidine gluconate 0.2%).
2-A.M.C. (amyl-meta-cresol 0.5%).
3-H2O2 6% as mouth washer.
4-listerine solution of ethanol 96% +benzoic acid 0.12%+eucalyptus 0.09% +
menthol 0.04%+methyl salicylic acid 0.05%+ thymol 0.06%.

Ophthous ulcer Pharmacology 3
rd
-stage
3 |
P a g e
5-phenol gargle liquefied phenol 2mg +glycerin 15 ml in 300 ml water.
6-P.T.A. gargle menthol 0.4 gm + thymol 0.4gm+ trikrameria 6ml liquefied
phenol 4ml+ glycerin 10 ml +alcohol 95% 20 ml all/ 60 ml .
7-sansilla gargle of aluminum chloride 15.3% + calcium chloride 3.4%+
menthol 0.12% (50ml).
…………………………………………………………….
ANTACID:-
The term 'peptic ulcer' refers to an ulcer in the lower oesophagus , stomach
or duodenum ,in the jejunum after surgical anastomosis to the stomach ,or
rarely in the ileum adjacent to a Meckle
'
s diverticulum
[1]
. A peptic ulcer can
be also defined as a form of ulceration which develop for a reason in the
epithelial lining surface expose to acid secretion of gastric glands
[2]
.
Management of Peptic Ulcer:
(1) General:
a- avoid coffee, smoking and drinking alcohol since all worse the
Ulcer and prevent or delay their healing.
b- Stop taking aspirin and other NSAIDs, instead use paracetamol or
the type of NSAIDs of less gastric irritation that called COX-2
inhibitor e.g. (Rofecxib).
(2) Drug therapy: drugs used in treatment of peptic ulcer can be
divided into two types:
(a) Classic drugs. (b) New eradication therapy.
(a) Classic therapy:-
This can be divided into two groups:
(1) Gastric anti-secretary drugs: which include the following:
(a)H
2
-receptor antagonist (Cimetidine, Ranitidine, Famotidine and
Nizatidine). This group of drug is capable of 90 % reduction in the basal
(fasting), food stimulation and nocturnal secretion of gastric acid after single
dose .This inhibit gastric secretion elicited by histamine and other H
2
agonist
in a dose dependent (inhibition parallel to the plasma concentration of drug),
it also inhibits acid secretion elicited by gastrin and to less extend that by
muscarinic agonist. The H
2
receptor antagonists reduce both the volume and

Ophthous ulcer Pharmacology 3
rd
-stage
4 |
P a g e
hydrogen ions concentration of the gastric juice. The dosage is as following:
cimetidine 400 – 600 mg twice daily or 800 mg at bed time , ranitidine 150
mg twice daily or 300 mg at bed time , famotidine 20 mg twice daily or 40
mg at bed time and to prevent the recurrence half of the dose given at bed
time . Duodenal ulcer usually heal within 4-8 weeks of treatment, in 50 % of
the patient the ulcer re-occur within a year after successful treatment which
can be reduced by giving the patient maintenance dose (half daily dose at
bed time) to 20 %. The gastric ulcer (benign) heals with 8 weeks of the
treatment in (50 -75) % of the patients and up to 16 weeks of treatment gives
high rate of healing. H
2
antagonist drugs are hydrophilic so they reach the
CNS to limited extent while the new drug like zolinidine is lipophilic (this
drug under study)
.
Adverse Effect: The longest clinical experience with the cimetidine which
may cause.
(1) Confusion state in elderly patients.
(2) On high dose cause reversible gyaencomastia in men (which is due to
blockage of androgen receptor, rarely caused by ranitidine or famotidine
(3) Dose dependent elevation of serum prolactin and may alter estrogen
metabolism in men.
(4) Headache in 34 % of the patients taking famotidine.
(5) Cimetidine slows the hepatic microsomal metabolism of some drugs like
(warfarin, theophylline, diazepam and phenytoin) while ranitidine is of
less effect. Famotidine and nizatidine of no effect on the hepatic
metabolism of drugs.
(b) Muscarinic antagonist: This group includes (pirenzepine and
telenzepine) both are less effective than H
2
receptor antagonist since they
can reduce basal (fasting) gastric secretion in (40–50) % and stimulated
secretion is inhibited to a less extent. Both are selective M
1
antagonist
with lower affinity to M
2
and M
3
receptors although they may also inhibit
the secretion of gastrin, mucus and HCO
3
and produce comparable rate of
healing of both gastric ulcer and duodenal ulcer. On a maintenance dose
they prevent the recurrence of ulcer in equivalent with cimetidine.
Pirenzepine is used as 50 mg 2-3 times daily while telenzepine is more
potent and effective in dose of 3 mg per day 30 minutes before meal for
4-6 weeks and up to 3 months in resistant case .Their adverse effects

Ophthous ulcer Pharmacology 3
rd
-stage
5 |
P a g e
include (dry mouth, blurred, vision, constipation, mental confusion and
headache.
(c)Proton pump inhibitors (PPI): The members of this class include
(omeprazole and lansoprazole) these are the classic ones while the new
drug include the (rabeprazole and pantoprazole). They irreversibly inhibit
the gastric parietal cells proton pump (H/K ATPase). They need acid
environment of secretary canaliculus of the parietal cells for activation
(pro-drug). These agents offer a mean to inhibit acid secretion to any
desired level and they are useful for patients with hypergastrinemia. At
neutral pH PPI are stable, lipid soluble weak bases, they reach the parietal
cells through blood and diffuse into the secretary canaliculi where they
are protonated into sulfenic acid and sulfonamide .The sulfonamide
interacts covalently with the sulfhydryl group at critical site in the extra-
cellular (luminal) domain of the membrane spanning H-K ATPase. Full
inhibition occurs with two molecules of inhibitor per molecule of the
enzyme. Lansoprazole is available either as 15 mg or 30 mg to be given
in similar pattern to omeprazole. Pantaprazole is available as 40 mg to be
given either as single dose or twice daily. Rabeprazole which appear to
be a well tolerated PPI with a rapid onset of action and a low potential for
drug interaction, is prepared as 10 mg or 20 mg, both can be given as
single or twice daily.
The adverse effect : using of 60- 360 mg of proton pump inhibitors per a
day up to 6 years does not cause any serious side effect, only 1.5-3 % of
patients of suffer from nausea, diarrhea, abdominal colic and central nervous
system effect (headache , somnolence and dizziness) , skin rash are
occasionally observed .
(d)Octreotide: It is a long acting synthetic somatostatin analog, it has been
found to inhibit the secretion of several circulating peptide hormones and to
inhibit the secretion of gastric acid and pancreas .The limitation of its use in
treatment of gastrointestinal tract disease is due to its requirement of
parenteral administration, but its effectiveness will further stimulate the
search to prepare orally active somatostatin analog.
(2) Mucosal protective agents:
(a)Sucralfate: It is a basic aluminum salt of sulphated sucrose .Its mode of
action:

Ophthous ulcer Pharmacology 3
rd
-stage
6 |
P a g e
(1) It is viscous at acid pH below 4 form a paste that selectively adhere to the
ulcer base and acts as a barrier to the diffusion of acid, pepsin and bile
salt.
(2) It forms a complex with the protein at the ulcer surface which resist the
peptic hydrolysis.
(3) It appears to bind and inactivate pepsin and bile salt.
(4) It may stimulate the endogenous prostaglandin synthesis.
Sucralfate cannot be given simultaneously with antacid , H
2
antagonist
or proton pump inhibitors since it requires acid pH to be activated .The
adherent gel to the ulcerated surface epithelium continues for more than 6
hours . It adhere to the duodenal ulcer more than to the gastric ulcer. Their
dosage 1g four times daily one hour before meal for 4-8 weeks. The
maintenance dose 1g twice daily. It seems to be more efficacious in
duodenal ulcer than gastric ulcer .The adverse effect includes constipation in
about 2% of the cases, dry mouth in < 1% of the cases and skin rash.
(b)Colloidal bismuth compounds: It acts to:
(1) Coat the ulcer with selective chelating with the protein material in the
ulcer surface and protect it from the action of acid, pepsin and bile
.
(2) Stimulate the secretion of the HCO
3
.
(3) Inhibit pepsin activity.
(4) Stimulate the mucus production.
(5) Increase the prostaglandin synthesis.
(6) It may have some anti-microbial activity against H. pylori.
Bismuth chelate promotes healing of both gastric ulcer and duodenal
ulcer. The bismuth may adhere to the food particles rather than ulcer base so
food should be avoided 2 hours before and 30 min after each dose. The dose :
elixir 10 ml twice daily 30 min before breakfast and evening or 5ml four
times daily 30 min before each meal and 2 hours after the last meal for 28
days can be followed by another 28 days if necessary . Maintenance is not
recommended but drug course can be repeated after an interval of 4 weeks.
As tablets 2 x 2 or 1 x 4 swallow with water for 28 days. The adverse effects
include:
1- Black color of oral cavity and feces.
2- Ataxia, encephalopathy and osteodystrophy. All possible with excessive
over dose or ingestion.
Ophthous ulcer Pharmacology 3
rd
-stage
7 |
P a g e
5- Reduce the bio-availability of tetracycline, constipation and should be
avoided in patient with sever renal dysfunction.
(c)Carbenoxolone (it was used since 1962):
It is a synthetic derivative of glycyrrhizic acid, it is found to be effective
in healing of both gastric and duodenal ulcer.
Its mode of action is by increase the amount and quality of mucus which
protect the ulcer from the acid and pepsin, this mechanism is not clear and
may be due to:
1- Lipophilic property of the drug.
2- Stimulate gastric glycoprotein synthesis.
3- Its capacity to inhibit pepsin activity.
The adverse effect : steroid cogener has a major aldosterone like side
effect so that the hypertension, fluid retention and hypokalemia limit its use,
to abolish this effect only thiazids can be used (spironolactone should not be
use since it abolishs both the side effect and ulcer healing effect.
(3) Agent with both anti-secretary and mucosal protective effecs
(a)Prostaglandin analog (Misoprostol):
This is a derivative of archidonic acid, Misoprostol is a methyl-l-analog
of prostaglandin (E1) used to prevent ulcer induced by NSAIDs.
The mode of action:
1-stimulate secretion of mucus and HCO3
.
2-Inhibit the secretion of gastric acid which is mediated by inhibition of
histamine stimulation of CAMP production, CAMP is the major second
messenger for histamine induced acid secretion. It is moderately effective in
the treatment of gastric ulcer and duodenal ulcer. The dosage is 200
microgram four times daily with food to produce inhibition of gastric
secretion of acid and in higher dose than that need to increase mucus and
HCO
3
secretion. The adverse effect:
1- Dose dependent diarrhea in 30 % of the patients.
2- Because of its stimulation to the uterus it should not be used in pregnant
woman and in child bearing one since it causes abortion.
(b)ANTACID
It is an agents that used to neutralize secretion & over acid secretion of
stomach by interaction with the acid to produce salt + water.
Ophthous ulcer Pharmacology 3
rd
-stage
8 |
P a g e
The mode of action include:-
1-Gastric acid (HCL) + weak base of antacid → salt + H2O so it will result in a
reduction in gastric acidity & inactivate pepsin (not act at pH less than 4).
2-Mucosal protection by stimulation of PG synthesis or binding of
unidentified injurious substances.
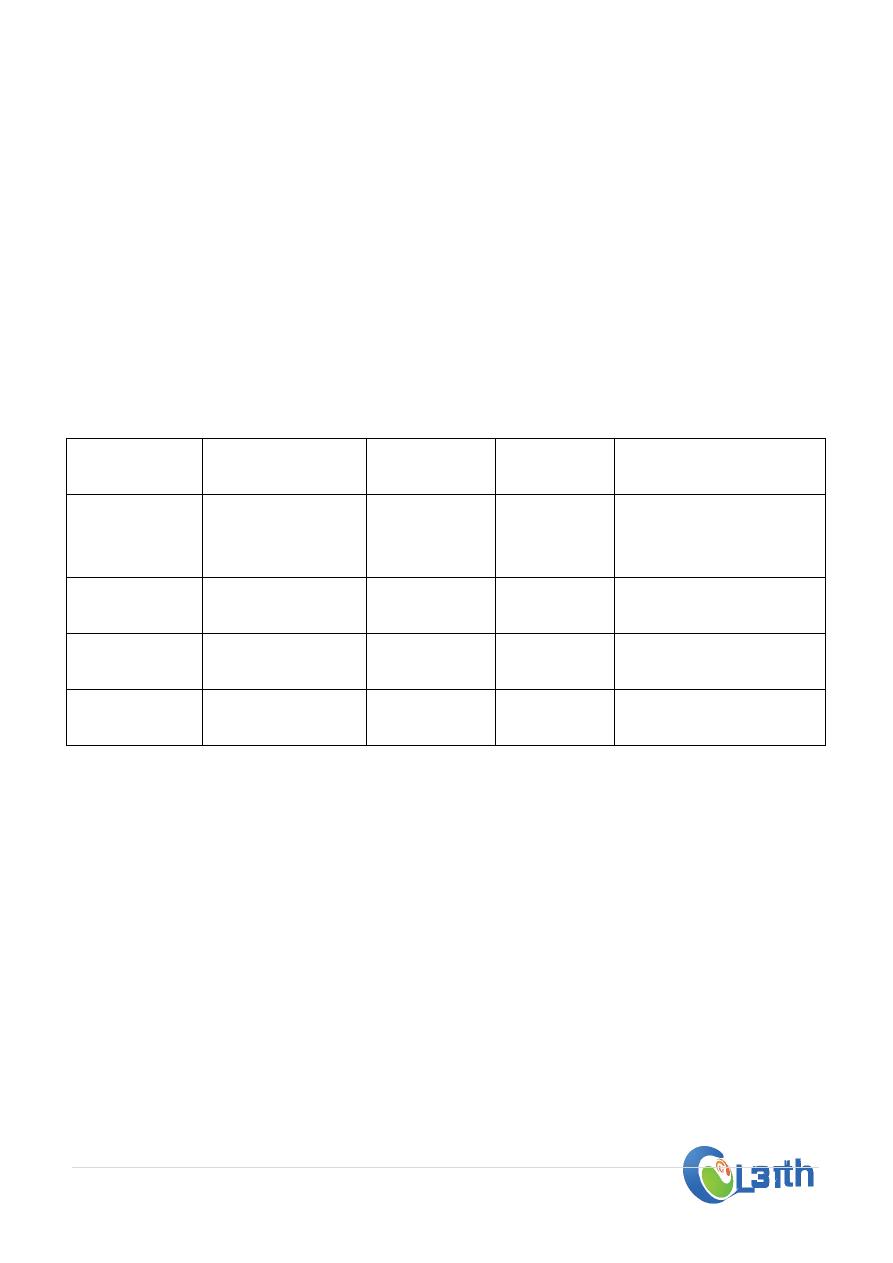
--- most of antacid consist of Mg(OH)2 , Al(OH)3 to be use alone or in
combination with each other , occasionally antacid consist of NaHCO3 or Ca
+2 salts .
Constituent Neutralizing
capacity
Salt form
in stomach
Salt
solubility
Adverse effects
NaHCO3
High
NaCl
High
Systemic
alkalosis+
fluid
retention
CaCO3
Moderate
CaCl2
Moderate Hyper-Ca
+2&
nephrolithiasis
Al(OH)3
High
AlCl3
Low
Constipation&
hypophosphatemia
Mg(OH)2
High
MgCl2
low
Diarrhea & hyper-
Mg+2
---Clinical uses include peptic ulcer, esophageal reflux &pathological hyper-
secretary state (zollinger Ellison syndrome).
---clinical dose after meal in one hour as single dose of 156 meq of
antacid(when acid production at average of 45meq/hour) this will
neutralize gastric acid for 2 houirs , if a second dose give after 3 hours of
meal this will keep a maintenance state of effect for 4 hours .
--- Their effects depend on
1- Rate of emptying antacid from stomach.
2- Gastric secretary capacity.

Ophthous ulcer Pharmacology 3
rd
-stage
9 |
P a g e
--- Not cause a healing of gastric ulcer, but heal duodenal ulcer in a dose of
140 meq 1& 3 tours after each meal & at bedtime.
(b) New H. pylori eradication therapy:
The eradication treatment of H. pylori is not only improve ulcer healing
and make the patient free of symptoms, but also reduces the possibility of
recurrence. The eradication therapy (triple and quadruple) include the
combination of two or three antibiotics plus acid suppressor or gastric
protector. The antibiotics regimens recommended for the patients may differ
across the world because of the possibility of H. pylori resistance to the
antibiotics. The most proven effective treatment is a 2 weeks course of
treatment called triple therapy that involve 2 antibiotic plus either acid
suppressor or stomach lining shield, this may:
1- Reduce the ulcer symptoms even abolish them.
2- Kill the bacteria.
3- Prevent the ulcer recurrence in more than 90 % of patients.
The patients may find the triple therapy complicated, because it involves
taking more as many as 20 pills per-day. The antibiotic that is used in such a
therapy may cause mild side effects such as (nausea , vomiting , diarrhea ,
black stool , metallic taste in the mouth , dizziness headache and yeast
infection in woman, most of these disappear on withdrawal of the
drugs) .Recent studies show that 2 weeks of the triple therapy is ideal . Early
results of the studies suggest that 1week of triple therapy may be as effective
as 2 weeks therapy with fewer side effects .The dual therapy (using of one
antibiotic plus acid suppressor or gastric protector is not effective as triple
therapy.