Poliomyelitis

Session objectives
Definition & PathogenesisSymptoms (basic patterns of polio infection)
Laboratory Diagnosis
Epidemiology (Occurrence, Reservoir, Transmission, Temporal Pattern, Communicability)
Prevention (Poliovirus Vaccines)
Polio Eradication (because of)
Poliomyelitis
The words polio (grey) and myelon (marrow, indicating the spinal cord) are derived from the Greek. It is the effect of poliomyelitis virus on the spinal cord that leads to the classic manifestation of paralysis.The virus enters through the mouth, and primary multiplication of the virus occurs at the site of implantation in the pharynx and gastrointestinal tract.
The virus invades local lymphoid tissue, enters the bloodstream, and then may infect cells of the central nervous system.
Replication of poliovirus in motor neurons of the anterior horn and brain stem results in cell destruction and causes the typical manifestations of poliomyelitis.
Flaccid paralysis occurs in <1 % of polio virus infection
Aseptic meningitis occurs in about 1% of infections
• proportion of cases
90–95%
4–8%
1–2%0.1-0.5%
79% of paralytic cases19% of paralytic cases
2% of paralytic cases
Outcome
• Asymptomatic
• Minor illness• Non-paralytic aseptic meningitis
• Paralytic poliomyelitis
— Spinal polio
— Bulbospinal polio
— Bulbar polio
Outcomes of poliovirus infection
Clinical responses are extremely varied:
Inapparent: > 90 % of infections are either inapparent or result in non specific fever
Minor illness: 10%
low grade fever, malaise , headache , nausea & vomiting.
• Major illness
• Sever muscle spasm & pain +• Neck & back stiffness with flaccid paralysis may occur, characterized by:
• Asymmetrical with fever at onset(reach max. extent within 3-4 days)
• Site is depend on the location of nerve cell destruction in the spinal cord or brain stem
• Legs are affected more than arms
• Proximal parts more often than distal parts
Affected muscles are floppy, reflexes are diminished ,sense of pain & touch remain normal
Some improvement in paralysis may occur in convalescence but paralysis present after 60 days likely to be permanent.
Severe cases : quadriplegia , abdomen & thoracic muscles , bulbar polio
DDx: of Acute flaccid paralysis (AFP)
paralytic polio ;Guillian Barre syndrome
transverse myelititis,
traumatic neuritis
acute motor axonal neuropathy
myasthenia gravis
Non paralytic polio;
encephalitis , meningitis ,tumors, brain abscess.
Laboratory diagnosis:
Routine CSF examination (increased number of white blood cells10–200 cells/mm3, primarily lymphocytes) and a mildly elevated protein (40–50 mg/100 mL)
Test for levels of antibodies (Neutralizing antibodies appear early and may be at high levels by the time the patient is hospitalized; therefore, a fourfold rise in antibody titer may not be demonstrated)
Viral cultures of throat washings, stools, or cerebrospinal fluid (CSF)
Causative agent : There are three poliovirus serotypes (P1, P2, and P3). There is minimal heterotypic immunity between the three serotypes. That is, immunity to one serotype does not produce significant immunity to the other serotypes.
Poliovirus(Enterovirus )
Type 1 2 & 3
Paralytogenic less commonly
Most frequent frequent cause
Cause of outbreak of vaccine
associated.
Occurrence :
Prior to immunization it had a world wide distribution.It is eradicated from the western Hemispheres & industrialized countries
The greatest risk of polio now occurs on the Indian sub continent 89% ,&to lesser extent , in the countries of west ¢ral Africa 10%.
If cases appeared in industrialized countries they are either imported or vaccine associated
Risks groups include:
Lack of immunization against polio and then exposure to polioTravel to an area that has experienced a polio outbreak
In areas where there is an outbreak, those most likely to get the disease include children, pregnant women, and the elderly. The disease is more common in the summer and fall
Age of distribution:
Remains primarily a disease of infants & young children ,in many polio endemic regions 70-80% of cases are < 3 years of age & 80-90% are <5 years of age.
About half the vaccine-associated paralytic poliomyelitis among adult contacts of vaccinees.
Seasonality :
Poliovirus infection typically peaks in the summer months in temperate climates. There is no seasonal pattern in tropical climates.Reservoir :Humans are the only known reservoir of poliovirus, most frequently persons with inapparent infections esp. children .
Long term carriers have not been found.
Mode of transmission:
• Direct person –to- person principally through fecal –oral transmission- bad standard of sanitation
- young children
• Pharyngeal droplets
- good sanitation
- older age groups
• Food , milk, & other materials contaminated with feces (rare)
• No reliable evidence of spread by insects exists
• Water and sewage , rarely implicated .
Incubation period:
7- 14 days for paralytic cases
Reported range of 3-35 days
Period of communicability:
Not precisely definedTransmission is possible as long as the virus is excreted
Virus appeared in throat secretion as early as 36 hrs & in feces 72 hrs after exposure to infection
Virus persists in the throat for (1) week &in the feces for 3-6 weeks
Susceptibility: Universal
Type specific immunity of life longRate of paralysis among infected non immune adults higher than those in infants & young children.
Second attacks are rare & result from different type .
IM injection, trauma, or surgery during I.P or prodromal illness may provoke paralysis in affected extremetes.
Prevention:
• Education of public on the advantages of immunization in early childhood• Vaccination trivalent (OPV) sabin
inactivated (IPV)salk
OPV:
Recommended by WHO for polio eradication
3 doses will protect at least 80-85 % of immunized children
Induces both circulating antibody &intestinal and pharyngeal resistance to infection.
OPV Low cost, ease of administration& superior capacity to provide population immunity.
(however )Low rates of seroconversion and reduced vaccine efficacy in developing countries.
It is contraindicated in (acute infectious illness, fever, diarrhea, all immune deficient dis.)

Complications
Vaccine associated paralysis (VAPP) 1:2.5,000,000 dosesOr Vaccine associated paralysis (1:800000 in 1st dose)
IPV:
Prevents paralytic polio by producing sufficient Ab. In the serumIt has no risk of vaccine associated paralysis
Lower level of int. immunity
More expensive.
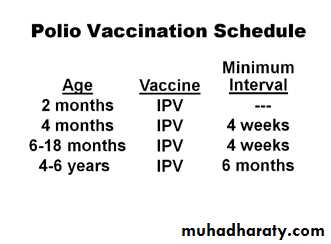
A dose of IPV on or after age 4 years is recommended regardless of the number of previous doses.
Vaccine Schedule
Birth zero dose
6-8 wks 1st dose
10-12 wks 2nd dose 4basic ds
14-16 wks 3rd dose of OPV
9 months for children not immunized at birth
If OPV is given to child with diarrhea the dose should be repeated
four doses of any combination of IPV or OPV by 4–6 years of age is considered a complete poliovirus vaccination series.
The recommended schedule of immunization in Iraq
• root• vaccines
• age
• ID+ORAL+IM
• B.C.G+POLIO(0)+HB1
• 1 week
• IM+ORAL+IM
• D.P.T(1)+POLIO(1)+HB2
• 2 Months
• IM+ORAL
• D.P.T(2)+POLIO(2)
• 4 Months
• IM+ORAL+IM
• D.P.T(3)+POLIO(3)+HB3
• 6 Months
• SC+ORAL
• MEASLES+VIT A
• 9 Months
• SC
• M.M.R
• 15Months
• ORAL+IM
• FIRST.B00STER POLIO+D.P.T
• 18-24 Months
• ORAL+IM
• 2nd..B00STER POLIO+D.P.T
• 4-6 Years
Control;
Reporting is obligatory any case of AFP under 15 y should be fully inv.(clin ,epidm,and stool culture )
Isolation
Concurrent disinfection
Protection of contacts
Investigation of sourse
Sp Rx: none
Polio is one of a small limited number of diseases that can be eradicated, reasons are:
polio only affects humans, and there is no animal reservoiran effective and inexpensive vaccine exists, called Oral PolioVirus (OPV)
immunity against polio is life-long
the virus can only survive for a very short time in the environment
Long term carriers have not been found.
Strategy of Eradication:
High routine immunization coverage with OPV i.e giving the 4 basic doses during the 1st year of lifeSupplementary immunization in the form of mass campaigns or NIDs
Effective surveillance.
Final stage when Very few or no cases are occurring ,door-to-door immunization campaigns (mopping up) in areas where the virus persists.