Lecture 14 pathology gall bladder 3
rd
Stage
1
Cholelithiasis (gall stones)
Affect 10-20% of population in developed countries. It's the most common
disease of gall bladder & bile ducts . > 80 % of gall stones are silent in that
most patients remain free of biliary pain or stone complications .
There are 2 main types of gall stones:
80% are cholesterol stones, 20% are pigmented stones according to major
constituents of each.
Risk factors
Cholesterol stones (Europe, north & south America)
Advanced age
Female gender
Oral contraceptives
Pregnancy
Obesity
Bile stasis
Hyperlipidemia syndromes
Pigmented stones (Asian more than Western, rural more than urban)
Chronic hemolytic anemias
Biliary tract infections
Lecture 14 pathology gall bladder 3
rd
Stage
2
Pathogenesis
Cholesterol is water insoluble & converted to water soluble by combination
with bile salts, when cholesterol concentration exceed the solubilization
capacity of bile (supersaturated) cholesterol becomes nucleated into solid
cholesterol monohydrate crystals. 3 important conditions for stone
formations
supersaturated bile with cholesterol .
cholesterol crystals remain in bile for long time .
presence of calcium salts to serve as nucleation sites for cholesterol stones.
bile stasis is important for stone formation .
the presence of unconjugated bilirubin in the biliary tree increase
the possibility of pigmented stones formation (as occur in hemolytic anemias).
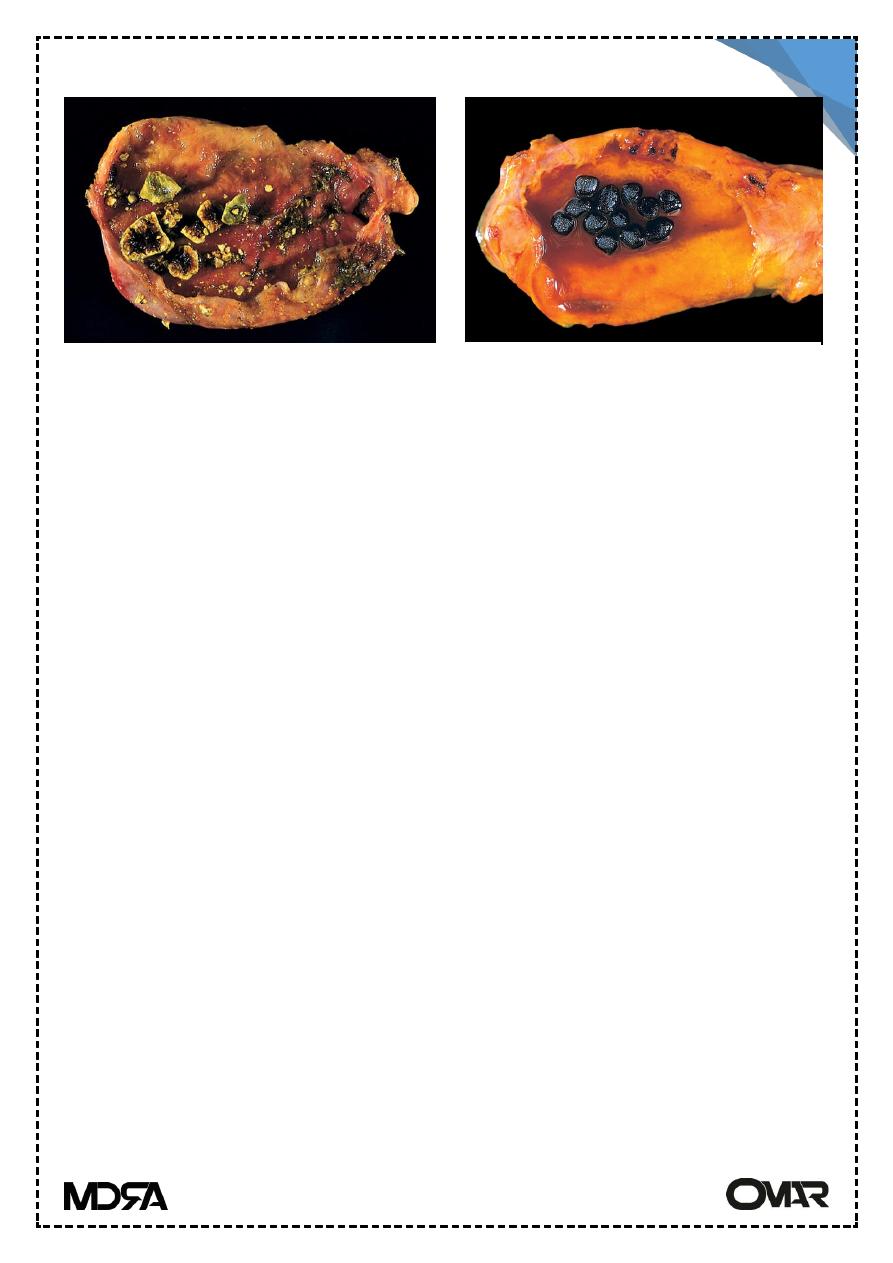
Morphology & composition
Cholesterol stones consist of cholesterol, they are pale yellow if they are
pure cholesterol stone. With increasing proportions of calcium carbonate
become grey-black colored, most are radiolucent, up to 20% radioopaque
(containing calcium carbonate) they are ovoid, multiple or single , faceted
surfaces.
Pigmented stones arise any where in the biliary tree (classified
into black & brown) .
Cholesterol gallstones
Pigmented gallstones
Lecture 14 pathology gall bladder 3
rd
Stage
3
Black stones arise in sterile gall bladder, they are small & crumbled easily
most are radioopaque & brown stones arise in infected extra or intrahepatic
bile ducts are radiolucent They are soft in consistency.
Complications
70% of gall stones remain clinically silent, the main clinical complication is
obstruction of the cystic duct or common bile duct by a stone.
Acute Cholecystitis
Acute calculous cholecystitis
Acute inflammation of the gall bladder that contain stones precipitated
by obstruction of the gall bladder neck or cystic duct. It's the most common
reason for emergency cholecystectomy. It result from chemical irritation &
inflammation of the gall bladder wall induced by obstructed bile out flow.
With distension of increased intraluminal pressure which decrease the blood
supply to the mucosa. Bacterial infection occur only later.
Acute acalculous cholecystitis:
12% of cholecystectomies contain no gall stones, mostly occur in :
postoperative, after major surgery
severe trauma
severe burns
sepsis
postpartum state
Factors enhance acalculous cholecystitis including: dehydration , gall bladder
stasis, ischemia & bacterial contamination
Chronic cholecystitis
Is the result of repeated bouts of acute cholecystitis, but may develop with
out acute attacks. It's almost always associated with gall stones.
Supersaturation of bile predispose to chronic inflammation chronic
Lecture 14 pathology gall bladder 3
rd
Stage
4
calculous cholecystitis are the same as the acute form (right upper quadrant
pain)
Morphology
Gall bladder may be contracted, or of normal size or enlarged with presence
of stones, mucosal ulcerations are infrequent, submucosa & serosa are
thickened due to fibrosis.
Microscopically : muscular hypertrophy, submucosal fibrosis & chronic
inflammation, out pouches of the mucosa into the wall form small cystic
spaces termed Rokitansky Aschoff-Sinuses.
Secondary changes include extensive calcification of gall bladder wall
(porcelain gall bladder) & development of mucocele of gall bladder.
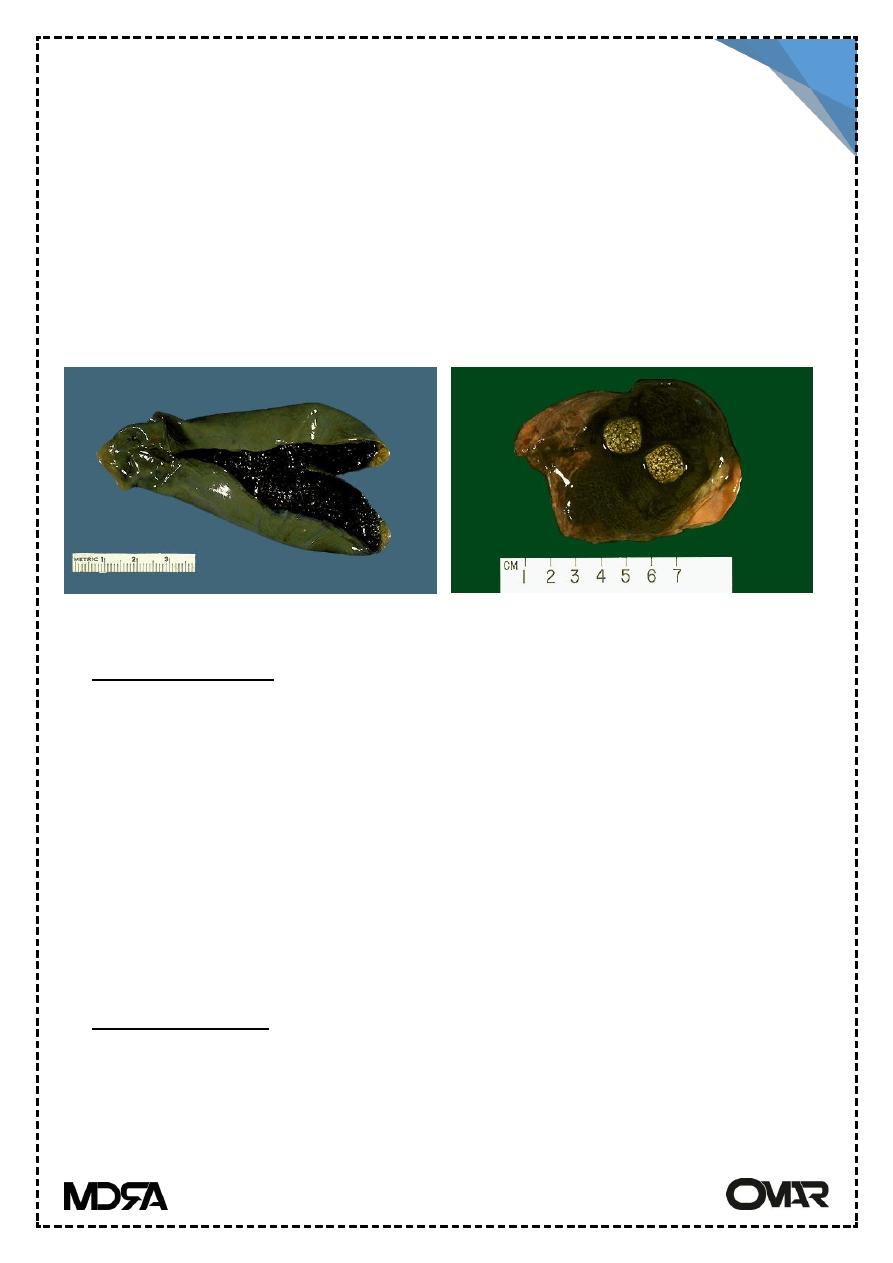
Carcinoma of the gall bladder
It's the fifth most common cancer of the digestive tract, it is slightly more
common in women & most frequently occur in the 7th decade. 60-90% of
cases containing stones. Probably gall bladder containing stones or
infectious agent develop cancer as a result of recurrent trauma & chronic
inflammation.
Morphology
Either infiltrating or fungating patterns or growth.In infiltrating type , poorly
defined area of diffuse thickening of the gall bladder, with scirrhous
consistency. In fungating growth, irregular cauliflower mass growing into the
lumen.
Microscopically most carcinomas of the gall bladder are moderately
differentiated adenocarcinomas
Prognosis : poor, 5 year survival rate 1%.
Spread: via lymphatics, direct invasion of adjacent organs(mainly the liver).