Theories of caries reduction by fluoride:
Lec.4 Dr.Jihan Abdulhussein
The precise and complete mechanisms of actions of F in relation to dental
caries are not fully understood. There are three theories present
explaining the role.
1st theory (pre eruptive theory):
This is a widely accepted theory claims that when F is taken during the
period of tooth formation it may cause changes in composition and
morphology of teeth. Fluoride ion may replace the hydroxyl group of the
hydroxyl apatite crystal forming a new crystal known as fluoroapatite
crystal.
Ca10 (PO4)6 OH2 + 2F-
Ca10 (PO4)6 F2+ 2OH-
This reaction is irreversible that is to say once fluoroapatite crystal is
formed it will remain so for the life time. The new crystal is more stable
and less soluble, and more resistance to acid dissolution. Thus fluoride
improves the crystallinaty of teeth. These teeth have more rounded cusps
and shallower pits and fissures, thus reduce the predisposing factor for
dental caries.
Ingestion of fluoride in the pre eruptive stage will allow the incorporation
of F in the whole enamel and dentin. This will increase the resistance
against dental caries in addition reduces the progression of dental caries.
2
nd
theory (post eruptive theory):
When F is present in saliva and dental plaque, it will react with the outer
enamel surface to enhance re mineralization. Two types of reaction may
develop, the main reaction is formation of calcium fluoride, while the 2
nd
type of reaction is the formation of fluoroapatite crystal.
Ca10 (PO4)6 OH2 + 20F-
CaF2 + 6(PO4)3- +2OH-
Ca10 (PO4)6 OH2 + 2F-
Ca10 (PO4)6 F2+ 2OH-
Calcium fluoride is not permanent as it dissociated to calcium and F ions.
There for fluoridated products need to be applied continually and at a
high concentration, otherwise the enamel will be opened to renewed
demineralization. These types of reactions can be initiated at any time of
subject life.
3
rd
theory (antibacterial theory):
The presence of F in high concentration (more than 40 ppm) in dental
plaque may affect the growth and fermentation of bacteria. These by:
Interference with bacterial adherence by retardation of extra
cellular poly saccharide.
F affect metabolism of bacteria by inhibition of intercellular
enzymes as enolase and phosphotase.
Change the microbial composition of dental plaque.
The general Mechanisms of fluoride Action by which reduces dental
caries involve:
1. Increased enamel resistance or reducing enamel solubility [acid
dissolution].
2. Interferes in the formation and functioning of dental plaque
microorganisms.
3. Increases the rate of post-eruptive maturation.
4. Remineralization of incipient lesions.
5. Improves tooth morphology.
1- Increased enamel resistance or reducing enamel solubility [acid
dissolution]. Caries process involves dissolutions of enamel by
acids from bacterial plaque. This dissolution inhibited by the
presence of fluoride. When enamel is exposed to acid (pH less than
5.5) it will dissolve to its ionic form (Ca, HPO4, OH), this occurs
beneath bacterial plaque. The concentrations of calcium, phosphate
and other ions in the solution will increase. When plaque stop
producing acid, the pH will raise and the dissolved minerals get
participated in the outer enamel surface. Thus the carious process is
a cyclic phenomenon consisting of phases of demineralization and
re precipitation. The presence of fluoride reduces the solubility of
enamel by promoting the precipitations in the form of fluoroapatite
crystals and calcium fluoride.
Ca10 (PO4)6 (OH)2 + 2F-
Ca10 (PO4)6 F2 + 2OH
Ca10 (PO4)6 (OH)2 + 20F-
10CaF2 + 6(PO4)-3 +2OH-
2- Interferes in the formation and functioning of dental plaque
microorganisms. In high concentration F is bactericidal, thus reduces
plaque. In relatively low concentration, fluoride is bacteriostatic,
affecting growth of bacteria.
3- Increased rate of post-eruptive maturation
At the time of tooth eruption the enamel is not completely calcified and
undergoes a post-eruptive period of approximately 2 years during which
enamel calcification continues. Throughout this period-period of enamel
maturation’ there is continuous accumulation of fluoride as well as other
elements in the superficial part of enamel.
4- Remineralization of incipient lesions. By depositions of minerals in
to previously damaged areas, this will also lead to reduce solubility.
Fluoride enhances the re mineralization process by accelerating the
growth of enamel crystals that have been demineralized by caries process.
5- Improves tooth morphology: Ingestion of fluoride during the period
of tooth formation lead to changes in tooth morphology as smaller cusps
depth of teeth turn to more self-cleansing area.

Systemic fluoridation
History:
at the beginning of the 20th century (1901), Dr Fredrick Mckay noticed
that many of his patients who had lived in Colorado spring (Colorado
USA) had a permanent stain on their teeth named as Colorado stain. He
noticed also it low caries severity among those patients. In 1902 Eager
noticed the same stain upon Italian people migrates from Naples, Italy.
He found that only people born and lived all their lives in that area had
this deformity that is mottled teeth. In 1931, Churchill showed a presence
of high concentration of F in area with mottled teeth, but yet no
correlation was found. Trendily Dean discovered that F concentration in
drinking water affected the severity of mottling and dental caries severity.
He conducted a series of studies regarding level of F in water and severity
of dental caries in 21 cities among 7257 person, 12-14 year olds. Two
important conclusions were reached:
-The number of carious teeth and concentration of fluoride is inversely
related.
-The amount of F in the water and mottled enamel are directly
related. The condition of mottled enamel was changed to endemic dental
fluorosis.
Dental fluorosis
:
It is a developmental hypoplastic defect caused by excessive fluoridation
during the period of tooth formation. It is the 1st sign of chronic toxicity
appears clinically as a white spots or lines involving incisal edge or cusps
of posterior teeth or as a white opaque or brown area,in individuals with
moderate dental fluorosis, yellow to light brown staining observed in the
areas of enamel damage which involve the entire tooth. In severe cases
acorroded appearance will occur. Changes in human enamel have been
examined using light and electron microscopy. In principle, increased
exposure to F during period of tooth formation leads to increase enamel
porosity. In severe cases the fluorotic teeth are highly porous because of
increase of inter crystalline spaces these spaces are occupied by water and
protein more than enamel. The fluorosed teeth contain more immature
protein. In more sever condition changes involve enamel as well as
dentin. After eruption of teeth, although the surface layer is well

mineralized it is susceptible to mechanical trauma leading to break down
of the outer enamel surfaces.
The exact cause of this hypoplasia is not clear it may be attributed to:
1- altered metabolism in any or all phase of the enamel formation.
2- altered ameloplastic activity.
3- Interference with crystal nucleation or growth.
4- faulty enzymatic factor.
Factors affecting severity of dental fluorosis:
1- Fluoride concentration in drinking water: a direct relation ship
is present between dental fluorosis and level of F ingested.
2- Total amount of fluoride ingested: F ingested from water, food,
inhalation because of pollution all affect severity of dental
fluorosis. The total amount of water intake is affected by
temperature. In hot area, there is an increase ingestion of F due to
increase intake of water thus increasing the risk of dental fluorosis,
the opposite is true in cold area.
3- Duration of exposure to fluoride: excessive intake of F for a
long time as eight years during the period of tooth formation may
increase the severity of dental fluorosis. teeth mineralized early in
life develop less dental fluorosis, thus posterior are affected more
than anterior, also primary teeth are affect less severely compared
to permanent teeth, due to shorter maturation period. In addition
enamel maturation and calcification of primary teeth take place in
the intra uterine life, and the placenta do regulated the amount of F
reaching the fetus, also F concentrated in bones of the mother and
the fetus more than teeth.
4- Others: dental fluorosis was found to increase among children
with mal nourishment. The exact cause for this is not clear.
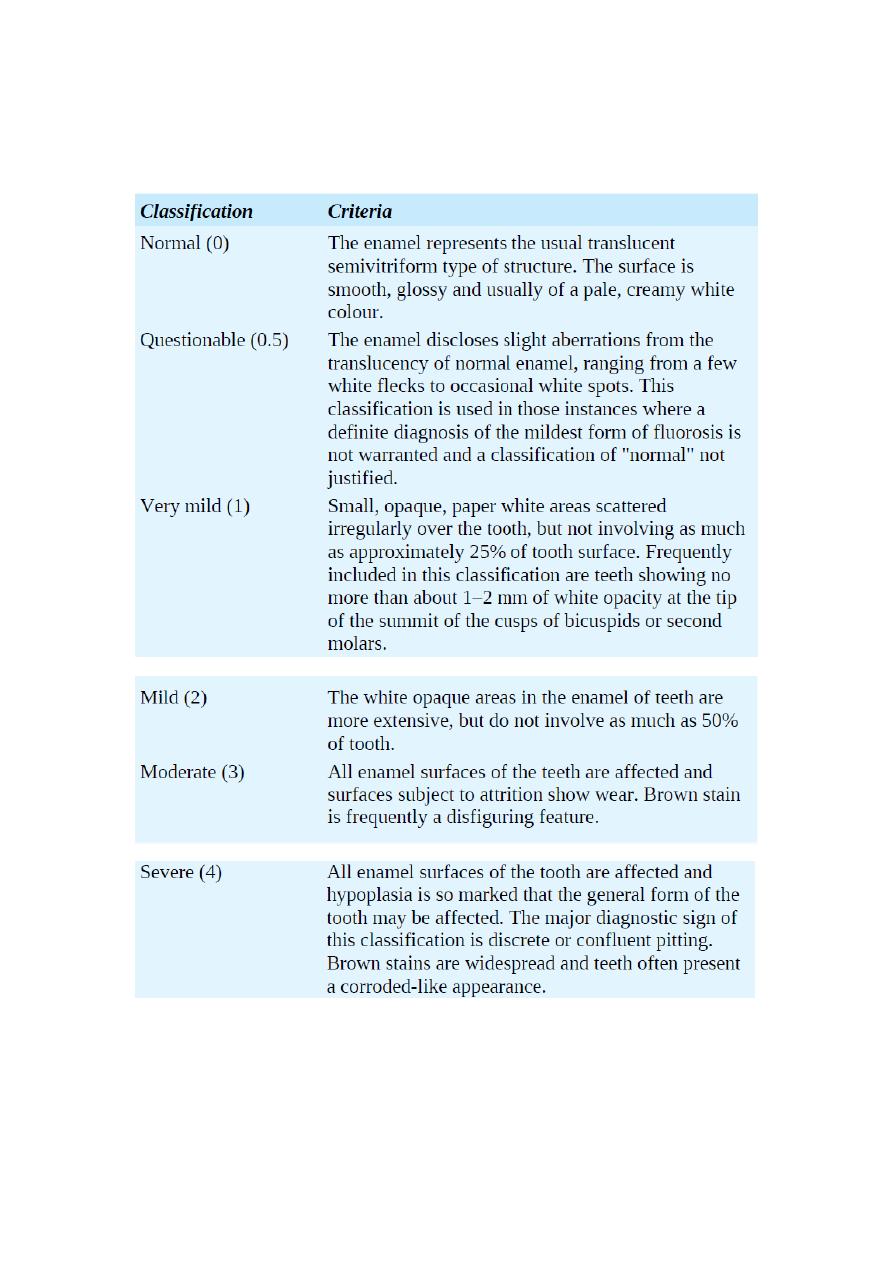
Classification of dental fluorosis:
Treatment of dental fluorosis:
The damage of dental fluorosis is permanent, thus preventing of this
hypoplasia is much more important. This is by defluoridation of high

fluoride content and avoiding chronic fluoride toxicity. The treatment of
dental fluorosis is:
Bleaching for the mildest form
Composite restorations combined with Microabrasion or aesthetic
veneers for moderate fluorosis
Prosthetic crowns for sever form
T
he optimal level of fluoride:
Dean conducted his study among 7257, 12 - 14 year- old in seven cities in
USA. This was to explore the association between F level in drinking
water and severity of both dental caries and dental fluorosis. In measuring
dental fluorosis a special index was applied called Community Index of
Dental Fluorosis, dividing the condition in to different categories
according to severity by weight (normal, questionable, very mild, mild,
moderate and sever). While the DMF index was applied for recording
dental caries.
Results revealed a maximum reduction of dental caries at a level of F of
(1 ppm). At this level, dental fluorosis will involve 10 % of the
population, but it is of the very mild type with no practical aesthetic
significance. Increasing f level in drinking water will cause a dramatic
increase in dental fluorosis but with no further reduction of dental caries.
Thus the optimal level is (the level of F in drinking water causing
maximum reduction of dental caries but with no clinical signs of dental
fluorosis).
Because people in hot climates drink more water than do those
in moderate climates, thus the optimal level of fluoride was changed to
0.7 - 1.2 ppm (mg/l) according to the temperature. The higher the
average temperature in a community, the lower is the recommended level
of fluoride in drinking water.
Fluoride administration
1- Water fluoridation.
a) Communal water fluoridation
b) School water fluoridation (or home water fluoridation).
2- Dietary fluoride supplements by:

a) Fluoridated tablets (dropings or lozenges).
b) Fluoridated salt.
c) Fluoridated milk (or juice).
d) Fluoride vitamins preparation
Communal water fluoridation:
it is the controlled or artificial adjustment of the level of F in a communal
water supply to achieve maximum reduction of dental caries and
clinically no significant level of fluorosis. Fluoride was 1
st
added to
water supply in 1945 in grand rapids (michigan) while muskegon was the
control. Caries reduction was reported to be 55%. In USA, now more
than 126000,000 people (64%) are receiving systemic fluoridation. It is
also applied in Europe and other countries.
FLUORIDE COMPOUND USED IN WATER FLUORIDATION
1. Fluorspar: It is a mineral containing calcium fluoride [CaF2].
2. Sodium fluoride.
3. Silicofluorides.
4. Sodium silicofluorides: Most commonly used due to its low cost.
Solutions of this compound are corrosive hence materials for piping, etc.
should be chosen accordingly.
5. Hydrofluosilicic acid & Ammonium silicofluoride.
These materials are added to water by an automatic feeding apparatus and
concentration of F is continuously adjusted.
From different epidemiological observation studies concerning water
fluoridation it was concluded that:
1- Artificial water fluoridation is effective in caries reduction in
similarity to naturally fluoridated area.
2- Caries reduction involved primary, permanent teeth as well as root
caries. The reduction is more in permanent teeth compared to
primary because of their shorter maturation period, also its more
reduction in smooth surface rather than occlusal surface.
3- Communal water fluoridation is a public health measure. All
people in the community can gain the benefits from water
fluoridation. No effort is needed by recipients to prevent caries.
4- It is a cheap and successful measure of prevention.
5- A reduction in periodontal disease was also reported in fluoridated
area.
Disadvantages
1. Political and/or emotional objections to water additives.
2. Possibility of mild to moderate fluorosis if other sources of fluoride are
ingested inadvertently.
3. alleged toxicity.
Alternative to systemic water fluoridation
the communal water fluoridation is a successful method for the
prevention of dental caries. In presence of objection against this method
or there is no piped water supply as in rural area, there are alternative
methods to flouride provide systemically. These are:
1- School water fluoridation (or home water fluoridation).
2- Dietary fluoride supplements by:
e) Fluoridated tablets (dropings or lozenges).
f) Fluoridated salt.
g) Fluoridated milk (or juice).
h) Fluoride vitamins preparation
School water fluoridation:
This method was first applied in USA, 1954, in which the F content of the
water supply was adjusted for the prevention of dental caries. The optimal
level of F here is about 4.5 times the optimal amount in the community.
This is because:
1-children spend only a part of their total waking hours in schools.
2-they enter the school at 6- year of age, thus the incisors are no longer at
risk of dental fluorosis.
3-only a part of daily water intake is consumed.
4-there is holiday and weekends.

For all of the above and to compensate for the part exposure to F, the
level of fluoride in school water supply increased.
Special equipment can be used for the addition of F, which should be
adjusted continuously by well-trained employer.
Advantages of school water fluoridation
:
- technically feasible.
- low in cost.
- no effort is needed by the recipients.
The disadvantage of this method
-the fluoridation started late in life, that is at 6 years of age,
-there is an interruption of fluoridation due to holidays and week ends.
A maximum benefit of systemic water fluoridation is by early intake of F
from the first years of life till 13-15 years of age.
The home water fluoridation is also of beneficial in caries prevention
however the level of water is in similarity to communal water
fluoridation.