1
L4
Dysmenorrhea
D. Wsn
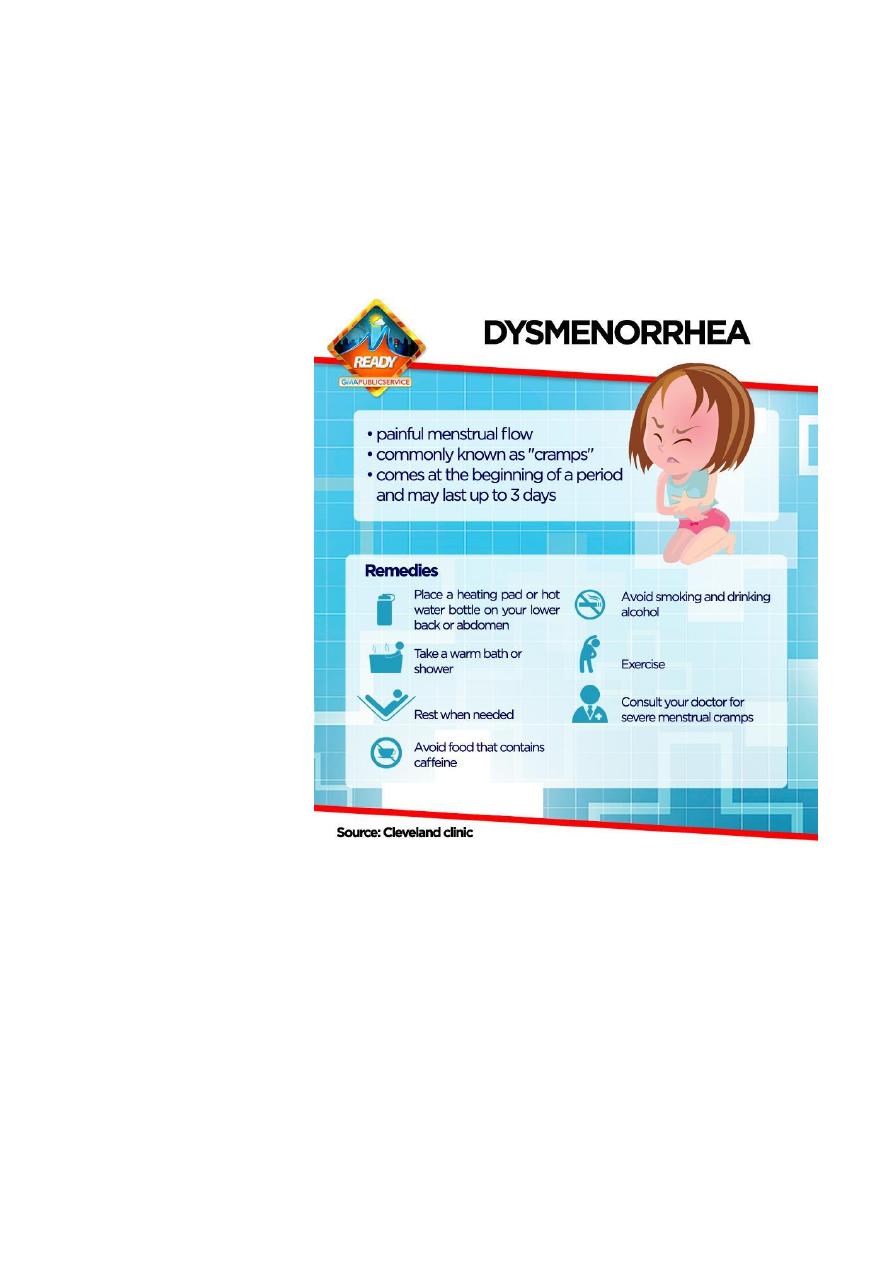
Definition is painful menstruation
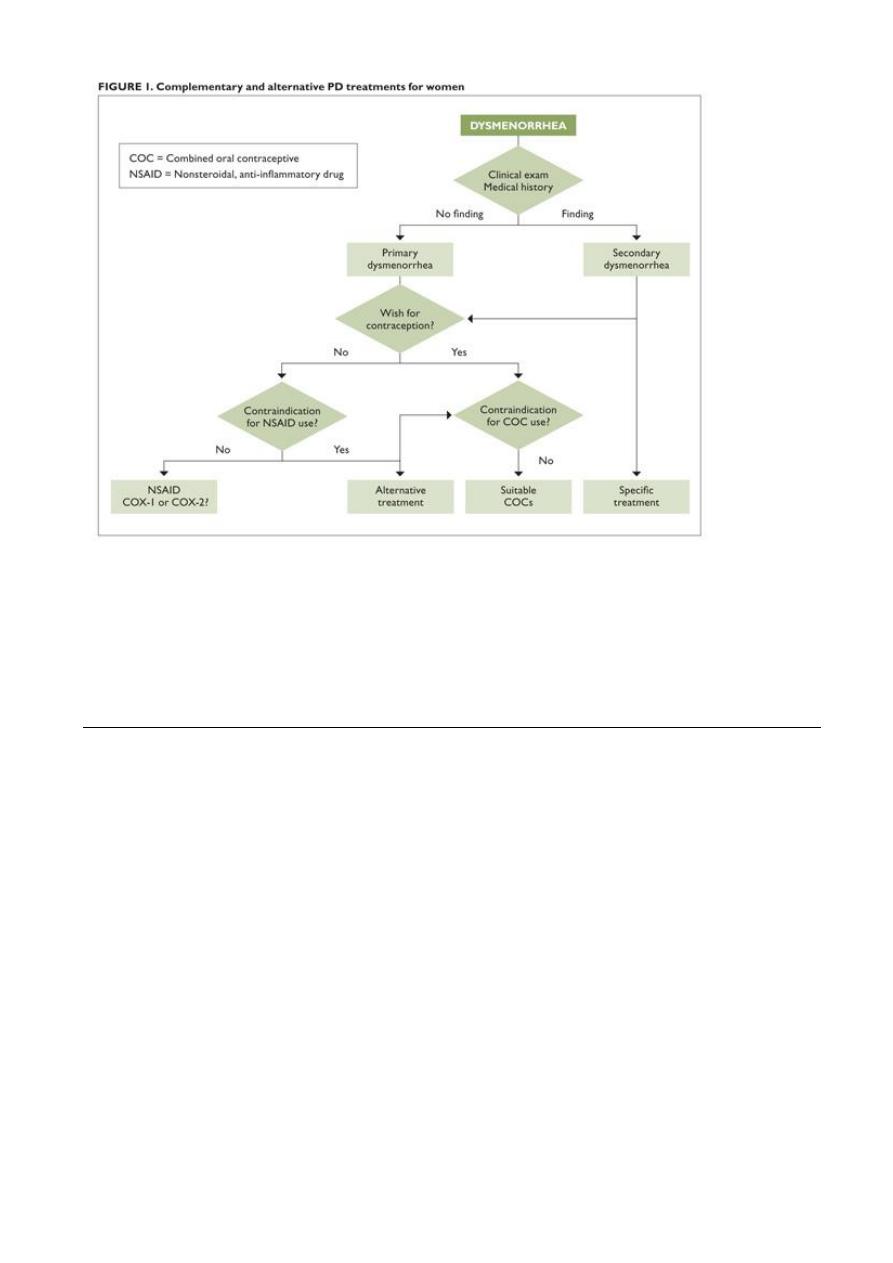
Classification: 1. Primary dysmenorrhea
2. Secondary dysmenorrhea
Epidemiology
The age and parity are inversely related to the incidence of dysmenorrhea
Family history
Stress increase incidence
Smoking . low body mass index
Early menarche . heavy menstrual loss
Exercise and high intake of fruit and vegetables reduce incidence
Psychological morbidity . sexual abuse
Causes
Primary dysmenorrhea
Uterine myometrium hyperactivity
Excess prostaglandin production during menstruation –increase myometrium
contraction –reduction uterine blood flow –increase ischemia and pain
Physiological
Ovulatory cycle is essential for development
Secondary dysmenorrhea
Underlying pathological causes
Causes gynecological
. Endometriosis . adenomyosis. Uterine fibroid
. Cervical stenosis and other obstructive causes
. Pelvic venous congestion
. Residual \trapped ovary syndrome
o . Pelvic adhesion . Pelvic inflammatory disease
Gastrointestinal: irritable bowel syndrome
Chronic constipation
Urinary tract: bladder pain syndrome (interstitial cystitis)
Musculoskeletal: pelvic floor myalgia
Myofascial pain
Neurology: nerve entrapment
2
Symptoms and sign
Primary spasmodic dysmenorrhea:
Is colicky cramping suprapubic pain that may radiate to the back and thigh
Associated with gastrointestinal and systemic symptoms
Is usually begin few hours before or within the onset of menstruation
Continue for 8 to 72 hour
Typically, in young female
Onset within 6- 12 months after menarche
Cause significant morbidity and negative pelvic pathology
Secondary dysmenorrhea
Pain associated with identifiable pelvic pathology
is more sever before menstruation
Exacerbated by menstruation and continue throughout the cycle
Usually associated with deep dyspareunia
Usually more common in older woman
Investigation
Investigation of primary dysmenorrhea is unnecessary unless there are atypical symptoms or
abnormal finding on pelvic examination
Ultrasound: endometriomata, PID sequelae, fibroid, congenital abnormalities
STI screan including chlamydia swab
Laparoscopy is usually reserved for woman with ultrasound abnormalities, medical
treatment failure or those with concomitant subfertility
hystrosalpingogram useful to identify intrauterine adhesion
MRI
Treatment
In the majority nothing more than general advice, reassurance and empirical relief of pain
The girl should realize that her complaint is likely to be short lived
NSAIDs: produce moderate or excellent pain relief
More effective than paracetamol
Selection according to cost and patient preference (naproxen, mefenamic acid,
diclofenac …)
Limited by its side effect
May be used in combination with another drug like codeine and paracetamol
Calcium channel blocker
Oral contraception
For inhibition of ovulation
LNG-IUS
Effective for pain and as contraception
GnRH analogues
3
Act through induce hypo estrogen state
Limited use
Relive the symptom if waiting for hysterectomy or as a form of assessment as to the benefits
of hysterectomy
Heat: effective as NSIAD in relieving pain
Life style changes
.low fat, vegetable diet may improve the symptoms
.exercise may improve symptoms by improving blood flow to the pelvis
Vitamin B1 and magnesium
Treatment of underlying pathology in case of secondary dysmenorrhea
Therapeutic laparoscopy :diagnosis and management of endometriosis adhesion and PID
.hysterectomy is now rare
. laproscopic uterine nerve ablation is not currently recommended
.injection of pelvic plexus with anesthetic agent
.dilation of the cervix
4
Self-assessment
Q1: how can you clinically differentiate between primary and secondary dysmenorrhea
Q2: what types of birth control methods help control dysmenorrhea?
Q3: what is the surgery done to treat dysmenorrhea?
Q4: what alternative treatment help ease dysmenorrhea (non-medical)
.
.