Orthodontic Diagnosis
INTRODUCTIONOrthodontic diagnosis deals with recognition of the various characteristics of the malocclusion. It involves collection of different data in a systemic manner to help in the identifying the nature and cause of the problem.
Diagnostic aids – comprehensive orthodontic diagnosis is established by use of certain clinical implements called diagnostic aids.
There are two types of diagnostic aids :
a. Essential diagnostic aids:i. Case history
ii. Clinical examination
iii. Study models
iv. Certain radiographs – Periapical radiograph, bite wing, occlusal , Panoramic radiograph, lateral cephalometric.
v. Facial photographs
b. Supplemental diagnostic aids :
i. Specialized radiographs
ii. Electro myographic examination of muscle activity
iii. Hand – wrist radiograph
iv. Endocrine tests
v. Estimation of basal metabolic rate
vi.magnatic resonance imaging (MRI)
vii. Sensitivity test
viii. Computed axial tomography (CT scan)
• i. Case history
• Case history Is the information gathered from the patient and/or parents to aid in the overall diagnosis of the case. It includes certain personal details, the chief complaints and present and past history.
1. Name
The patients name should be recorded not only for the purpose of communication and identification but because it gives a personal touch to the following conversation. It makes the patients more comfortable when he is addressed by his first name and arouses a feeling of familiarity, which has a positive psychological effect on the patient.2. Age and Date of Brith
The chronologic age of the patient helps in treatment planning and growth prediction. certain transient conditions, which might be perceived as malocciusion by the patient and parents, can be identified and the concerned are counseled accordingly . The age of the patient also dictates the use of certain treatment protocols-for example, surgical correction might be advocated following cessation of growth whereas the same malocclusion might be treaded using functional appliances if the patient has a potential to grow.3. Sex (gender)
Sex of the patient also helps in treatment planning. Girls mature earlier than boys, i.e. the timing of growth related events including growth spurts, eruption of teeth and onset of puberty are different in males and females. Psychologically also the reaction of males and females maybe different to similar malocclusion since females are generally more concerned about facial aesthetics.4. Address and Occupation
These are important for communication , assessing the socioeconomic status as well for records . The socioeconomic status might dictate the kind of appliance required .Also, patients coming from far may require a different appliance therapy as they might not be able to visit the clinician frequently.5. CHIFE COMPLAINT
The patients chief complaint should be recorded in his or her own words. It should mention the conditions the patient feels and what he/she is suffering from. This helps in identifying priorities and desires of the patients. The parents perception of the malocclusion should also be noted. This will help in setting the treatment objectives and satisfying the family in general.6. MEDICAL HISTORY
Knowledge of a patients general health is essential and should be obtained prior to examination. It is best obtained by a questionnaire . In most cases orthodontic treatment can be undertaken but precautions may be required in patients with rheumatic fever or cardiac anomalies even for molar band placement /removal, if the adjacent gums are inflamed or bleeding is anticipated . Mentally or physically challenged patients may require special management . Information regarding allergies, especially latex or nickel sensitivity and the use of certain drugs should be considered.7. DENTAL HISTORY
The patients dental history should include information on the age of eruption and exfoliation of deciduous and permanent teeth. Reason for exfoliation will also hint at the oral hygiene maintenance capabilities of the patient. The past dental history will also help in assessing the patients and parents attitude towards dental health. Also it should include the history to previous trauma.
8. PRENATAL HISTORY
Prenatal history should concentrate on the condition of the mother during pregnancy and the type of delivery. Her nutritional state and any infections that she might have will affect the developing teeth of the child. The use of certain drugs or even excess use of certain vitamins can result in congenital deformities of the child. Forceps deliveries have been associated with injuries to the temporomandibular joint (TMJ). Excess forceps pressure in the TMJ region can cause ankylosis of the joint and associated mandibular growth retardation.9. POSTANTAL HISTORY
The postnatal history should concentrate on the type of feeding , presence of habits especially thumb sucking and the milestones of normal development. Tongue thrust and thumb sucking habits are associated with malocclusions.10. FAMILY HISTORY
skeletal malocclusions especially skeletal class lll malocclusions and congenital conditions such as cleft lip and palate are inherited . Detailed records of such malocclusion might aid in any future studies on the subject .ii. CLINICAL EXAMINATION
1. GENERAL EXAMINATIONGeneral examination should begin as soon as the patient first comes to the clinic. A general appraisal of the patient is done. The clinician should observe the gait, posture and physique of the patient . Height and weight are recorded to assess for the physical growth and development of the patient. Abnormal gait may be present due to an underlying neuromuscular disorder. Abnormal posture also may lead to malocclusions.
2. BODY BUILD
Sheldon classified body build into :Ectomorphic : Tall and thin physique
Mesomorphic : Average physique
Endomorphic : Short and obese physique
3. Cephalic and Facial Examination
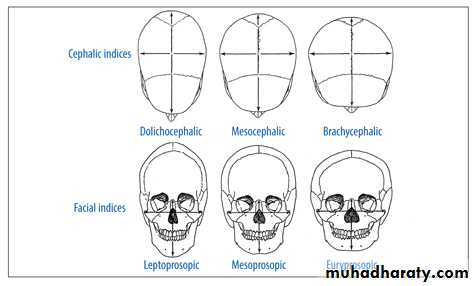
1- SHAPE OF HEAD:
The shape of the head can be evaluated based on the cephalic index of the head which was fourmulated by Martin and saller (1957)as:
Maxiamum skull width__
Maximum skull length• Mesocephalic – average shape of the head. They posses normal dental arches.
• Dolicocephalic – long and narrow head. They have narrow dental arches.• Brachycephalic – broad and short head. They have broad dental arches.
Index value
Mesocephalic : average skull (76-80.9)Dolicocephalic: long narrow skull ( equel or less than 75.9)
Brachycephalic: short broad skull (81-85.4)
Hyperbrachycephalic =>85.5
2- FACIAL FORM :
The shape of the face is assessed by the morphologic facial index which was given by Martin and saller (1957)as:Morphologic facial height (distance between nasion and gnathion)
Bizygomatic width (distance between the zygoma points)
2- FACIAL FORM :
• simple classification – round, oval or square.• scientific classification –
a. Mesoprosopic – average or normal face form (84-87.9)
b. Euryprosopic – broad and short face form (79-83)
c. Leptoprosopic – long and narrow face form(88-92.9)
The type of facial morphology has a certain relationship to the shape of the dental arch, e.g. euryprosopic face types have broad , squar arches ; border line crowding in such cases should be treated by expansion. On the other hand , leptoprosopic face types often have narrow apical base/arches. Therefore, extraction is preferred over expansion .
4. ASSESMENT OF FACIAL SYMMETRY :
The patient’s facial symmetry is examined to determine disproportions of the face in transverse and vertical planes. In most people the right and left sides are not identical , so some degree of asymmetry is considered normal.Gross facial asymmetries can occur as a result of :
• Congenital defects
• Hemi – facial atrophy/hypertrophy
• Unilateral condylar ankylosis
Unilateral condylar hyperplasia
Composite photographs are the best way to indicate normal facial asymmetry. For this boy, whose mild asymmetry rarely would be noticed and is not a problem, the true photograph is in the centre. On the right is a composite of the two right sides, While on the left is a composite of the two left sides. This technique dramatically illustrates the difference in the two sides. Although the normal asymmetry usually is less than in this boy, mild asymmetry is the rule rather than the exception. Usually, the right side of the face is a little larger than the left ,rather than the reverse as in this individual.

Facial proportions and symmetry in the frontal plane.
An ideally proportional face can be divided into central , medial ,and lateral equal fifths. The separation of the eyes and the width of the eyes, which should be equal ,determine the central and medial fifths. The nose and chin should be cantered within the central fifth, with the width of the nose the same as or slightly wider than the central fifth. The inter – pupillary distance (dotted lines) should equal the width of the mouth.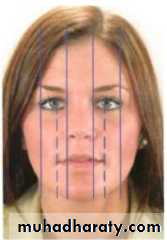
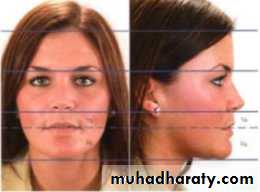
Vertical facial proportions in the frontal and lateral views are best evaluated in the context of the facial thirds, which the Renaissance artists noted were equal in height in well-proportioned faces. In modern Caucasians, the lower facial third often is slightly longer than the central third. The lower third has thirds : the mouth should be one-third of the way between the base of the nose and the chin.
5. FACIAL PROFILE :
The facial profile is examined by viewing the patient from the sides by making the patient view at a distant object , which the FH plane parallel to the floor.The facial profile helps in diagnosing gross deviations in the maxillo-mandibular relationship.
The profile is assessed by joining the following two reference lines:
• A line joining the forehead and the soft tissue point A( deepest point in curvature of upper lip).
• 2. A line joining point A and the soft tissue pogonion (most anterior point of the chin).
Profile convexity or concavity results from a disproportion in the size of the jaws, but does not by itself indicate which jaw is at fault. A convex facial profile( A) indicates a Class ll jaw relationship, which can result from either a maxilla that projects too far forward or a mandible too far back. A concave profile( C) indicates a Class lll relationship, which can result from either a maxilla that is too far back or a mandible that protrudes forward.
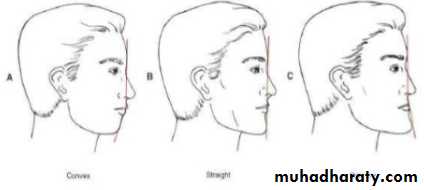
Three types of profiles are seen
Straight/Orthognathic profile: The two lines form an almost straight lineConvex profile : The two lines form an acute anglewith the concavity facing tissues.this type of profile is seen in class II div 1 patients due to either a protruded maxilla or a retruded mandible.
Concave profile : The two lines form an obtuse angle with the convexity facing the tissues . This type of profile is seen in class Ill patients due to either a protruded mandible or a retuded maxilla.
6. FACIAL DIVERGENCE : Facial divergence is defined as anterior or posterior inclination of the lower face relative to the forehead. Facial divergence can be of 3 types :
a. Anterior divergence : a line drawn between the forehead and chin is inclined anteriorly towards the chin.
b. Posterior divergence : a line drawn between the forehead and chin slants posteriorly towards the chin.
c. Straight divergence : the line between the forehead and chin is straight or perpendicular to the floor.
