Dr.Nawaf Al-Neaimy
CABMS ( Internal Medicine )College of Medicine
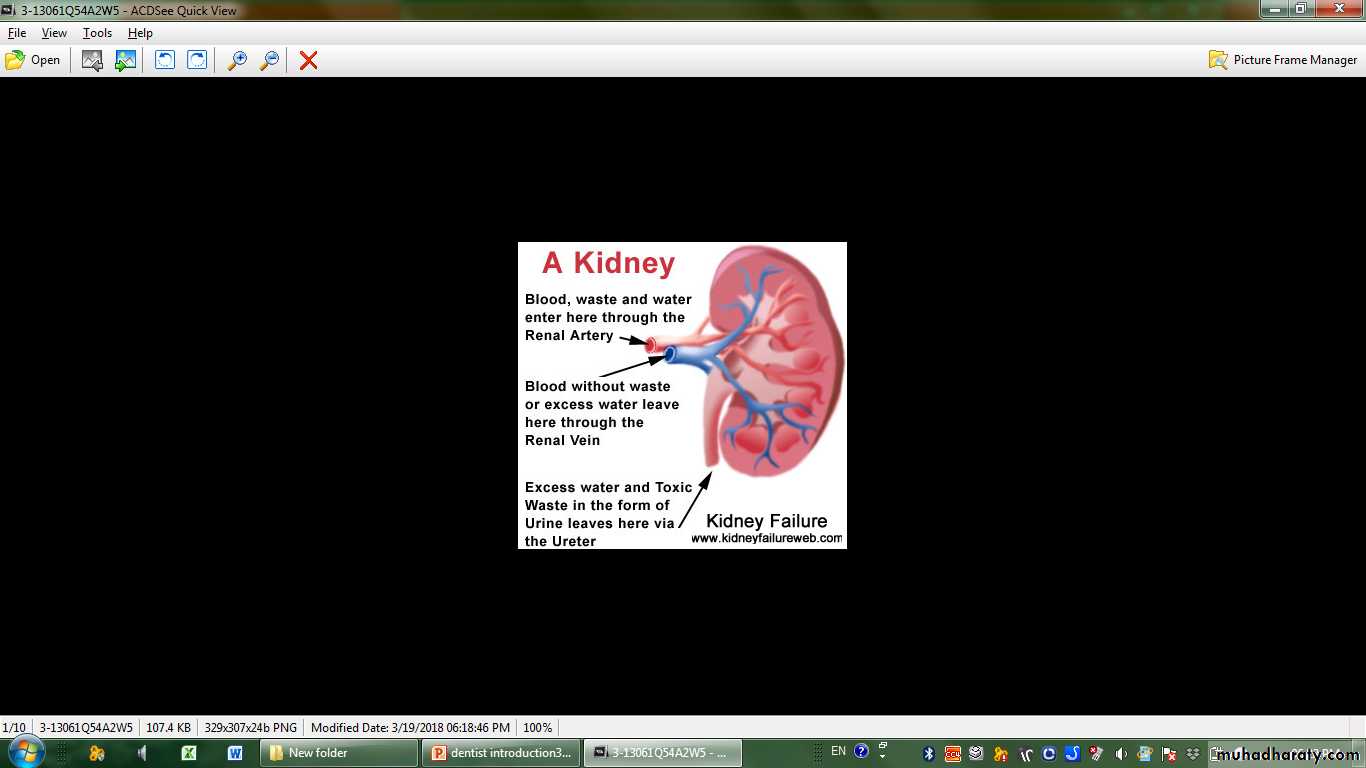
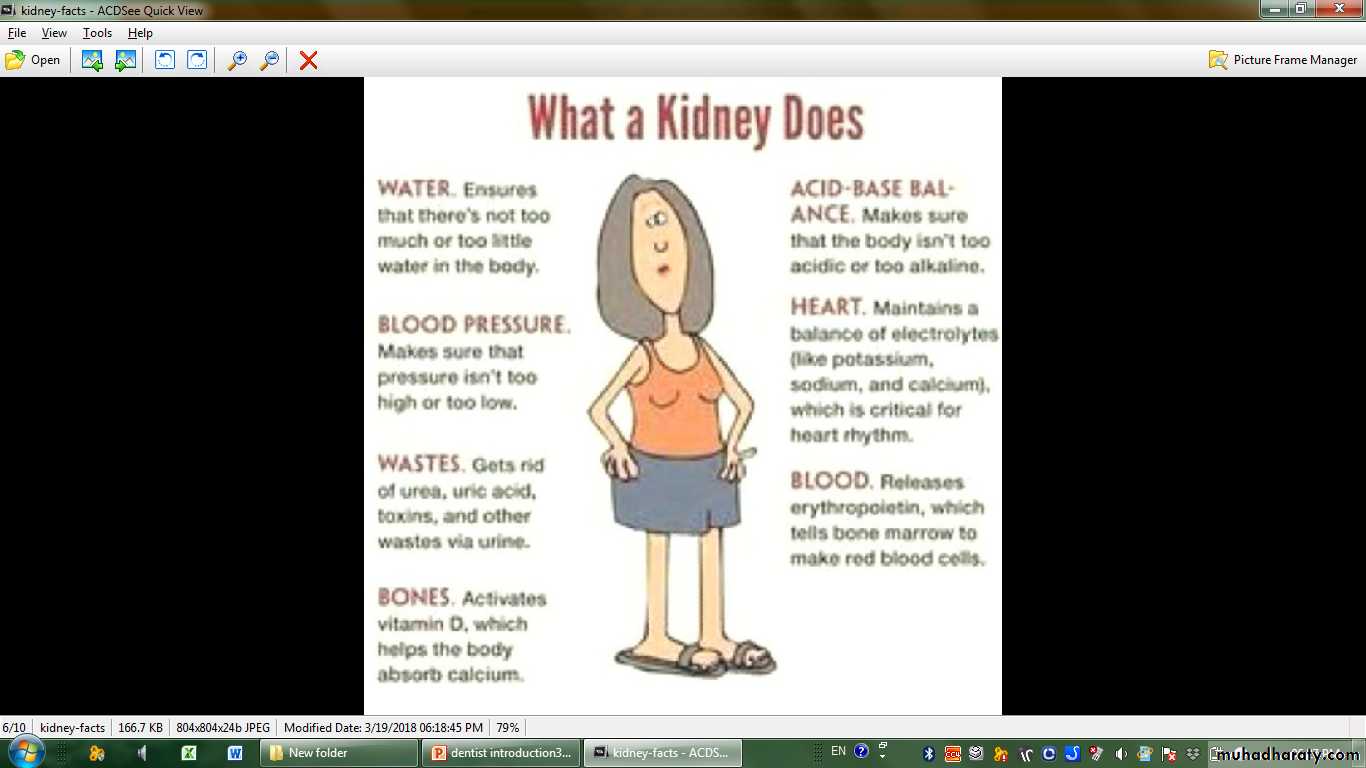
RENAL SYSTEM
Invetigations and oral manifestations of renal diseases
Oedema:
• Means excessive accumulation of fluid especially in the lower limbs.• Renal causes:
• Hypertension:
• Is a common feature of renal disease, on the other hand long term uncontrolled hypertension by itself can increase the risk of evidence of renal failure.
• A) General urine examination: include
• Blood: usually is not present
Glucose: usually is not present
Ketone: usually is not present
Protein: normally not exceed 150 gm./ day
Bilirubin: is not present in normal urine
Urine PH : normally acidic.
Investigations of Urinary Tract
B) Renal function tests1- glomerular filtration rate (GFR): in most renal dieases the GFR is an accurate index of overall renal function (normally= 115-125 ml/min).
2- blood urea: is a poor guide to renal function as it varies with protein intake, liver metabolic state and perfusion (normal range 3.5-6.5)mmol/l
increased in the followings
• A) High intake as high protein diet or GIT hemorrhage
• B) High production: trauma, burn, severe infection
• C) Reduce excretion of urea: hypovolemia, renal failure
3- Creatinine is more reliable guide as it is produced from muscles at a constant rate and almost completely filtered at the kidney.
• ( Normal range 0.6- 1.2 mg/dl)
C) Imaging studies:
1- Plain radiographs (KUB)
• may show renal outlines in prepared patient, opaque calculi and calcification within renal tract can be seen.
2- Renal ultrasound:
• It is a quick non invasive method. It can reveal renal size, shape, position, diltation of collecting system, and also diffrentiate tumour and cyst in addition to other abdominal and pelvic pathology and urinary bladder capacity.
3- CT scan : useful for showing stone, mass and can differentiate between cyst and mass
4- MRI : offer excellent resolution and distinction between different tissues.D) Renal biopsy:
• Is used to establish the nature and extent of renal disease in order to judge the prognosis and need for treatment• Definition:
• a sudden and often reversible loss of renal function, and usually present with oliguria or anuria.• Causes:
• Pre renal: as heart failure, dehydration, sepsis, blood loss.
• Renal: as infection, glomerulonephritis.
• Post renal: as stone, prostatic enlargement.
Acute renal failure
• Any such case need urinary catheterization to exclude obstruction, andto estimate the exact amount of urine.
Oliguria/ Anuria:
means decrease volume of urine
Oliguria → < 400 ml/ day
Anuria → < 100 ml/ day• Definition: irreversible deterioration in renal function which usually occur over a period of years.
• Causes:
• Diabetes mellitus (20-40%)
• Hypertension (5-20%)
• Others: as congenital polycystic kidney, interstitial disease, and glomerulonephritis.
• Unknown ( 5-20%)
Chronic renal failure( Uremia)
• Clinical Features: initially there is biochemical abnormality, but eventually loss of metabolic, endocrine, and excretory functions of the kidney that is called ( Uremia ).
• Diagnosis:
• 1- high b. urea & s. creatinine.
• 2- ultrasound: usually there is small size shrinked kidneys.
• 3- renal biopsy for unexplained cases.
• Management:
• Conservative: initially as cotrol of Bp, and D.M., correction of anemia, fluid and electrolyte imbalance.
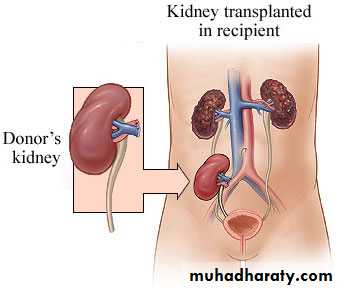
• Renal replacement therapy: by either dialysis or renal transplant.

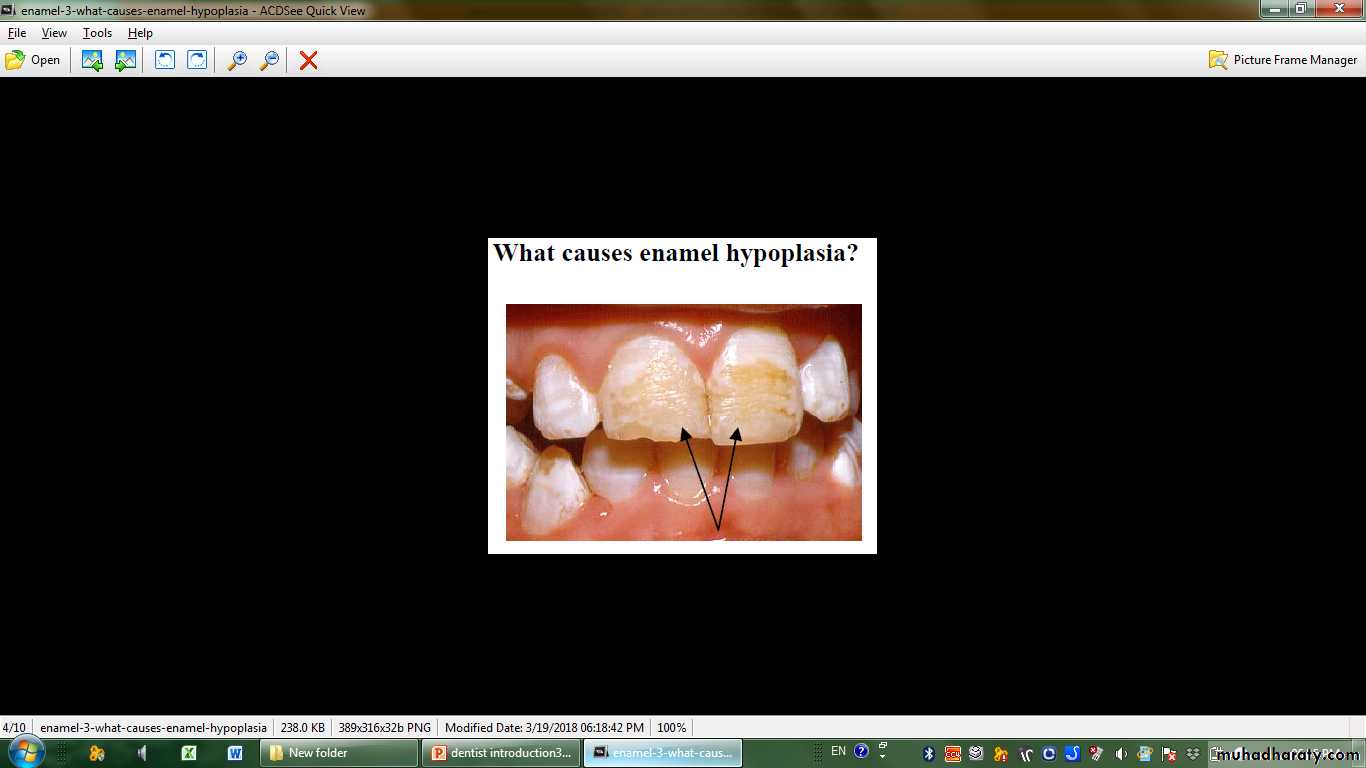
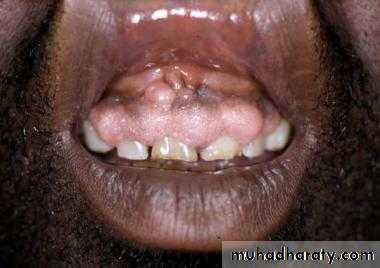
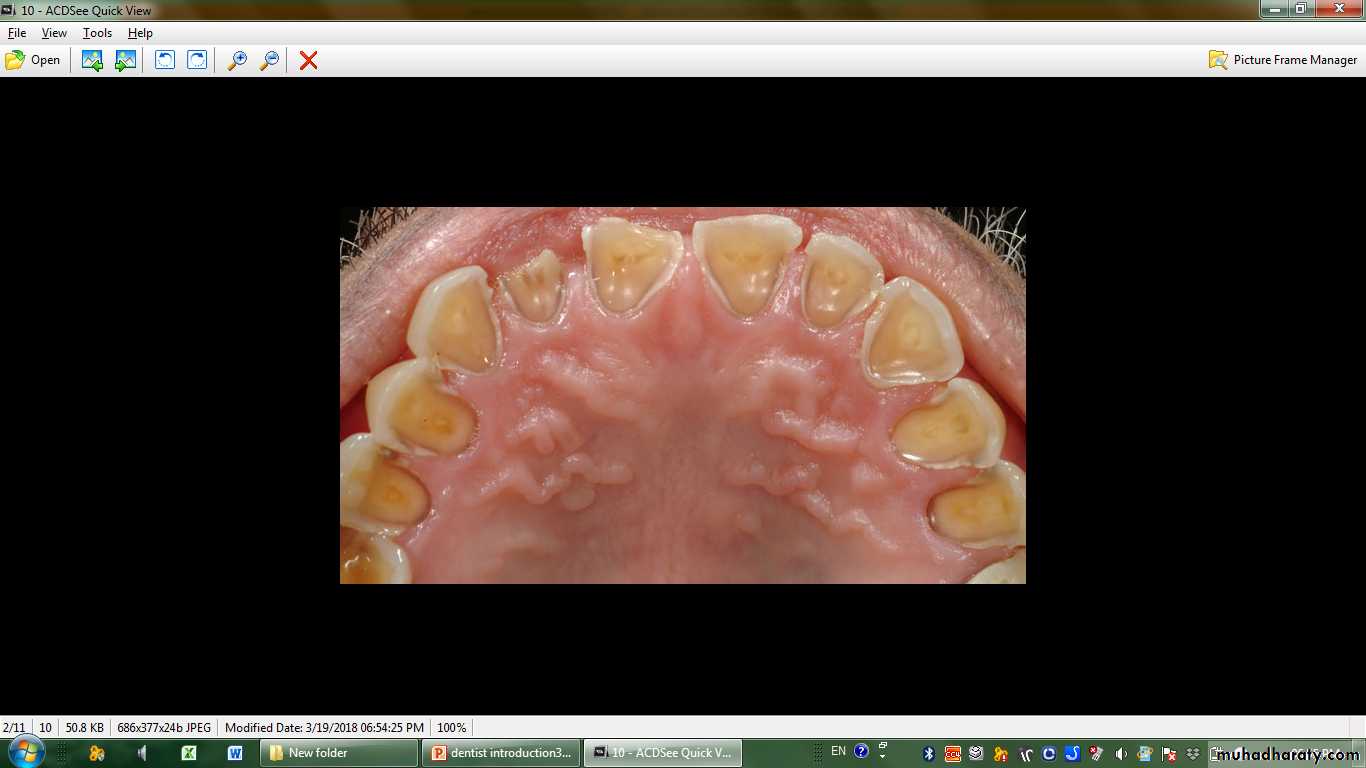
• 1- Dental disorders: occur mainly due to disturb Ca & Po4 metabolism.
Enamel hypoplasiaIn developing dentition: red-brown discoloration and delayed eruption.
Repeated vomiting may result in severe erosions in lingual surface of teeth.
Painful response to percussion, thermal, and electric tests.
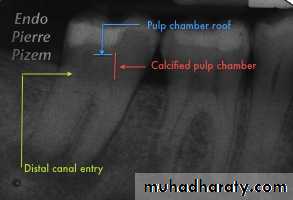
Narrowing of pulp chamber(by meta Ca)
osteodystrophy
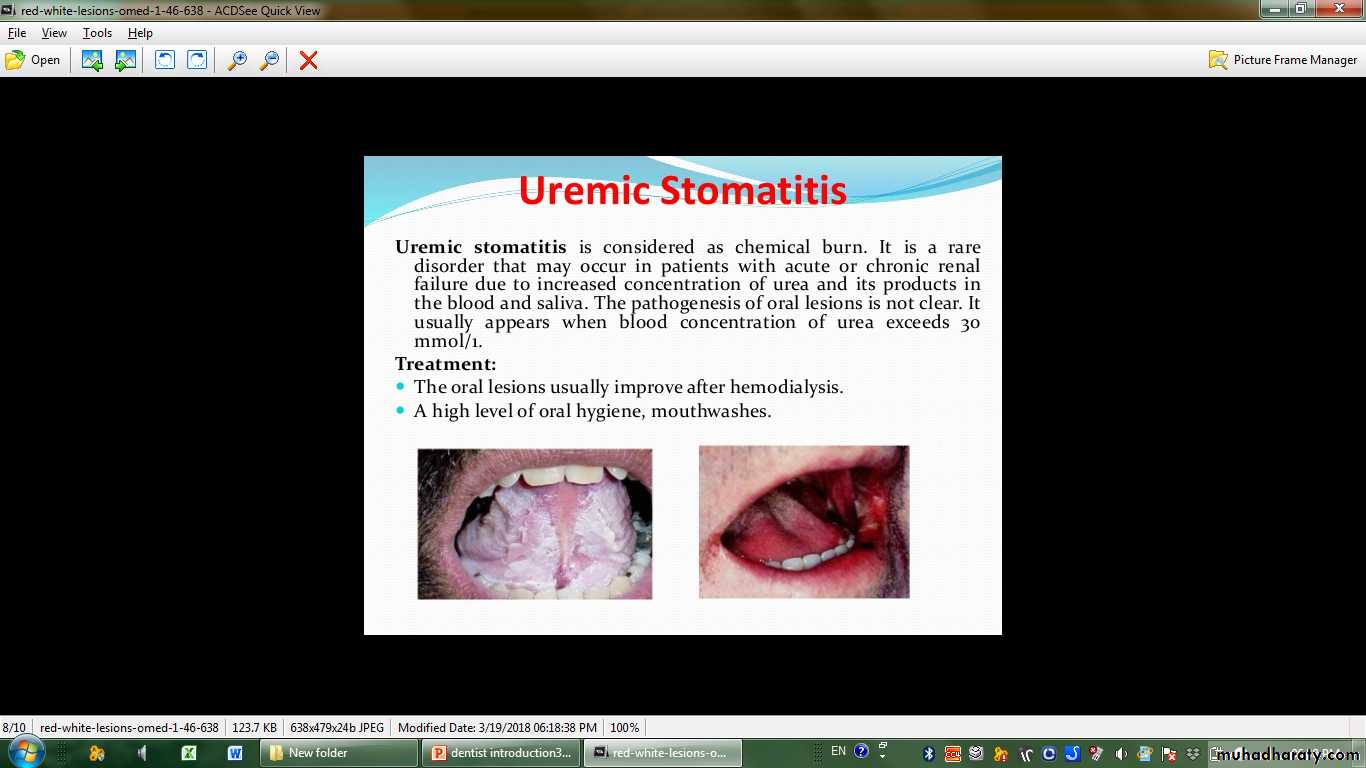
Oral manifestation of uremia:
2- Soft tissue & salivary glands:Bad metalic taste and unpleasant odor in early morning(halitosis:VSCs)
(xerostomia)+/-dysguesia
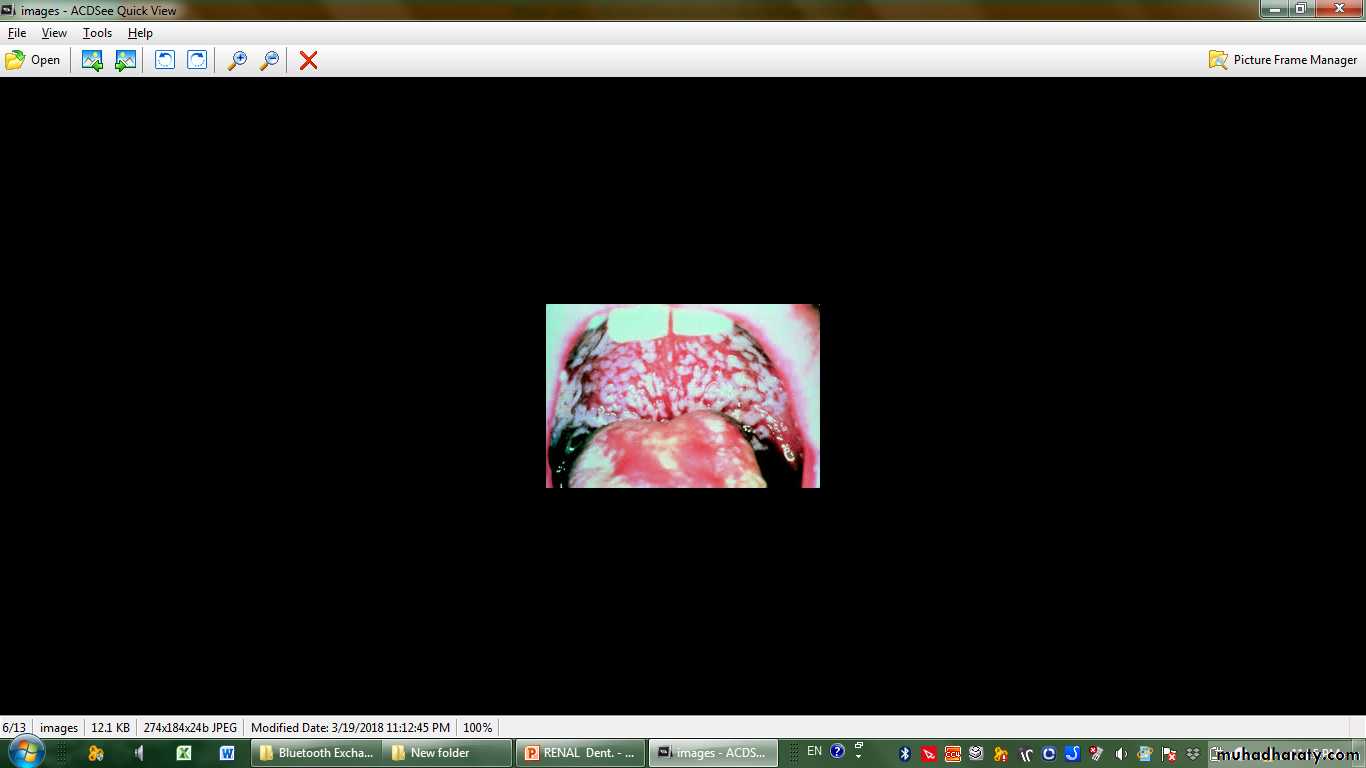
Uremic stomatitis is a rare condition which can exist as a result of sudden rise of b. urea.
It is clinically represents as white plaques distributed predominantly on the buccal mucosa, floor of the mouth and tongue
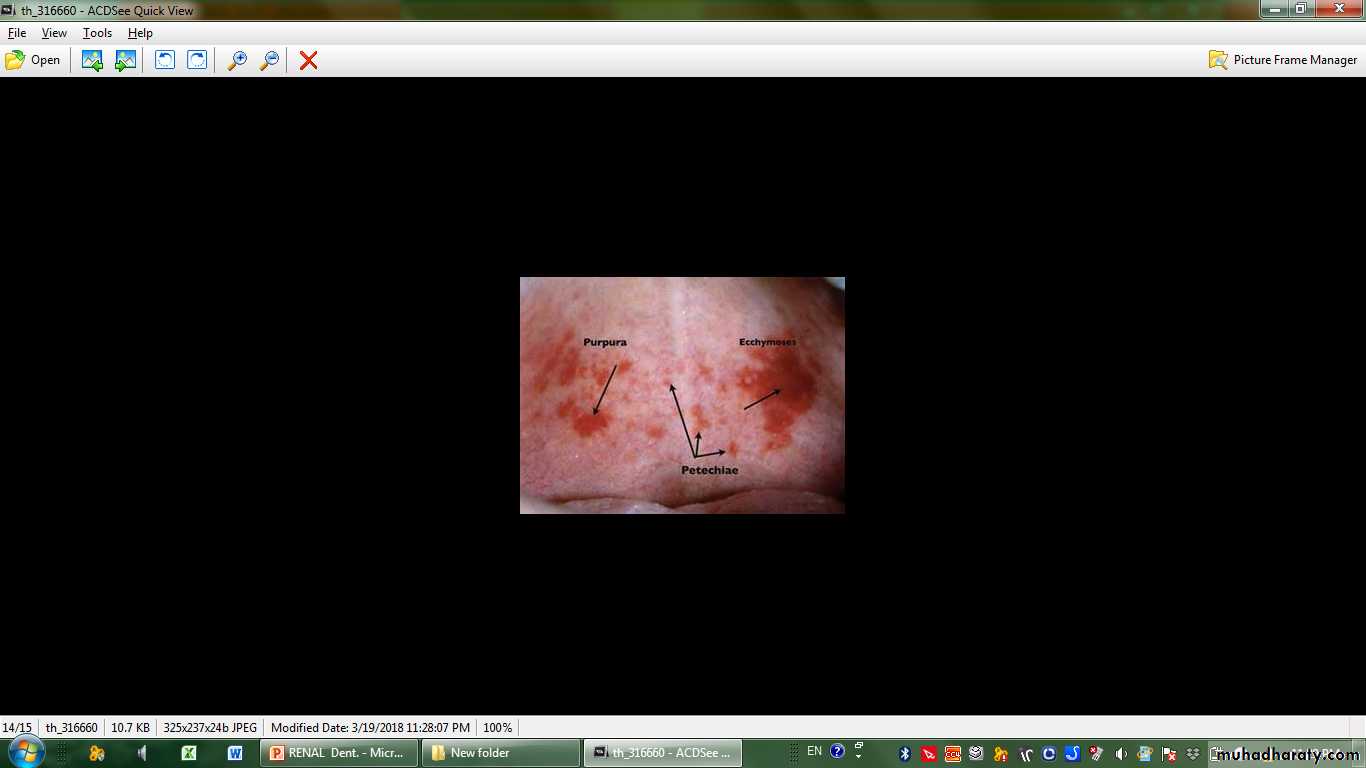
► bleeding(Mucosal Petechiae and Ecchymosis),pallor,
.
3- Post renal trasplant due to immune compromise and drug side effects
(as cyclosporin):
Ugly gum hyperplasia(CCB,cyclosp)
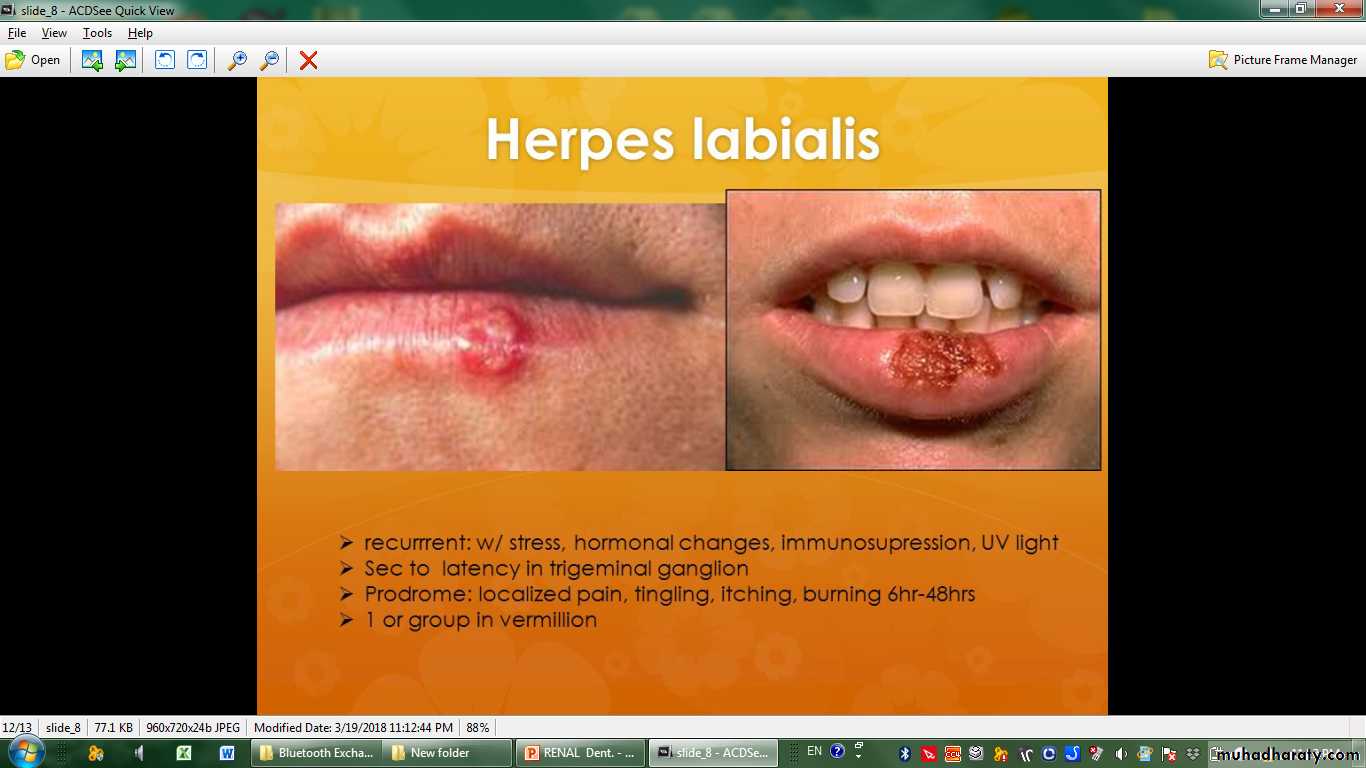
Recurrent viral, bacterial and fungal infections of the oral cavity
Malignancy(OHL.. Esp cyclosporin..reactv EBV; NHL)


DENTAL CONSIDERATIONS
The main management problems in renal failure include the following:
Bleeding Tendencies
Careful hemostasis should be ensured, if oral surgical procedures are necessary. Dental treatment is best carried out on the day after dialysis when there has been maximal benefit from dialysis and the effect of the heparin has worn off. The hematologist should be first consulted. Should bleeding be prolonged, desmopressin may provide hemostasis for up to 4 hours. If this fails, cryoprecipitate may be effective and lasts up to 36 hours. Conjugated estrogens may aid in hemostasis: The effect takes 2 to 5 days to develop, but persists for 30 days
Infections
They are poorly controlled by the patient with renal failure, especially if the patient is immunosuppressed, Hemodialysis predisposes to blood borne viral infection, such as hepatitis virus.Antimicrobials consideration include erythromycin, cloxacillin, fucidin and can be given in standard dosage.
Penicillin, metronidazole and cephaloridine should be given in lower doses


Q) Best test reflect kidney function is:
• Urine analysis
• CT scan
• Serum creatinine
• Ultrasound
• Blood urea.