1
Development of dental caries
Lec.2 Dr. Jihan Abdulhussein
Theories of dental caries
Early theories of caries etiology
The legend of the worm: ancient Sumerian text known as “the legend of
worm” found 5000 BC
Endogenous theories
1) Humoral theory: according to which an imbalance between the
humors of body caused tooth decay. (ancient creeks)
2) Vital theory, a theory that postulated that inflammation arising from
within a defective tooth itself caused a surface lesion. Like a bone
gangrene (18
th
century).
Exogenous theories:
Chemical acid theory On the basis of Robertson in 1835, this theory
proposed that tooth decay was caused by fermentation of food particles
around the teeth.
Parasitic (septic) theory:
This was the first theory that related the micro-organisms with caries
on a causative basis(Dubos, 1854). Accordingly, It was proposed that
even though caries starts purely as a chemical process, but the micro
organisms continued the disintegration in both enamel and dentin.
Modern theories:
Chemico-parasitic theory: (1890): (Acidogenic theory)
Microbiological basis of dental caries, proposed by W.D. Miller in his
book "the microorganisms of human mouth" based on work done in
Robert Koch’s laboratory in berlin.
According to MILLER dental decay is a chemo-parasitic process. It is a
two stage process:
2
1- Decalcification of the enamel which also results in the destruction of
the dentin by acid attack.
2- then in 2nd stage: there is dissolution of the softened residue of (E &
D) by proteolytic action of bacteria.
(acid and parasite) showed that the degradation of carbohydrate-
containing foods resulted in acid formation and was able to demonstrate
this process in vitro with isolated oral bacteria and extracted tooth.
Hence Miller advocated an essential role of 3 factors in the caries
process:
The oral microorganisms, the carbohydrate substrate, and the acid, this
theory is still considered the backbone of current knowledge and
understanding of etiology of dental caries.
Proteolytic theory: by Gottlieb and Gottlieb (1944)
In this theory, the organic or protein elements of tooth (not the inorganic
constituents of enamel) are essential pathways of invasion by
microorganisms; and, caries is essentially a proteolytic process, in which
the microorganisms invade the organic pathways and destroy them while
advancing through them by forming acids.
So certain structures of enamel having high (protein) organic material
composition, like enamel lamellae could serve as a pathway for
microorganism invasion through the enamel.
The acidogenic and the proteolytic theory were addressed in the
proteolysis chelation theory. This theory was put forward by Schwartz
and his co-workers 1955
Chelation: It is a process in which there is complexing of the metal ions
to form complex substance through coordinate covalent bond which
results in:
1- poorly dissociated /or
2- weakly ionized compound

3
Dental caries definition:
It is a multifactorial disease mainly bacterial etiology, characterized by
demineralization of the inorganic portion and destruction of the organic
substance of the tooth.
The carious process affects the mineralized tissues of teeth (enamel,
dentine, and cementum) and caused by action of m.o. on fermentable
carbohydrates in the diet. The disease is often described to be progressive
and if not treated may expand in size and progress to the pulp leading
pulp inflammation thus pain and discomfort and the end result will be
loss of vitality then loss of tooth.
Carious process is complicated; there should be an interaction of several
etiological and predisposing factors for caries to occur, and this may
explain the variation in the susceptibility of individuals to caries process.
There is either mild or moderate challenge to caries attack, usually
affecting deep pits and fissures and approximal surfaces.
Rampant caries on the other hand is a sudden rapid destruction of many
teeth affecting surfaces that relatively immune to caries attack.
Other terms are also present as:
Nursing caries caused by prolonged breast or bottle feeding, especially
during night.
Recurrent or secondary caries: seen in the margins of an old restored
area.
Arrested caries: re mineralized caries lesion.
Dental caries is a multifactorial disease; it is the result of complex
interaction between host, plaque, diet, and time
1- Host factors:
Involves susceptible tooth and saliva, in addition to the subject him/her
self.
Teeth vary in their susceptibility from one surface to other and from one
subject to other.

4
There are several factors affecting tooth susceptibility:
a) Morphology of teeth: susceptible sites
Sites on the tooth which favors plaque retention are prone to decay.
These are
1- Enamel pits and fissures.
2- Approximal enamel smooth surfaces.
3- Cervical margin of teeth.
4- Exposed root surfaces because of gingival recession.
5- Deficient or over hang restoration (recurrent caries).
6- Tooth surfaces adjacent to denture and bridges.
b) Positions of teeth: posterior teeth are labial to be affected by caries
compared to anterior.
c) Composition of teeth, teeth composed of inorganic elements (96%
in enamel, 70% in dentin), organic elements and water.
Composition of teeth is effected by environmental factors (water,
diet and nutrition).
Inorganic components: involve major elements as calcium, phosphate,
hydroxyl group these are the constituents of hydroxy apatite crystals
Ca10(PO4)6(OH)2 .
The Ca/P ratio is 2.15. Any change in this ratio is an indication of
presence of other types of crystals.
There are minor elements in teeth as Zinc, copper, magnesium, fluoride
etc. These elements may incorporate the enamel crystal in substitutions
with one if its major elements as for example substitution of Ca ions by
Mg,
Ca9 Mg (PO4)6(OH)2
Or substitution of the OH by Fluoride ions Ca10(PO4)6F2. These minor
or trace elements may also be adsorbed on the surface of the crystals.

5
This incorporation may take place either in the pre eruptive stage
including all layers of enamel and dentin, or in the post eruptive stage
involving the outer enamel surface only.
Some of these elements when incorporated may increase the resistance of
teeth to dental caries as fluoride ions, tin ions, zinc, strontium, and
molybdenum. While other elements, may increase the susceptibility to
dental caries as magnesium. However, the role of other elements may not
well understood as K, Mn, and Al.
Saliva affects caries etiology through the rate of secretion and
composition. Saliva affects the integrity of teeth by the composition of
(buffer system, calcium and phosphate). By the cleansing action of saliva
(oral clearance), it can affect the number of oral micro-organisms and
food debris from the mouth. The oral immune system (specific and non-
specific) affect to a large degree the cariogenic bacteria.
Subject: The behavior, attitude and dental knowledge affect the caries
etiology. These can influence the oral hygiene of the person as well as his
dietary habits.
2- Dental plaque:
Plaque quantity and quality greatly influence caries etiology. Bacteria
adhere to tooth surface and ferment carbohydrate causing release of acid
thus demineralization of tooth surfaces. Cariogenic bacteria involve
mutans streptococci, lactobacilli and others.
3- Diet:
Sweet consumption especially between meals may lead to continuous
drop of pH and not allowing the enough (time) for the pH to return to
normal, thus de mineralization of teeth.
Structure of enamel :
Enamel most highly mineralized tissue in the body
stronger than bone
Consists of microscopic crystals of hydroxyapatite arranged in
structural layers or rods, also known as prisms.

6
The enamel crystals are surrounded by water.
The water and protein components in the tooth are important for the acid
travel in to tooth and the minerals travel out and the tooth structure
dissolved.
enamel is approximately 95% inorganic, and 5% organic material
and water.
there are morphologic structures in the enamel with a high protein
content, such as (the striae of Retzius, enamel lamellae, enamel
tufts, and pores etc .).
These diffusion channels probably serve two very important
purposes in preserving the teeth:
1) permit physiological re mineralization throughout life .
2) the voids and protein content in the enamel probably cushion
intense biting pressures to help prevent fractures.
Stages of caries development:
The development of a carious lesion occurs in three distinct stages:
ž The earliest stage is (the incipient lesion), which is accompanied
by histologic changes of the enamel.
ž The second stage includes the progress of the demineralization
toward the dentino-enamel junction (DEJ) and/or into the dentin.
ž Final stage is the development of the frank lesion (cavitation)
The speed of progression of caries depend on:
o Ion concentration.
o Ph of saliva.
o Buffering actions.
o Salivary flow. All continually changing.
The initial acid attack dissolve Mg. and carbonate ions and later less
soluble Ca ion and Ph and other ions that part of crystal.
7
Caries zone in incipient lesion:
The zones seen before complete disintegration of enamel are: 10- 100
micron
Zone1: The translucent zone
o the deepest zone is seen in approximately 50% of the carious
lesions examined.
o Lies at the advancing front of the lesion,
o Slightly more porous than sound enamel about 1%.
o It is not always occur.
Zone2: The dark zone
o pore volume ranges from approximately 5% -25%.
o Found between the surface and dark zone, it is the area of greatest
demineralization.
Zone3: The main body of the lesion.
o pore volume ranges from approximately 5% -25%.
8
o Found between the surface and dark zone, it is the area of greatest
demineralization
Zone4: the surface zone
o Near-normal pore space of approximately 1%.
o Relatively unaffected area, greater resistant due to greater degree
of mineralization and greater degree of F concentration
Caries of enamel
Smooth surface Caries:
Due to plaque formation on enamel. The earliest manifestation of
incipient caries (early caries) of enamel is usually seen beneath dental
plaque as areas of decalcification (white spots).
The first change seen histologically is the loss of inter-rod substance of
enamel with increased prominence of the rods, this is followed by the loss
of mucopolysaccharides in the organic substance. presence of transverse
striations of the enamel rods, as it goes deeper, the caries forms a
triangular pattern or cone shaped lesion with the apex towards DEJ and
base towards the tooth surface. Finally there is loss of enamel structure,
which gets roughened due to demineralization, and disintegration of
enamel prisms.
Once cavitation occur the zones of incipient lesion become not clear less
defined because of :
a. Mineral loss
b. Presence of bacteria
c. Bacterial end product, plaque, residual substrate, which support further
lesion development
Pit and Fissure Caries:
-lesion begins beneath plaque, with decalcification of enamel
-pit and fissures are often deep, so may lead to food stagnation

9
-enamel in the bottom of pit or fissure is very thin, so early dentin
involvement frequently occurs.
- Here the caries follows the direction of the enamel rods.
- It is triangular with the apex facing the surface of tooth and the base
towards the DEJ.
- When reaches DEJ, greater number of dentinal tubules are involved.
- it produces greater cavitations than the smooth surface caries and there
is more undermining of enamel.
CARIES OF DENTIN
Begins with the natural spread of the process along the DEJ and rapid
involvement of the dentinal tubules which act as:
o Tracts leading to the pulp, during caries infection more fluid is
forced into tubule.
o Also act as a path for micro-organisms.
Early Dentinal Changes:
-Initial penetration of the dentin by caries. dentinal Sclerosis (because
odontoblast loss their vitality and became dead tract and began to calcify)
-Calcification of dentinal tubules and sealing off from further penetration
by micro-organisms, (protective barrier) more prominent in slow chronic
caries.
-The pulp begin to form amorphous reparative dentin for further
protection of the pulp.
-If surface intact in slow caries theoretically can be remineralized.
-Shape of the lesion is triangular with the apex towards the pulp and the
base towards the enamel
Advanced Dentinal Changes:
a- Decalcification of walls, confluence of the dentinal tubules, tiny
“liquefaction foci” described by Miller are formed by the focal
coalescing and breakdown of dentinal tubules.
11
These are ovoid areas of destruction parallel to the course of tubules
which filled with necrotic debris and increase in size by expanding. The
adjacent tubules are distorted and their course is bent due to this
expansion.
b- The destruction of dentin by decalcification and then proteolysis
occurs in numerous focal areas leading to a necrotic mass dentin of
a leathery consistency.
c- Clefts present in the carious dentin that extends at right angles to
the dentinal tubules, accounts for the peeling off from dentin in
layers while excavating.
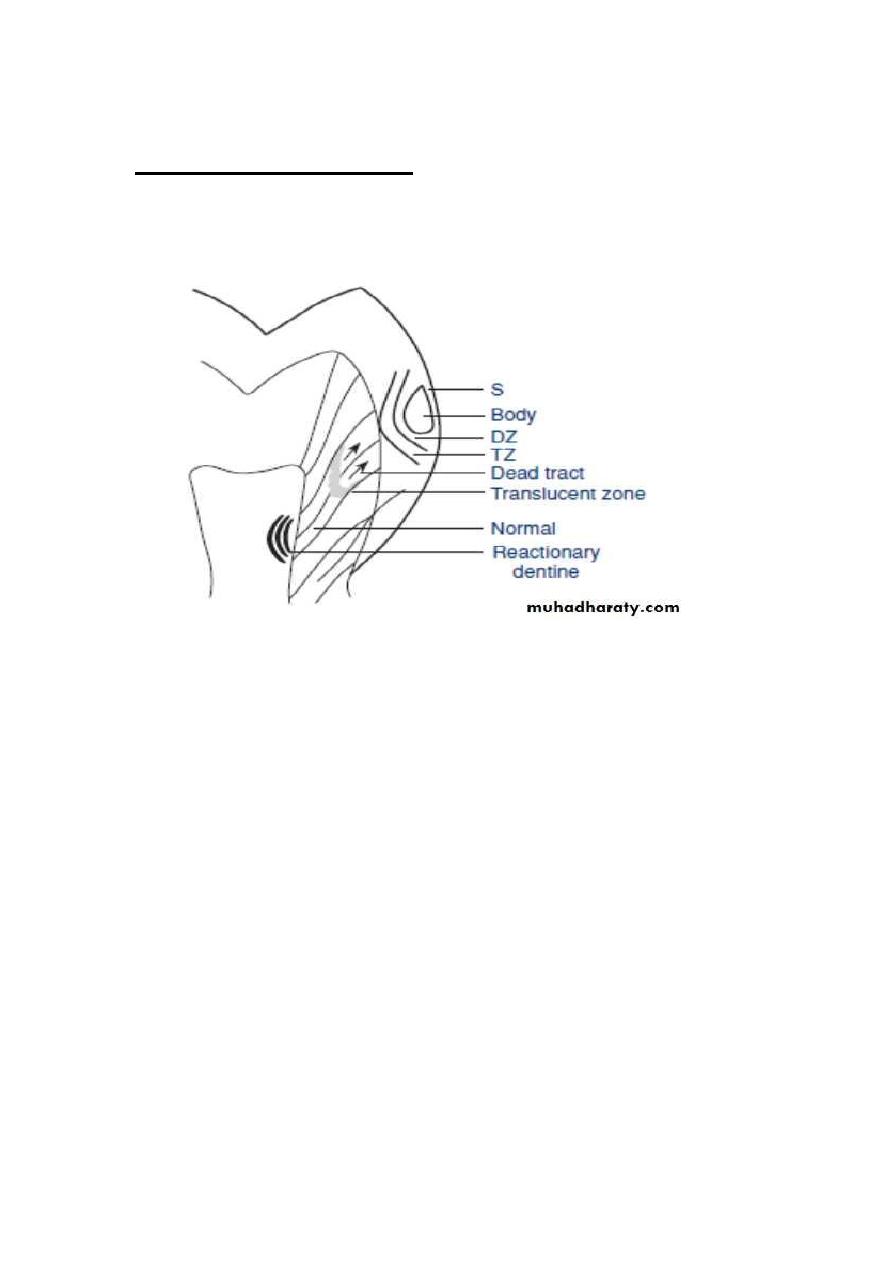
The appearance of lesion
Shape of the lesion is triangular with the apex towards the pulp and
the base towards the enamel.
Zone 1; Zone of Fatty Degeneration of Tome’s Fibers,(next to pulp)
-due to degeneration of the odontoblastic process. This occurs before
sclerotic dentin is formed and makes the tubules impermeable.
Zone 2; Zone of dentinal sclerosis, deposition of Ca salts in the
tubules.
Zone 3; Zone of decalcification of dentin
Zone 4; Zone of bacterial invasion
Zone 5; Zone of decomposed dentin due to acids and enzymes.
Root Caries
Root caries defined : is a soft, progressive lesion that is found anywhere
on the root surface that has lost its connective tissue attachment and is
exposed to the oral environment.
-prevalence in men 1.1-2.5 more than women
-the root surface must be exposed to the oral environment before caries
can develop here
11
-Katz found that in age 30s 1/1000, in 50s 1/5 may have dental caries.
-Plaque and micro-organisms are essential for the cause and progression
of the lesion, mostly Actinomyces,
-micro-organisms invade the cementum either along the Sharpey’s fibers
or between the bundles of fibers.
-spread laterally, since cementum is formed in concentric layers.
-after decalcification of cementum, destruction of matrix occurs similar to
dentin with ultimate softening and destruction of this tissue.
-invasion of micro-organisms into the dentinal tubules, finally leading to
pulp involvement. The rate is slower due to fewer dentinal tubules than
crown area.
The root caries appears clinically as yellowish –brown coloration, non
cavitated, soft ,may assume any out line ,depth 0.5-1 mm ,complete loss
of cementum.Expose the dentine ,it may undergo remineralization or
arrest.
Arrested root caries:
Its demonstrate 3 physical characteristics:
1-outer barrier layer of hypermineralized dentin
2- sclerotic inner barrier between carious and sound dentin
3-mineralization occurring within the dentinal tubules
The mineralized lesion appears glossy, smooth, hard , while the active
lesion has leathery feeling