Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
1
Cardiovascular system
Diagnostic imaging modalities:
1.
Echocardiography.
2.
Radionuclide examination
.
3.
Plain radiographs
are useful for looking at the effects of cardiac disease
on the lungs and pleural cavities, but provide only limited information
about the heart itself.
4.
MRI .
5.
Fast CT scanner.
6.
Cardiac catheterization and angiography.
Plain radiography
-The standard film for evaluation of cardiac disease are erect PA & Lateral chest films.
-
Viewing points :
- heart size & shape
- pulmonary vasculature
- lung fields
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
2
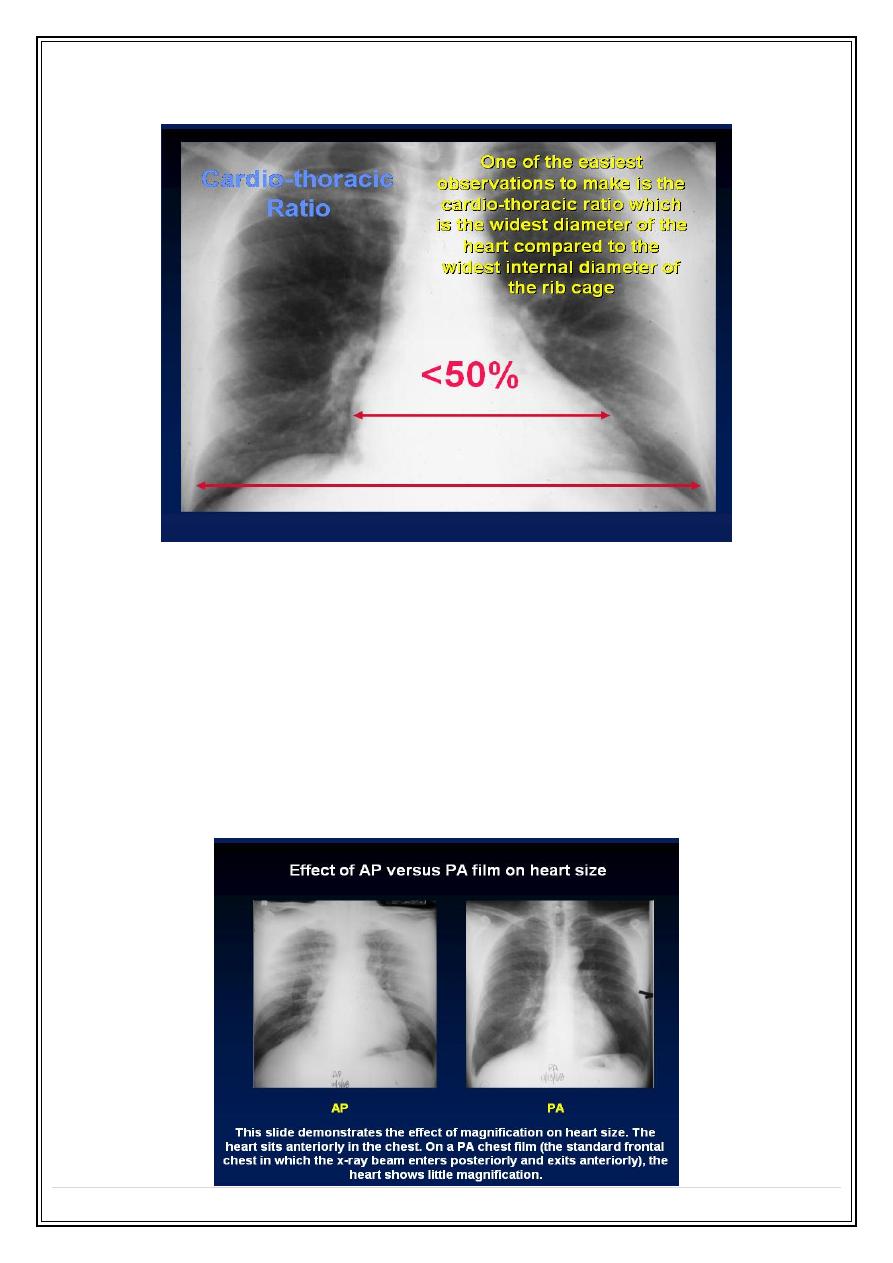
1. Recognizing Cardiomegaly
In most normal people the cardio-thoracic ratio is less than 50%.
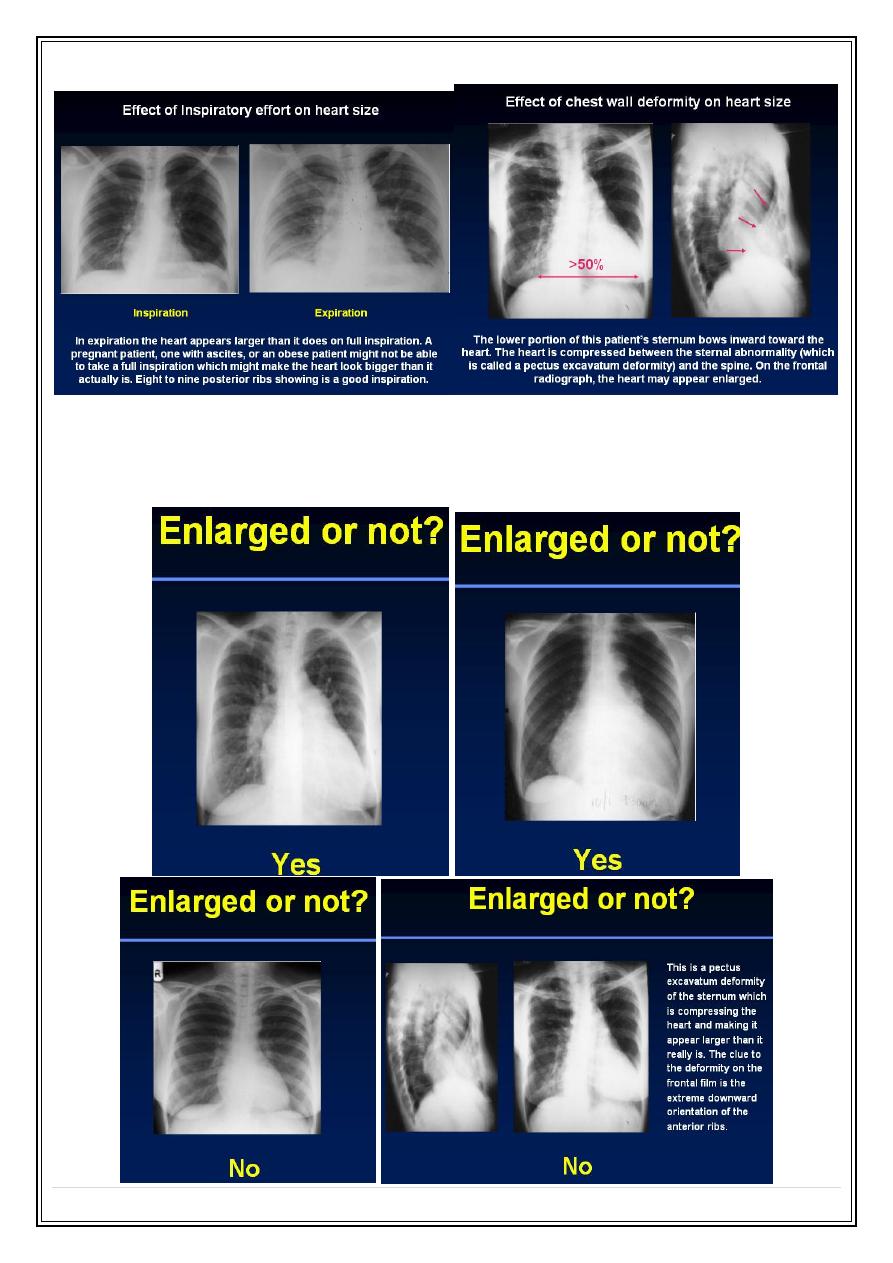
Sometimes, the cardiothoracic ratio is >50% but the heart is still normal. These are the
causes:
•
Extracardiac causes of cardiac enlargement:
o
Portable AP Films
o
Obesity
o
Pregnant
o
Ascites
o
Straight back syndrome
o
Pectus excavatum
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
3
Cardiomegaly and the AP Film
•
How can you tell if the heart is enlarged on an AP (usually portable) film?
o
If the heart touches the lateral chest wall, it's enlarged
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
4
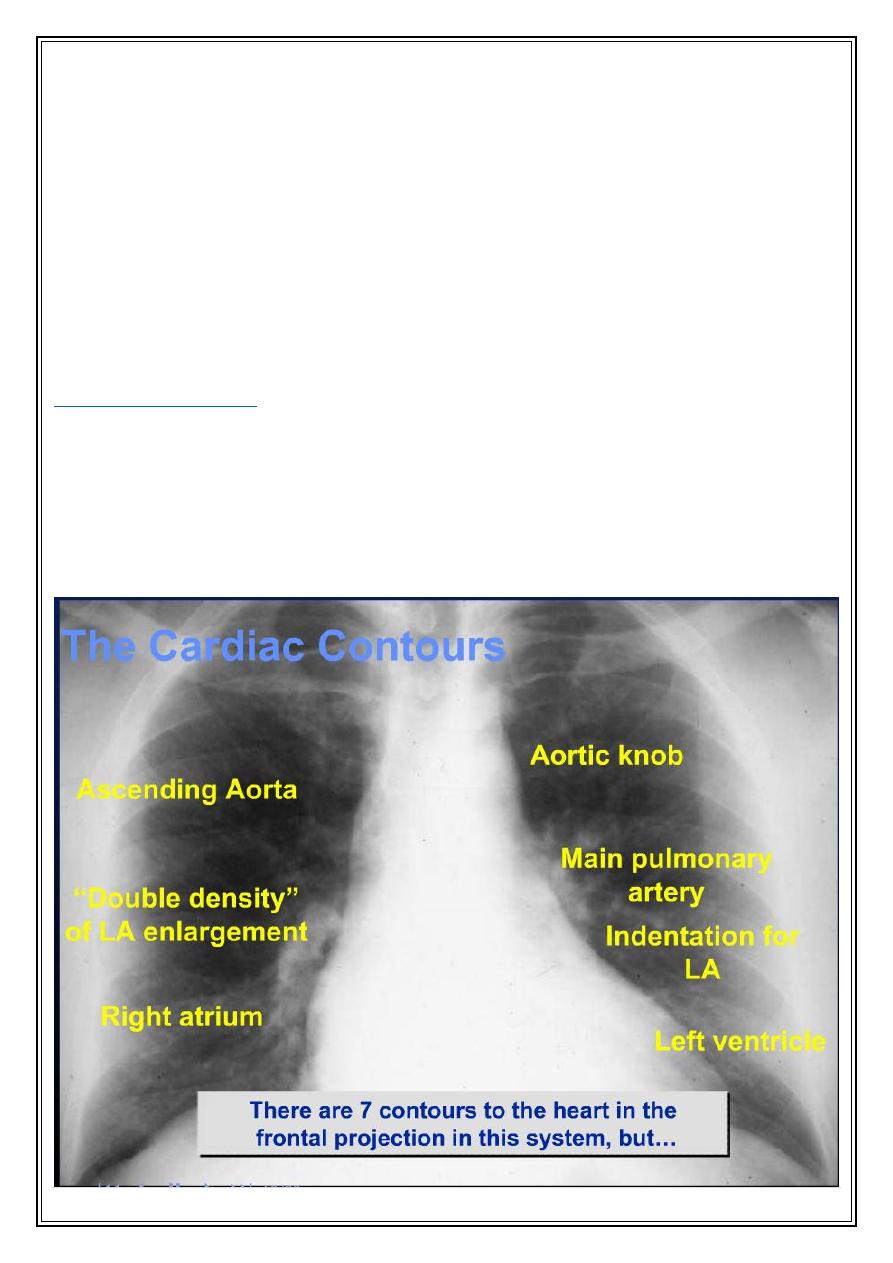
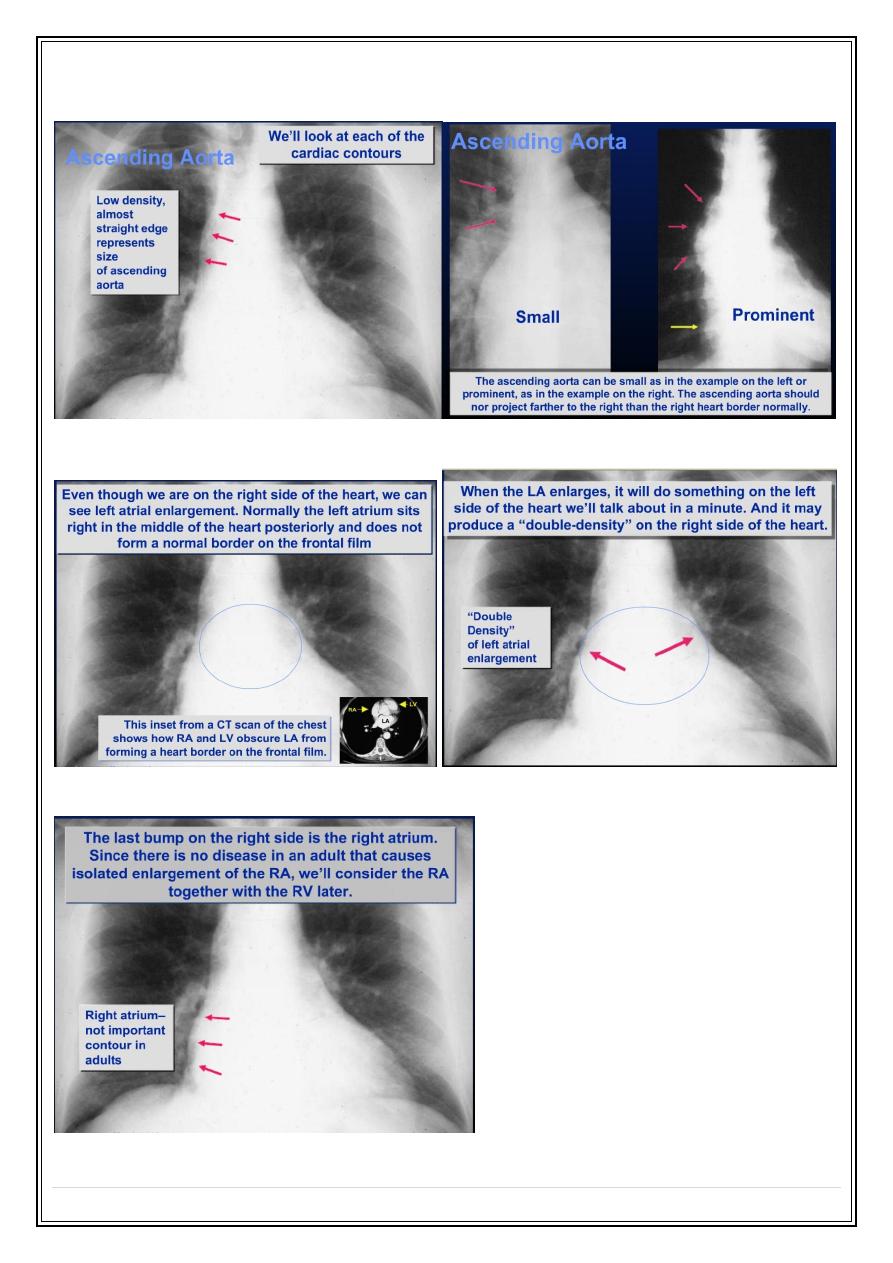
Ascending Aorta
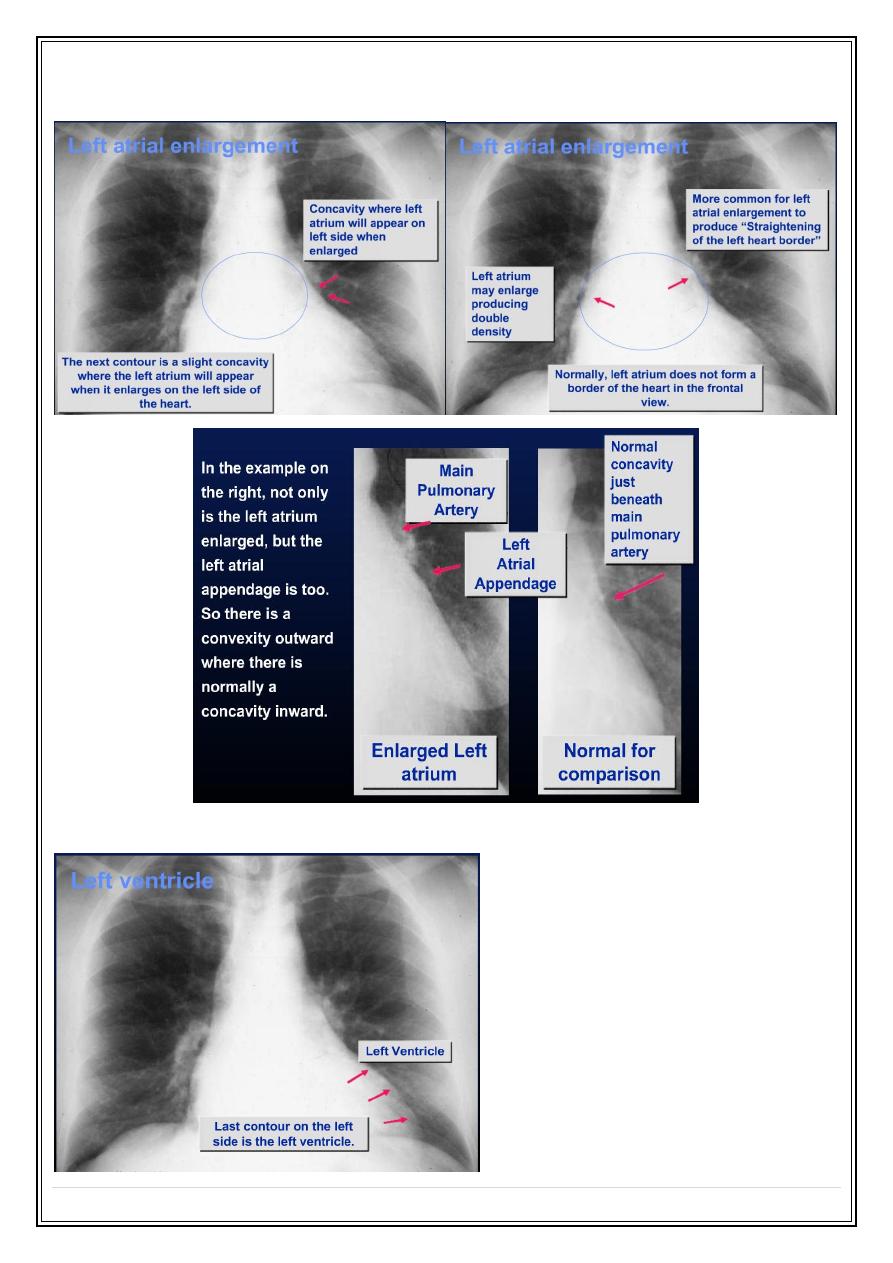
Left atrium
Right atrium
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
5
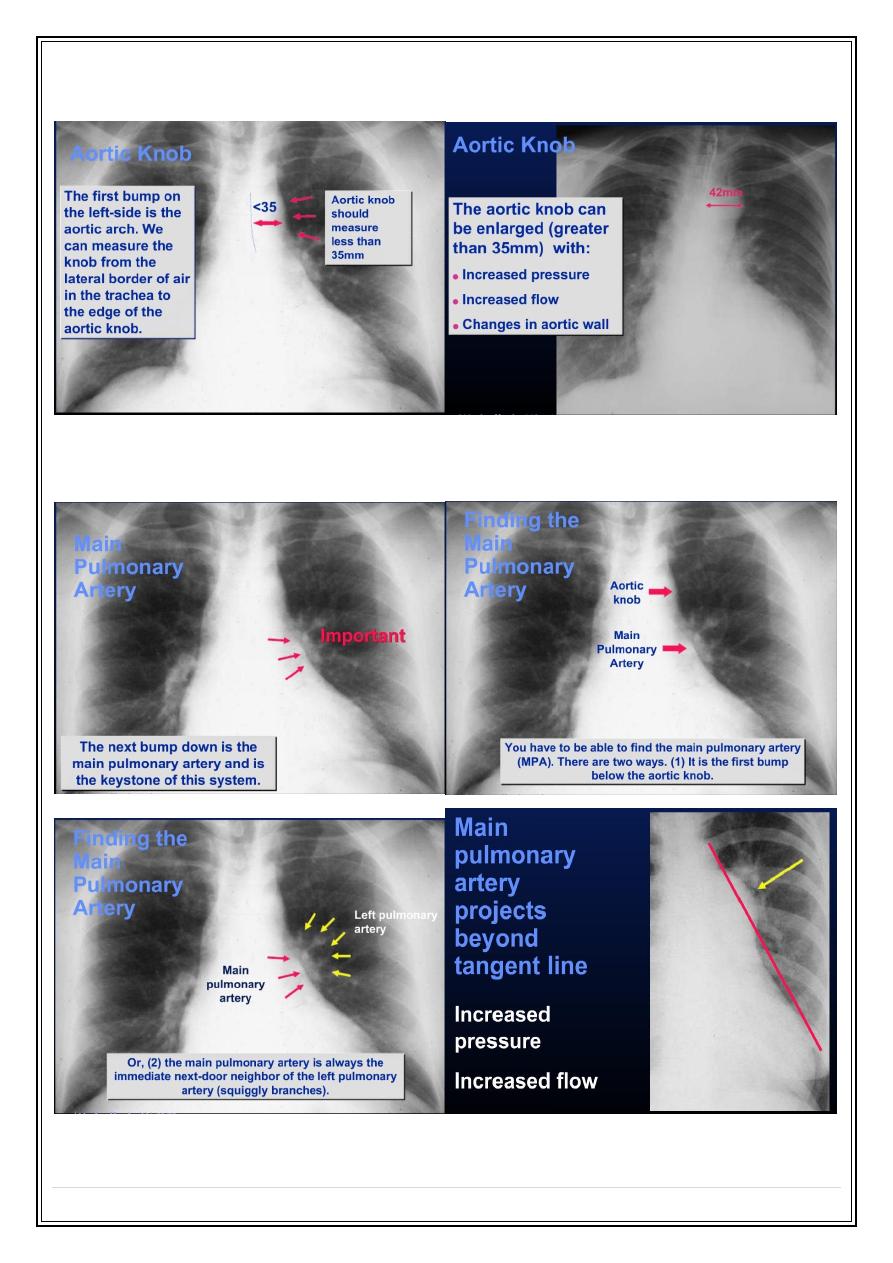
Aortic knob
Main pulmonary artery
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
6
Lt atrial appendage
Lt ventricle
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
7
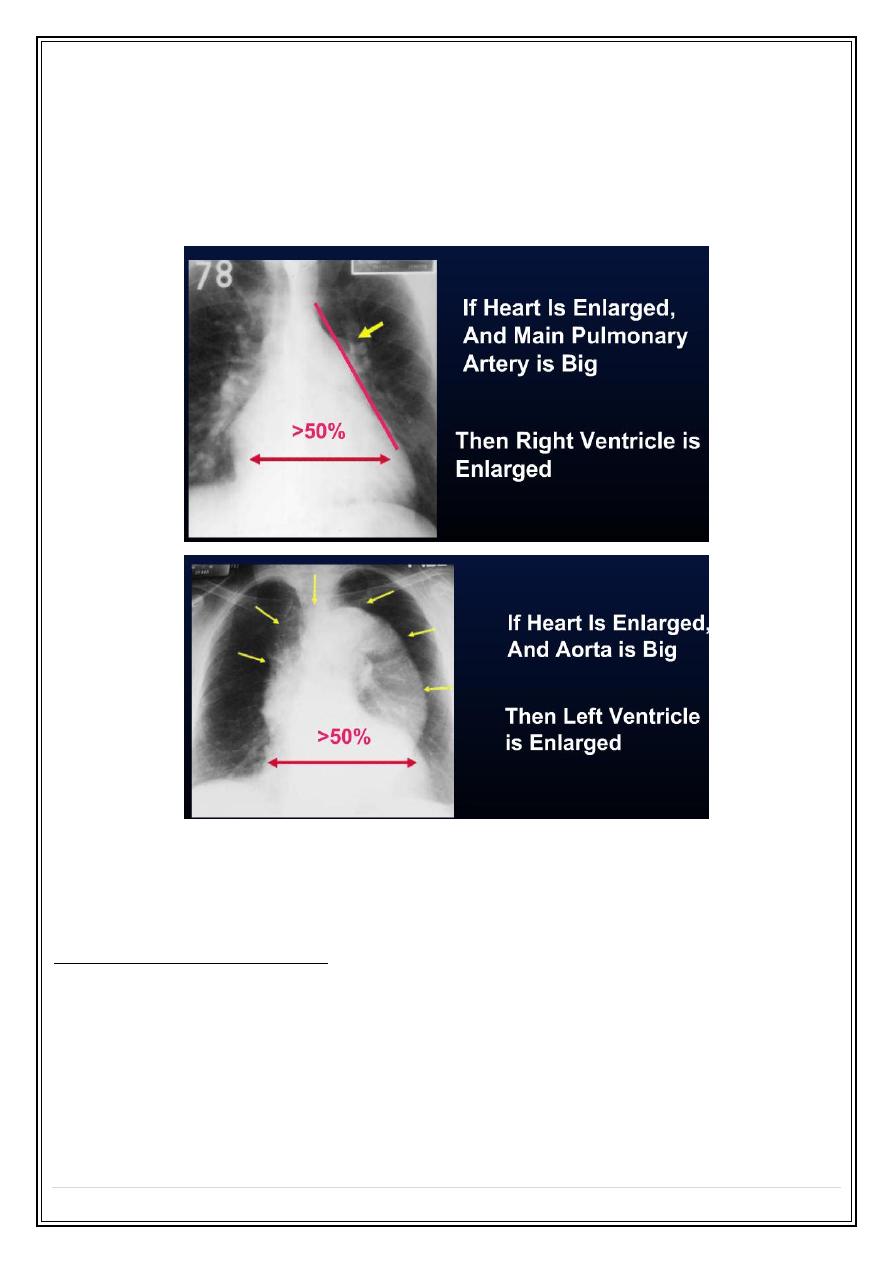
Which Ventricle is Enlarged ?
The best way to determine which ventricle is enlarged is to look at the corresponding
outflow tract for each ventricle
•
Aorta for the LV
•
MPA for the RV
Once one ventricle is enlarged, it's impossible to tell if other ventricle is also enlarged by
chest x-ray
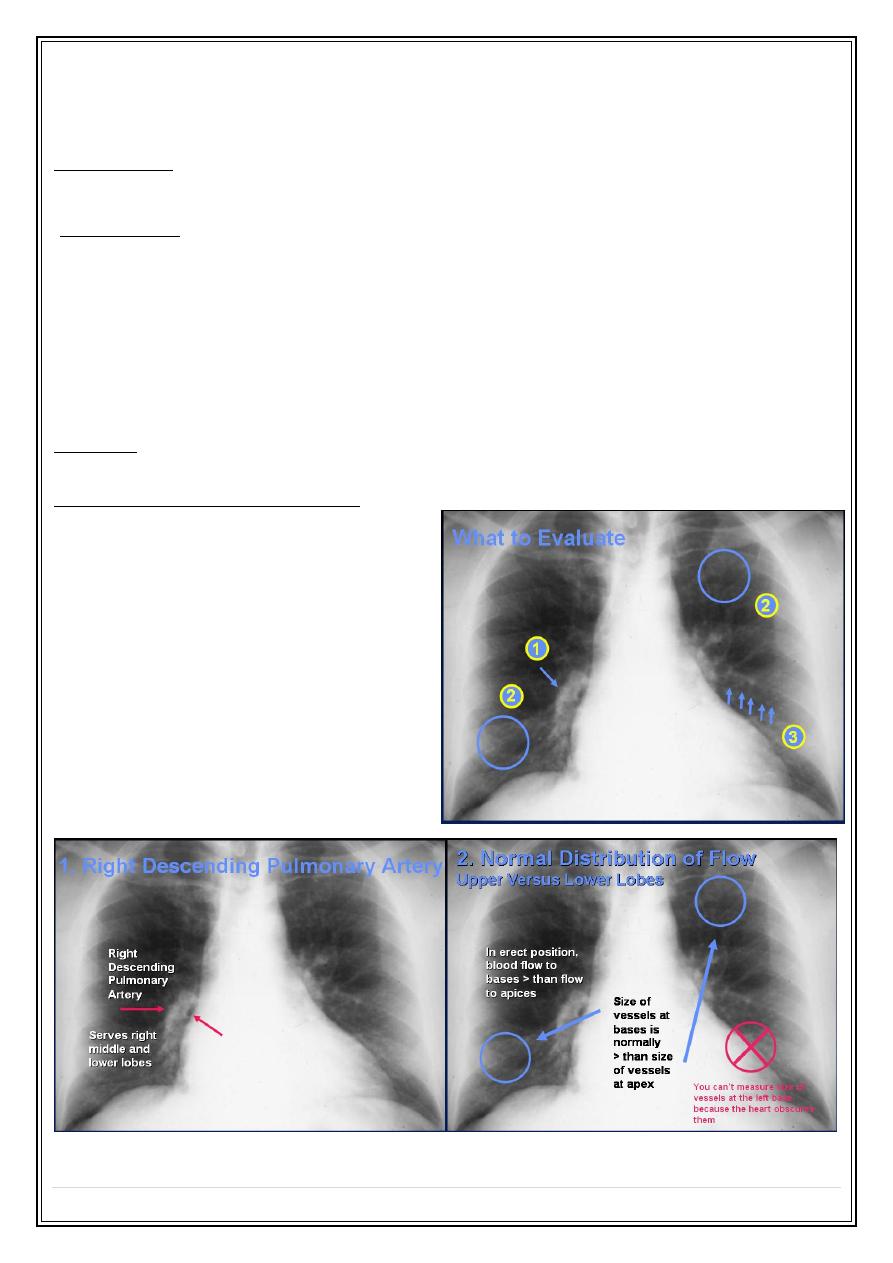
2. Pulmonary vessels
Where is to look?
1. Main pulmonary artery.
2. Descending branch of Rt pulmonary artery ( normal 9-16 mm ).
3. The size of vessels within the lung ( subjective ).
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
8
Abnormalities :
1.
Increase
pulmonary blood flow (
pulmonary plethora
).
( ASD, VSD, PDA )
Lt to Rt shunt
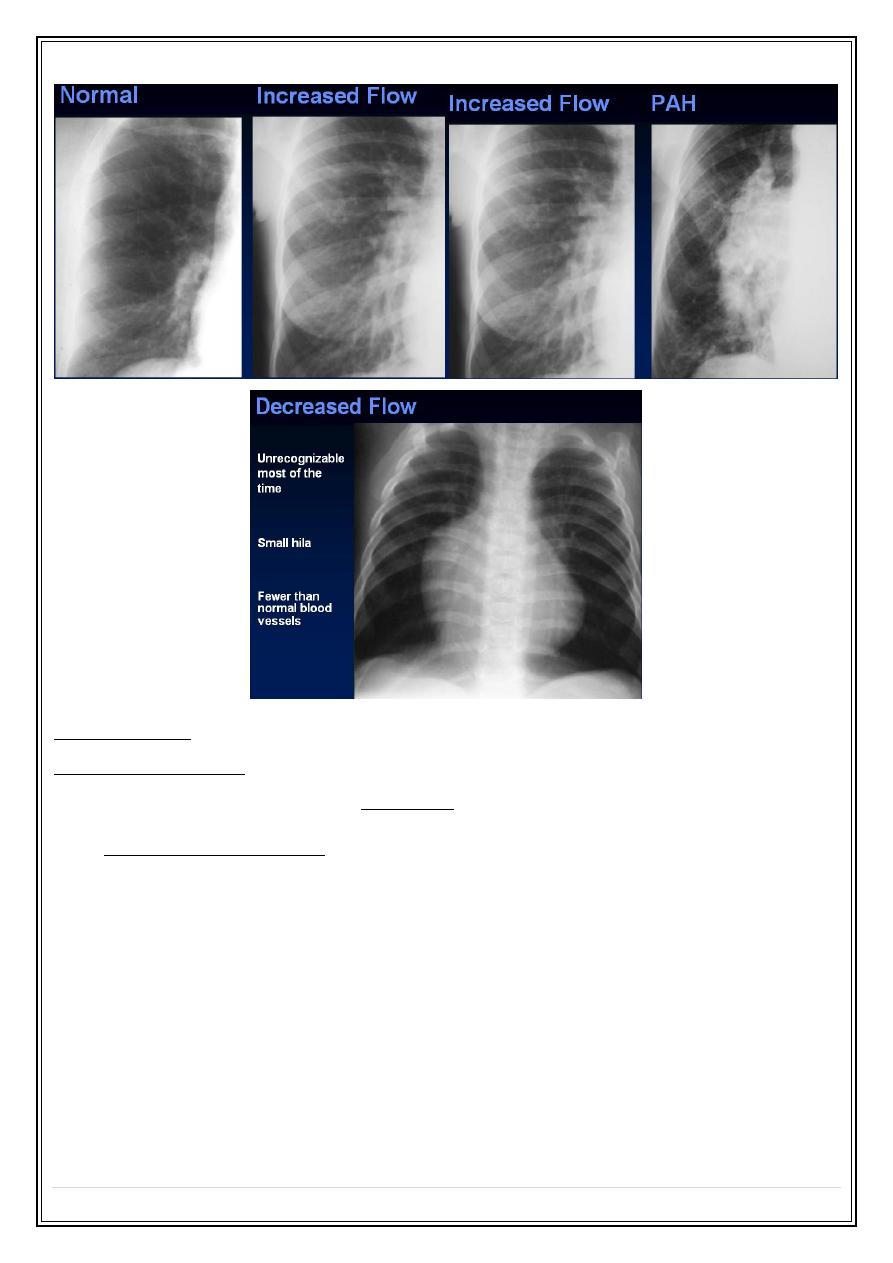
2.
Decrease
pulmonary blood flow (
pulmonary oligaemia
).
( TOF, Severe pulmonary valve stenosis)
Rt to LT shunt
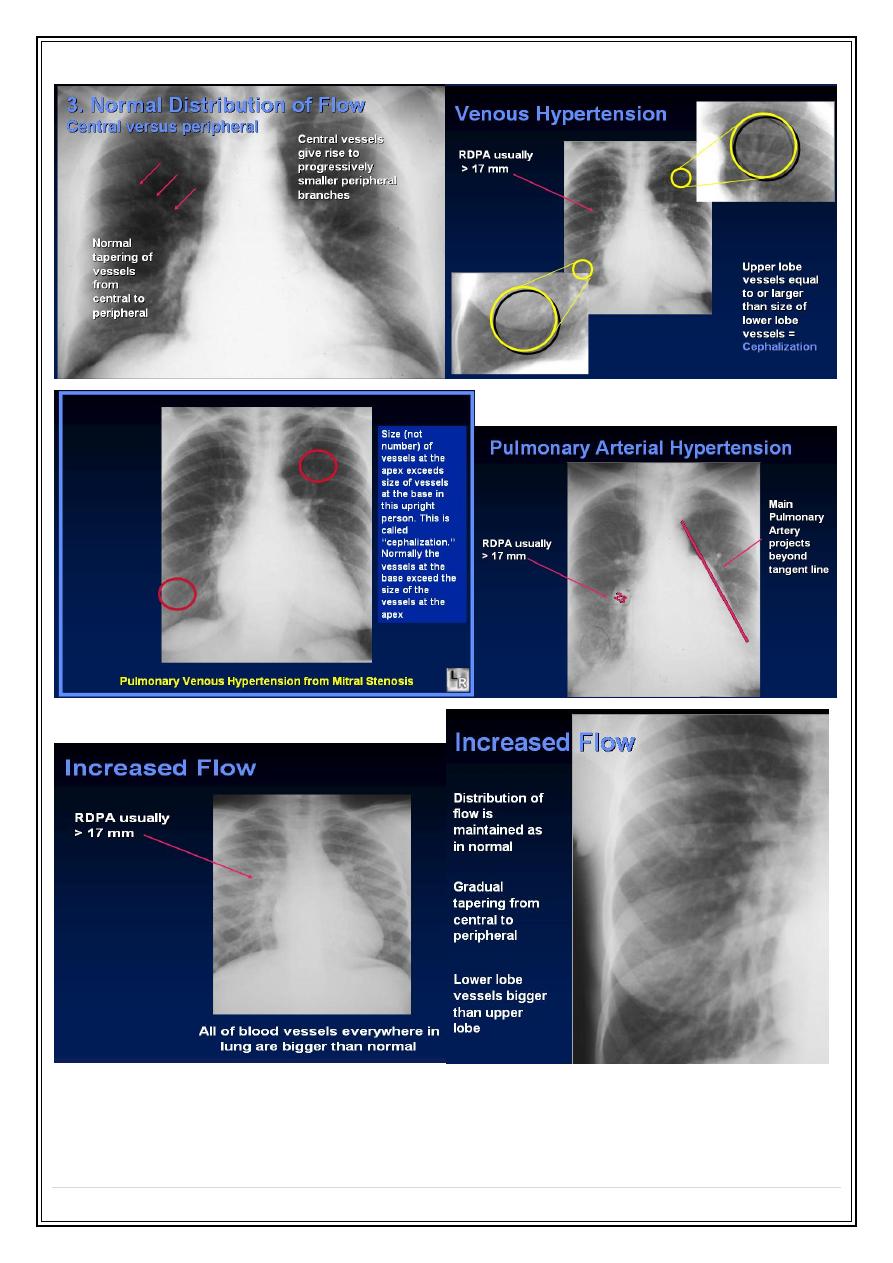
Pulmonary arterial hypertension :
Plain radiograph features
:
1.
Enlargement of the pulmonary artery and hilar arteries.
2.
The vessels within the lung being normal or small.
Pulmonary venous hypertension :
In normal up right person , the lower zone vessels are larger than those in the lower
zones.
In pulmonary venous hypertension, the upper zone vessels enlarged and in severe cases
become larger than those of
lower zones. (
upper lobe blood
diversions
-cephalization)
The Pulmonary Vasculature
Five States of the pulmonary vasculature:
•
Normal
•
Pulmonary venous hypertension
•
Pulmonary arterial hypertension
•
Increased flow
•
Decreased flow
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
9
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
10
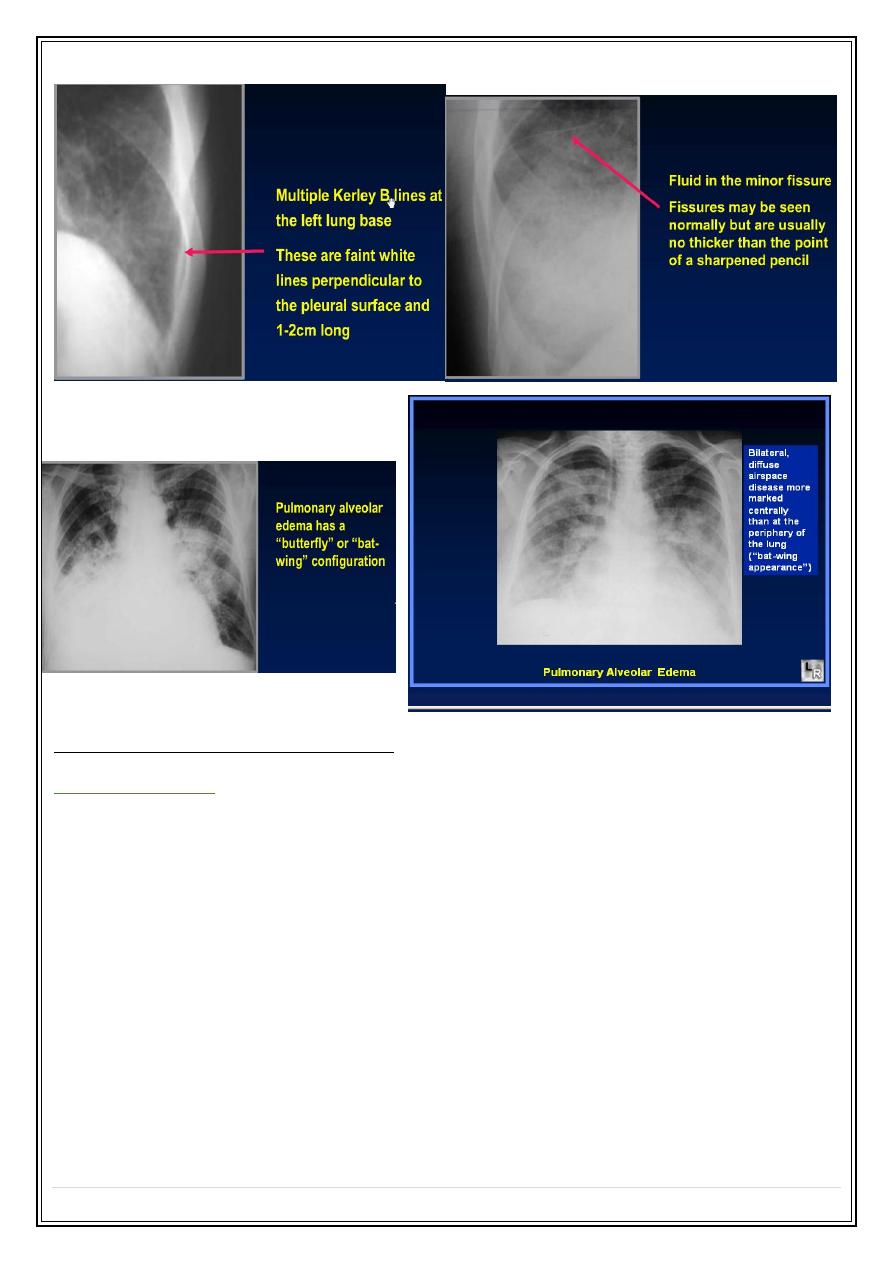
3.The lung
Pulmonary oedema
1.
Interstitial pulmonary edema
.--- Septal line ? ( e.g.
Kerley B lines
—horizontal lines,
never more than 2 cm , seen laterally at the lower zones , reaching lung edge ).
Thickening of the fissure.
2.
Alveolar pulmonary edema.
1. always acute.
2. almost always bilateral &involve all the lobes.
3. in early stages, the shadowing is maximal close to the hila & fades out
peripherally, leaving a relatively clear zones around the edge of the
lobes, (
bat's wing or butterfly patterns
).
4. later on the shadowing becomes more widespread , but is often most obvious
in the lower zones.
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
11
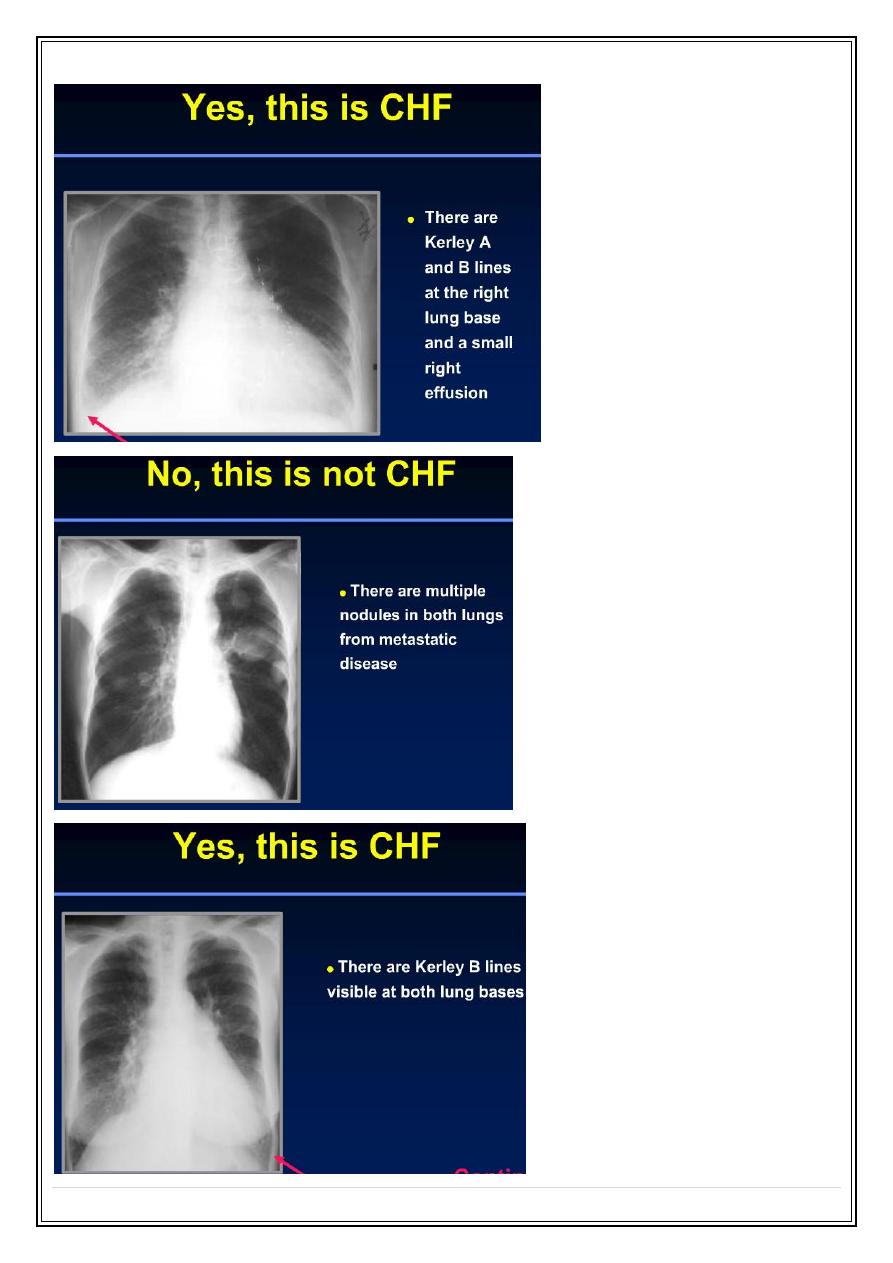
Specific cardiac diseases :
Heart failure :
Signs of heart failure seen on plain radiograph :
1.
cardiac enlargement
, with or without specific chamber enlargement.
2.
pulmonary venous hypertension
.
3.
pulmonary edema
.
4.
pleural effusion
, usually bilateral, often larger on the right than on the
left, if unilateral are almost always right sided.
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
12
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
13
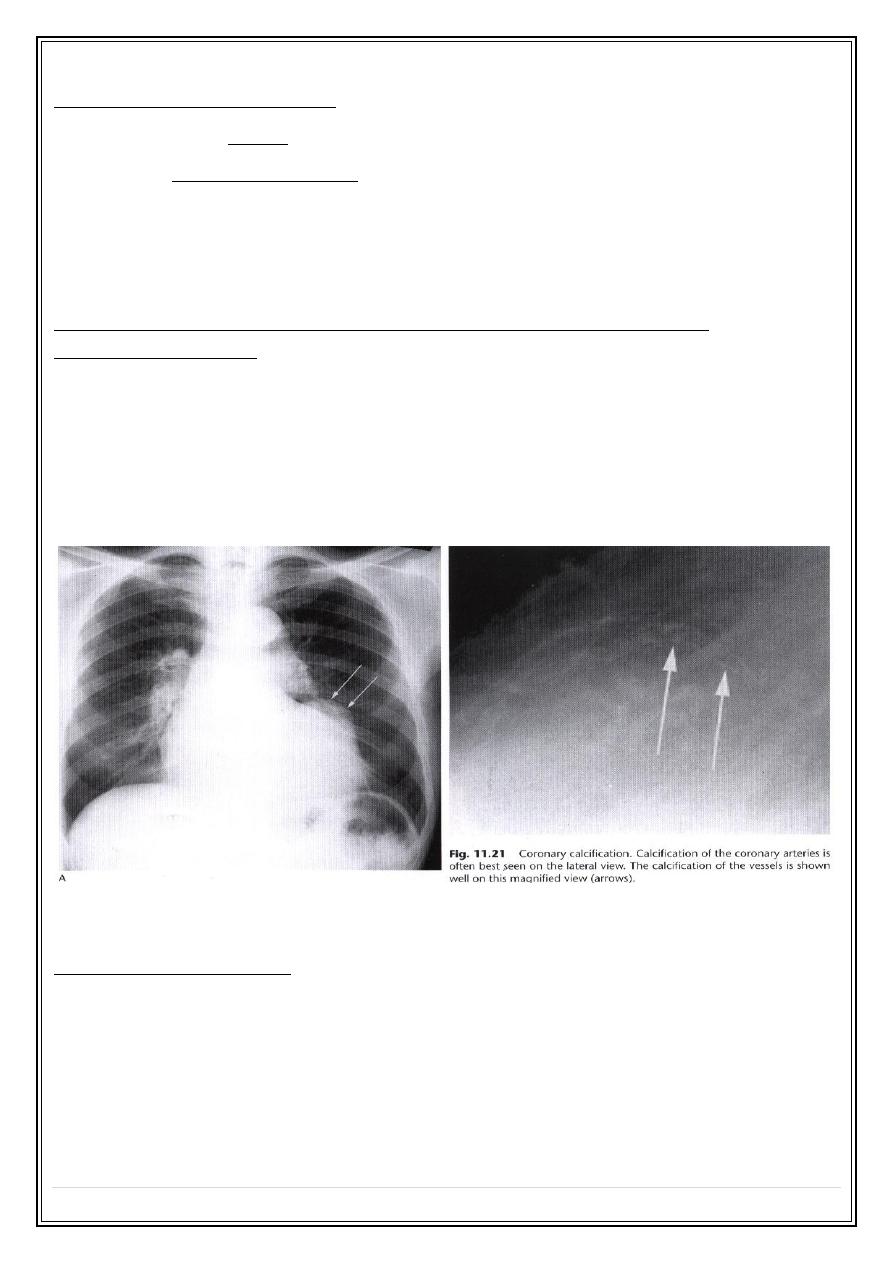
Ischemic heart diseases:
-Most patients with angina have a normal chest films.
-The signs of myocardial infarction that may be present on chest radiograph include :
1. signs of raised pulmonary venous pressure.
2. cardiac enlargement & aneurysm formation.
3. atheromatous calcifications in the coronary arteries
Hypertensive heart disease & other myocardial problems
(cardiomyopathy)
•
ventricular dilatation.
•
moderate left atrial enlargement & signs of elevation of pulmonary venous
pressure.
•
The aorta is large only in systemic HT
Lt ventricular aneurysm
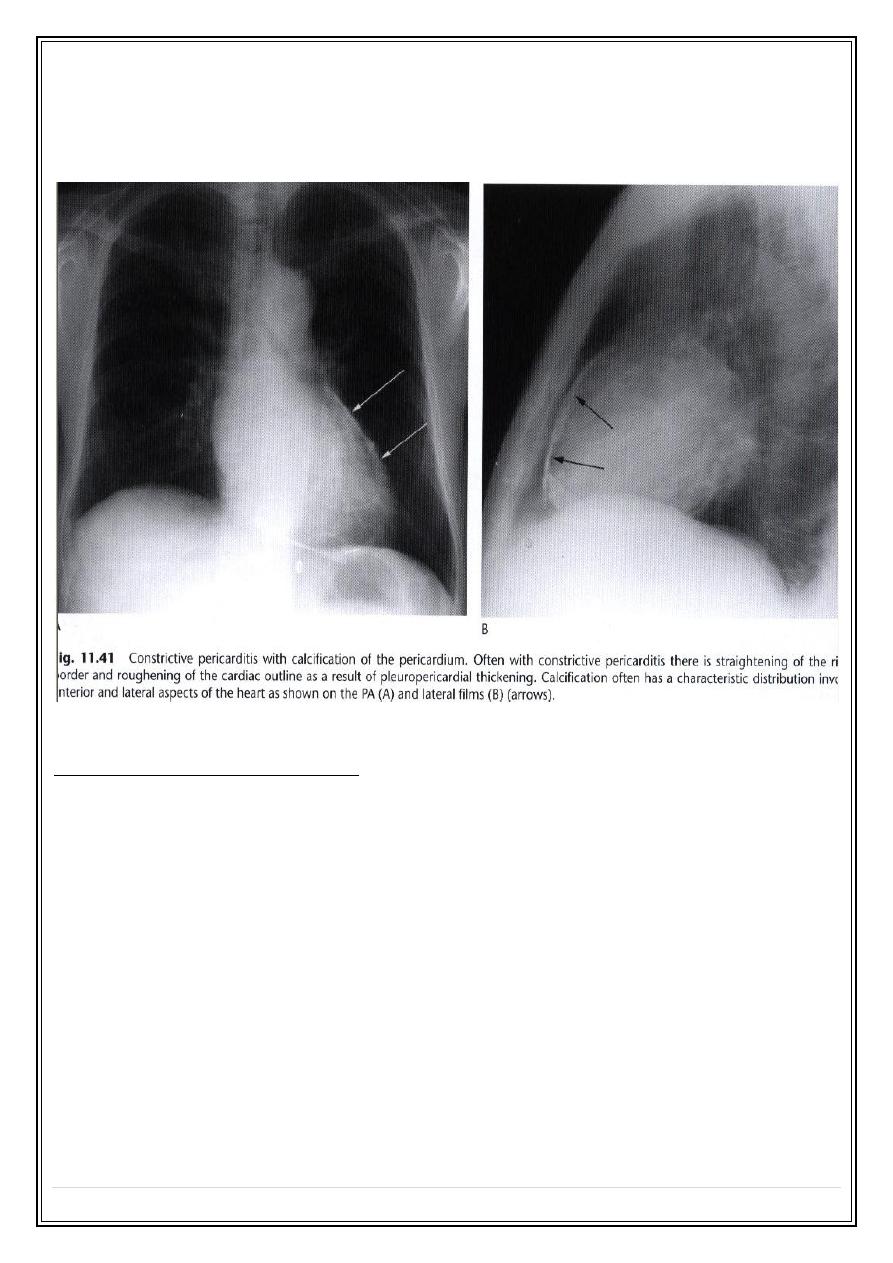
Pericardial diseases:
Pericardial effusion:
- Marked increase or decrease in transverse cardiac diameter within a week or two,
particularly if no pulmonary edema occurs, is virtually diagnostic of pericardial effusion.
-
Pericardial effusion also considered if the heart is greatly enlarged and there are
no features to suggest specific chamber enlargement ( cardiomegaly with
nonspecific chamber enlargement ).
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
14
Pericardial calcification :
- It may be difficult or even impossible to see calcifications on the frontal view, on lateral
view, its usually maximal along the anterior and inferior pericardial borders.
Congenital heart diseases:
1. Left to right shunt (ASD, VSD,PDA):
-
Cardiac enlargement.
-
Enlargement of main pulmonary artery.
-
Large hilar arteries.
-
Pulmonary plethora.
2. pulmonary valve stenosis :
specific appearance:
-
Enlargement of main pulmonary artery.
-
Enlargement of Lt pulmonary artery (post stenotic dilation).
-
The remaining lung vasculature being normal.
-
Usually, the heart is not enlarged.
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
15
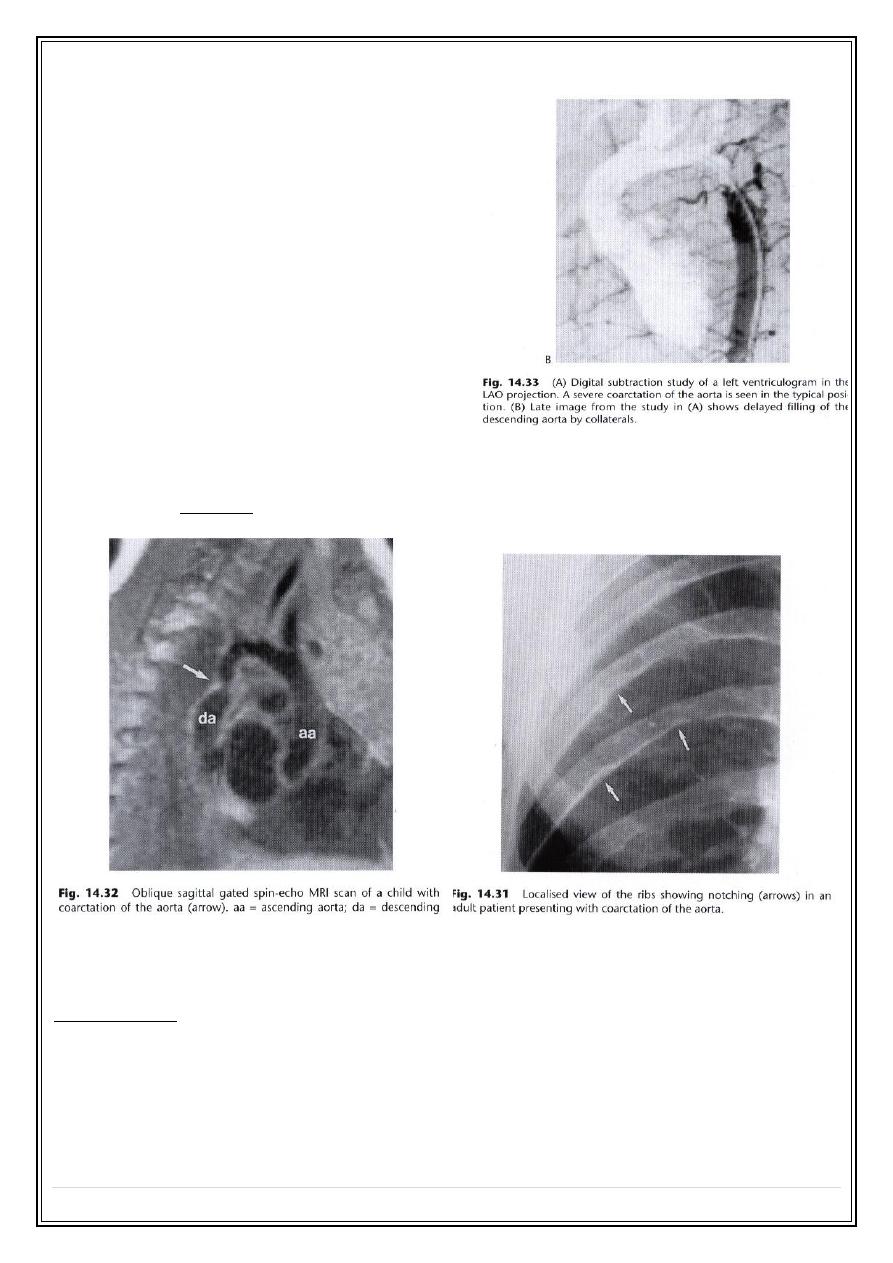
3.Coarctation of aorta :
➢
Abnormal arch :
-
the site of narrowing usual
occurs just distal to left
subclavian artery. may be seen
on a plain film as an
indentation.( best seen by
angiography & MRI )
-
some time bulge above the
coarctation from dilatation of
left subclavian artery, as well
as a bulge below due to post
stenotic dilatation of the aorta.
➢
The heart and ascending
aorta are often enlarged
due
to long standing hypertension.
➢
Rib notching
, is a frequent sign in older children & adults, due to
enlargement of intercostals arteries which acts as a collateral vessels (
features: one or more small cortical indentations on the inferior margins of
the posterior halves of the ribs from the 3rd or 4th ribs downwards ).
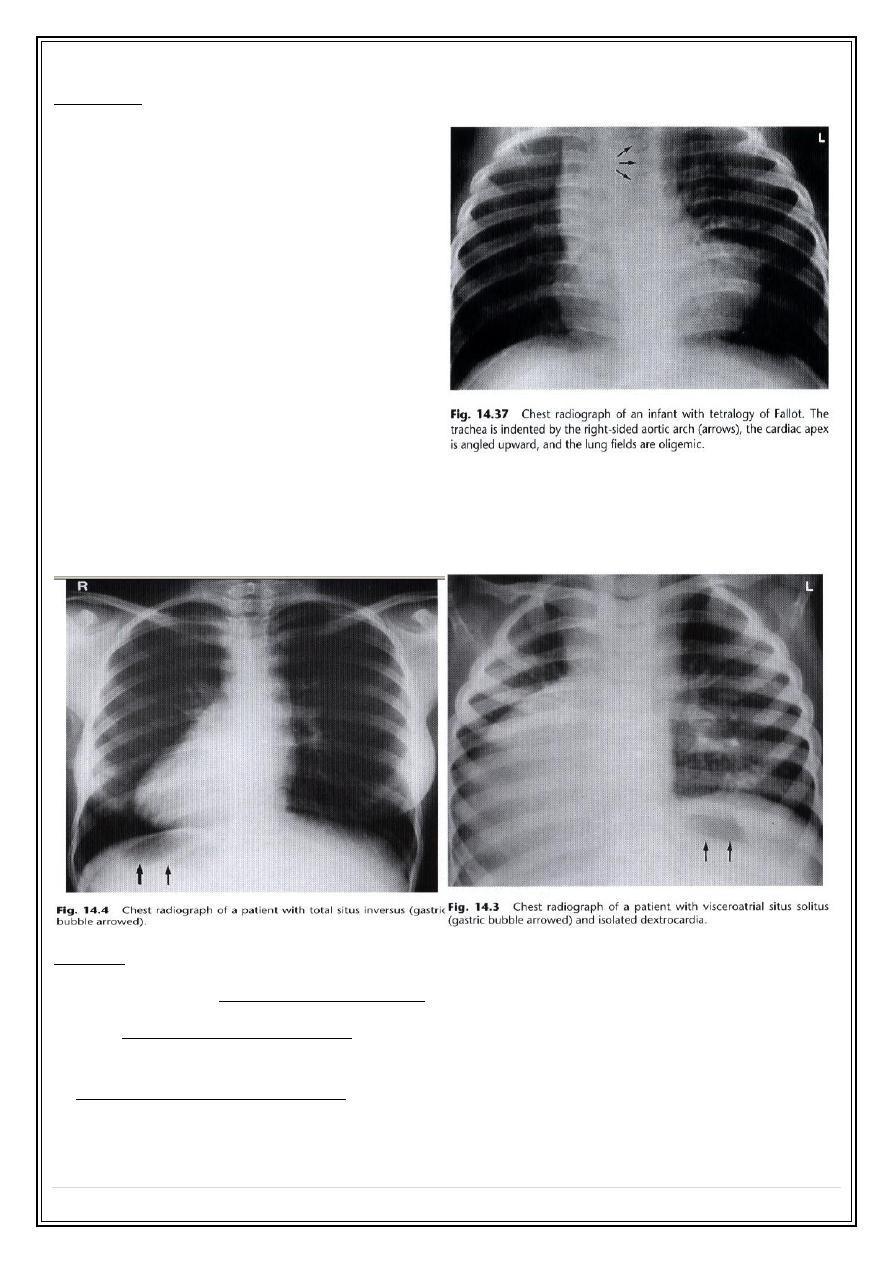
4.Tetralogy of Fallot (TOF ):
Components :
1. VSD.
2. Right ventricular out flow obstruction ( usually subvalvular or valvular stenosis ).
3. Rt ventricular hypertrophy.
4. Aorta overriding the ventricular septal defect.
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
16
Features :
-
half cases have a normal chest
radiograph.
-
the abnormal radiological signs,
when present are:
1. upturned cardiac apex. Boot
shaped heart
2. a bay in the region of the main
pulmonary artery .
3. pulmonary oligaemia.
4. Right sided aortic arch in 25 % of
cases.
5. Dextrocardia
- isolated
- total situs inversus
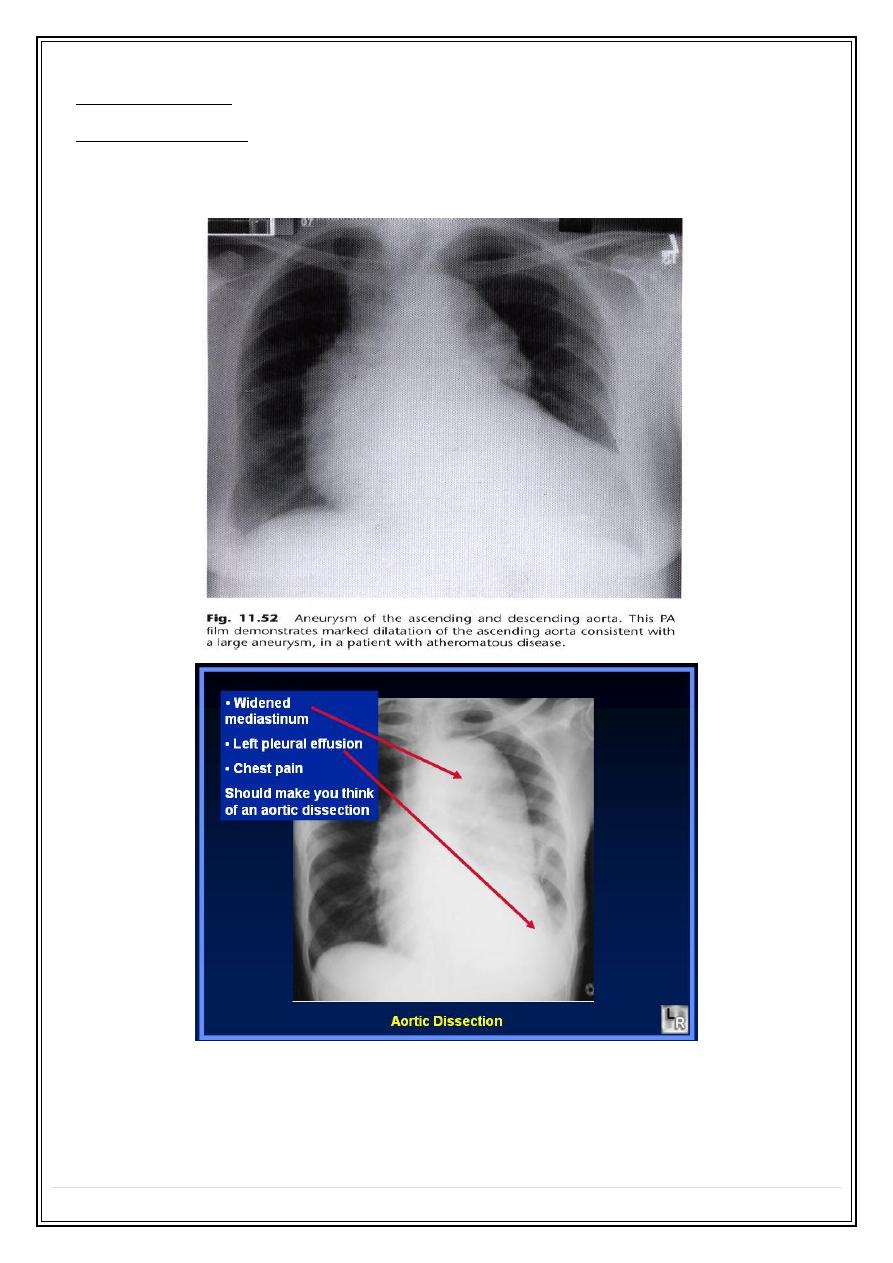
Aorta:
1. Aging process---elongation & unfolding.
2. True ascending aorta dilatation may be due to aneurysm formation or aortic
regurgitation , aortic stenosis or systemic hypertension.
3. Aneurysm of descending aorta . the two common causes are atheroma and aortic
dissection, a rarer cause is previous trauma. CT angiography & MRI are very useful
tests.
Secret Lectures
(8)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
17
4. Aortic coarctation.
5. Rt sided aortic arch :associated with intracardiac malformations ( TOF, pulmonary
atrasia, & truncus arteriosus ) or in isolation.
Thank You,,,