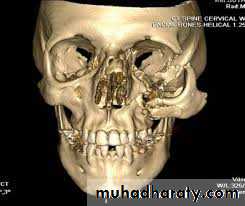
Fractures Of The
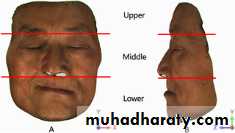
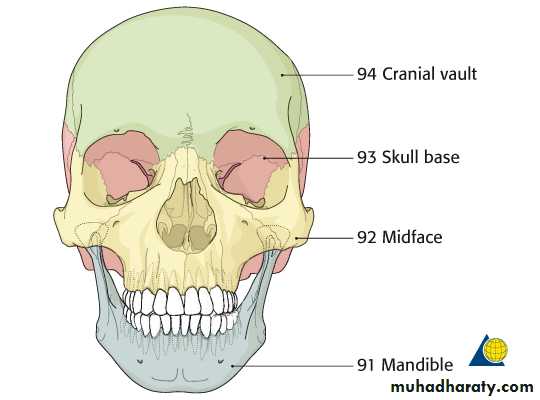
Midfacial SkeletonThe facial skeleton can be roughly divided into 3 areas:1- Lower third (mandible)2- Upper third is formed by frontal bone3- Middle third from the frontal bone to the level of upper teeth (or the upper alveolus if edentulous)
Etiolog :1- Road traffic Accident (RTA)2- Fall form height3- Occupational accidents4- Altercations (fighting)5- Sport injuries6- Missile injures (war injures)
Surgical Anatomy:The middle third of facial skeleton: is the area bounded superiorly by a linedrawn across the skull from the zygomatico-frontal suture across the frontonasal and fronto-maxillary sutures to the zygomatico-frontal suture on the opposite side, and inferiorly by the occlusal plane of the upper teeth or the upper alveolus (if edentulous).
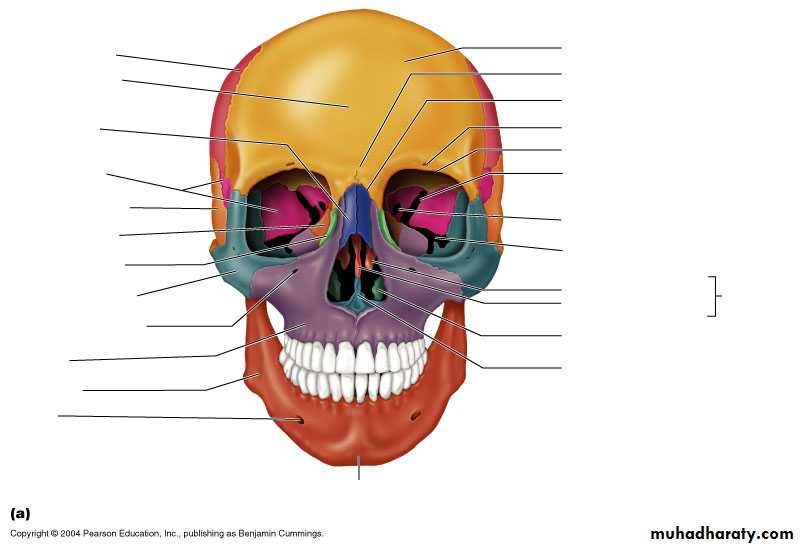
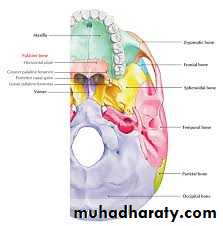
The middle third is made up of the following bones:1- Two maxillae2- Two zygomatic bones3- Two zygomatic processes of the temporal bone4- Two palatine bones5- Two nasal bones6- Two lacrimal bones7- The vomer8- The ethmoid and its attached conchae9- Two inferior conchae10- The pterygoid plates of the sphenoid
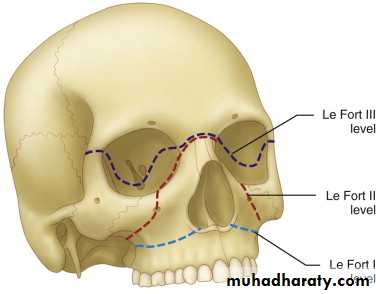
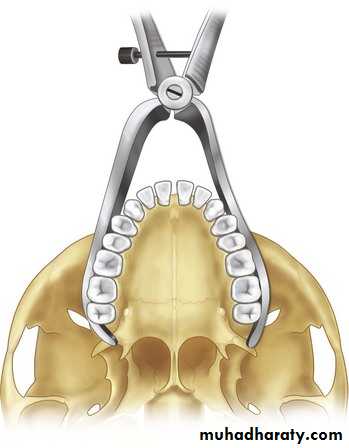
Classification:Following experimental trauma to the cadaver head carried out by Rene Le Fort in 1901, he discovered that the complex fracture patterns could be broadly subdivided into 3 groups:
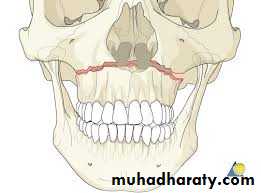
1- Le Fort I (Guerin or Low - level fracture)
2. Le Fort l (pyramidal or sub-zygomatic fracture)
3- Le Fort Il (high level or suprazygomatic fracture)
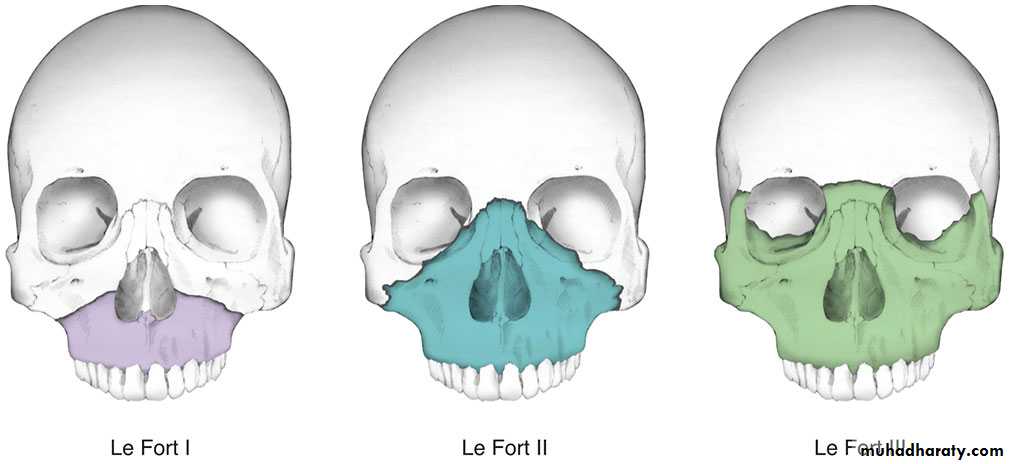
A simple classification which is practical for the purposes of diagnosis and treatment, base divide fractures into:1. Dento-alveolar fractures2. Zygomatic complex fractures3. Orbital floor fracture4. Nasal complex fractures5. Le Fort I (low-level fracture)6. Le Fort Il (pyramidal or subzygomatic fracture).7. Le Fort Ill (high-level or suprazygomatic fracture).
Clinical findings in the various types of fractures Siqns and Symptoms):I. Dentoalveolar fractures:A. Damage to the teeth:1. Fracture of the crown of the tooth with or without pulp exposure.2. Vertical splitting of upper premolar and molar teeth.3. Fracture of the roots, should be detected by intra oral periapical x-ray.4. Avulsion, intrusion or subluxation of teeth.5. For unconscious patient who have missed, avulsed or fractured teeth; chest x-ray should be taken to exclude inhalation of teeth.
B. Damage to the lip:1. Edema and ecchymosis of the inner aspect of the lip.2. laceration of inner aspect of the lip.3. The fractured crowns may be embedded in the upper lip and should bedetected by x-ray.
C. Alveolar fracture:1. Fracture of the maxillary tuberosity and antral floor.2. Comminuted fractures of the alveolus if the blow is violent which is usually in the incisor area.3. Bony deformity and crepitus.
II. Fracture of the zygomatic complex:The zygomatic bone is intimately associated with the maxilla, frontal and temporal bones and they are usually involved when a zygomatic bone fracture occurs, so it is called zygomatic complex fracture. The zygomatic bone usually fractures in th region of the zygomatico-frontal, zygomatico-temporal and zygomatico-maxillary.sutures. The zygomatic bone fracture may be simple or comminuted
Classification of zygomatic complex fracture is according to the site of the fracture, degree and direction of the displacement:
• a- Fracture of the body of the zygomatic complex involving the orbit:
1. Minimal or no displacement2. Inward & downward displacement3. Inward & posterior displacement4. Outward displacement5. Comminution of the complex as a wholeb- Fracture of the zygomatic arch alone not involving the orbit:1. Minimal or no displacement2. V-type in-fracture3. Comminuted
A practical classification of zygomatic fractures+ Segmentala. Zygomatic archb. Infraorbital rim+ Minimally displaced+ Displaced+ Comminuteda. Associated with midface or complex orbital fracturesb. Associated with soft tissue including ocular injury
physical signs (zygomatic complex)On inspection externally:1. Circumorbital ecchymosis
2. Subconjunctival ecchymosis 3. Oedema of cheek 4. Flattening in the region of zygoma on injured side 5. limitation of ocular movements6. diplopia 7. Strabismus 8. Enophthalmos 9. Limitation of lateral excursion
of mandible to injured side 10. Limitation of opening or closing of manible l1. Unilateral epistaxis on injured side



On palpation:1. Tenderness over cheek bone2. Tenderness & separation at fronto-zygomatic suture3. Notch in lower rim of orbit in the region of the zygomatico-maxillary Suture4. Anesthesia or paraesthesia of the cheekOn inspection intra-orally:1. Ecchymosis in upper buccal sulcus in region of zygomatico-maxillary buttress.2. Possible gagging of occlusion in molar area on injured sideon palpation
1. Tenderness in upper buccal sulcus in region of zygomatic buttress2. Anesthesia of upper gum
Symptoms of The patient complain of:1. Flattening of cheek2. Swelling and bruising around the eye3. Blood-shot eye4. Double vision5. Squint6. One eye too far back7.One eye lower than the other (hypoglobus)8. Tenderness over the cheek9. Anaesthesia of the cheek and gums10. Lump on the lower orbital rim11. Difficulty in either opening or closing the mouth12. Inability to move the jaw towards the injured side13. Gagging of the back teeth to the injured side
Summary of clinical findings in zygomatic complex fractures 2015
- Flattening of cheek- Swelling of cheek- Anesthesia of cheek, temple, upper teeth and gingiva- Periorbital hematoma- Sub-conjunctival hemorrhage- Tenderness over orbital rim and fronto-zygomatic suture- Step deformity of infraorbital margin- Palpable separation at fronto-zygomatic suture- Ecchymosis and tenderness intra-orally over zygomatic buttress- Limitation of ocular movement- DiplopiaFractures of the zygomatic arch:the only visible evidence of fracture is a depression of about 2.5 cm in diameter over the zygomatic arch associated with limitation of mandibular opening or closing.
Fractures of the zygomatic arch can be divided into two main groups:-I. Minimal or no displacementII. The triple fracture of the arch with a depressed V- type displacementIII. Comminution of the zygomatic archin the v-type-in fracture, the apex of the "V" may impinge on the coronoid process usually reposition themselves presumably as a result of movement of the temporalis muscle and coronoid process beneath them.
III. orbital Floor Fracture (Blow out fracture):Applied surgical anatomy:The orbit is said to be roughly pyramidal in shape with its apex at the optic foramen, It is made up of the orbital portion of the maxillary bone and part of the zygomatic bone. The eyeball is suspended by Lockwood's suspensory ligament from whitnall’s tubercle just below the zygomaticofrontal suture to the inner wall of the orbital rim (lacrimal crest)
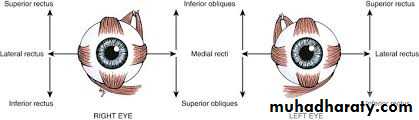
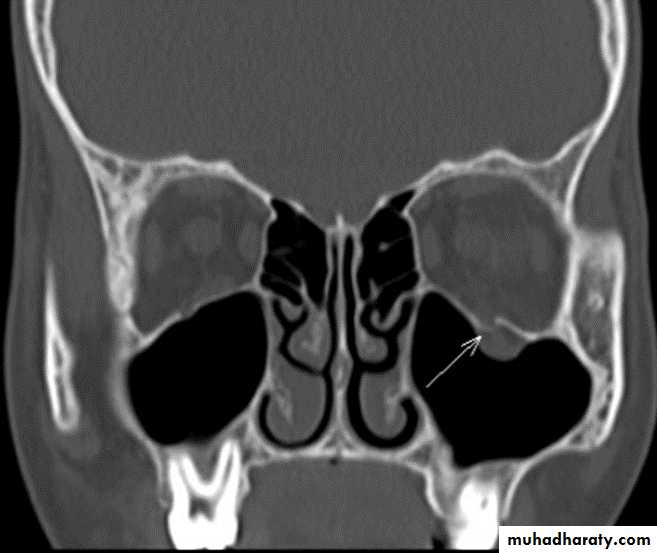
With this fracture, the fragments of bone are displaced downwards into the antralcavity remaining attached to the orbital periosteum rather like a trap-door the peri-orbital fat tends to herniate the defect and this has the effect of interfering with the action of the inferior rectus and inferior oblique muscles ( prevent upward movement and outward rotation of the eye with resulting diplopia or double vision in these directions of gaze ) . if a large amount of orbital fat is displaced through the orbital floor defect it may result in enophthalmos .
It is important to recognize that two distinct types of orbital floor fractures can be identified : 1. Those occurring as part of the natural fracture pattern in fractures (Impure) of the zygomatic complex or Le Fort ll and Ill type fractures of the middle third of the face.2. Those occurring as an isolated orbital floor fracture (Pure), either as a so-ca'blow-out' or rarely as a localized elevation or 'blow-in' fracture.
Summary of possible clinical findings in isolated orbital floor fractures- Periorbital ecchymosis- Sub-conjunctival hemorrhage- Diplopia- Limitation of eye movement especially in upward gaze- Globe retraction on upward gaze- Enophthalmos- Surgical emphysema of eyelids (leakage of air from the paranasal sinuses)- Paraesthesia within distribution of infraorbital nerve
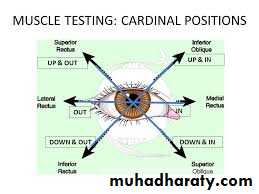
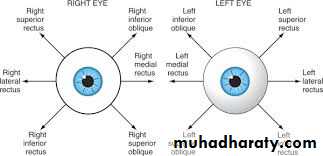
The tethering of the inferior muscles can be demonstrated by the:1- Forced duction test under local or general anesthesia2- Cardinal positions of gaze (horizontal, vertical, torsional, or combination ofthese)3- Hess chart

Radiology:Radiopacity of the maxillary and ethmoidal air sinuses which appear cloudy due to extravasation of blood into them via a fracture of the overlying bone. With standard sinus views there may be the characteristic "hanging drop sign", which is best demonstrated by Waters projection of the face (OM projection employing a horizontal beam of X-ray emerging through the infra-orbital rim). CT scan demonstrate the normal sigmoid outline of the orbital floor giving the so-called 'posteromedial bulge'.


IV. Nasal complex fracture:The nasal bone may be fractured alone. But the more usual fracture involves the frontal processes of the maxillae, the nasal septum, vomer, perpendicular and cribriform plates of ethmoid.
Summary of possible clinical findings in nasal complex fractures* Bruising of skin over nasal bones* Laceration of skin of bridge of nose* Bilateral medial orbital ecchymosis* Epistaxis* Deformity of nose and inter-orbital area (septal deviation or saddle-type depression)*Crepitus of bones of nasal complex* Unilateral or bilateral telecanthus*Airway obstruction* Septal laceration or hematoma*Cerebrospinal fluid (CSF) rhinorrhea* Epiphora due to damage to the nasolacrimal duct
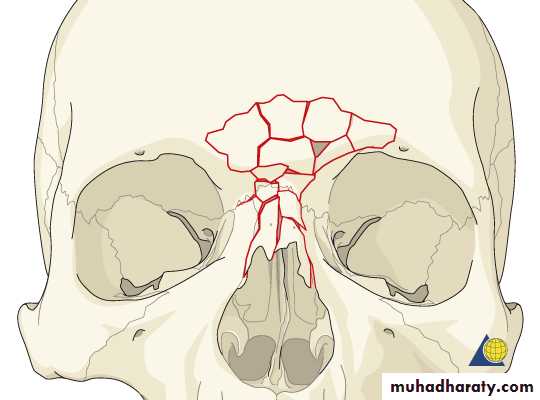
Possible planes of nasal fracture.
1. Nasal tip only2. Nasal bones
3. Naso-orbito-ethmoid complex
“Rule of fifths” showing the assumed facial proportion on frontal view for assessing of traumatic telecanthus,
V. Le Fort I fracture:Sumnary of possible clinical findings in Le Fort I fractures- Mobility of whole dento-alveolar segment of upper jaw and disturbed occlusion- Palpable crepitation in upper buccal sulcus
- Cracked-Pot sound on percussion note from upper teeth- Hematoma intraorally over root of zygoma- Ecchymosis or laceration in palate- Fractured cusps of check teeth (Subluxed, avulsed and fractured teeth)- Bruising and swelling of upper lip and lower half of midface
VI. Le Fort Il fracture:Summary of possible clinical findings peculiar to Le Fort II type fractures- Step deformity at infraorbital margins- Mobility of midface detectable at nasal bridge and infraorbital margins- Anesthesia or paresthesia of cheek- Possible diplopia- Pupils tend to be level unless there is gross unilateral enophthalmos- Nasal bones move with midface as a whole but often otherwise intact- Cerebrospinal fluid rhinorrhea may not be clinically delectable- No tenderness over, or disorganization and mobility of zygomatic bones and arch
VII. Le Fort III fracture:Summary of Signs and svmptoms peculiar to Le Fort III fractures:1- Tenderness and separation at fronto-zygomatic suture.2-Tenderness and deformity of zygomatic arch.3- Lengthening of face "Dish-face"4- Depression of ocular levels (hypoglobus).5- Enophthalmos.6-Hooding of eyes (pseudoptosis).7-Lengthening and sometimes extreme disorganization of nasal skeleton.8- Often cerebrospinal fluid rhinorrhea.9-Tilting of occlusal plane with gagging on one side only.10-Lateral displacement of midline of upper jaw.11- Mobility of whole of facial skeleton as a single block.
Cerebrospinal fluid rhinorrhea (CSF rhinorrhea):salty or metallic taste.In most instances CSF leak arrest within few days, either spontaneously or as a result of reduction and fixation of the #. Whenever there is a tear in the dura mater there is a risk of meningitis either in the early days after injury or even many years later.
Detection:
• halo of ring line on pillow
• 2. Glucose level using glucose oxidase sticks, however, so does lacrimal fluid which contain glucose also (unreliable test). The quantity of glucose can be detected using Dextrostix as CSF has a much higher glucose content. However, it is of no value in the bleeding nose.3. Protein content of CSF (of no use because it is impossible to obtain uncontaminated samples of CSF).4. Radioactive isotope preparation such as 11In DTPA administered intrathecaland detected subsequently in the nasal cavity or gastric contents.


Note: As a prophylactic measure, we shouldn't give penicillin because it doesn't cross the blood-meningeal barrier in effective concentration so we should give the patient:
2g sulphadiazine
followed by Ig, 6- hourly
and continue the course until 48 hours after any CSF leak has ceased to prevent meningitis.
radiographical examination of MTFS:1. Intraoral views (periapical and occlusal)2. Extraoral views: a- Occipito mental 15', 30 and 45 c- Postero-anterior PA view) d- True lateral (to midface, skull vault to include the cervical spine, and soft tissue) e- Orthopantomogram (OPG) f- Ocipiofontal 25º, Fronto occipital (Townes projection) for stull vault g- CT scan h- MRI
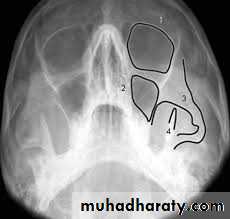
The 'elephant's head approach to the assessment of zygomatic fractures. Fracture lines are commonly seen at:
(1) infraorbital rim
(2) frontozygomatic suture region
(3) lateral wall of the maxillary antrum (zygomatic buttress) and the zygomatic arch ('trunk).
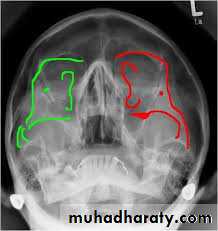
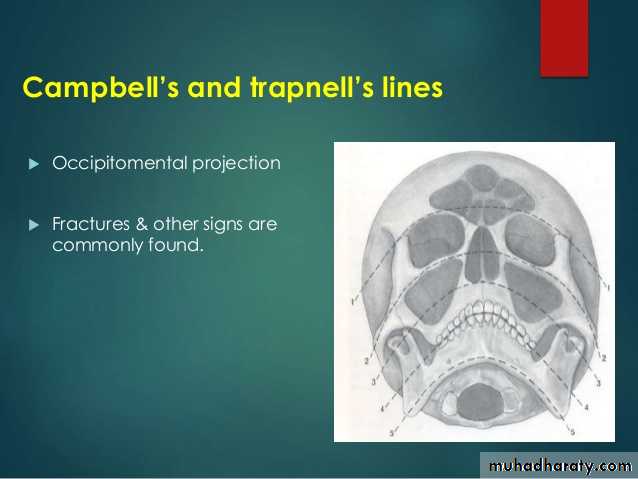
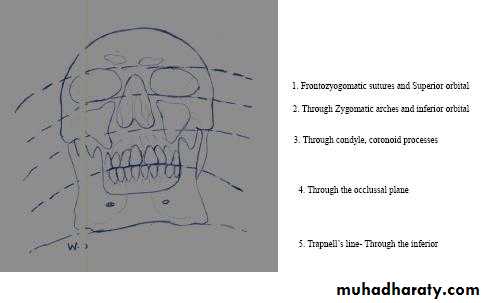
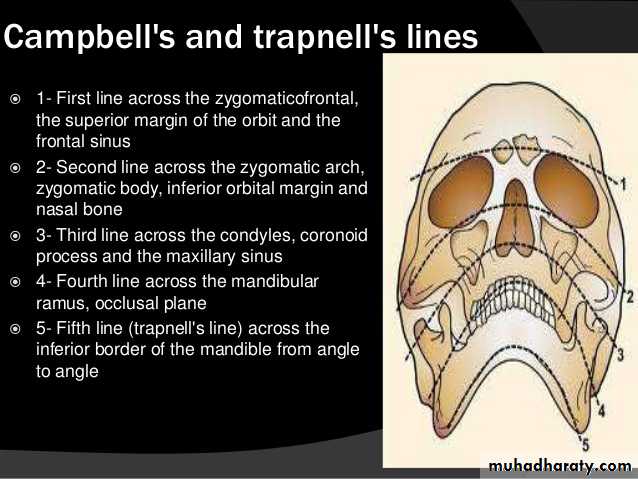
(a) The 4 search lines (Campbell's lines) that can be systematically followed as an aid in interpreting occipitomental radiographs
(b) The 5th liner by Trap Nell OM radiograph of a patient with Le Fort Il and IIl type fracture
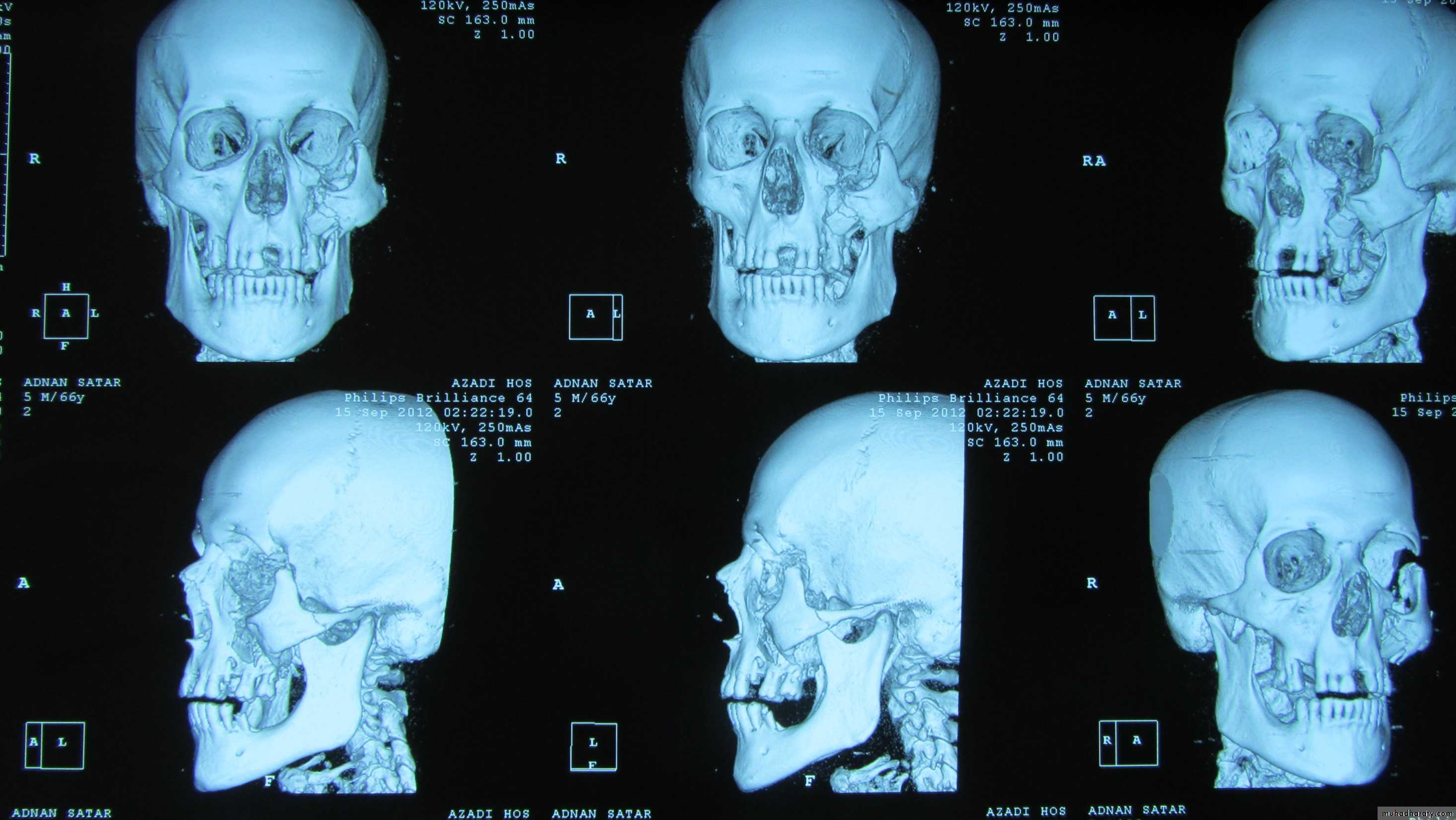
Main indications for CT in macillofacial trauma 1. Suspected or obvious fracture of the frontal bone. 2. Extensive fractures of the midface (including naso-orbito-ethmoid andcomminuted zygomatic complex fractures). 3. Isolated orbital trauma. 4. Displaced condylar neck fractures and complex injuries to the temporomandibular joint. 5. Comminuted fractures of the mandible requiring complex repair. 6. Suspected pathological fracture of the mandible.
Definitive treatment of MTFS fractures:The definitive treatment is varying according to the type of fracture.Steps (principles) of definitive treatment of fractures:a- Reduction (manual, elastic traction or wires)b-Fixation and immobilizationc- Follow up and rehabilitation
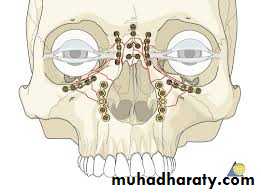
Diagram to illustrate sequencing of multiple facial fracture repair. The outer circle defines the frame' of stronger bones that are reduced and immobilize first (frontal bone, lateral orbitalmargins, zygomas and mandible). The middle circle contains the 'contents' of this frame (essentially the maxillae) that are reduced and repaired next, and finally the nasal complex (inner circle) is resorted.
Dentoalveolar fractures:
zygomatic complex fractures:Zygomatic complex fractures with minimal displacement that are not causingsymptoms do not necessarily require treatment. The indications for treatment are asfollows:1. To restore the normal contour of the face both for cosmetic (relative) reasons and to re-establish skeletal protection for the globe of the eye.2. To correct diplopia.3. To remove any interference with the range of movement of the mandible.
4. when patient has enophthalmos 5. When pressure on the infraorbital nerve results in significant numbness orparesthesia.
symptomless zygomatic complex factures with minimal displacement doesn't require treatment. Sometimes a severely displaced zygomatic bone is left untreated if the patient is old and medically compromised.
Reduction:-The optimum time for reduction of a fractured zygoma is between the 5th -10thpost injury day this allows the gross edema to disperse, permit good assessment todiplopia, provide an improved radiographs, and hematoma has not started to organize into fibrous tissue).
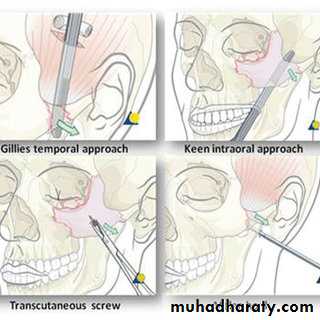
Reduction of a recent fracture is carried out by:1. Gillis approach, (1927 still the method of choice)
• 2. Iintra-oral approach (Keen 1909)
Quinn, 1977 described a modification for correction of the medially displacedzygomatic arch. This employs a lateral coronoid approach through an incision over the anterior border of the ramus, a finger inserted into the wound, then an elevator inserted medial to the arch and moved anteroposterior. The disadvantage of intraoral approach is the possible herniation of buccal pad of fat.
3. Percutaneous approach (Poswillo, 1976).
4. Intranasal transantral approach.
Fixation:-Following reduction, the bone may be stable or additional fixation is required.Instability of the fragment commonly occurs when there has been delay in treatment; the fractured ends of the bone tend to become rounded off by osteoclastic activity (eburnation) and after the zygomatic bone has been elevated into place it falls back into its original position, so it needs fixation.
Methods of Fixation :1- Transosseous wiring at the frontozgomatic suture (Crow's-foot). 2-Transosseous wiring at the zygomatico-maxillary suture line (infra-orbital rim):



3-A combination of lateral& infra-orbital rim wiring.4-Fixation with a pack in the maxillary sinus: (Temporary Support)
5-Pin fixation from zygomatic bone to the supra-ortbital rim:Is especially useful for:A- Excessively mobile zygoma.B- Following surgical refracture of a badly displaced zygomatic bone which has healed.
Fracture of the zygomatic arch:If the zygomatic arch alone is fractured, the fragments should be reduced via a Gillis approach. Fixation is unnecessary as the temporalis fascia attach along the superior aspect of the arch will effectively immobilize the fragments (in recent fracture)
Fractures of the orbital floor (Blow out fracture):Treatment is indicated if there is:1. Diplopia which does not resolve significantly during the first 10 days after injury.2. A fracture with a large herniation of tissue into the antrum.3. Incarceration of tissue sufficient to cause globe retraction and increase in intra ocular pressure on upward gaze.4. Significant exophthalmos (greater than 3mm).


Indications and relative contraindications for orbital floor repairIndications1. Significant restriction of eye movement (diplopia) with CT confirmation ofentrapment2. Significant enophthalmos (greater than 3 mm)3. Large 'blowout' defect (large herniation into the antrum)4. Significant orbital dystopia
Relative contraindications1. Visual impairment2. Anticoagulant medication3. Patient unconcerned4. Proptosis5. An already at 'risk' globe
Surgery in the form of grafting (bone graft or implant) the orbital floor mostly used for correction of orbital floor fracture. However, grafting of the orbital floor may lead to postoperative complications as:
persistent enophthalmos,
persistent diplopia in vertical gaze
persistent edema of the lower eye-lid
infection and chronic fistula,extrusion of the implant (alloplastic sheets),
dacryocystitis,
depression of the globe,tissue reaction to the implant,
intra-orbital hemorrhage,
and blindness.
Possible complications of orbital floor exploration- Intraorbital hemorrhage- Lower eyelid retraction and ectropion- Persistent edema of lower eyelid- Persistent enophthalmos- Persistent globe depression- Persistent diplopia in vertical gaze- Tissue reaction to implant- Extrusion of implant- Infection and chronic fistula formation- Dacryocystitis- Blindness
Nasal complex fracture:Reduction:

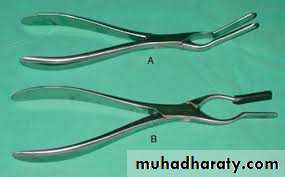
Fixation:-
1. The most commonly used splint is a plaster-of-Paris splint2. If the nasal fracture is too mobile, a lead plate splint on either side of the nose is used
3. Open reduction and direct wiring of the fragments for certain complicated naso-ethmoidal fractures.
Reduction of Le Fort Fractures:The optimum time for reduction of midface fractures is usually between the 5th-8th post injury days.Le Fort I fracture:


Le Fort Il fracture:Le Fort III fracture:

Immobilization of Le Fort I, II and Ill type fractures :.The fixation of a mobile fracture of the MTFS presents a difficult problem because there is no suitable adjacent structure to which it can be immobilized.Forms of immobilization may be classified as follows:A- Extra-oral immobilizationB- Immobilization within the tissues
A-Extra-oral immobilization:1. CRANIOMANDIBULARa. "Box-frame" systemb. "Halo-frame"c. Plaster-of-Paris headcap2. CRANIOMAXILLARYa. Supra-orbital pinsb. Zygomatic pinsc. "Halo-frame"3. SUSPENSIONFrom "halo-frame"or plaster-of-Paris headcap using cheek wireB- Immobilization within the tissues:
B- Immobilization within the tissues
1. DIRECT FIXATIONa. Transosseous wiring of fracture sites:i. Frontozygomaticii. Infira-orbitalii. Midline of palateb. Transfixation with kirschner wire or Steinmann pini. Transfacialii. Zygomaticoseptal
2. INTERNAL WIRE SUSPENSIONf. Nasal septum mandibulara. Circumzygomatico-mandibular b. Zygomatico-mandibularc. Inferior orbital border- mandibulard. Frontomandibulare. Pyriform -circummandibular3. SUPPORTa. Antral packb. Antral balloonc. External acrylic splintd. Silicone elastomer wedge
Extra oral immobilization:* suspension from plaster-of Paris head cap:Some surgeons prefer to use halo frame
Indirect skeletal pin fixation:
Disadvantages:All are cumbersome, conspicuous, and may lengthen the period of hospitalization.
Immobilization within the tissues:Advantages of this method over the extra oral means:-1-No need for special laboratory work for construction of splints.2- Invisible and less postoperative discomfort.3-The patient can be discharged from the hospital earlier.4- Suitable for cerebrally irritated or mentally retarded patient.
Types of immobilization within the tissues:1. Direct fixation:
2. Internal wire suspension:Advantages:To the patient comfortable, well-tolerated and inconspicuousTo the surgeon rapid, accurate, dependable, and technical facilities are notrequired.
Disadvantages:* Is not a rigid fixation*Oblique upward and backward pull (in lateral frontal & , circumzygomaticsuspension) which may lead to subsequent relapse.
The suspension achieved by:-a-Fronto-mandibular:b-Zygomatico-mandibular:c-Circumzygomatico-mandibular:d-Infra orbital-mandibular:e- Pyriform fossa-mandibular:f-Nasal septum-mandibular:
3. Support:a. Antral pack:To support zygomatic bone or orbital blow-ou fracturesb. Antral balloons:Produce uniform pressure and may cause ischemic necrosis of antral mucosa.c. Silicone elastomer wedged. External acrylic splint
Various incisions used for surgical access to the orbito-zygomatic region. (a) Coronal or hemi- coronal. (b) Extended preauricular. (e) Lateral brow. (d) Supratarsal fold. (e) Lateral canthus. (0 Subciliary. (g) Midtarsal. (b) Transconjunctival. (i) Paranasal.
Surical approaches to midface and upper face fracture1.incisions for surgical exposure of the maxilla
a. Vestibular b. Palatal c. Midface degloving procedure
2-Incisions for surgical exposure of the zygomatic complex and orbit)a. Supero-lateral orbital rim-Lateral eyebrow-Supratarsal fold-Extended preauricular-Coronal and hemi-coronal (scalp flap)b. Lateral orbital rim, body and arch of zygoma-Lateral canthal (crow's foot crease)-Extended preauricular-Coronal and hemi-coronal (scalp flap)
c. Inferior orbital rim and orbital floor-Midtarsal or orbital rim-Subciliary (lower blepharoplasty')-Transconjunctival (with or without lateral canthotomy)d. Medial orbital wall-Paranasal (Lynch incision)-Transcaruncular(+/- transconjunctival approach)
3. Incisions for surgical exposure the frontonasal regiona. Local skin incisions (forehead, paranasal or nasal bridge)b. Coronal (bi-temporal scalp flap)
Late complications of fractures of the MTFS:Complications from the Head Injuries:1. Postconcusional syndromeconsist of headache, insomnia, diplopia,intolerance to noise, changes in disposition, intellectual impairment andintolerance to alcohol.2. Aerocele or a cerebral abscess within few weeks of the accident3. Meningitis4. Epilepsy occasionally develops
Complications arising from the Fracture:1. Bony Deformity: this may be cosmetic deformity or may, in addition, be functional problems.1- Flattening of the zygomatic complex2- Dish-face deformity
3- Considerable deformity of the orbit and forehead.4- Mis-shapen nose,
2. The lacrimal system: Epiphora and Dacryocystitis
3. Ophthalmic Complication:Residual ophthalmic problems arise from 3main causes deformity of bony orbit, neurological damage, and damage to the globe of the eye and its soft-tissue adnexae.1- Diplopia and enophthalmos.2- Strabismus, ptosis, superior orbital fissure syndrome which consist of(ophthalmoplegia, ptosis, proptosis and fixed dilated pupils), partial orcomplete blindness (orbital apex syndrome) as a result of optic nerve damage.3- Disturbances of vision and diplopia caused by direct muscle damage
4. Other Neurological Damage:1- Anosmia as a result of fracture of cribriform plate of the ethmoid.2- Anaesthesia or paraesthesia of the cheek, upper lip and maxillary teeth.5. Non-union:
Possible components of post-traumatic deformity in inadequately treated severe actual midface fractures:1. Retrusion of upper dentition.2. Anterior or lateral open bite.3. Intraoral fistulae into nose or maxillary Sinus.4. Expansion or contraction of the orbital volume.5. Orbital dystopia.6. Tethering of ocular muscles.7. Depression of the nasal bridge.
8. Deviation of the nasal septum.9. Telecanthus.10. Obstruction of drainage of the paranasal sinuses, particularly maxillary andfrontal.11. Contour deficiency of the frontal bone with distortion of the orbital roof.12. Persistent cerebrospinal rhinorrhea.13. Varying degrees of soft tissue scarring and mal-alignment.