
Exodontia Practice
Oral and maxillofacial surgery is a medical specialty
concerned with diagnosis and treatment of diseases of
jaws, teeth, mouth and face.
Exodontia can be defined as painless removal
of a tooth or tooth root from its socket with
minimal injury to the bone and surrounding
structure so that postoperative healing is
uneventful.
Dentistry is one of the fastest growing science of
medicine. With the introduction of many newer
instruments and anesthesia, extraction is a routinely
carried out procedure in dental office. Tooth extraction
remains an essential component of both the art and
science of dentistry despite the enormous progress in
the prevention of dental disease made during the last
three decades of the twentieth century. The effect of
the fluoride revolution and increasing public awareness
of oral health means that people in the western world
are retaining their teeth longer and fewer teeth are being
extracted, particularly in adolescents and young adults.
This trend towards the retention of the natural dentition
into later life is resulting in more extractions being needed
in older patients, who have more complicated medical
history and bone is more brittle than the young. Thus,
the difficulty and complexity of extraction procedures
is increasing with the average age of our patients.
Dental surgeons, especially those in practice, are
required to face these challenges in medico-legal climate
in which litigation exists when complications arise for
whatever reason. It is therefore more important that
the principles and techniques of removing teeth are
understood by all those in the dental profession who
would pick up a pair of extraction forceps.
Having a tooth extracted may also pose a daunting
challenge to patients whose imagination of what is
to happen are often governed by misbeliefs, others
experience and existing social taboos could get the better
of them. Calm, reassuring approach by the dental
surgeon whilst explaining the procedure goes a long
way towards allowing such fears and building their
confidence. The successful outcome of tooth extraction
depends not only on the surgeon's practical skills, but
also on his or her ability to emphasize with patients and
the way they perceive the problem.
The extraction of tooth is a surgical procedure
involving bony and soft tissue of oral cavity, access to
which is restricted by the lips and cheeks and further
complicated by the movement of tongue and mandible.
An additional hazard is that this cavity communicates
with pharynx which in turn opens into larynx and
oesophagus. Further this field of operation is flooded
by saliva and inhabited by the largest number and variety
of microorganisms. Finally it lies close to the vital centres.
It is therefore essential that this aspect of oral surgery
be properly understood judiciously performed and be
based on sound surgical principles as it applies to any
other part of human body. No operation performed
by the dentist is fraught with such great danger to the
patient as those of oral surgery, a large part of which
is the extraction of teeth.
While the great majority of extractions can be done
in the dental office, some patients require hospitalization
for this surgery because of predisposing systemic
conditions which increases the surgical risks.
Dental extraction has always been considered to be
an unpleasant procedure for the patients due to pain
F i g u r e 1.1: Tooth extraction: Traditional method

Introduction
phobia. With the advent of local anesthetic drugs
techniques and standardization of surgical procedure,
extraction is no longer considered to be painful
experience to the patients. Gone are the days when
extraction was supposed to be one of the crude procedure
(Figure 1.1).
The control of the patient is fear and anxiety has
long been a challenge to the dental practitioner. Today's
extraction procedure is painless and anxiety-free provided
that one employs good principles of patient management
and pharmacokinetics (Figure 1.2).
In the initial few chapters of this book armamentarium
required for tooth extraction, principles of exodontia,
various methods of extraction are described. Then a brief
idea about anatomical considerations and anesthesia
is described. Next few chapters describe special techni-
ques like pediatric extractions serial extractions and
F i g u r e 1.2: Extraction of tooth in dental office
extractions for medically compromised patients. Lastly,
the complications are described in details with their
management.
Armamentarium
6
Exodontia Practice
The purpose of this chapter is to introduce the instru-
ments that are required to perform routine oral surgical
procedures. These instruments are used for a wide variety
of purposes, including both soft tissue and hard tissue
procedures. This chapter deals primarily with a
description of the instruments; subsequent chapters
discuss the actual use of the instruments in the variety
of ways for which they are intended.
INSTRUMENTS USED TO EXTRACT TOOTH
(DENTAL FORCEPS)
Dental forceps were used in Greek times and were first
illustrated by Albucasis. He described a short handled pairs
which were first applied to the crown of the tooth to shake
it up and then the long handled forceps were used to
complete the extraction. Cyrus Fay in 1826 was first to
describe forceps design to fit the neck of the tooth and
these were said not to apply any force to the crown. The
credit for anatomically designed forceps is frequently given
to Sir John Toms (1841), and there is no doubt his
instruments were superior to those of Fay and it is from
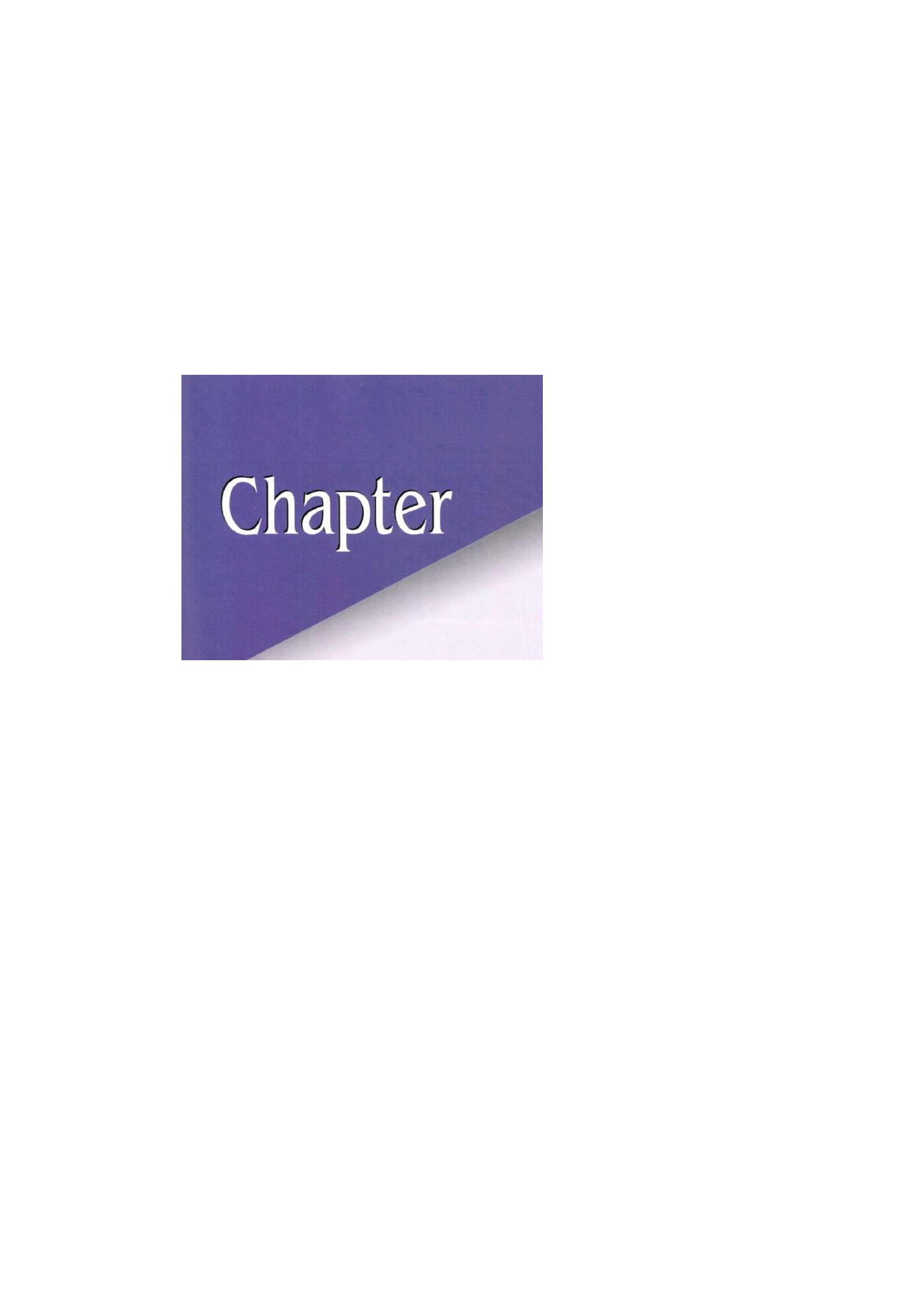
his design modern forceps have developed (Figure 2.1).
The dental forcep is the most widely used instrument
in the extraction of teeth. The use of this instrument makes
it possible for the operator to grasp the root portion of
a tooth and to luxate the latter from its socket by exerting
pressure upon it. The forceps have blades and handles
united by a hinge joint. The larger the ratio between
the length of the handles and the length of the blades
the greater is the force which can be exerted upon the
root. The length of the handle must be such that the
forceps fits the operator hand. Greater the distance
between the hinge joint and operator's hand, the greater
is the movement of the forceps within the hand. Thus,
greater energy may be dissipated to the tooth.
The blades of the forceps are forced into the
periodontal ligaments to separate it from the tooth. Thus,
the blades should be always sharp. The blades of stainless
steel forceps can be sharpened with a sandpaper disk
applied to the outside of the tips.
Ideally the whole of the inner surface of the blade
should fit the root surface. In practice the size and shape
of roots vary so greatly that it is not possible to achieve
this aim and root is grasped by the edges of the blades
F i g u r e 2 . 1 : Dental forceps: Various designs in literature

Armamentarium
F i g u r e s 2.2A a n d B: Effective use of forceps: (A) Maxillary, (B) Mandibular
establishing a two point contact. If there is a single point
contact between the tooth and blade, the tooth will
probably crushes when it is gripped. It is better to use
forceps with blades which are slightly narrow than a
forceps with blades which are too broad.
The effective use of various instrument depends on
understanding the design of the instruments and their
principles. Forceps permits controlled force application
on the tooth that allows dilatation of alveolar socket,
luxation of tooth and its subsequent removal.
The forceps can be classified as American pattern
of forceps and English pattern of forceps. In the Indian
subcontinent the English pattern is more popular.
The forceps used for the maxillary and mandibular
teeth differ in their design.
In mandibular forceps, the beaks are at right angle
to the long axis of the handle while in maxillary forceps
beaks are in the same line, i.e. parallel to the long axis
of the handle.
The handles of forceps are held differently depending
on the position of tooth to be removed. Maxillary forceps
are held with the palm underneath the forceps. So that
the beak is directed in a superior direction. The forceps
used for the removal of mandibular teeth are hold with
palm on top of the forceps so that beak is pointed down
towards the tooth (Figures 2.2A and B ) .
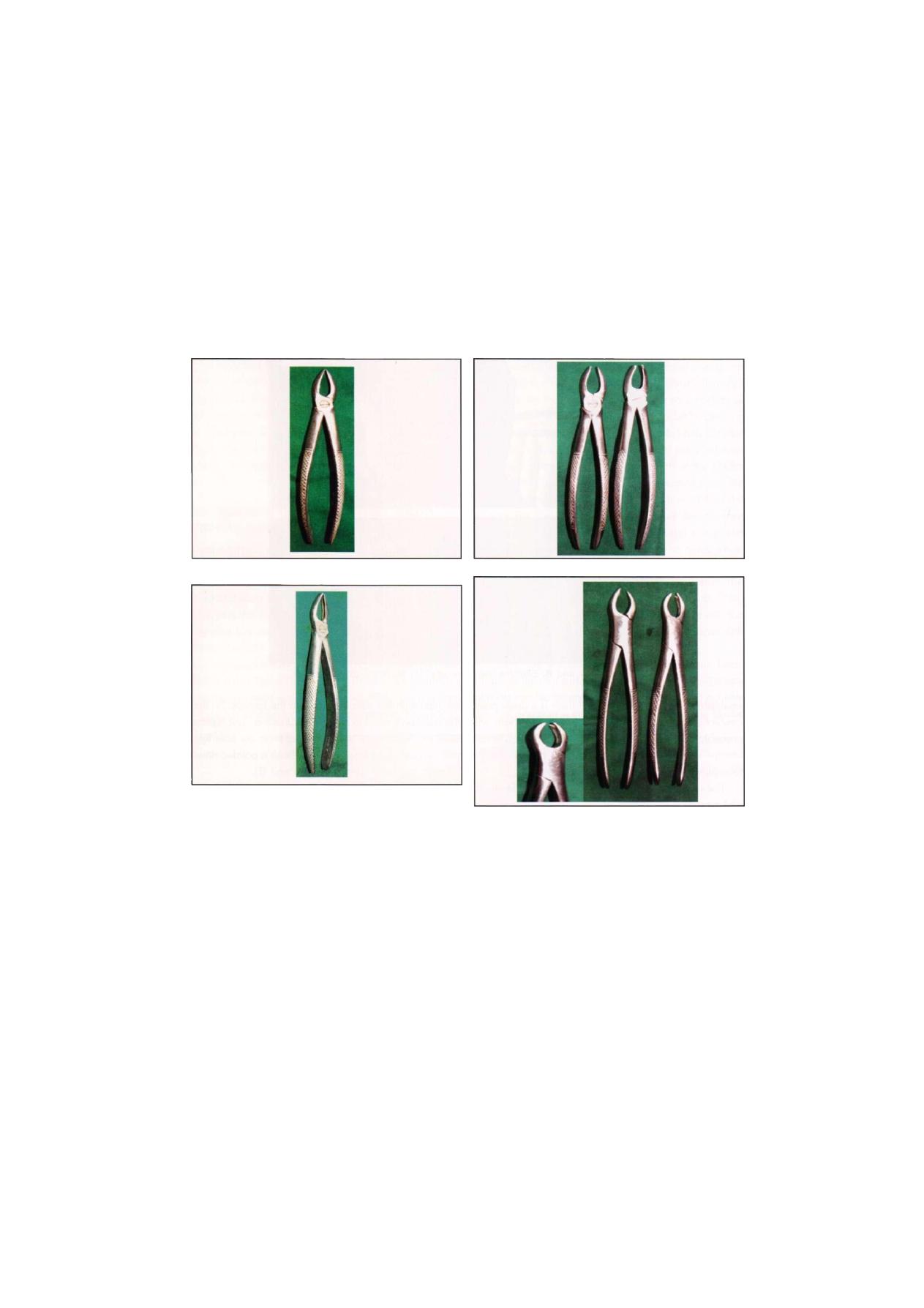
MAXILLARY FORCEPS
Maxillary Anterior Forcep
This forcep has beaks in approximation with each other
and the handle is straight without curvature. Beaks are
symmetrical and are placed in the same line as the
handle. Beaks are shorter than the handle. This forcep
is used for the extraction of maxillary incisors and
canine (Figure 2.3).
Maxillary Premolar Forcep
This forcep is having beaks which are approximating each
other and placed parallel to handle. Handle is having
concavity on one side and convexity on other side (Figure
2.4). This provides better grip and allows the forcep
8
Exodontia Practice
F i g u r e 2.3: Maxillary anterior forcep
F i g u r e 2.4: Maxillary premolar forcep
to reach inside more posterior in oral cavity. This forcep
is used for removal of maxillary premolars and rarely
upper roots.
Maxillary Molar Forcep
These forceps are paired forceps having beaks which
are asymmetrical and broader as compare to anterior
forceps. The one beak is pointed to engage the bifurcation
of the tooth on buccal side and other engages the
palatal root. Depending upon the position of pointed
beak the forceps can be identified as right and left. The
handle is same as that of maxillary premolar forceps
(Figure 2.5).
F i g u r e 2.5: Maxillary molar forceps (right and left)
F i g u r e 2.6: Maxillary cow horn forceps (right and left)
Maxillary Cow Horn Forcep
These are the paired forceps having design same as that
of maxillary molar forceps except they are having beaks
that appear as the horn of the cow and called as cow
horn forceps. One beak is pointed which goes in buccal
bifurcation other beak is having notch which engages
the palatal root. These are paired forceps used for right
and left side separately (Figure 2.6). They are used for
maxillary molars which are badly carious in nature. The
major disadvantage is that they crush alveolar bone when
used on intact teeth.

Armamentarium
F i g u r e 2.7: Maxillary bayonet forcep Figure 2.8: Maxillary third molar forcep
Maxillary Bayonet Forcep
This forcep is designed for removal of maxillary roots.
Beaks are symmetrical and closely approximate to each
other. The beaks are narrow to fit it to the circumference
of the root (Figure 2.7). Handle is having angulations
so that it can reach as much posteriorly as possible.
Maxillary Third Molar Forcep
This forcep is specially designed for removal of maxillary
third molar. The forceps have beaks which engage the
crown of third molar and is having long handle to reach
the posterior most region in maxilla (Figure 2.8).
MANDIBULAR FORCEPS
Mandibular Anterior Forcep
This forcep is having beaks similar to maxillary incisor
forcep which approximate with each other. Beaks are
at right angle to the handles. This forcep is used for
extraction of mandibular incisor and canine (Figure 2.9).
F i g u r e 2.9: Mandibular anterior forcep
Mandibular Premolar Forcep
This forcep has same design as that of mandibular
anterior forcep except the space in between two beaks
is more compared to incisor forcep to accommodate the
crowns of premolar which are having greater diameter
(Figure 2.10).
Mandibular Molar Forcep
These are unpaired forceps having beaks broader and
stout. The beaks are symmetrically pointed so that sharp
pointed tips can engage the bifurcation both at buccal
and lingual surfaces. The beaks are at right angles to
the handle. These forceps are used for the extraction
of mandibular molars (Figure 2.11).

10
Exodontia Practice
F i g u r e 2.10: Mandibular premolar forceps
F i g u r e 2 . 1 1 : Mandibular molar forceps
Mandibular Cow Horn Forceps
The design of this forcep is same as that of mandibular
molar forcep except the beaks are pointed and conical
in shape. These forceps are used for the extraction of
mandibular molars.
Universal Forcep
This forcep is having the beaks similar to the mandibular
molar forcep except that they are facing forward towards
each other at right angle to the handle. This is a specially
designed forcep mainly used for extraction of third molars
(Figure 2.12).
INSTRUMENTS USED FOR TOOTH LUXATION
(ELEVATORS)
Elevators are the instruments used to elevate the tooth
or root from the alveolar socket. Elevation of tooth before
application of forcep makes a difficult extraction easy.
The elevators are designed on two basic patterns. In
general all the elevators have handle, shank and a blade.
In the straight pattern all these three components are
Figure 2.12: Universal forceps
placed in one plane. In the other design the blade and
shank are in one plane and handle is placed at right
angle to them. There are so many elevators available
commercially but a few are widely used because of their
efficiency and convenience.
The elevators deliver the force based on various
mechanical principles to drive the tooth or root along
its path of delivery or line of withdrawal. It represents
the direction along which the tooth move out of the
alveolar socket with economy of force and economy of
instrumentation. Hence, successful use of an elevator
depends on the determination of the convenient path
of its delivery. Principles of use of elevators are described
in the principles of exodontia chapter.
TYPES
The elevators which are widely used in the dental practice
are (Figure 2.13):
1. Straight elevator
2. Apexo elevator (Right and left)
3. Cross bar elevator
F i g u r e 2.13: Different types of elevators. (A,B) Straight
elevator, (C) Apexo elevator, (D) Cross bar elevator
11
Armamentarium
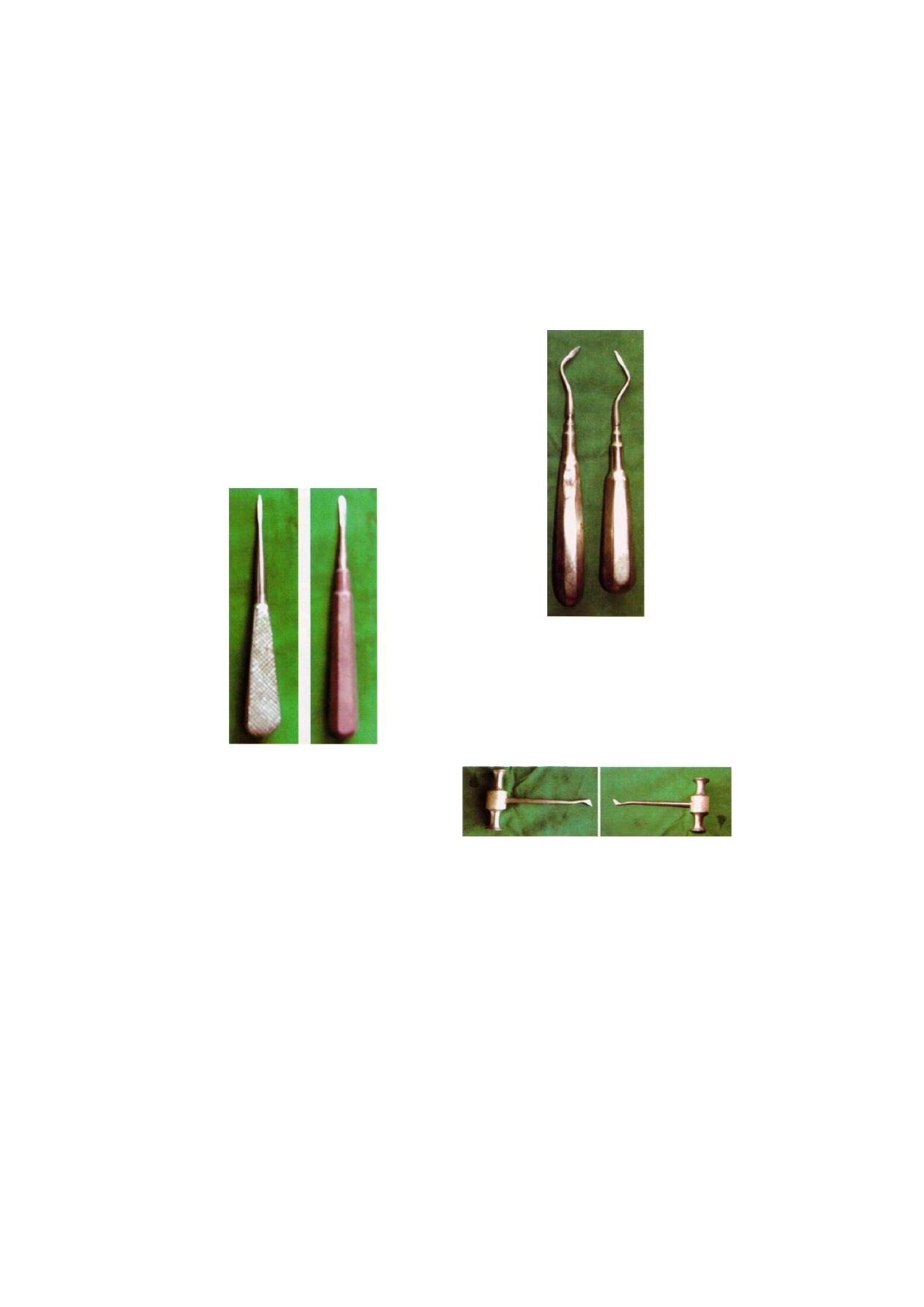
Straight Elevator
The blade, handle and shaft are in one line. The blade
is pointed or broad and bluff as in coupland elevator.
The blade is having concave surface on one side, so
that it can be used in same fashion as shoehorn.
The elevator is used to elevate the mandibular and
maxillary molars to luxate the teeth in case of multiple
extraction. It is usually avoided in anterior teeth (Figure
2.14).
B
F i g u r e 2.14: Straight elevators. A—Straight pattern, B—
Coupland pattern
Apexo Elevator
These elevators are paired having handle, shank and
blade which are in same plane. The blade is having
angulations so that it reaches the root apices. This elevator
works on the principle of wedge (Figure 2.15).
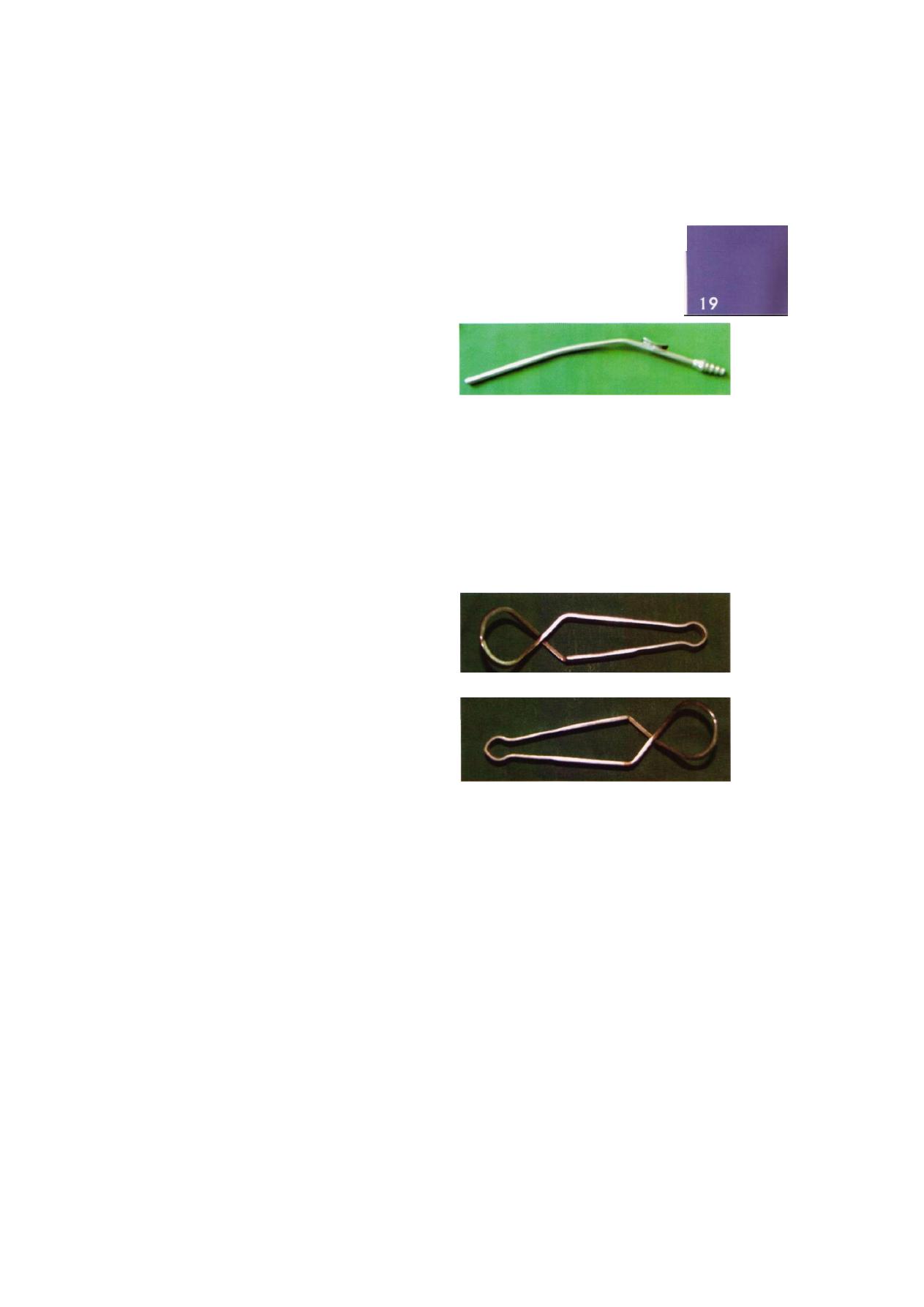
Cross Bar Elevator
These are paired elevators having blade and shank at
right angle and shank and handle at right angle to each
other. This is indicated for the removal of the mandibular
roots where the other root has already been removed.
In such cases the tip of the elevator is introduced to the
depth of the empty socket with the concave surface of
F i g u r e 2.15: Apexo elevator (Paired elevators)
the elevator facing the root to remove. By applying wheel
and axle principle with rotatory movement, the inter-
radicular septum and the root are elevated out of alveolar
socket. The same elevator is used for elevating the distal
root on the right side and the mesial root on the left
side (Figure 2.16).
F i g u r e 2.16: Cross bar elevators (Paired elevators)
Winter Cryer Elevator
This elevator is same as that of cross bar except handle
is parallel to the working end. This is a set of elevators
used for removal of root apices (Figure 2.17).
Axio Elevator
These are specially designed elevators which are used
for elevation of mandibular third molars (Figure 2.18).

12
Exodontia Practice
F i g u r e 2.17: Winter crayer elevator (Paired elevators)
F i g u r e 2.18: Axio elevator (Paired elevators)
INSTRUMENTS TO INCISE TISSUE
Most surgical procedures begin with an incision. The
instrument for making an incision is the scalpel, which
is composed of a handle and sharp blade. The most com-
monly used handle is the No. 3 handle, but occasionally
the longer, more slender No. 7 handle is used. The tip
of the scalpel handle is prepared to receive a variety of
differently shaped scalpel blades that can be inserted onto
a slotted receiver (Figure 2.19).
The most commonly used scalpel blade for intraoral
surgery is the No. 15 blade. It is relatively small and can
F i g u r e 2.19: Scalpels for making incision
(BP handle No. 3 and No.
7)
be used to make incisions around teeth and through
mucoperiosteum. It is similar in shape to the large
No. 10 blade, which is used for skin incisions. Other
commonly used blades for intraoral surgery are the'
No. 11 and the No. 12 blades. The No. 11 blade is
sharp pointed blade that is used for making stab incisions,
such as for incising an abscess. The hooked No. 12 blade
is useful for mucogingival surgery procedures where
incisions must be made on the posterior aspect of teeth.
The bard parker handle is of different number, i.e.
No. 3 handle is used to receive blades No. 15, No. 11,
No. 12, and No. 4 handle is used to receive No. 10
blade (Figure 2.20).
F i g u r e 2.20: Different types of blades. BP handle blade
The scalpel blade is carefully loaded onto the handle
with a needle holder to avoid lacerating the operator's
fingers. The blade is held on the superior edge where
it is reinforced with a small rib, and the handle is held
so that the male portion of the fitting is pointing upward.
The blade is then slid onto the handle until it clicks into
position. The knife is unloaded in a similar fashion. The
needle holder grasps the most proximal end of the blade

Armamentarium
F i g u r e 2 . 2 1 : Loading and unloading of scalpel blades
and lifts it to disengage it from the male fitting. It is then
slid off the knife handle in the opposite direction. The
used blade is discarded into a proper container (Figure
2.21).
When using the scalpel to make an incision, the
surgeon holds it in the pen grasp to allow maximal con-
trol of the blade as the incision is made. Mobile tissue
should be held firmly to stabilize it so that as the incision
is made, the blade will incise, not displace, the mucosa.
Whole length of the blade must be drawn for incising
tissue. If only one end is used cutting is inefficient and
uncontrolled. When a mucoperiosteal incision is made,
the knife should be pressed down firmly so that the
incision penetrates the mucosa and periosteum with the
same stroke. Other principles of mucoperiosteal incision
and flap design are described in subsequent chapters.
Scalpel blades are designed for single patient usage.
They are dulled very easily when they come into contact
with hard tissue such as bone and teeth. If several inci-
sions through mucoperiosteum to bone are required,
it may be necessary to use a second blade during a
single operation. It is important to remember that dull
blades do not make clean, sharp incisions in soft tissue
and therefore should never be used.
INSTRUMENTS FOR ELEVATING
MUCOPERIOSTEUM
After an incision through mucoperiosteum has been
made, the mucosa and periosteum should be reflected
from the underlying bone in a single layer with a
periosteal elevator (Figure 2.22). The instrument that is
most commonly used is the Molt periosteal elevator. This
instrument has a sharp, pointed end and a broader flat
end. The pointed end is used to confirm the depth of
incision and reflect dental papillae form between teeth,
The broad end is used for elevating the tissue from the
bone.
F i g u r e 2.22: Periosteal elevators
The periosteal elevator can be used to reflect soft
tissue by three methods. First, the pointed end can be
used in a prying motion to elevate soft tissue. This is
most commonly used when elevating a dental papilla
form between teeth. Second is the push stroke in which
14
Exodontia Practice
the broad end of the instrument is slid underneath the
flap, separating the periosteum from the underlying bone.
This is the most efficient stroke and results in the cleanest
reflection of the periosteum. The third method is a pull
stroke or scrape stroke. This is occasionally useful in some
areas but tends to tear the periosteum unless it is done
carefully.
The periosteal elevator can also be used as a retractor.
Once the periosteum has been elevated, the broad
blade of the periosteal elevator is pressed against the
bone with the mucoperiosteal flap elevated into its
reflected position.
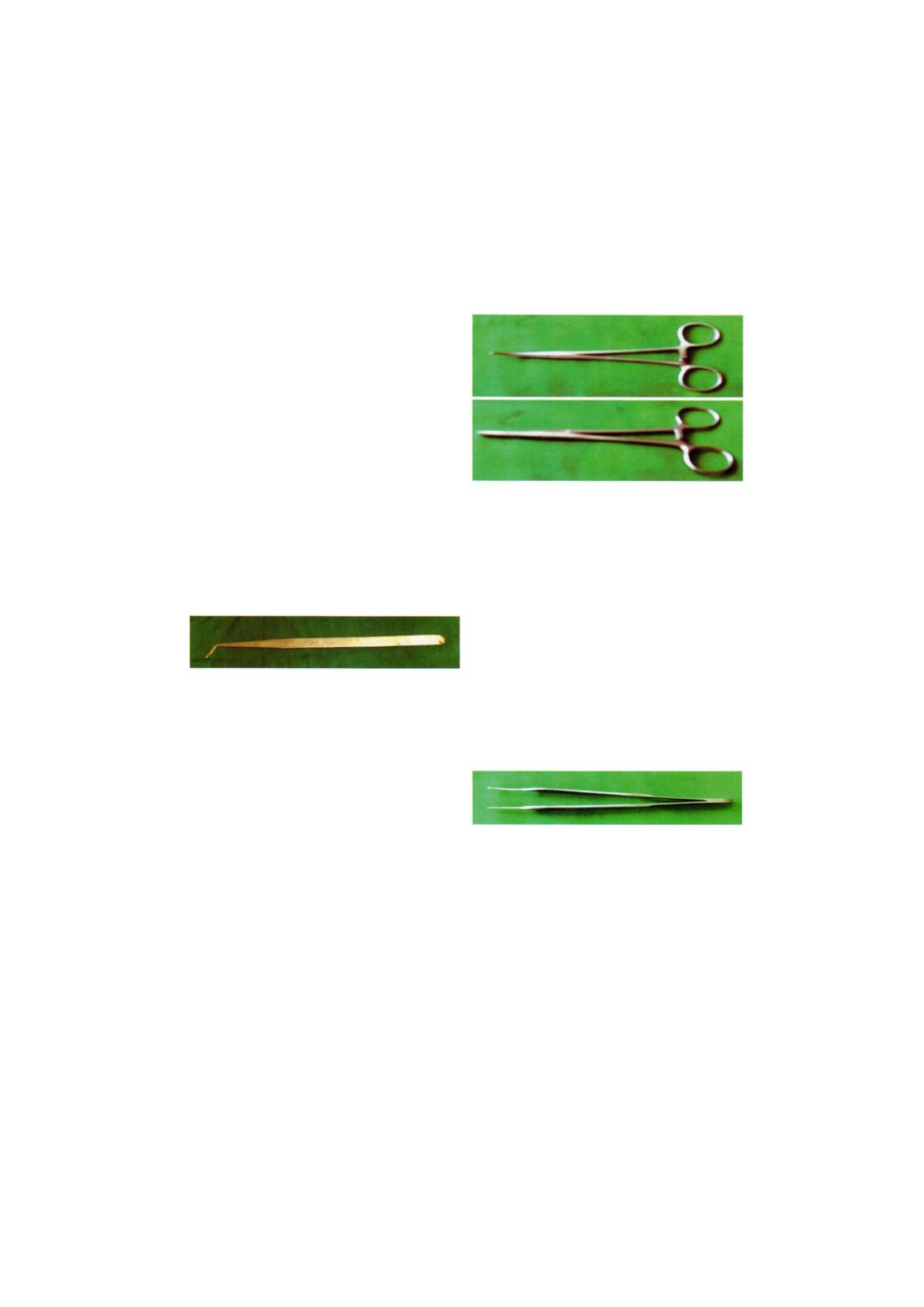
When teeth are to be extracted, the soft tissue attach-
ment around the tooth needs to be released from the
tooth. The instrument most commonly used for this is
the moons probe. This instrument is relatively small and
delicate and can be used to loosen the soft tissue via
the gingival sulcus (Figure 2.23).
F i g u r e 2.23: Moon's probe
INSTRUMENTS FOR CONTROLLING
HEMORRHAGE
When incisions are made through tissue, small arteries
and veins are incised, causing bleeding that may require
more than simple pressure to control. When this is neces-
sary, an instrument called a hemostat is used. Hemostats
come in a variety of shapes, may be relatively small and
delicate or larger, and are either straight or curved. The
hemostat most commonly used in oral surgery is a curved
hemostat (Figure 2.24).
A g o o d hemostat must have tips that opposes
accurately with each other. Blades must be closed firmly
on first ratchet and light should not pass through the
blades when handle is fully closed. Hemostat gets spoiled
if hard and bulky material is caught with it. Method of
application of hemostat includes visualization of bleeding
point, application of hemostat at right angle direction
to direction of force of blood. Catch the tip with
Figure 2.24: Hemostats (curved and straight artery forceps)
minimum amount of surrounding tissue as bulky ligation
may slip. In addition to its use as an instrument for
controlling bleeding, the hemostat is especially useful
in oral surgery to remove granulation tissue from tooth
sockets as well as to pick up small root tips from tooth
sockets.
INSTRUMENTS TO GRASP TISSUE
In performing soft tissue surgery, it is frequently neces-
sary to stabilize soft tissue flaps in order to pass a suture
needle. Tissue forceps most commonly used for this
purpose is the Adson forceps. These are delicate forceps
with small teeth that can be used to gently hold tissue
and thereby stabilize it. Adson forceps are also available
without teeth (Figure 2.25A).
F i g u r e 2.25A: Adson forcep
In some types of surgery, especially when removing
larger amount of fibrous tissue as in an epulis fissuratum
forceps with locking handles and teeth that will grip the
tissue firmly are necessary. In this situation Ellis forceps
are used. The locking handle allows the forceps to be
placed in the proper position and then to be held by
an assistant to provide the necessary tension for proper
dissection of the tissue. The Ellis forceps should never
be used on tissue that is to be left in the mouth because
Armamentarium
15
they cause a relatively large amount of crushing injury.
The Ellis forceps are most commonly used instrument
having straight blades and tip slightly curved or angulated
for better grip. Tip is provided with interlocking teeth.
They are three to four in number and interlock with each
other (Figure 2.25B).
F i g u r e 2.25B: Ellis forcep
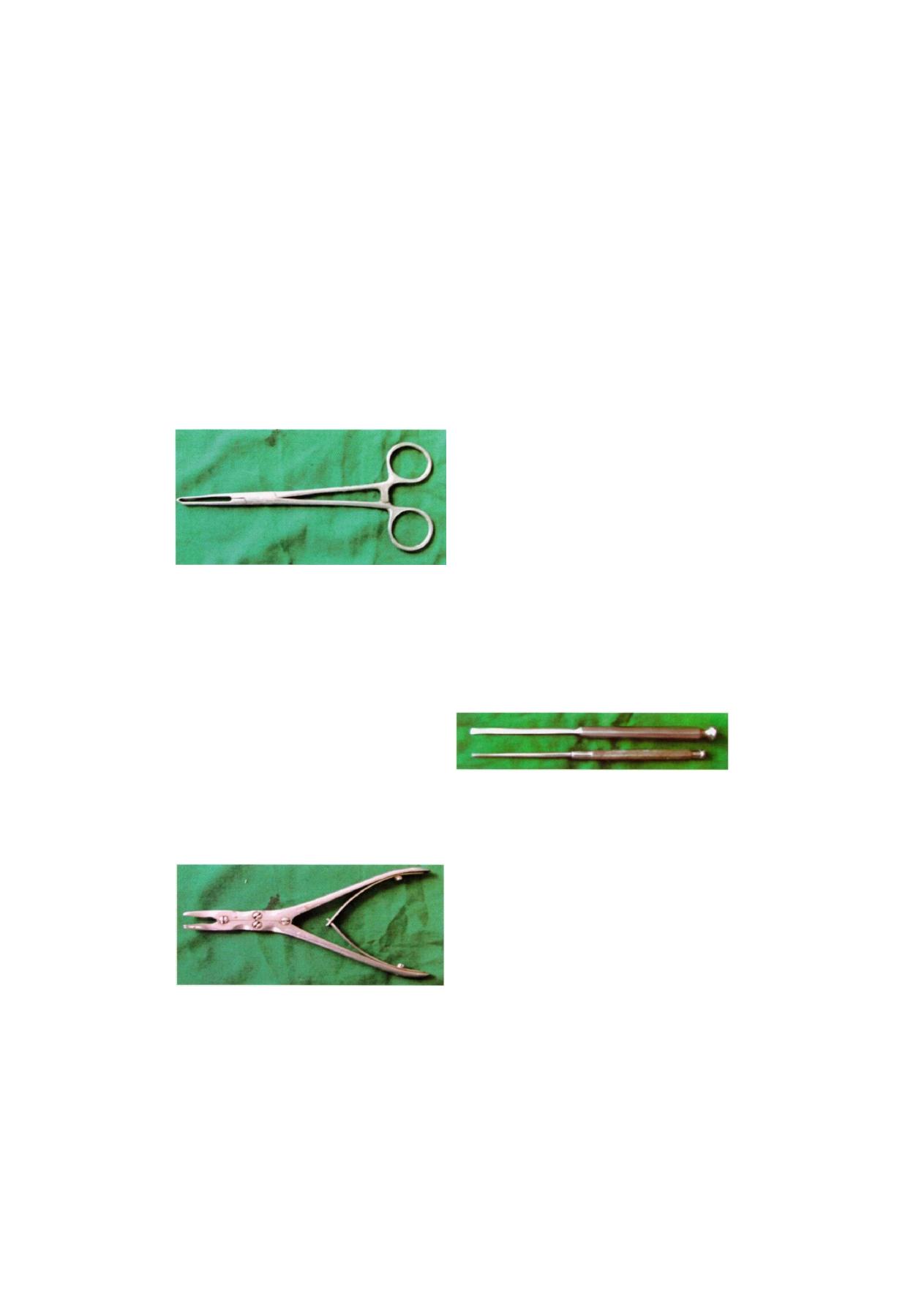
INSTRUMENTS FOR REMOVING BONE
RONGEUR FORCEPS
The instrument most commonly used for removing bone
is the rongeur forceps. These instruments have sharp
blades that are squeezed together by the handles cutting
or pinching though the bone. Rongeur forceps have a
spring between the handle so that when hand pressure
is released the instrument will open. This allows the
surgeon to make repeated cuts of bone without making
special efforts to open the instrument. There are two
major designs for rongeur forceps, a side-cutting forceps,
end-cutting forceps (Figure 2.26).
The end-cutting forceps are more practical for most
dentoalveolar surgical procedures that require bone
removal. These forceps can be inserted into sockets for
F i g u r e 2.26: Rongeur forcep
removal of inter-radicular bone. They can also be used
to remove sharp edges of bone. Rongeurs can be used
to remove large amounts of bone efficiently and quickly.
Because rongeurs are relatively delicate instrument, the
surgeon should not use the forceps to remove large
amounts of bone in single bites. Rather, smaller amounts
of bone should be removed in each of multiple bites.
Likewise, the rongeurs should not be used to remove
teeth, since this practice will quickly dull and destroy the
instrument. Rongeurs are usually quite expensive so care
should be taken to keep them in working order.
CHISEL AND MALLET
One of the obvious methods of bone removal is to use
a surgical chisel and mallet. Bone is usually removed
with a mono bevel chisel, and teeth are usually sectioned
with a bi-bevel chisel. The success of chisel use depends
on the sharpness of the instrument. Therefore, it is
necessary to sharpen the chisel before it is sterilized for
the next patient. Some chisels have carbide tips and can
be used more than once between sharpening. A mallet
with a nylon facing imparts less shock to the patient,
is less noisy, and is therefore recommended (Figure 2.27).
F i g u r e 2.27: Chisel and and osteotome
BONE FILE
Final smoothing of the bone before suturing the
mucoperiosteal flap back into position is usually
performed with a small bone file. The bone file is usually
a double ended-instrument with a small and large end
(Figure 2.28). It cannot be used efficiently for removal
of large amounts of bone, and it is used only for final
smoothing. The teeth of the bone file are arranged in
such a fashion that they remove bone only on a pull
stroke. Pushing the bone file results only in burnishing
and crushing the bone and should be avoided (Figure
2.28).
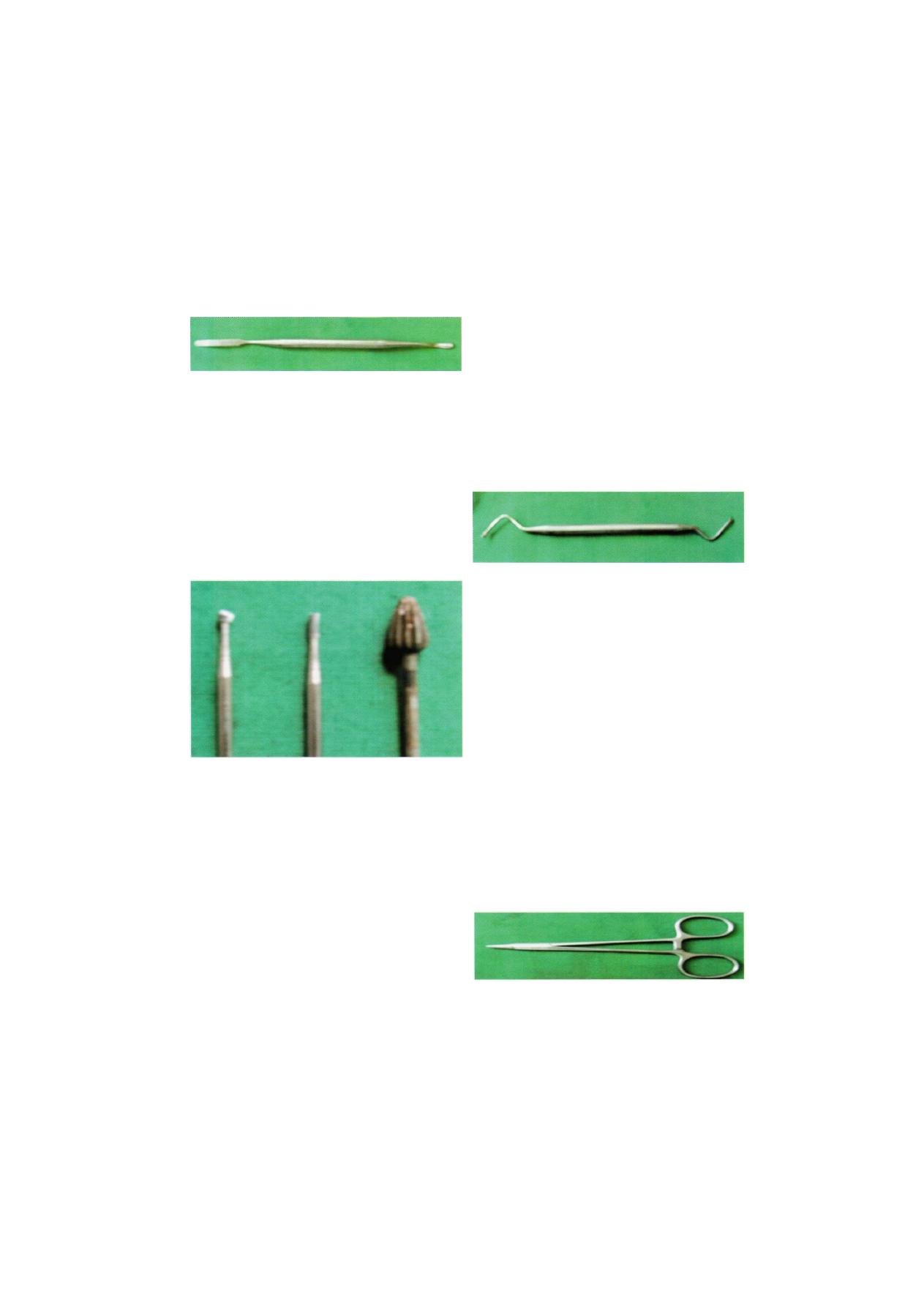
16
Exodontia Practice
Figure 2.28: Bone file
BUR AND HANDPIECE
A fine method for removing bone is with a bur and
hand-piece. This is the technique that most surgeons
use when removing bone. Relatively high-speed
handpieces with sharp carbide burs remove cortical bone
efficiently. Burs such as fissure bur, round bur are
commonly used. Occasionally, large amounts of bone
need to be removed such as in torus reduction. In these
situations, a large bone bur that resembles an acrylic
bur is used (i.e. carbide trimmer) (Figure 2.29).
F i g u r e 2.29: Different types of burs
The handpiece that is used must be completely
sterilizable in a steam autoclave. When a handpiece is
purchased, the manufacturer's specifications must be
checked carefully to ensure that sterilization is possible.
It should have relatively high speed and torque. This
allows the bone removal to be done rapidly and allows
efficient sectioning of teeth. The handpiece must not
exhaust air into the operative field as dental drills do.
Most high-speed turbine drills used for routine restorative
dentistry cannot be used. The reason is that the air
exhausted into the wound may be forced into deeper
tissue planes and produce tissue emphysema, a
potentially dangerous phenomenon.
INSTRUMENTS TO REMOVE SOFT TISSUE
FROM BONY DEFECTS
The curette, sometimes called the periapical curette, is
an angled, double-ended instrument used to remove soft
tissue from bony defects (Figure 2.30). The principle
use is to remove granulomas or small cysts from
periapical lesions, but it is also used to remove small
amounts of granulation tissue debris from the tooth
socket. The periapical curette is distinctly different from
the periodontal curette in design and function.
F i g u r e 2.30: Bone curette
INSTRUMENTS FOR SUTURING MUCOSA
Once a surgical procedure has been completed, the
mucoperiosteal flap is returned to its original position
and held in place by sutures. The needle holder is the
instrument used to place the sutures.
NEEDLE HOLDER
The needle holder is an instrument with a locking handle
and a short, stout beak. For intraoral placement of
sutures, a 6-inch (15 cm) needle holder is usually
recommended. The beak of the needle holder is shorter
and stronger than the beak of the hemostat. The face
of the beak of the needle holder is crosshatched to permit
a positive grasp of the suture needle and suture (Figure
2.31). The hemostat has parallel grooves on the face
of the beaks, thereby decreasing the control over needle
and suture. Therefore, the hemostat should not be used
for suturing.
Figure 2 . 3 1 : Needle holder

Armamentarium
17
In order to properly control the locking handles and
to direct the relatively long needle holder, the surgeon
must hold the instrument in the proper fashion.
Thumb and ring finger are inserted through the rings.
The index finger is held along the length of the needle
holder to steady and direct it. The second finger aids
in controlling the locking mechanism. The index finger
should not be put through the finger ring, because this
will result in dramatic decrease in control.
SUTURE CUTTING SCISSOR
Usually sutures are cut at the end of eighth day. Scissor
used for this purpose is specially designed so that it can
reach to the most posterior teeth (Figure 2.32).
F i g u r e 2.32: Suture cutting scissor
NEEDLE
The needle is held approximately two thirds of the
distance between the tip and the end of the needle. This
allows enough of the needle to be exposed to pass
through the tissue, while allowing the needle holder to
grasp the needle in its strong portion to prevent bending
of the needle (Figures 2.33A to C ) . The needle used in
closing mucosal incisions is usually a small half circle
or three-eighth circle suture needle. It is curved to allow
the needle to pass through a limited space where a
straight needle can not reach. Suture needles come in
a large variety of shapes from very small to very large.
The tips of suture needles are either tapered, such as
a sewing needle, or have triangular tips that allow them
to be cutting needles. A cutting needle will pass through
mucoperiosteum more easily than the tapered needle.
The cutting portion of the needle extends about one-
third the length of the needle, and the remaining portion
of the needle is round. The suture can be threaded
through the eye of the needle or can be purchased
already swaged. If the dentist chooses to load his own
1/4 ( ircle 3/81
ircle
1/2 (
J _
ircle , 5/8 c
^|
J ^
Straight
V
El
ra
El
ra
Micropoint spatula £
sj
C. A n a t o m y of a s u r g i c a l needle
F i g u r e s 2.33A to C: Shape, size and anatomy of sutural
needles

18
E x o d o n t i a P r a c t i c e
T a p e r c u t ^ ^ Z ^
B
o
d
y
F i g u r e 2.34A: Different shapes at needle
F i g u r e 2.34B: Tissue disrup- Figure 2.34C: Tissue disrup-
tion is more by double surface t i o n m i n i m i z e d by s i n g l e
stand with eyed needle s u t u r e s t r a n d s w a g e d to
needle
needles for the sake of economy, he must use needles
that have eyes, as has a typical sewing needle. Needles
that have eyes are larger at the tip and may cause slightly
increased tissue injury when compared to the swaged-
on needles (Figures 2.34A to C ) .
SUTURE MATERIAL
Many types of suture materials are available for use.
The materials are classified as resorbable and non-
resorbable, natural and synthetic, monofilament and
polyfilament.
The size of suture is designated by a series of zeros.
The size most commonly used in the suturing of oral
mucosa is 3-0 (000). A larger size suture would be
2-0, or 1-0. Smaller sizes would be 4-0, 5-0, and 6-0
sutures. Sutures of very fine size such as 6-0 are usually
used in conspicuous places on the skin such as the face,
since smaller sutures, usually cause less scarring. Sutures
of size 3-0 are large enough to prevent tearing through
mucosa, are strong enough to withstand the tension
placed on them intraorally, and are strong enough for
easy knot-tying with a needle holder.
Sutures may be resorbable or non-resorbable. Non-
resorbable suture materials include types as silk, nylon
and stainless steel. The most commonly used non-
resorbable suture in the oral cavity is silk. Nylon and
stainless steel are rarely used in the mouth. Resorbable
sutures are primarily made of gut. While the term catgut
is often used to designate this type of suture, gut actually
is derived from the serosal surface of sheep intestines.
Plain catgut resorbs relatively quickly in the oral cavity,
rarely lasting longer than 5 days. Gut that has been
treated by tanning solutions (chromic acid) and is
therefore called chromic gut lasts longer, up to 10 to 12
days. Several synthetic resorbable sutures are also
available. These are materials that are long chains of
polymers braided into suture material. Examples are
polyglycolic acid and polylactic acid. These materials are
slowly resorbed, taking up to 4 weeks before they are
resorbed. Such long-lasting resorbable sutures are rarely
indicated in the oral cavity.
Finally, sutures are classified based on whether or not
they are monofilament or polyfilament. Monofilament
sutures are sutures such as chromic gut. If the dentist
chooses to use the disposable needles, then the suture
will be swaged onto the needle.
Armamentarium
INSTRUMENT TO HOLD THE MOUTH OPEN
When performing extractions or other types of surgery
that requires patients to hold their mouths open widely
for prolonged period of time, dentists commonly use
instruments to assist patients. The bite block is just what
the name implies. It is a rubber block upon which the
patient can rest the teeth. The patient opens his or her
mouth to a comfortably wide position and the rubber
bite block is inserted, which holds the mouth in the
desired position. Should the surgeon need the mouth
to open wider, the patient must open wide and the bite
block must be positioned more to the posterior of the
mouth.
The side action mouth gag can be used by the
operator to open the mouth wider if necessary. This
mouth gag has a ratchet-type action opening the mouth
wider as the handle is closed. This type of mouth gag
should be used with caution as great pressure can be
applied to the teeth and temporomandibular joint and
injury may occur with injudicious use. This type of mouth
gag is useful in patients who are deeply sedated.
F i g u r e 2.35: Suction tip
INSTRUMENT TO HOLD TOWELS AND DRAPES
IN POSITION
When drapes are placed around a patient, they must
be held together with a towel clip. This instrument has
a locking handle and finger and thumb rings. The action
ends of the towel clip are sharp, curved points that
penetrate the towels and drapes (Figure 2.36). When
this instrument is used, the operator must take extreme
caution not to pinch the patient's underlying skin.
INSTRUMENT FOR PROVIDING SUCTION
In order to provide adequate visualization, blood, saliva,
and irrigating solutions must be suctioned from the
operative site. The surgical suction is one that has a
smaller orifice than the type used in general dentistry,
so that the tooth sockets can be suctioned in case a
root tip is fractured and adequate visualization is
necessary. Many of these suctions are designed with
several orifices, so that the soft tissue will not become
aspirated into the suction hole and cause tissue injury
(Figure 2.35).
The suction has a hole in the handle portion that
can be covered as the need dictates. When hard tissue
is being cut under copious irrigation, the hole is covered
so that the solution is removed rapidly. When soft tissue
is being suctioned, the hole is uncovered to prevent tissue
injury.
Figure 2.36: Towel clips
INSTRUMENTS FOR IRRIGATION
When a handpiece and bur are used to remove bone,
it is essential that the area be irrigated with a steady stream
of irrigating solution, usually sterile saline. The irrigation
cools the bur and prevents bone damaging heat
build-up. The irrigation also increases the efficiency of
the bur by washing away bone chips from the flutes of
the bur and by providing a certain amount of lubrication.
Additionally, once a surgical procedure is completed and
before the mucoperiosteal flap is sutured back into

20
Exodontia Practice
position, the surgical field should be irrigated thoroughly
with saline. There are two major systems for accomp-
lishing this. The bulb syringe can be used effectively and
can be refilled easily with one hand. However, the
disadvantage is that it is difficult to sterilize. More
commonly, a large plastic syringe with a blunt 18-gauge
needle is used for irrigation purposes. Although the
syringe is disposable, it can be sterilized multiple times
before it must be discarded. The irrigation needle should
be blunt and smooth so that it does not damage soft
tissue, and it should be angled for more efficient direction
of the irrigating stream.
Anatomical
Considerations

22
Exodontia Practice
Differential diagnosis of the source, or the course, of
pathology in the facial area may, in many instances,
depends on depth understanding of the structure and
relations of the alveolar processes. The extraction of teeth,
surgical exposure of root tips, surgical access to the
maxillary sinus, surgical preparation for oral prosthesis,
etc. must obviously proceed from a familiarity with the
detail and variation found in alveolar structures and their
relations. Planning local anesthesia where the anesthetic
fluid must penetrate the cortical plates to reach the nerves
within the medullary bone clearly depends on knowing
the structural minutiae details of these parts.
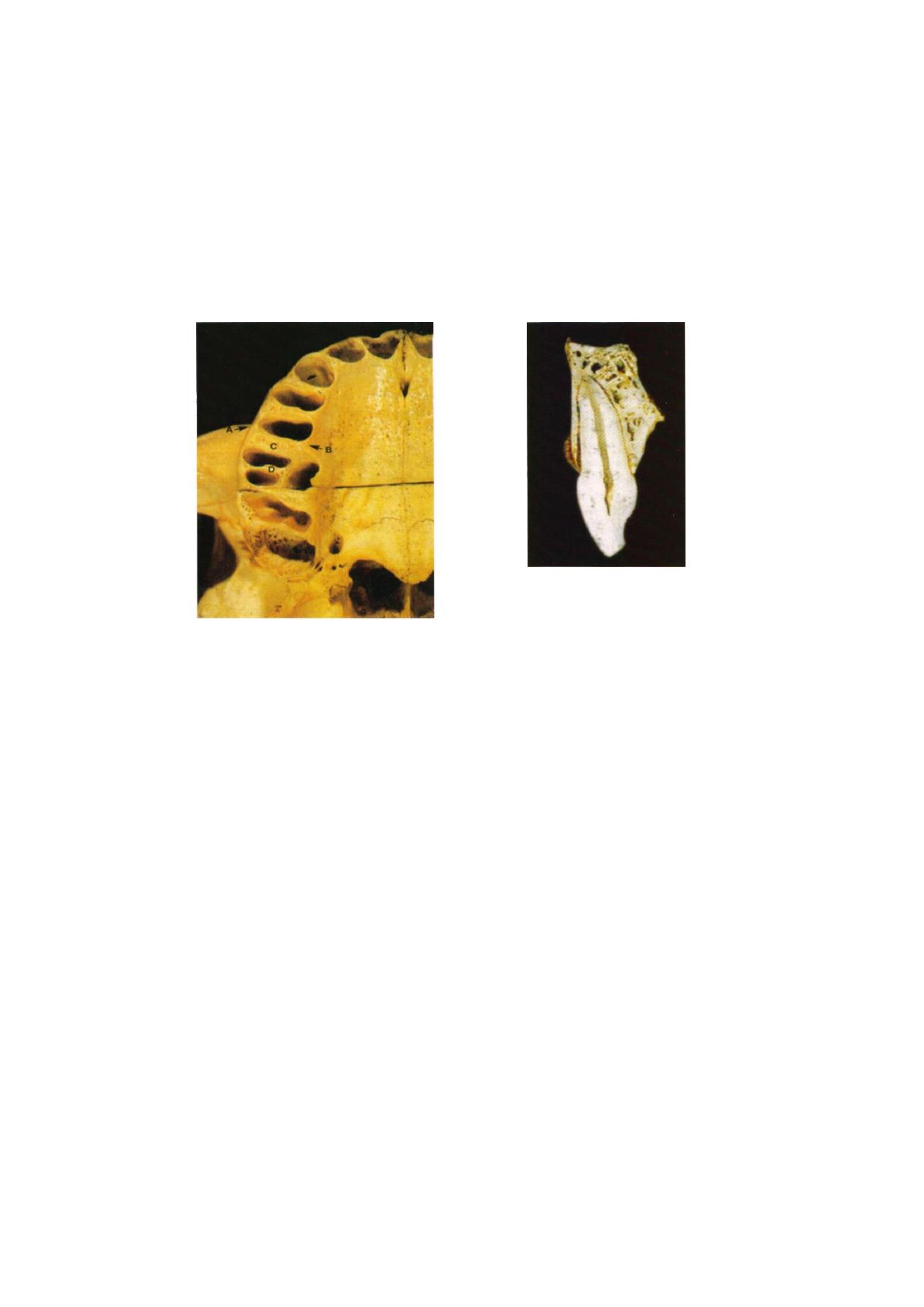
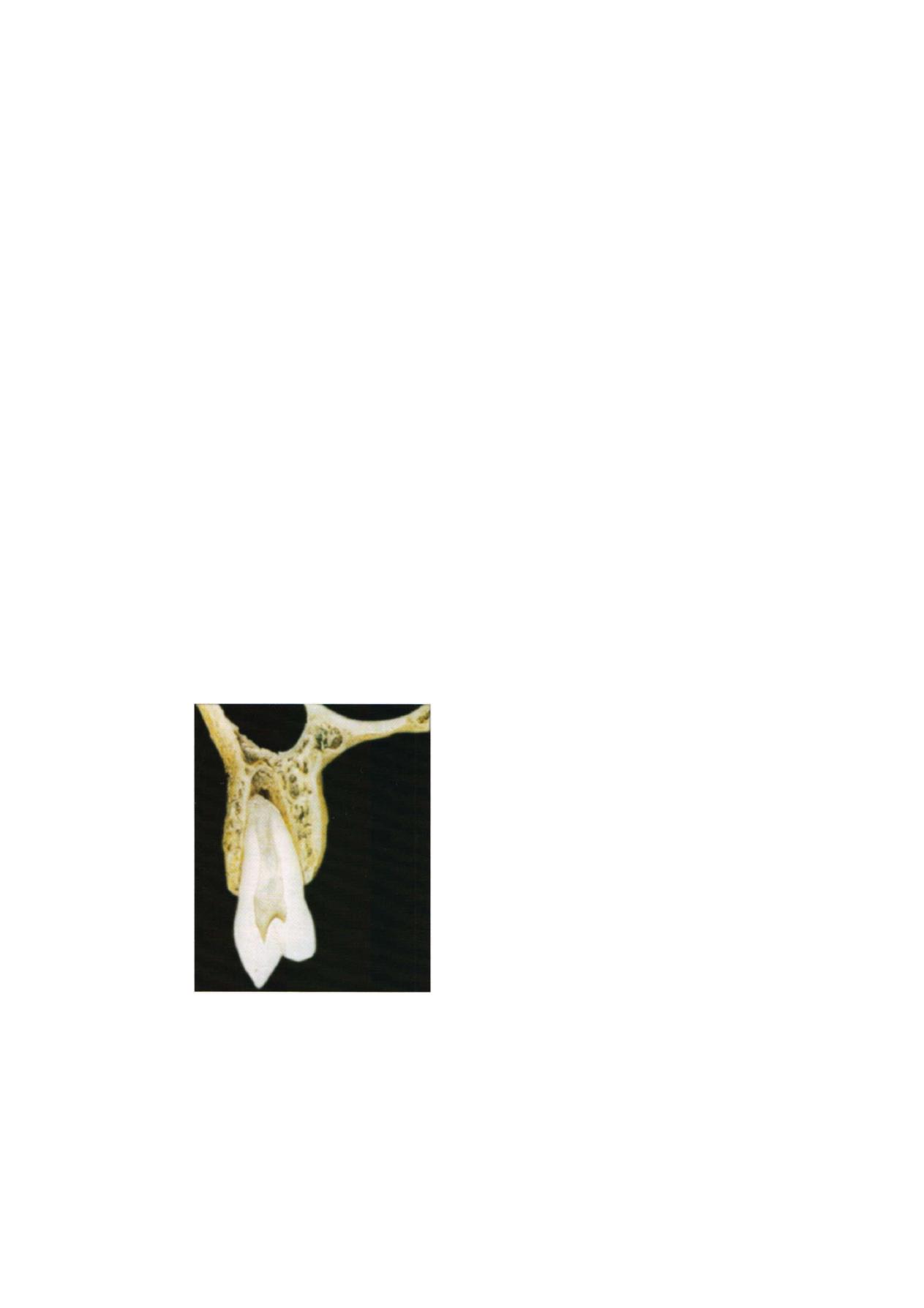
ALVEOLAR PROCESS OF THE MAXILLA
The alveolar process of the maxilla is in relation with
the floor of the nasal cavity and the floor of the maxillary
sinus. Its relation to these cavities is determined by the
functional structure of the maxilla. The canine pillar of
the maxilla, arising from the socket of the canine and
extending upward along the lateral border of the piriform
aperture into the frontal process of the maxilla, is the
most constant bony structure in the base of the alveolar
process (Figure 3.1). The canine pillar is situated lateral
to the entrance into the nasal cavity. Being a functional
reinforcement of the bone, it determines the medial and
anterior expansion of the maxillary sinus, which replaces
nonfunctional bone. It is, therefore, a general rule that
the incisors are below the floor of the nasal cavity, the
premolars and molars are below the floor of the maxillary
sinus, and the canine occupies a neutral position between
the two cavities. This is true even if the nasal cavity is
abnormally wide, because the widening does not
markedly involve the area in front of the incisive canal.
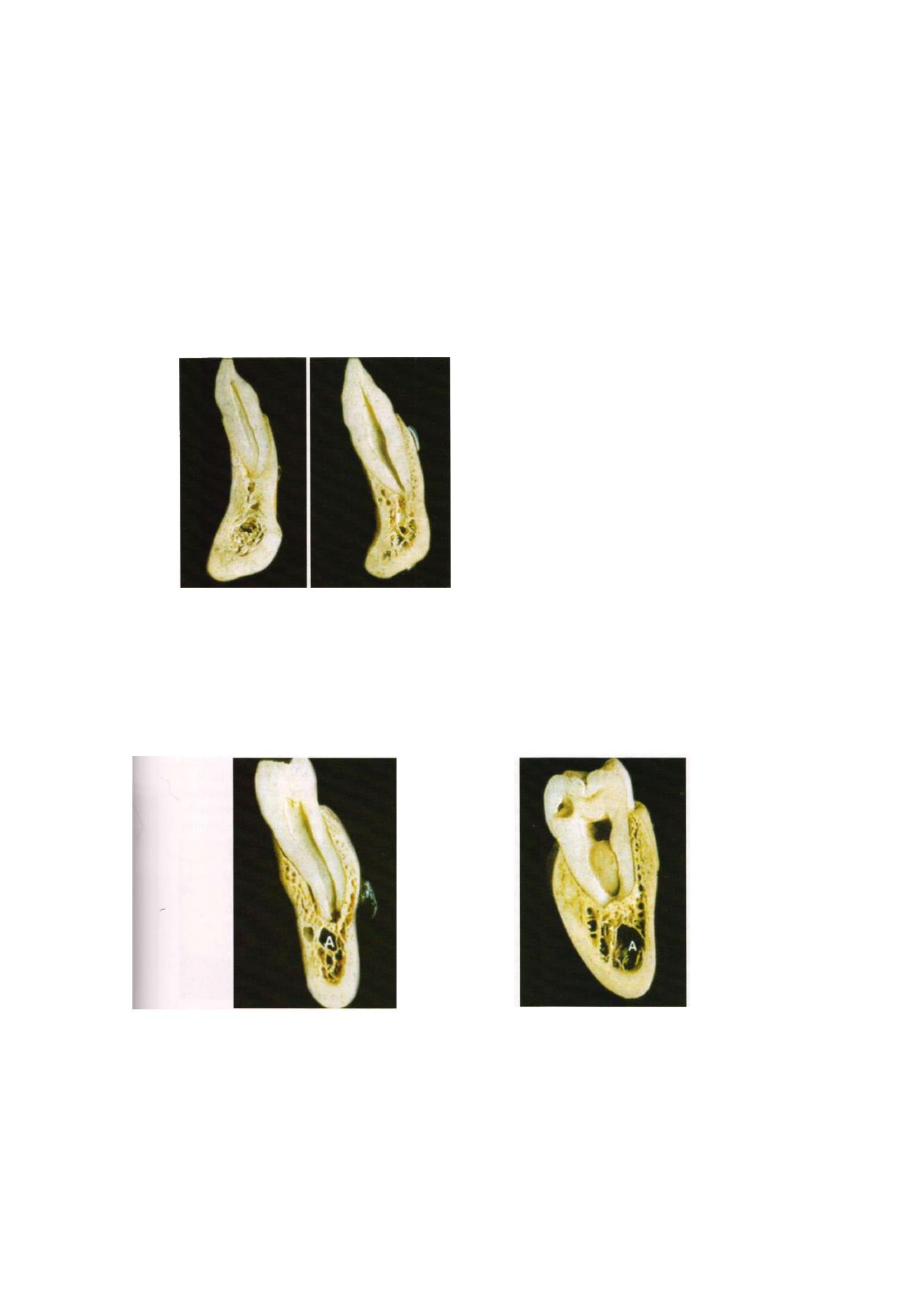
The relations of the apices of the incisors to the nasal
floor are dependent on two factors: height of the face,
especially height of the upper alveolar process, and length
of the incisor roots. Since these two measurements are
not correlated, it is necessary to examine each case
individually and to ascertain the relations between the
incisor sockets and the nasal floor by radiographic
examination. It is a general rule that the root of the lateral
incisor does not show as close a relation to the nasal
floor as does the root of the central incisor, because the
root of the lateral incisor tends to curve toward the outer
rim of the nasal aperture. In addition, it has to be
remembered that the floor of the nasal cavity ascends
slightly laterally, which also increases the distance
between the fundus of the socket of the lateral incisor
and the nasal floor (Figures 3.2A and B ) .
In persons with a relatively short alveolar process and
long roots, the central incisor may actually reach the thin
F i g u r e 3 . 1 : Relation of maxillary teeth with
nasal floor and maxillary sinus
F i g u r e 3.2A: Maxillary teeth
Anatomical Considerations
23
F i g u r e 3.2B: Thickness of alveolar process
of maxillary teeth
compact bony plate that forms the floor of the nasal
cavity. The apex of the tooth is then separated from the
nasal cavity by only a thin plate of bone. In the other
extreme a rather thick layer of spongy bone may be
interpose between the nasal floor and the socket of the
central incisor.
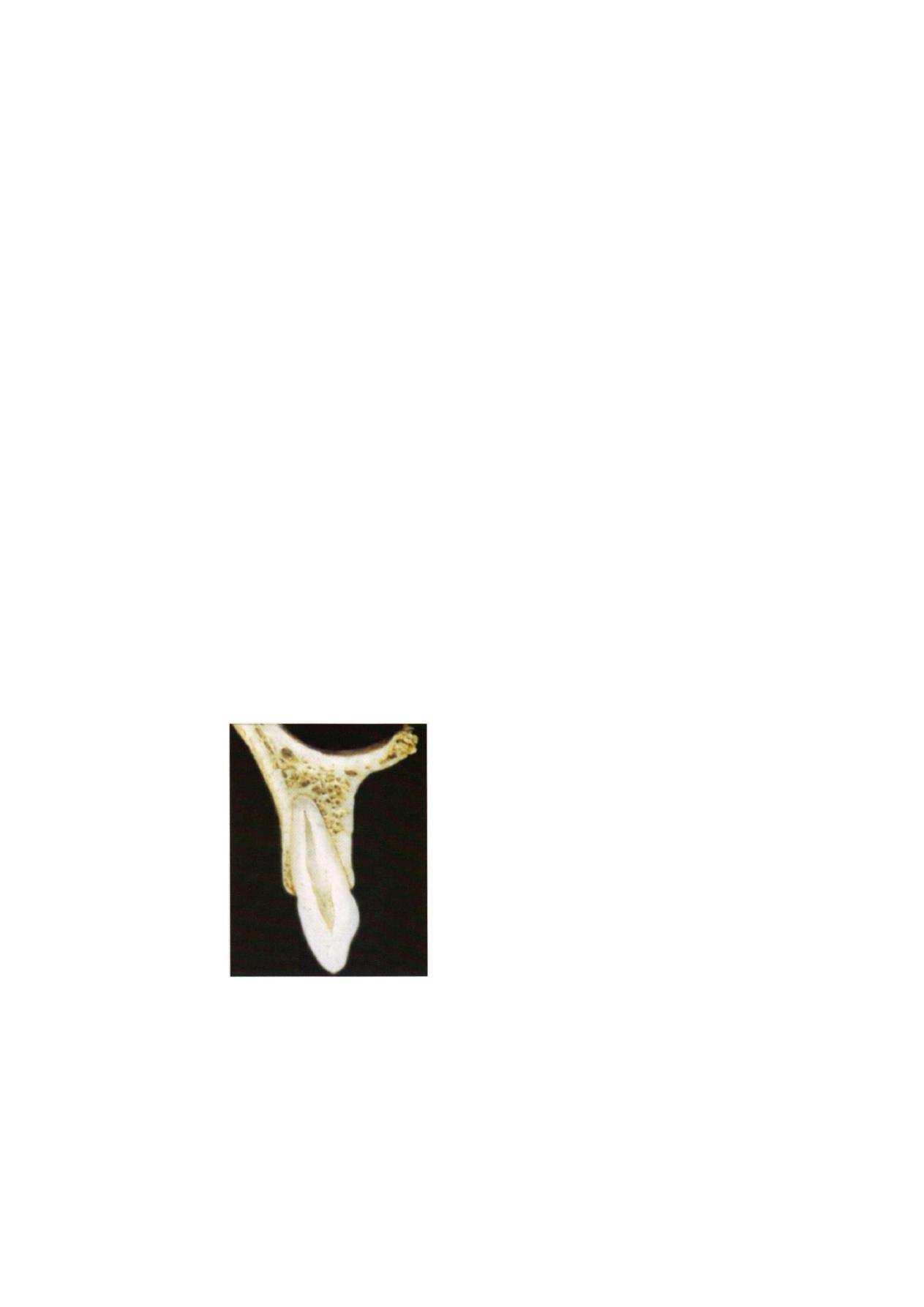
The apex of the lateral incisor shows, in principle,
the same variations in its relation to the nasal floor, but
it rarely actually comes into contact with the nasal floor
(Figure 3.3) The configuration of the alveolar process
in the incisal region is, dependent on the formation of
the palate. The inner plate of the alveolar process ascends
at a moderate angle if the palate is low and then curves
without a break into the horizontal roof of the oral cavity.
If the palate is high, the inner plate of the alveolar process
is steep in its anterior part, and there is a fairly sharp
angle between the alveolar process and the roof of the
mouth. These variations decisively influence the amount
and the configuration of the spongy bone, the
retroalveolar spongiosa, between the outer and inner
Figure 3.3: Lateral incisor in alveolar bone
plates of the alveolar process and the nasal floor. In a
flat or low palate this space is roughly triangular and
rather wide. In a high palate the retroalveolar spongiosa
is restricted and occupies, a more rectangular area.
It has to be remembered that the difference between
a low and a high palate is expressed not only in
quantitative measurements but also in the changed
configuration of the palate. In the incisor region the
differences in shape and in the molar region the differen-
ces in relative size are more prominent, whereas the
premolar area is a zone of transition. In the anterior
region of the maxilla the inclination of the inner alveolar
plate, or palatine plate, is slight in the low palate and
steep in the high palate. In the molar region of the maxilla
the angle between the oral roof and the inner surface
of the alveolar process is always nearly a right angle,
so that the high palate is characterized mainly by an
increase in the length of the alveolar process.
The sockets of the incisors are eccentrically placed
in the alveolar process, the axis of the root and socket
being more nearly vertical than the axis of the alveolar
process. Thus, the alveolar bone proper on the labial
surface of the root fuses with the external plate of the
alveolar bone, whereas palatally a wedge-shaped area
2
Exodontia Practice
of spongy bone is found between the alveolar bone
proper and the palatine or inner plate of the alveolar
process. This is why abscesses originating in the incisor
teeth in most instances perforate the labial plate of the
alveolar process and open into the vestibule of the oral
cavity. There is, however, one important exception to
this rule. In a rather high percentage of incisors the apical
part of the root of the lateral incisor is sharply curved
lingually, and its apical foramen is placed in or near the
center of the retroalveolar spongiosa and rather distant
from the outer alveolar plate.
The relations of the incisors to the nasal floor explain
the fact that an abscess arising from the central incisor
may open into the nasal cavity or that a radicular cyst
of an incisor may bulge into the inferior nasal meatus,
even causing an occlusion of the nostril.
The canine is embedded in the lower part of the
canine pillar of the maxilla . If this pillar contains a great
amount of spongy bone, it is continuous with the retro-
alveolar spongiosa in the incisal region (Figure 3.4).
Because of the position of the canine tooth in the canine
pillar, neither nasal cavity nor maxillary sinus has intimate
relations to the socket and the root of the canine. In
extreme cases, however, the maxillary sinus may extend
Figure 3.4: Canine position in the maxillary alveolus
forward so that it approaches the distolingual circum-
ference of the socket of the canine in a rather broad
front. The same is sometimes true for the nasal cavity,
which approaches the mesiolingual surface of the canine.
The relation of the canine to the plates of the alveolar
process is, in principle, the same as that of the incisors,
its root being eccentrically embedded in the alveolar
process. The compactness and the size of the canine
root cause an even greater bulging of the socket toward
the labial surface of the alveolar process, and the alveolar
eminence of the canine tooth is the most prominent
in the upper jaw.
The premolars and molars are, as a rule, situated
below the floor of the maxillary sinus. Whether the
relations between the tooth and the sinus are intimate
or not depends on the development of the inferior
alveolar recess of the maxillary sinus. But even in cases
in which the base of the alveolar process is deeply
excavated by the maxillary sinus, the first premolar is
almost always farther removed from the floor of the
sinus than are the second premolar and the molars,
because in the premolar area the floor of the sinus arises
before continuing into the anterior wall. This, in turn,
is correlated to the widening of the canine pillar at its
base. Thus, with exception of extreme expansion of the
maxillary sinus, the alveolar fundus of the first premolar
is separated from the sinus floor by a layer of spongy
bone.
The transition of the inner plate of the alveolar process
into the horizontal part of the hard palate occurs in the
region of the first premolar in a more pronounced angle,
and differences between a low and a high palate are
here of a more quantitative character than they are in
the anterior region of the maxilla. The relation of the
first premolar socket to the alveolar process as a whole
and to the retroalveolar spongiosa varies according to
the formation of the root. If the first premolar has a single
root, the socket is in close relation to the outer alveolar
plate and is separated from the inner plate by spongy
bone. As in the incisor-canine area, the outer alveolar
plate is, in reality, a fusion between the alveolar bone
Anatomical Considerations
25
proper and the alveolar plate and often is extremely thin.
In many persons the outer plate may even be defective,
or fenestrated, especially in the apical third of the alveolar
eminence. If the first premolar possesses two roots, the
buccal one is closely applied to the outer alveolar plate,
whereas the socket of the lingual root is placed almost
in the center of the retroalveolar spongiosa.
The relation of the second premolar to the maxillary
sinus is closer than that of the first premolar. Only if the
alveolar recess of the maxillary sinus is absent or poorly
developed does a layer of spongy bone intervenes
between the socket of the second premolar and the floor
of the sinus. In the majority of persons the floor of the
sinus dips down into the immediate neighborhood of
the second premolar. Its socket is then separated from
the sinus only by a thin layer of compact bone. The sinus
may even extend below the level of the alveolar fundus
of the second premolar, and the socket causes a slight
prominence at the floor of the sinus. If the expansion
of the sinus goes further, the thin bony plate between
the sinus and the socket of the second premolar may
F i g u r e 3.5: Premolar in maxillary alveolar bone
showing relation with maxillary sinus
even disappear, so that only soft tissues separate the apex
of the root from the cavity of the sinus; in other words,
the periodontal tissue is then in direct contact with the
mucoperiosteal lining of the sinus. In the region of the
second premolar the inner alveolar plate is more nearly
vertical, except in cases of extremely low palate. The
retroalveolar spongiosa is reduced, and it almost
disappears in the region of the molars (Figure 3.5).
Intimate relations between the tooth and the maxillary
sinus are the rule in the region of the molars. The inter-
vention of a substantial layer of bone between the
alveolar fundus and the maxillary sinus is here an
exception. The sockets of the molars almost always reach
the floor of the sinus, and frequently the apices of some
or all of the molar roots protrude into the sinus, where
small rounded prominences at the floor of the sinus
mark the position of the root apices. Bony defects at
the height of these prominences are not at all rare and
sometimes are of fairly large extent. The divergence of
the molar roots, especially in the first molar, frequently
permits an extension of the sinus downward toward the
furcation of the roots. Often sickle-shaped buttresses of
bone traverse the floor of the sinus in a frontal plane
between the molars whose roots protrude into the sinus.
Sometimes these ridges connect the prominence of one
of the buccal roots with that of the lingual root. Branches
of the alveolar nerves, destined for the palatal roots of
the molars, use these sickle-shaped folds as bridges; they
run in narrow canals that often are open toward the
sinus for a variable length. The bony crests divide the
alveolar process into several chambers, a peculiarity that
should be kept in mind in the search for a root fragment
that has been displaced into the sinus.
Differences in the relation between the first and the
second molars to the sinus are caused mainly by the
greater divergence of the palatal and the buccal roots
in the first molar. The palatal root of the first molar
frequently extends toward the base of the bony partition
between the nasal cavity and the maxillary sinus and
may, in extreme cases, even extend toward the lateral
area of the nasal floor.
26
Exodontia Practice
Behind the socket of the upper third molar the
posterior end of the alveolar process forms a variably
large knob-shaped bony prominence, the alveolar
tubercle. The junction of the maxilla and the pterygoid
process of the sphenoid bone, mediated usually by the
palatine bone, occurs at a variable level-above the free
margin of the alveolar process behind the last molar.
If this junction is high and if the alveolar tubercle is
hollowed out by the maxillary sinus, the bone behind
the maxillary third molar is weak. If the extraction of
a third molar is attempted by applying an instrument
that exerts pressure distally, the entire corner of the
maxilla may be broken off and the wisdom tooth is not
removed from its socket, but the tooth and socket are
separated from the maxilla. As a consequence of this
fracture, the oral cavity and the maxillary sinus
communicate through a wide opening. The possibility
of this alveolar fracture should caution against attempts
to extract or to loosen the upper third molar by
introducing an elevator between the second and third
molars and exerting pressure distally.
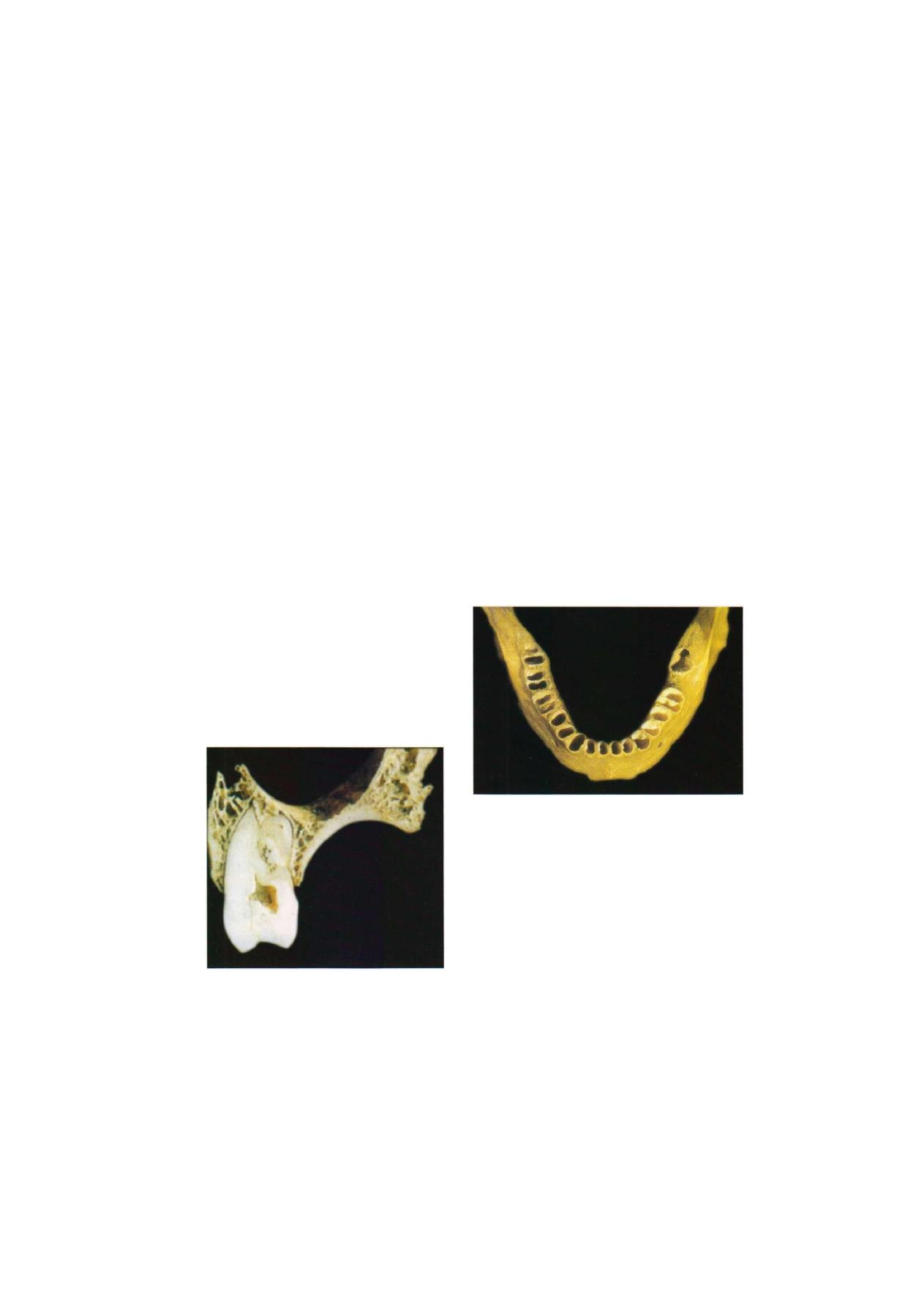
The vertical position of the inner plate of the alveolar
process in the molar region restricts the retroalveolar
spongiosa to small areas lingual to the mesiobuccal root
because the lingual root is situated alongside the
F i g u r e 3.6: Position of the molar in
maxillary cellular process
distobuccal root. The socket of the lingual root fuses
with the inner plate of the alveolar process or is at least
close to it. Mesial to the lingual root, however, a block
of spongy bone intervenes between the socket of the
mesiobuccal root and the lingual plate of the alveolar
process. This arrangement of the spongy bone is the rule
in the region of the first and the second molars; it is,
however, often obscured around the third molar because
of the great variability of third molar roots (Figure 3.6).
ALVEOLAR PROCESS OF THE MANDIBLE
Conforming to the great strength and more uniform
solidity of the mandible, the lower alveolar process is
in most areas far stronger than that of the upper jaw.
Only in the incisor and canine areas are the outer and
inner plates of the alveolar process thin; distally,
however, they increases rapidly in thickness (Figure 3.7).
F i g u r e 3.7: Alveolar process of the mandible
It is of clinical importance that the relation of the
alveolar bone proper to the compact plates and the
spongiosa of the alveolar process varies widely. In the
anterior part of the mandible, in the region of the incisors
and the canine, the alveolar process is narrow in the
labiolingual direction, and in most jaws the alveolar bone
proper fuses for the entire length of the root, or at least
for most of its length, with the outer and the inner alveolar
plates (Figures 3.8A and B). Only rarely is there a restricted
zone of spongiosa lingual to the apical part of the socket.
Anatomical Considerations
2
of the alveolar process. The alveolar bone proper is then
fused for a variable length with one of the alveolar plates.
The premolars and the first molar are mostly in close
relation to the outer alveolar plate. The second and third
molars, however, often show a reversed relation, which
is almost a rule for the third molar. This is not so much
the consequence of a different inclination of the last
mandibular teeth but of a medial shift of the alveolar
process itself in relation to the bulk of the mandibular
body. The oblique line on the outer surface of the
mandible in the region of the second and third molars,
and a fairly thick layer of spongy bone is interposed
between the socket and the outer compact layer of the
bone, but this bone cannot be regarded as part of the
alveolar process in a strict sense. The described relations
are of clinical importance because an inflammation
originating in the second and especially in the third molar
will often perforate the inner plate of the mandible. The
variable relations of the socket and root can best be
evaluated in buccolingual sections through the mandible
at the level of the third molar. In such sections the socket
of the wisdom tooth projects on the inner, or medial,
surface of the mandible somewhat like a balconu. and
F i g u r e s 3.8A a n d B: (A) Incisor and canine in
mandibular alveolar process
The position of the sockets of the premolars and
molars in the spongy bone of the mandible varies (Figure
3.9). Only infrequently is the socket symmetrically placed
between the outer and inner plates. In most cases the
position of the socket is asymmetrical; that is, the axis
of the root and the socket is inclined against the axis
F i g u r e 3.9: Position of premolar in the F i g u r e 3.10: Position of molar in the
mandibular alveolar process mandibular alveolar process

28
Exodontia Practice
in some persons it is shifted entirely inside the arch of
the mandibular body. The further the socket projects
inward, the thinner is its lingual wall and the closer is
the apex of the root to the inner surface of the bone
(Figure 3.10).
At or above the level of the fundus of the socket the
mylohyoid line can be seen on the medial surface of
the jaw. The variations in the relation of this line to the
third molar are of great importance because the
mylohyoid muscle, which forms the floor of the oral
cavity, is attached to this line. The relations of the
mylohyoid line to the apex of the third molar depend
on three factors: the height of the mandibular body, the
anteroposterior length of the mandibular alveolar
process, and the length of the roots of the third molar.
The level of the apex of the third molar roots is found,
as a rule, below the level of the mylohyoid ridge,
especially if the roots of the wisdom tooth are long, if
the alveolar process is relatively short, and if the
mandibular body is of below-average height. It is clear
that in such cases a perforating abscess of the wisdom
tooth will not appear in the oral cavity but below its floor
in the connective tissue of the submandibular region.
Lateral, or buccal, to the alveolus of the lower third molar,
the massive bone forms either a variably wide horizontal
edge or a variably wide and variably deep groove. The
outer edge of this bony field is the oblique line where
it turns anteriorly and inferiorly in continuation of the
anterior border of the mandibular ramus. According to
the relative length of the alveolar process, the wisdom
tooth is either entirely in front of the ascending ramus
or its distal part is flanked by the most anterior part of
the ramus. In the latter case the accessibility of the lower
wisdom tooth is restricted; especially if the superficial
tendon of the temporal muscle is well developed and
accentuates the anteriorly projecting border of the ramus.
Of special importance are the relations of the lower
teeth to the mandibular canal and to its contents, the
inferior alveolar nerve and the accompanying blood
vessels. The second premolar and the molars may be
rather close relation to the mandibular canal itself,
whereas the first premolar shows relation to the mental
canal. Canines and incisors are placed in the region of
the narrow incisive canal, the anterior continuation of
the mandibular canal.
In the relation of the root apices to the mandibular
canal three types can be established. The most frequent
type is that in which the canal is in contact with the
alveolar fundus of the third molar, and the distance
between the canal and the roots increases anteriorly.
When the canal is in proximity to the third molar root,
the thin lamella of bone that bounds the mandibular canal
may even show a fairly large defect, and the periapical
connective tissue of the third molar is in direct contact
with the contents of the mandibular canal. Severe pain
of a neuralgic character after the extraction of a lower
wisdom tooth or during inflammations of its periodontal
ligament is easily explained by these relations.
The other two types of topography of the mandibular
canal occur only in a small number of persons. In cases
of a relatively high mandibular body combined with
roots of moderate length, the mandibular canal has no
intimate relations to any one of the posterior teeth. The
reverse is true in those who have a low mandible and
relatively long roots. In these cases the mandibular canal
may be in close contact with the roots of all the three
molars and the second premolar (Figure 3.11).
The last-described type is normal for children and
most young persons in whom the definite height of the
mandible has not yet been attained. During further
F i g u r e 3 . 1 1 : Relation of tooth apices with inferior
alveolar nerve and mandibular canal

Anatomical Considerations
29
growth, the mandibular body increases in height by
apposition at the free border of the alveolar process,
and the teeth, by their correlated vertical eruption, move
away from the mandibular canal.
The frequent impaction of the lower third molar may
bring about a still closer and more complicated relation
of its root to the mandibular canal and its contents. In
impaction of the wisdom tooth the developing roots
grow into the bone. If the tooth is in an oblique or nearly
vertical position, and if the growing roots are not stunted
or bent, they frequently extend beyond the level of the
mandibular canal. However, an actual meeting between
roots and canal is rare, although a routine radiograph
may give this illusion. Since the impacted lower third
molar is usually lingually inclined, its roots pass the
mandibular canal on its buccal side. Only in a minority
of cases are the roots located lingual to the canal if the
wisdom tooth is abnormally inclined and especially if
there is a considerable lingual shift of the posterior end
of the alveolar process.
In rare instances the roots of an impacted third molar
grow straight toward the mandibular canal and then, con-
tinuing to grow, envelop its contents. The wisdom tooth
then has a root that is, to a variable extent, divided into
a buccal and a lingual part. The mandibular canal may
lie in this abnormal bifurcation, or, if the apices of the
roots fuse below the canal, the alveolar nerve and blood
vessels may pass through a canal in the roots of the
wisdom tooth. The complications caused by this
fortunately rare situation during extraction of such a
wisdom tooth are self-evident. It is as though the loosened
wisdom tooth were held in its socket by an elastic band.
Cutting of this "band" means cutting the alveolar nerve
and blood vessels. In view of these complications, the
routine radiographs should be supplemented by one
taken in vertical projection with the film in the occlusal
plane. If by such a picture the diagnosis of the described
situation can be made, division of the wisdom tooth
into a buccal and a lingual part should be attempted
to liberate the contents of the mandibular canal.
The relations of the first premolar to the mental canal
and foramen deserve special attention. Ordinarily the
mental canal arises from the mandibular canal in the plane
of the first premolar; sometimes its origin is slightly distal
to this plane. From its origin inside the mandible, the
short mental canal runs outward, upward, and backward
to open at the mental foramen, situated between the
two premolars or in the plane of the second premolar.
The oblique course of the mental canal makes it
understandable that its outer end is at a higher and more
posterior level than its inner end. This explains the fact
that in radiographs the mental foramen often is projected
on the apex of the second premolar but rarely on the
apex of the first premolar. Since at this point the
mandibular canal is seldom in the immediate contact to
the apices of these teeth, the mental foramen appears
to have no connection with the mandibular canal and
often is diagnosed wrongly as a pathologic defect of the
bone, for instance as a periapical granuloma.
It was mentioned that in the premolar and molar
region the outer and inner plates of the lower alveolar
process consist of a fairly thick layer of compact bone.
Attempts to anesthetize the inferior dental nerves by
subperiosteal or supraperiosteal injections in this region
are failure. In the region of the canine and incisors this
method of injection is successful if the anesthetic is
injected into the mental fossa above the mental
tuberosity. Two facts make it advisable to inject fairly
close to the lower border of the mandible and rather
far below the level of the apices of the anterior teeth.
The first fact is that the incisal canal is situated at a lower
level than the mandibular canal itself; the second is that
the outer compact of the mandible in the mental fossa
is always perforated by a few small openings that allow
an entrance of the injected fluid into the spongy core
of the bone and thus to the incisive nerve.
Chapter
Indications
and
Contraindications

32
Exodontia Practice
INDICATIONS
Following are the indications of exodontia.
PERIODONTAL DISTURBANCES
They form the common cause for dental extraction in
India. When the teeth are periodontally involved, the
clinician must decide whether to extract the tooth or not.
The final decision depends on (a) the success of
periodontal therapy, (b) patient's attitude towards the
concept of conserving such teeth and (c) economic and
time factors. Even if the patient desires to save the tooth,
loss of more than 40% of periodontal support warrants
extraction.
DENTAL CARIES
When the tooth is extensively damaged by dental caries,
the dental surgeon must evaluate the feasibility of
conserving the carious tooth. Even if the patient and the
dental surgeon desire to save the tooth, it is indicated
for extraction if all the conservative procedures have
failed. This may be either because of technical reasons
or if the patient fails to cooperate. Sometimes, the sharp
margins of the teeth repeatedly ulcerate the mucosa.
Multiple carious teeth may lead to deteriorating oral
hygiene. In such cases, removal of teeth will improve
the oral hygiene.
PULP PATHOLOGY
If endodontic therapy is not possible or if the tooth is
having pulpal pathology, extraction is indicated.
APICAL PATHOLOGY
If the teeth fail to respond to all conservative measures
to resolve apical pathology, either because of technical
reasons or because of the systemic factors, such teeth
are indicated for extraction before the apical pathology
widens with the consequent involvement of the adjoining
teeth.
ORTHODONTIC REASONS
During the course of orthodontic treatment, a few teeth
may require extraction. They fall into any one of the
following reasons:
Therapeutic Extractions
To gain pace during the realignment of malposed teeth,
extraction of teeth like premolars or molars are indicated.
Malposed Teeth
The teeth in the dental arch are malpositioned.
Orthodontist may find it difficult to realign them. In
such circumstances, those teeth are indicated for
extraction.
Serial Extraction
During mixed dentition period, dental surgeon may have
to extract a few deciduous teeth in a chronological order
to prevent malocclusion as the child grows. As part of
preventive dentistry, judicious extraction of deciduous
teeth provides enough space eruption of permanent
successors in a sequential way. This is known as serial
extraction. However before advising extraction, these
teeth require proper evaluation and expert orthodontic
opinion. Otherwise, instead of achieving stability of the
dental arch, injudicious extraction can lead undesirable
esthetics like spacing between teeth may even produce
unacceptable facial profile Therefore, decision for
extraction of teeth for orthodontic reasons should be
based on:
a. Orthodontic assessment
b. Evaluation of the soft tissues like lips, tongue, etc.
PROSTHETIC CONSIDERATIONS
Extraction of teeth is indicated for providing efficient
dental prosthesis. For example, to provide better design
and success of partial dentures, a few selected teeth may
have to be extracted. At the same time, caution is required
if a patient requests the dental surgeon to extract a few

Indications and Contraindications
remaining teeth to enable him to have complete dentures.
It is a known fact that atrophies of the bone results in
decreased denture bearing area and the consequent
decreased denture stability. But the retention of a few
teeth like canines control the atrophy of the jaws.
Likewise, intentional retention of a few teeth may be
helpful to utilize them as abutments. Hence, careful
evaluation by the prosthodontist is necessary for
extracting teeth for prosthetic considerations.
IMPACTIONS
Retention of unerupted teeth beyond the chronological
eruption may sometimes be responsible for facial pain,
periodontal disturbances of the adjoining teeth temporo-
mandibular joint problems, bony pathology like cysts and
pathological fracture of the jaws. Impact ions may
predispose to anterior overcrowding of teeth. Careful
evaluation of such patients including general condition
and professional competence of the dental surgeon are
some of the important considerations for removal of such
impacted teeth.
SUPERNUMERARY TEETH
These teeth may be malpositioned or unerupted. Such
teeth predispose to malocclusion, periodontal distur-
bances, facial pain, bony pathology or may even
predispose to esthetic problems. Unless retention of such
supernumerary teeth are advantageous to the patients,
they are indicated for extraction.
TOOTH IN THE LINE OF FRACTURE
This has been controversial over the course of years.
The present concept is to extract the tooth in the line
of fracture if (a) it is a source of infection at the site
fracture, (b) the tooth itself is fractured, (c) the retention
may interfere with fracture reduction or with healing of
the fracture. Formerly, all the teeth in the line of fracture
were routinely removed. But now, a conservative
approach is advocated and hence extraction of such
teeth requires guarded approach.
TEETH IN RELATION TO BONY PATHOLOGY
They are indicated for extraction. For example, they are
involved in cyst formation, neoplasm or osteomyelitis,
extraction is indicated. However, carefully evaluation is
required before extracting teeth involved in the cyst
formations. If any chance exists for guiding the tooth
to erupt to normal occlusion, efforts must be directed
to conserve such teeth. Hence, proper decision must be
taken based on the individual case.
ROOT FRAGMENTS
They may remain dormant for a long period. Hence,
every patient must be carefully evaluated to decide
whether removal of root fragments is necessary.
For example, roots may be at the submucosal level
producing recurrent ulceration under the denture. Such
ulceration may be painful or may undergo neoplastic
changes. Such roots warrant removal. Sometimes, root
fragment may be involved in the initiation of bony
pathology like osteomyelitis, cyst or neoplasm. If such
fragments are in close association with neurovascular
bundle, the patient may complain of facial pain or
numbness. Statistically, it has been observed that many
broken root fragments remain symptomatic. This has
resulted in the controversy as to whether they are
indicated for removal. As a general rule, very small
fragments may be left alone and the patient is to be kept
under periodical observation. All the other root fragments
are indicated for removal. As the age advances, the
patients become medically compromised. Hence,
removal is indicated as soon as it is diagnosed, instead
of waiting for the symptoms to appear before general
health of the patient presents any problems.
TEETH PRIOR TO IRRADIATION
Irradiation is one of the modalities of treating oral
carcinomas. Previously as a prophylactic measure, all
the teeth in the region of irradiation used to be extracted.
But now, all the precautions are taken to conserve the
teeth prior to irradiation. Hence, all the patients before

Exodontia Practice
irradiation must be carefully examined so that a decision
is taken regarding the extraction of such teeth. If the
oral hygiene can be maintained satisfactorily, routine
prophylactic extraction of these teeth are not to be
encouraged. Only teeth which cannot be maintained in
a sound condition require removal.
FOCAL SEPSIS
Sometimes, teeth may appear apparently sound. But
radiological evaluation is a guiding factor to decide
whether any teeth are to be considered as foci of
infection. In such circumstances, weightage is in favor
of the underlying systemic disorders like dermatological
lesions, facial pain, uncontrollable ophthalmic problems
etc. In such conditions, doubtful teeth are extracted
instead of resorting to any conservative methods of
management.
ESTHETICS
Due to certain compelling reasons like marriage and
job opportunities, some teeth may require attention
for esthetic considerations. But due to time factor, it
may not be possible to improve esthetics by any
conservative orthodontic or surgical means. If so,
such teeth are indicated for extraction, provided it is
followed by immediate prosthetic restoration in a shorter
duration.
ECONOMIC CONSIDERATIONS
Sometimes, the dental surgeon and the patient are faced
with economic constraints even though technically
conservation of teeth may be feasible. In such cases,
extraction may be the only other alternative method of
choice. However, the benefit of doubt is left to the
discretion to the patient in such circumstances and
extraction of teeth is indicated as a last resort.
CONTRAINDICATIONS
Even if the tooth is indicated for removal, the presence
of certain factors makes the tooth contraindicated for
extraction. They may be relative or absolute contraindi-
cations. They can be considered relative, if the
contraindication is provided with additional care, one
can overcome the complication. In other words,
given the situation, the patient is made fit to undergo
extraction, once the underlying condition is treated. On
the contrary, there are a few conditions which are
absolute contraindications. These factors will be the
impediments for extraction, even if care is taken. If
extraction is carried out in the presence of such absolute
contraindications, the outcome may be even fatal. Hence,
it is essential to differentiate between these two types
of contraindications. To avoid legal consequences, it is
preferable to avoid extraction, if the contraindication is
absolute.
The contraindications may also be classified as
systemic or local factors. The presence of absolute
systemic contraindications indicates that this group of
diseases exists in an uncontrolled state. No attempt should
be made by the dental surgeon to thrust extraction on
such patients. By doing so the clinician will be inviting
disaster, e.g. (a) metabolic disorders like uncontrolled
diabetes, (b) uncontrolled cardiac problems, (c) leukemia
(d) renal failure and (e) liver disorders like cirrhosis of
liver. On the contrary, the following contraindications
are examples of relative contraindications. That means,
extraction is to be deferred until the underlying conditions
deserve attention to make the patient fit to undergo
extraction. In such patients, the underlying condition
is to be treated by way of precautions so that;
complications can be avoided due to extraction.
DIABETES AND HYPERTENSION
Usually patients with these systemic problems are under
medication to keep them under control. Hence, patients
with controlled hypertension and diabetes can undergo
extraction. However, it is good to investigate the state
of these disorders in every patient and extraction should
be carried out only after confirming that they are under
control. Such precautions will be a sure way of preventing
any potential complications subsequently.
34

Indications and Contraindications
PATIENTS ON STEROID THERAPY
If patient gives history of cortisone therapy, then, dental
surgeon has to take certain precautions. A physician's
opinion must be taken. Otherwise, the normal precaution
would be to safely double the dose of steroid, one or
two days prior to extraction and to continue one or two
days postoperatively. Then, the dose must be tapered
gradually to the usual dose. Otherwise, the patient is
liable to exhibit adrenal crisis due to stress.
PREGNANCY
The clinician should bear in mind the existence of the
possibility of obstetric complications during the first and
the last trimester. Hence, if possible, extraction can be
carried out after obtaining the obstetrician's expert
opinion.
BLEEDING DISORDERS
The patients who give definite history of bleeding
episodes need careful evaluation. It is not an absolute
contraindication. Complications can be avoided, if the
patient is properly evaluated and adequate precautions
are taken. If necessary, close coordination with the
hematologist is necessary to ensure uncomplicated
recovery of the patient following dental extractions.
Patients with anticoagulant therapy can undergo extrac-
tion after obtaining prior advice from the patient's
physician/cardiologist.
MEDICALLY COMPROMISED PATIENTS
In general, it is better to evaluate these patients pre-
operatively. Great caution should be exercised before
treating this group of patients. Failure to do so may result
in systemic complications.
ACTIVE INFECTIONS
These are relative contraindications. For example,
extraction in the presence of active and uncontrolled
infection will lead to the regional or systemic spread.
Hence, it is preferable to control the infection and
extraction can be safely carried out under the umbrella
of antibiotic therapy.
EXTRACTION OF TEETH IN RECENTLY IRRADIATED PATIENTS
These cases deserve special mention. Irradiation of the
jaws reduces blood supply due to fibrosis.
\
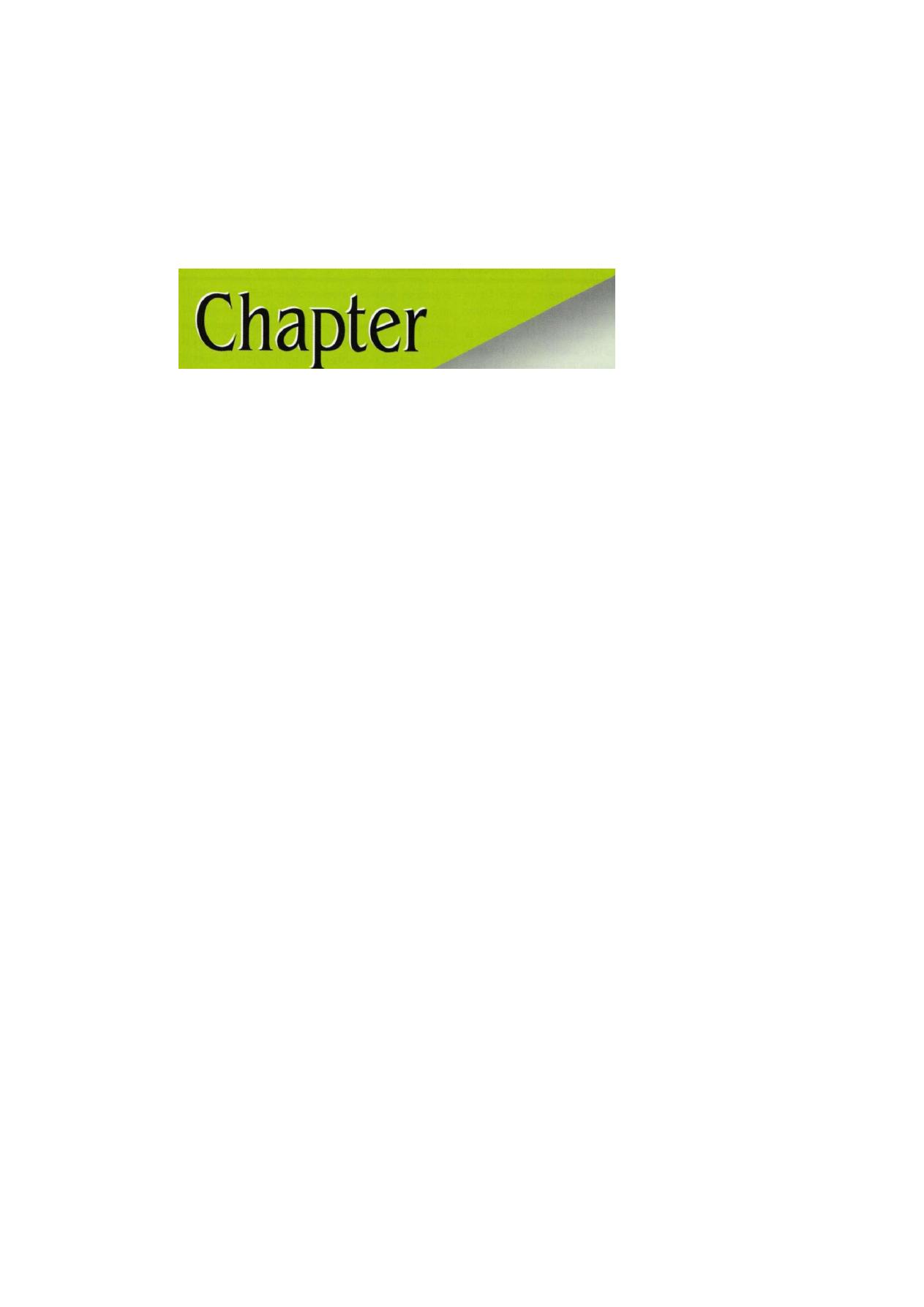
Principles of
Exodontia
5

Exodontia Practice
Dental extraction has always been considered to be an
unpleasant procedure for the patients due to pain phobia.
Geoffrey L Howe: The ideal tooth extraction is
the painless removal of the whole tooth, or tooth
root, with minimal trauma to the investing tissues,
so that the wound heals uneventfully and no post-
operative prosthetic problem is created.
Extraction procedure can be:
1. Simple exodontia or closed method of extraction or
intraalveolar extraction
2. Complicated exodontia or open method of extraction
or transalveolar extraction
Complex extractions are defined as those extractions,
not involving impaction, which cannot be removed by
a simple application of elevators and forceps. Complex
extractions are retrieval of tooth root and teeth which
are likely to fracture or for some other reason and have
an obstacle to extraction.
Extraction of teeth is a surgical operation involving
the bony and soft tissues of the oral cavity, access to
which is restricted by the lips, cheeks, tongue and
movements of the mandible.
Additionally the oral cavity communicates with the
pharynx, which in turn opens into the larynx and
esophagus. The field of operation is flooded by saliva
and is inhabited by the largest number of greatest variety
of microorganisms found in the human body. It also lies
close to the vital centers. Extraction of teeth is a procedure
that incorporates principles of surgery, and many from
physics and mechanics. Most of the teeth can be removed
intact after these principles are followed strictly.
Atraumatic extraction of tooth is a procedure that requires
finesse, knowledge and skill on part of the surgeon. It
is essential to give some careful study and application
of sound surgical principles as is given to surgery in any
other part of the body.
OBJECTIVES
Extraction is one of the most common surgical proce-
dures performed by dental or an oral surgeon. The main
objective is to serve the periodontal attachment carefully
and elevate the tooth out of alveolar socket without
damaging the adjacent structures. While doing extraction
certain amount of trauma is inevitable. Hence, success
in exodontia depends on how the trauma is kept
minimum. The skill and practical wisdom of any clinician
is directly proportional to personal experience and the
knowledge gain.
In general, according to difficulty faced the cases are
classified into four types:
Type 1—easy patient easy case
Type 2—easy patient difficult case
Type 3—difficult patient easy case
Type 4—difficult patient difficult case
Every clinician should bear in mind this classification
as a general rule before undertaking every minor surgery.
GENERAL PRINCIPLES INVOLVED IN
EXODONTIA
• Clinical evaluation
• Radiographic evaluation
• Patient and surgeon preparation
• Patient position
• Operator position
• Principles of extraction
• Principles of elevators
• Postoperative instructions
BASIC REQUIREMENTS
Following are the basic requirements of exodontia:
1. A good radiograph
2. Adequate anesthesia
3. Instruments
4. Adequate illumination
5. Efficient assistance
6. Suction apparatus
CLINICAL EVALUATION
In preoperative assessment period the tooth to be
extracted should be examined carefully to assess the
difficulty of extraction.

Principles of Exodontia
• Access—The first factor to see is the adequacy of
mouth opening. Any limitation of opening may
compromise the ability to do routine extraction.
The cause of limited mouth opening should be
ruled out. Plane for surgical removal is done.
• Status of the supporting structures—The status of
surrounding structure should be evaluated. Presence
of any infection periodontal problems should rule
out. Relation with adjacent vital structure and
maxillary sinus is also determined.
• Status of tooth and crown—The assessment of crown
of the tooth before extraction is always needed.
The presence of large carious lesion, root canal filled
tooth and large restoration should be checked. The
presence of calculus the condition of adjacent tooth
is also evaluated. One must check for the presence
of mobility of teeth.
INTERPRETATION OF A PREOPERATIVE RADIOGRAPH
• Radiographic anatomy
• Condition of surrounding bone
• Assessment of adjacent vital structures
• Assessment of condition of adjacent teeth
• Assessment of tooth in question
As bone density increases, the amount of socket
expansion obtained during forceps extraction becomes
less and tooth removal thus requires more force.
The more dense the bone, the greater the risks for
root fracture and/or fracture of alveolar bone.
Bone density may be interpreted radiographically by
the relative amount of trabeculation. This is only possible
by standardizing the radiographic procedure in your
office. Assessment of radiograph is discussed in details
in the subsequent chapter of exodontia.
PATIENT AND SURGEON PREPARATION
• The concept of universal precautions states that
all patients must be viewed as having blood borne
diseases that can be transmitted to the surgical
team.
• Before extraction: Patients should vigorously rinse
their mouths with an antiseptic mouth rinse such as
chlorhexidine.
To prevent teeth or fragments of teeth from falling
into the mouth and potentially being swallowed or
aspirated into the lungs, it is preferable to place a
4 x 4 inch gauze loosely into the back of the mouth.
However, it should not make the patient gag.
CHAIR POSITION FOR FORCEPS EXTRACTION
• Position of patient, operator and chair are critical for
successful completion of the extraction. Best position
is the one that is most comfortable for the operator
and the patient.
• A proper chair position allows for maximal control
over the force that is being delivered to the patient's
tooth through the forceps.
• A correct position allows:
a. The surgeon to keep the arms close to the body
b. Provide support and stability
c. To keep the wrists straight enough to deliver the
force with the arm and shoulder, and N O T with
hand.
For a Maxillary Extraction
The chair should be tipped backward so that the maxillary
plane is at 45° to the floor (Figure 5.1).
Height of the chair is such that the mouth is at
or slightly below the operator's elbow level (Figure 5.2).
Howe: Site of operation is about 8 cm below the
shoulder level of operator.
Archer: Occlusal plane is at 45° to 90°
• Maxillary right quadrant: The patient's head should
be turned substantially toward the operator for
adequate access and visualization (Figure 5.3).
• Maxillary left quadrant: Patient's head is turned
slightly toward the operator (Figure 5.4).
• Maxillary anterior portion: Patient should be looking
straight ahead (Figure 5.5).
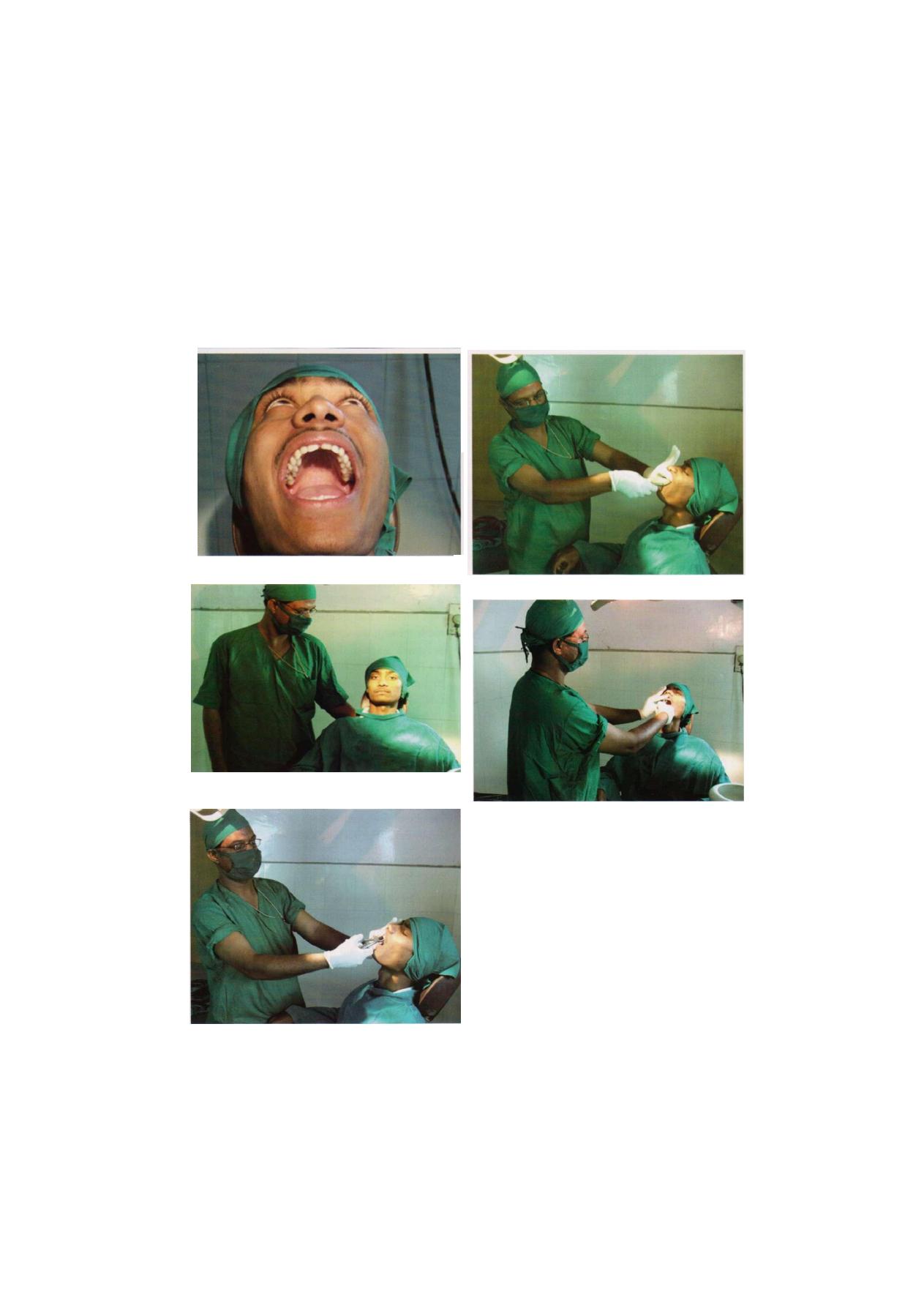
F i g u r e 5 . 1 : Maxillary occlusal plane at
45°
to the floor
F i g u r e 5.4: Maxillary left quadrant tooth extraction
F i g u r e 5.2: Position of patient's head on chair
F i g u r e 5.3: Maxillary right quadrant tooth extraction
• Placement of fingers during extraction
• Maxillary teeth: For the left and anterior teeth,
the left index finger of the surgeon should reflect
the lip and cheek tissue, thumb should rest on
the palatal alveolar process.
For the right side, the index finger is positioned
on the palate and thumb on the buccal aspect
(Figures 5.6A to C ) .
For a Mandibular Extraction
Patient to be positioned in a more upright position so
that the occlusal plane is parallel to the floor when the
mouth is opened widely (Figure 5.7).
F i g u r e 5.5: Maxillary anterior tooth extraction
Exodontia Practice
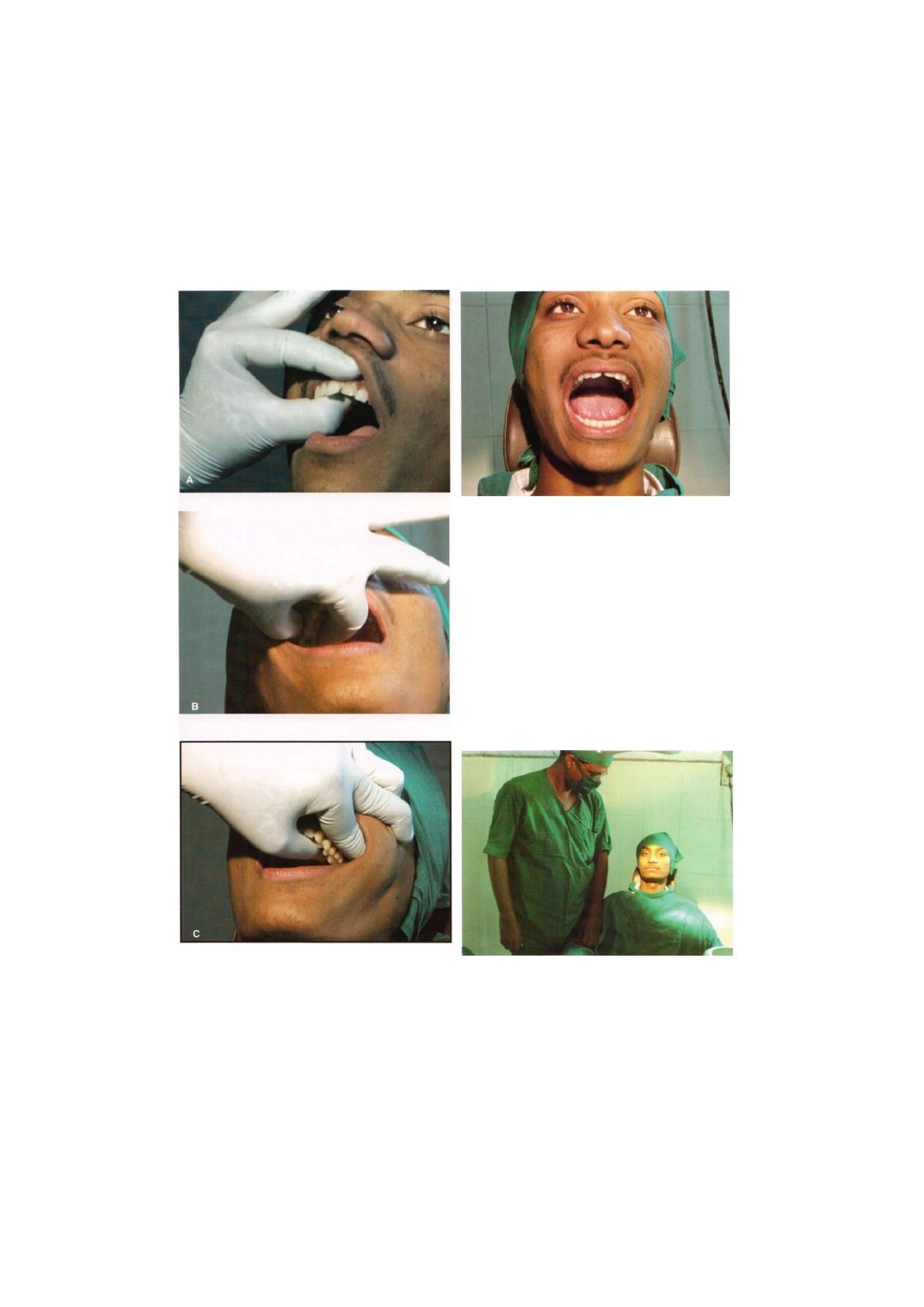
Principles of Exodontia
F i g u r e s 5.6A to C: Position of fingers during extraction of
maxillary teeth
F i g u r e 5.7: Mandibular occlusal plane parallel to floor
The chair should be lower than for extraction of
maxillary teeth, and the surgeon's arm is inclined
downward to approximately a 120° angle at the elbow
(Figure 5.8).
• Mandibular right posterior teeth: Patient's head is
turned toward the surgeon to allow adequate access
to the jaw and the surgeon should maintain proper
arm and hand position. Surgeon is usually at the side
of the patient or at the back at 11° clock position
(Figure 5.9).
• Mandibular anterior region: Surgeon is at the side
or at the front of the patient at 8° clock position (Figure
5.10).
F i g u r e 5.8: Patient's head position on chair
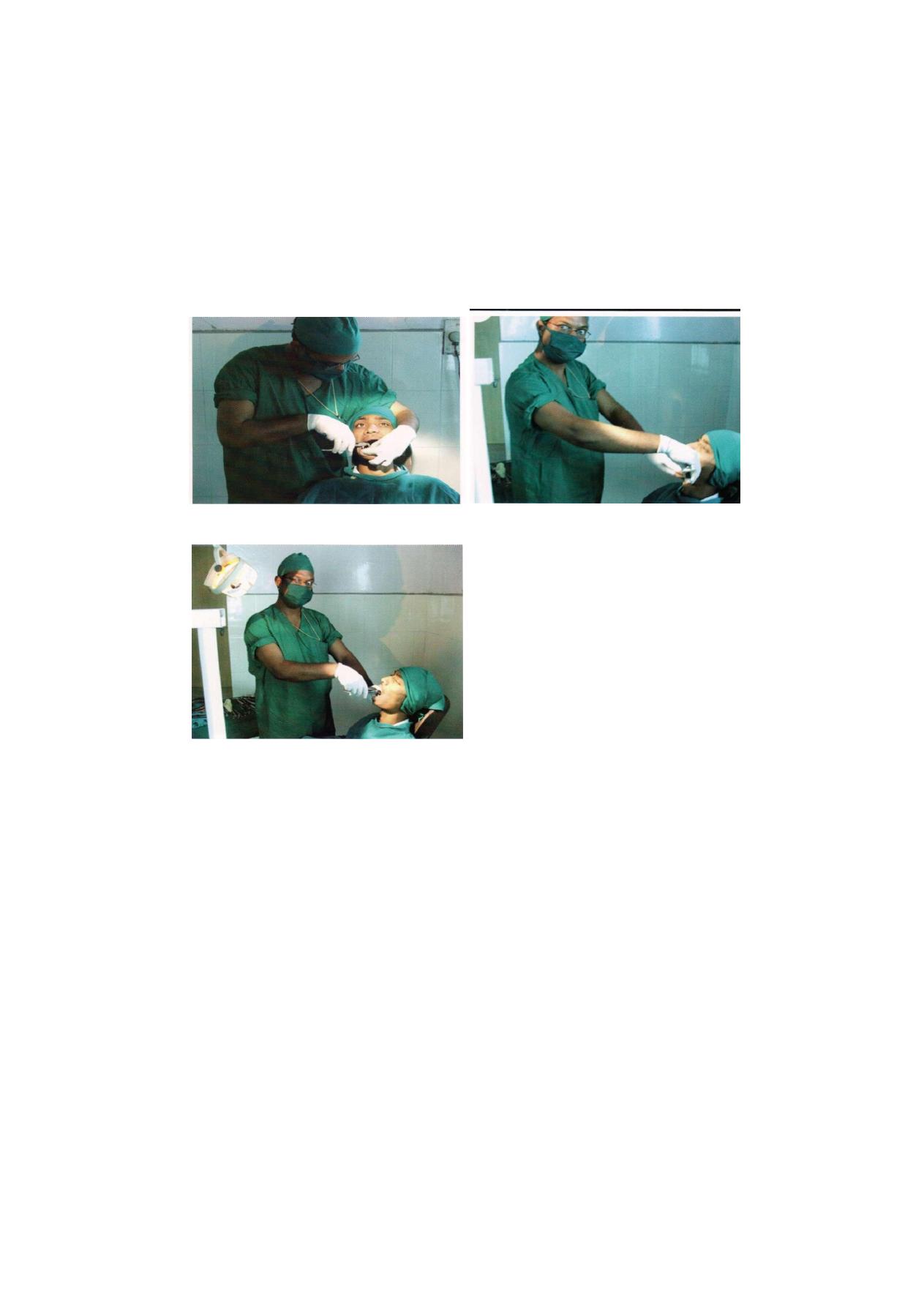
Exodontia Practice
F i g u r e 5.9: Operator position for extraction of mandibular
right posterior teeth
Figure 5.10: Extraction of teeth from mandibular anterior
region
• Mandibular left posterior region: Surgeon should
stand in front of the patient (Figure 5.11).
The operator should stand with his feet apart,
distributing his body weight equally.
Some surgeons prefer to approach the mandible from
the posterior portion. The left hand then goes around
the patient's head and supports the jaw.
PLACEMENT OF FINGERS DURING EXTRACTION
OF MANDIBULAR TEETH
• For the left posterior and anterior teeth, the index
finger of the left hand reflects the cheek and lips as
it is placed in the buccal vestibule.
F i g u r e 5.11: Extraction of teeth from mandibular left
posterior region
• The middle finger reflects the tongue as it is placed
in the lingual vestibule.
• The thumb is placed below the chin so that the jaw
is held between the fingers and the thumb.
• This technique provides less tactile information, but
during extraction of mandibular teeth the need to
support the mandible supersedes the need to support
the alveolar process (Figures 5.12A to C ) . For
mandibular right side, the thumb reflects the tongue,
the index fingers reflects the lip and middle finger
supports lower border of mandible.
• A useful alternative is to place a bite block between
the teeth on the contralateral side. It allows the patient
to provide stabilizing forces to limit the pressure on
the TMJ. However, the surgeon's hand should
continue to provide additional support.
ROLE OF OPPOSITE HAND
The opposite hand plays an active role in the procedure:
1. Reflecting soft tissues to p r o v i d e adequate
visualization of the area of surgery.
2. Protection of other teeth from the forceps.
3. Stabilization of the patient's head during extraction.
4. Most importantly it supports the alveolar process and
provides tactile information to the operator
concerning the expansion of the alveolar process
during luxation.
5. Compress the socket after removal of the tooth.
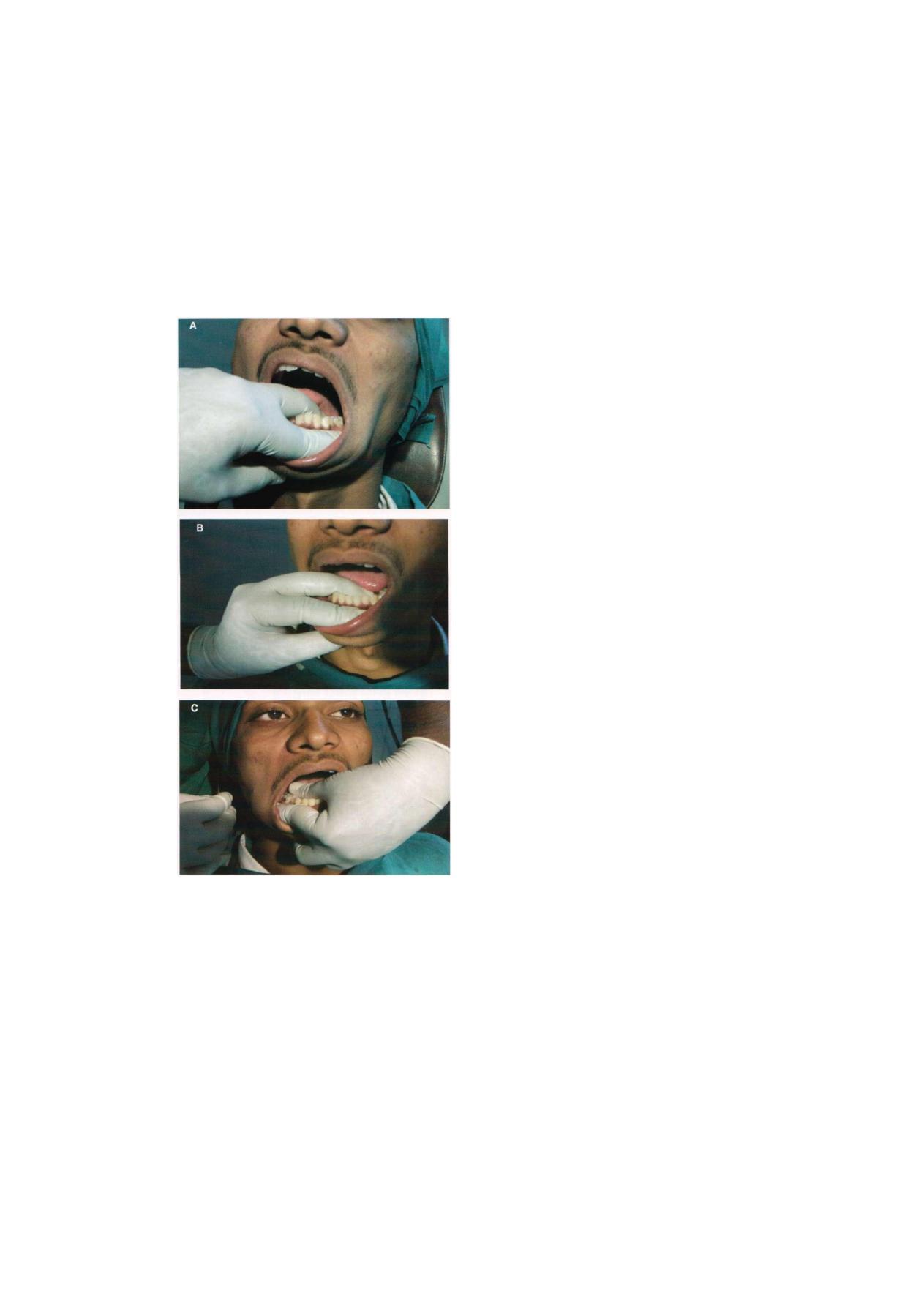
Principles of Exodontia
Figures 5.12A to C: Placement of fingers during extraction
of mandibular teeth. (A) left quadrant, (B) anterior quadrant,
(C) right quadrant
ROLE OF ASSISTANT DURING THE EXTRACTION
PROCEDURE
1. Helps the surgeon to get an unobstructed view and
access to the surgical field.
2. Suction away blood, saliva, irrigating solutions
used.
3. Support the mandible when required.
4. Provide psychologic and emotional support for the
patient.
However, the assistant must not make casual
and offhand comments that may increase patient's
anxiety.
MECHANICAL PRINCIPLES OF ELEVATORS
The removal of teeth from the alveolar process employs
the use of following mechanical principles and simple
machines:
a. Lever
b. Wedge
c. Wheel and axle
LEVER PRINCIPLE
The elevator is a lever of first class. The fulcrum lies
between the effort arm and load arm. The lever principle
has three components fulcrum, power and weight. While
extracting a tooth controlled force is delivered in a
predetermined direction. The power is represented by
handle and the weight is represented by the beaks. Lever
is a mechanism by which modest force is transmitted
at long power arm so that the mechanical advantage
is derived at the short weight arm. This principle is used
when elevators are used for extraction.
WEDGE
It is an established physical principle that a wedge can
be used to split, expand or displace the portion of
substance that receives force. The wedge is a movable
inclined plane which overcomes a large resistance applied
at right angles to the applied effort. The effort is applied
to the base of the plane and the resistance has its effect
on the slant side.
The sharper the angle of the wedge, the less effort
required to make it overcome a given resistance.

Exodontia Practice
• Wedge principle as applicable to extraction with
forceps:
Beaks of extraction forceps are usually narrow at their
tips. They usually broaden as they go superiorly.
The tips of the forceps are forced into the
periodontal ligament space to expand the bone and
force the tooth out of the socket.
• Wedge principle as applicable to the use of elevators:
A small apexo elevator displaces the root toward
the occlusal plane and therefore out of the socket.
WHEEL AND AXLE PRINCIPLE
It is a modified form of lever. The effort is applied to
the circumference of the wheel which turns the axle so
as to raise a weight.
It can be used as a sole work principle in removing
teeth.
It can also be used in conjunction with the wedge
principle and in some cases with the lever principle.
PRINCIPLES OF EXODONTIA
Forcep is the primary instrument used to remove a tooth
from the alveolar process:
1. Expansion of bony socket, i.e. the forcep creates
micro fracture in the alveolar process by the use of
wedge shaped beaks and movement of the tooth itself
with the forceps.
2. Lever principle—this works same as that for elevator.
3. Wedge principle—the tip of the forceps beak is
narrower anteriorly and broadens posteriorly. When
the tip is forced between the mucoperiosteum and
tooth it causes expansion of bony socket so that the
tooth displaced out of socket.
POSTEXTRACTION CARE
• Socket should be debrided only if necessary
• Careful curettage of periapical lesion if it is visible
on a radiograph
• Obvious debris such as tooth fragments, calculus,
amalgam must be gently removed
• Expanded buccolingual plates should be compressed
back to their original configuration.
• Sharp edges of bone to be smoothed with a bone
file.
• To gain control over the hemorrhage, a moistened
gauze to be kept over the socket so that it fits into
the space previously occupied by the crown of the
tooth.
INSTRUCTIONS TO PATIENTS
• Bleeding—The gauze pack to be held firmly between
the jaws for a full half hour to 45 minutes. After the
operation bleeding in the form of oozing may
continue beyond 24 hours in some individuals without
need for alarm. Force full spitting and excessive
physical activity tend to increase bleeding.
• Hygiene—Mouthwash to be avoided for 24 hours
after surgery. Then rinse the mouth with warm saline
and one tea spoon of salt. Do clean the teeth with
your routine tooth brush. Food debris needs to be
cleaned at the site of extraction.
• Swelling—Swelling and discoloration often follow any
procedure in oral cavity. Application of ice cap to
the face briefly and intermittently for first day only.
• Diet—For first 24 hours soft and cold diet is advisable.
Then take diet as near to normal as possible. Chew
on side opposite to that of surgery. Avoid food that
is difficult to masticate.
• Pain—To avoid pain take prescribed medications by
the dentist within 45 minutes of extraction. This will
avoid the medication to take effect before the effect
of anesthesia is worn off.
• To prevent stiffness and to stimulate circulation, jaw
exercises may be done.
• If any reason you are alarmed or unduly concerned
about the condition of your mouth please call your
dentist.

Chapter
Intra-alveolar
Extraction (Simple
Exodontia)

46
Exodontia Practice
Extraction of teeth is the most commonly performed
procedure in the dental office. This chapter aims the basic
steps involved in the extraction of individual teeth.
Dental forceps are used to extract the majority of
erupted teeth. These instruments enable the operator to
grasp the root of the tooth and exert force directly to
the root mass in order to displace it from the surrounding
bone.
Extraction of teeth is a procedure that incorporates
the principles of surgery as well as many principles
from physics and mechanics. When these principles are
applied correctly, a tooth can most likely be removed
intact from the alveolar process without untoward sequel.
This chapter presents the principles and mechanics of
uncomplicated exodontia, i.e. closed method of
extraction. In addition to a discussion of fundamental
underlying principles there also is a detailed description
of techniques for removal of specific tooth with specific
instrument.
It should be always remembered that the removal
of a tooth does not require a larger amount of force
but rather can be accomplished with finesse and control-
led force in such a manner that the tooth is gently lifted
from alveolar process. During preoperative assessment
if we feel that the degree of difficulty is high, a deliberated
surgical approach and not an application of excessive
force should be done. Excessive force may injure local
tissues and destroy surrounding bone and tooth.
PROCEDURE FOR CLOSED EXTRACTION
An erupted tooth can be extracted in one of two major
ways: closed or open. The closed technique is also known
as the simple, or forcep technique. The open technique
is also known as the surgical, or flap, technique. The
closed technique is the most frequently used technique
and is given primary consideration for almost every
extraction. The open technique is used when there is
reason to believe that excessive force is necessary to
remove the tooth or when a substantial amount of the
crown is missing and access to the root of the tooth
is difficult. The correct technique for any situation should
lead to a atraumatic extraction; the wrong technique
may result in an excessively traumatic extraction.
Whatever technique is chosen, the fundamental
requirements for a good extraction remain the same:
1. Adequate access and visualization of the field of
surgery,
2. An unimpeded pathway for the removal of the tooth,
and
3. The use of controlled force to luxate and remove the
tooth.
For the tooth to be removed from the bony socket,
it is necessary to expand the alveolar bony walls to allow
the tooth root an unimpeded pathway, and it is necessary
to tear the periodontal ligament fibers that hold the tooth
in the bony socket. The use of elevators and forceps as
levers and wedges with steadily increasing force can
accomplish these two objectives.
GENERAL STEPS
There are five general steps in the closed-extraction
procedure.
Step 1: Loosening of Soft Tissue
Attachment from the Tooth
The first step in removing a tooth by the closed-ex-
traction technique is to loosen the soft tissue from around
the tooth with a sharp instrument such as the moon's
probe. The purpose of loosening the soft tissue from
the tooth is two-fold. First, it allows surgeons to assure
both themselves and the patient that profound
anesthesia has been achieved. When this step has been
performed, the dentist informs the patient that the
surgery is about to begin and that the first step will be
to push the soft tissue away from the tooth. A small
amount of pressure is felt at this step, but there is no
sensation of sharpness or discomfort. The surgeon then
begins the soft tissue-loosening procedure, gently at first
and then with increasing force (Figure 6.1).
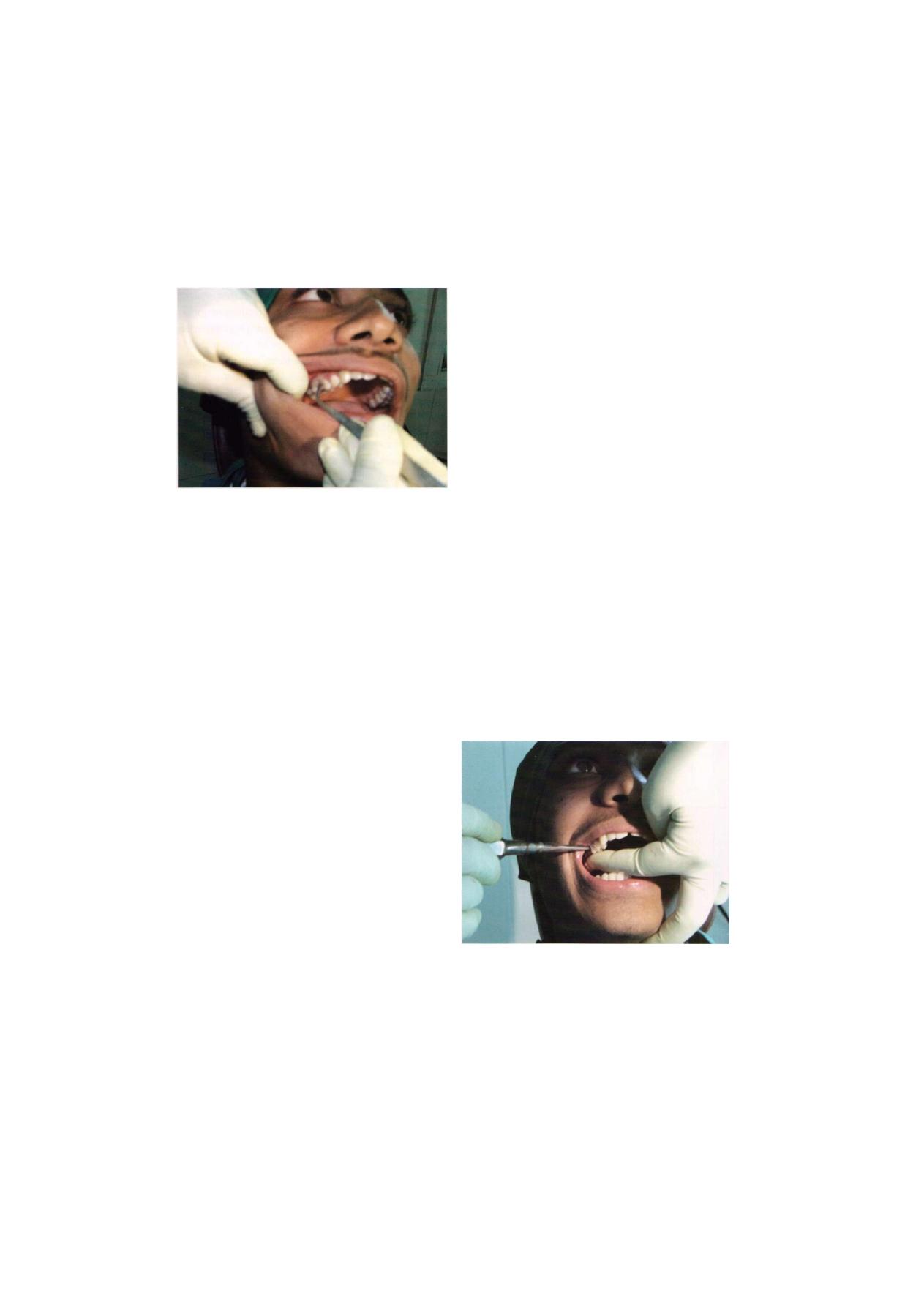
Intra-alveolar Extraction (Simple Exodontia)
47
F i g u r e 6 . 1 : Loosening of the soft tissue attachment from
the tooth
The second reason that the soft tissue is loosened
is to allow the tooth-extraction forcep to be positioned
more apically without interference from or impingement
on the soft tissue of the gingiva. As the soft tissue is
loosened away from the tooth, it is slightly reflected,
which thereby increases the width of the gingival sulcus
and allows easy entrance of the beveled wedge tip of
the forceps beaks.
If a straight elevator is to be used to luxate the tooth,
the moon's probe is also used to reflect the tooth's adja-
cent gingival papilla where the straight elevator will be
inserted, which allows the elevator to be placed directly
onto alveolar bone without crushing or injuring the
gingival papilla
Step 2: Luxation of theTooth with a Dental Elevator
The next step is to begin the luxation of the tooth with
a dental elevator, usually the straight elevator. Expansion
and dilation of the alveolar bone and tearing of the
periodontal ligament require that the tooth be luxated
in several different ways. The straight elevator is inserted
perpendicular to the tooth into the interdental space after
reflection of the interdental papilla. The elevator is then
turned in such a way that the inferior portion of the blade
rests on the alveolar bone and the superior or occlusal
portion of blade is turned toward the tooth being
extracted. Strong, slow, forceful turning of the handle
moves the tooth in a posterior direction, which results
in some expansion of the alveolar bone and tearing of
the periodontal ligament. If the tooth is intact and in
contact with stable teeth anterior and posterior to it, the
amount of movement achieved with the straight elevator
will be minimal. The usefulness of this step is greater
if there is no tooth posterior to the tooth being extracted
or if it is broken down to an extent that the crowns do
not inhibit movement of the tooth (Figure 6.2).
In certain situations the elevator can be turned in the
opposite direction, and more vertical displacement of
the tooth will be achieved, which can possibly result in
complete removal of the tooth.
Luxation of teeth with a straight elevator should be
performed with caution. Excessive forces can damage
and even displace the teeth adjacent to those being
extracted. It must be kept in mind that this is only the
initial step and that the forceps are the major instrument
for tooth luxation in most situations.
Step 3: Adaptation of the Forceps to the Tooth
After placing the left hand in position and thus obtaining
a clear view of the tooth to be extracted, the forceps
blade are applied to the buccal and lingual surface of
the roots of the tooth.
F i g u r e 6.2: Application of dental elevator

48
Exodontia Practice
The goals of forcep use are two-fold
1. Expansion of bony socket by use of the wedge shaped
beaks of the forceps and the movement of the tooth
itself with forceps.
2. Removal of the tooth from the socket.
C e r t a i n r u l e s m u s t b e o b s e r v e d i n the
application of forceps to the tooth.
• The correct forcep must be selected.
• Don't grasp the forcep near the beaks, instead hold
them so that the ends of the handles are almost
covered by the palm of the hands.
• The long axis of the forceps's beaks must be parallel
to the long axis of the tooth (Figure 6.3).
• Forcep beaks must be placed on sound root structure
and not on the enamel of the crown (Figure 6.4).
• The root structure must be grasped firmly so that when
pressure is applied the beaks do not move on the
cementum, otherwise breakage may occur (Figure
6.3)
Figure 6.3: Correct method of application of forcep to the tooth
• Make certain that beaks of the forceps will not impinge
on adjacent teeth during the application of force.
• Beaks should not touch the crown when the roots
are gripped (Figure 6.3).
• The root or root mass of the tooth is always gripped
with the forceps (Figure 6.3).
It is a good practice to apply the forceps blade to
the less accessible side to the tooth first under direct vision
and then apply the other blade. If either the buccal or
lingual surface of the tooth is destroyed by cervical caries,
the appropriate blade should be applied to the carious
side first, and the first movements made towards the
carious side. This will allow the forceps blade to grip
the sound tooth structure and reduce the risk of fracture
of tooth (Figure 6.4).
F i g u r e 6.4: Application of forcep to the tooth
(B—Buccal, L—Lingual)
The proper forceps are then chosen for the tooth to
be extracted. The beaks of the forceps should be shaped
to adapt anatomically to the tooth apical to the cervical
line—that is, to the root surface. The forceps are then
seated onto the tooth so that the tips of the forceps beaks
grasp the root underneath the loosened soft tissue. The
lingual beak is usually seated first and then the buccal
beak. Care must be taken to confirm that the tips of the
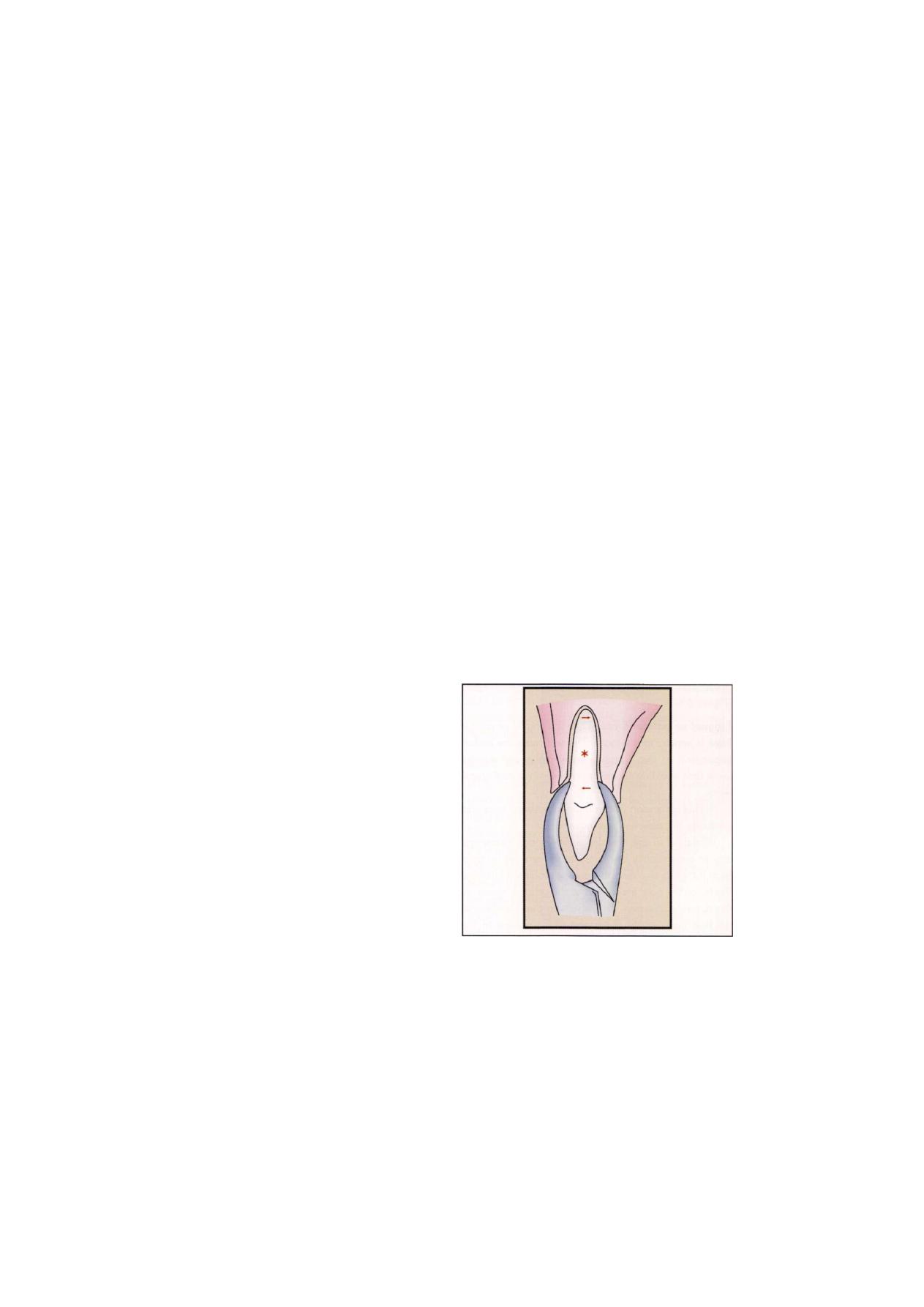
Intra-alveolar Extraction (Simple Exodontia)
49
forceps beaks are beneath the soft tissue and not en-
gaging the adjacent tooth. Once the forceps have been
positioned on the tooth, the surgeon grasps the handles
of the forceps at the ends to maximize mechanical advan-
tage and controlled force is applied.
If the tooth is malposed in such a fashion that the
usual forceps cannot grasp the tooth without injury to
adjacent teeth, another forceps should be employed. The
maxillary root forceps can often be useful for crowded
lower anterior teeth.
The beaks of the forceps must be held parallel to the
long axis of the tooth, because the forces generated by
the application of pressure to the forceps handle must
be delivered along the long axis of the tooth for maximal
effectiveness in dilating and expanding the alveolar
bone. If the beaks are not parallel to the long axis of
the tooth, there is increased likelihood of fracturing the
tooth root (Figure 6.3).
The forceps are then forced apically as far as possible
to grasp the root of the tooth as apically as possible.
This accomplishes two things. First, the beaks of the
forceps act as wedges to dilate the crestal bone on the
buccal and lingual aspects. Second, by forcing the beaks
apically the center of rotation (or fulcrum) of the forces
applied to the tooth is displaced toward the apex of the
tooth, which results in greater effectiveness of bone
expansion and less likelihood of fracturing the apical end
of the tooth.
At this point the surgeon's hand should be grasping
the forceps firmly with the wrist locked and the arm held
against the body; the surgeon should be prepared to
apply force with the shoulder and upper arm without
any wrist pressure. He or she should be standing straight
with the feet comfortably apart.
Step
4:
Application of Forces to the Tooth with the
Forceps
Once the forcep is properly applied to the tooth certain
forces are used to deliver tooth from its socket. They
are apical force, labial or buccal force, lingual or palatal
force, rotational force, and fractional force.
Apical force: As already explained beaks act as a
wedges between the alveolar socket and tooth surface.
Very little movement of the tooth in the apical direction
takes place. Instead this movement expands the bony
socket and helps in securing a firm grip over a larger
area of the tooth. Teeth with single conical roots
may jump out of the socket during this phase like an
orange seed jumping off the two fingers when pressure
is applied.
A second major accomplishment of apical pressure
with the extraction forceps is that the fulcrum, the center
of the tooth's rotation is placed more apically. Since the
tooth is moving in response to the force placed on it
by the forceps, the forcep becomes the instrument of
expansion. If the fulcrum is high, there is a large amount
of force on apical region of tooth, which increases
the chance of root fracture. If the beaks of the forcep
are forced a bit into the periodontal ligament space,
the center of rotation is moved apically, which results
in greater movement of forces at the crest of the
ridge and less force moving the apex of the tooth. This
process decreases the chance of apical root fracture
(Figure 6.5).
Figure 6.5: Apical force decrease the chance of apical
root fracture
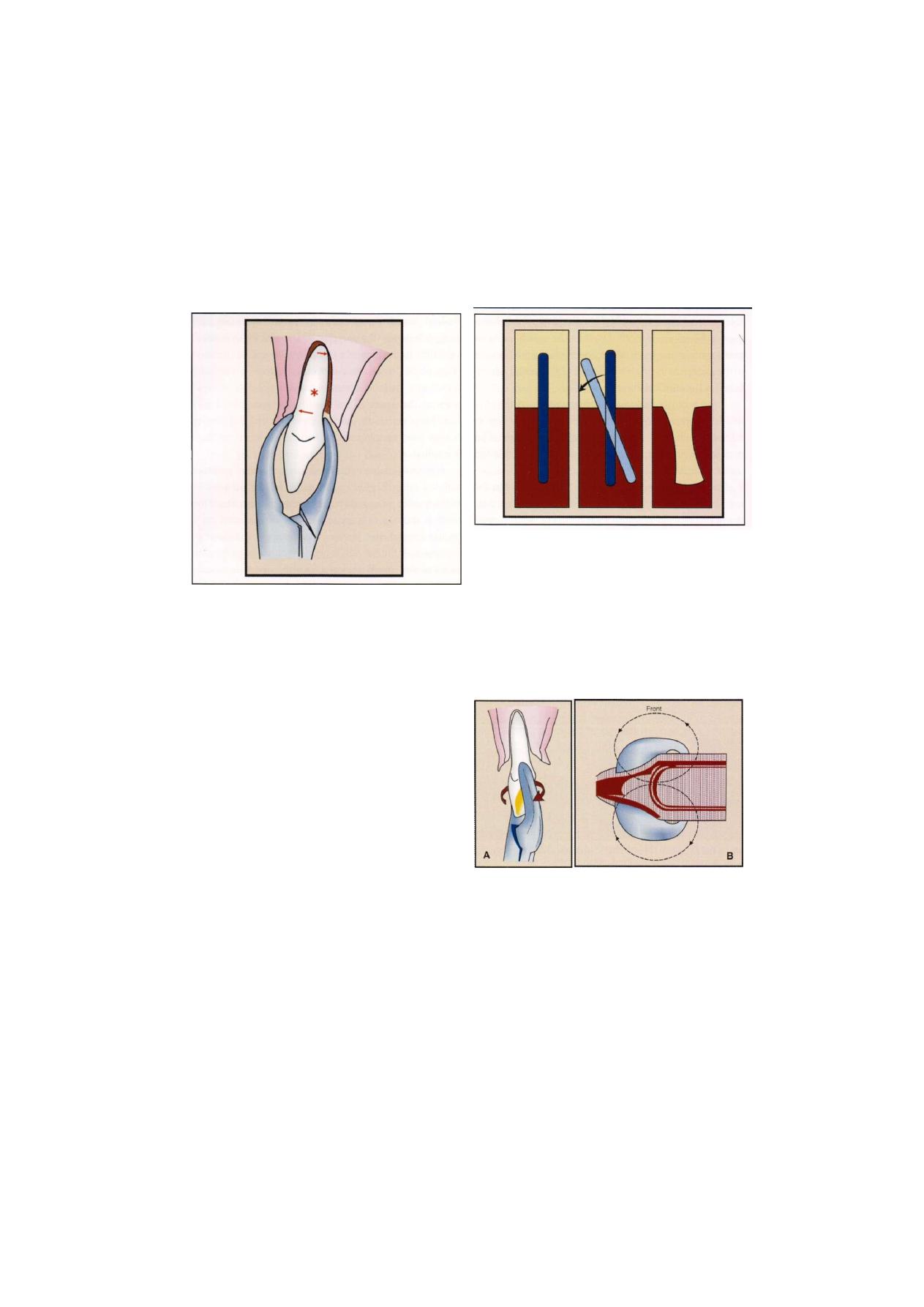
Exodontia Practice
F i g u r e 6.6: Buccal force application
Labial or buccal force: By keeping a continuous apical
pressure buccal force is added which expands the bony
socket still further. During this movement the forcep
takes fulcrum from the crest of the alveolus. When buccal
force is applied the expansion of buccal cortical plate
occurs at crest and lingual cortical plate at apical region
(Figure 6.6).
Lingual or palatal force: Then the lingual or palatal
force is applied to the tooth. This will cause the socket
expansion at the lingual crestal bone and at the
same time avoiding excessive pressure on buccal apical
bone.
Socket expansion is maximum in younger jaws and
gradually decreases as age advances.
Dilatation of the alveolar socket during extraction
can be conveniently compared to the removal of pole
from the ground. When the pole is mobilized laterally,
the tip of the pole embedded in the ground moves in
the opposite direction. This results in the dilatation of
the hole near the tip of the embedded portion of the
pole. If the pole is moved in the opposite direction there
will be dilatation in the opposite side (Figure 6.7).
F i g u r e 6.7: Principle of pole dilatation
Rotational forces: This is applied by using wheel and
axle principle in the form of an arc with fulcrum of the
lever principle on the crest to the buccal alveolus. This
is the most important phase in the tooth extraction
technique. Upper central incisor and lower second
premolars can be removed by applying rotational forces
along the long axis of root. Teeth that have multiple roots
are more likely to fracture (Figure 6.8).
F i g u r e s 6.8A a n d B: (A) Application of rotational force.
(B) Figure of eight force
Tractional forces: This type of force is useful in the
terminal phase of the tooth delivery out of the bony socket.
Hence, this should be as gentle as possible (Figure 6.9).
The surgeon begins to luxate the tooth by using the
motions discussed earlier. The major portion of the force
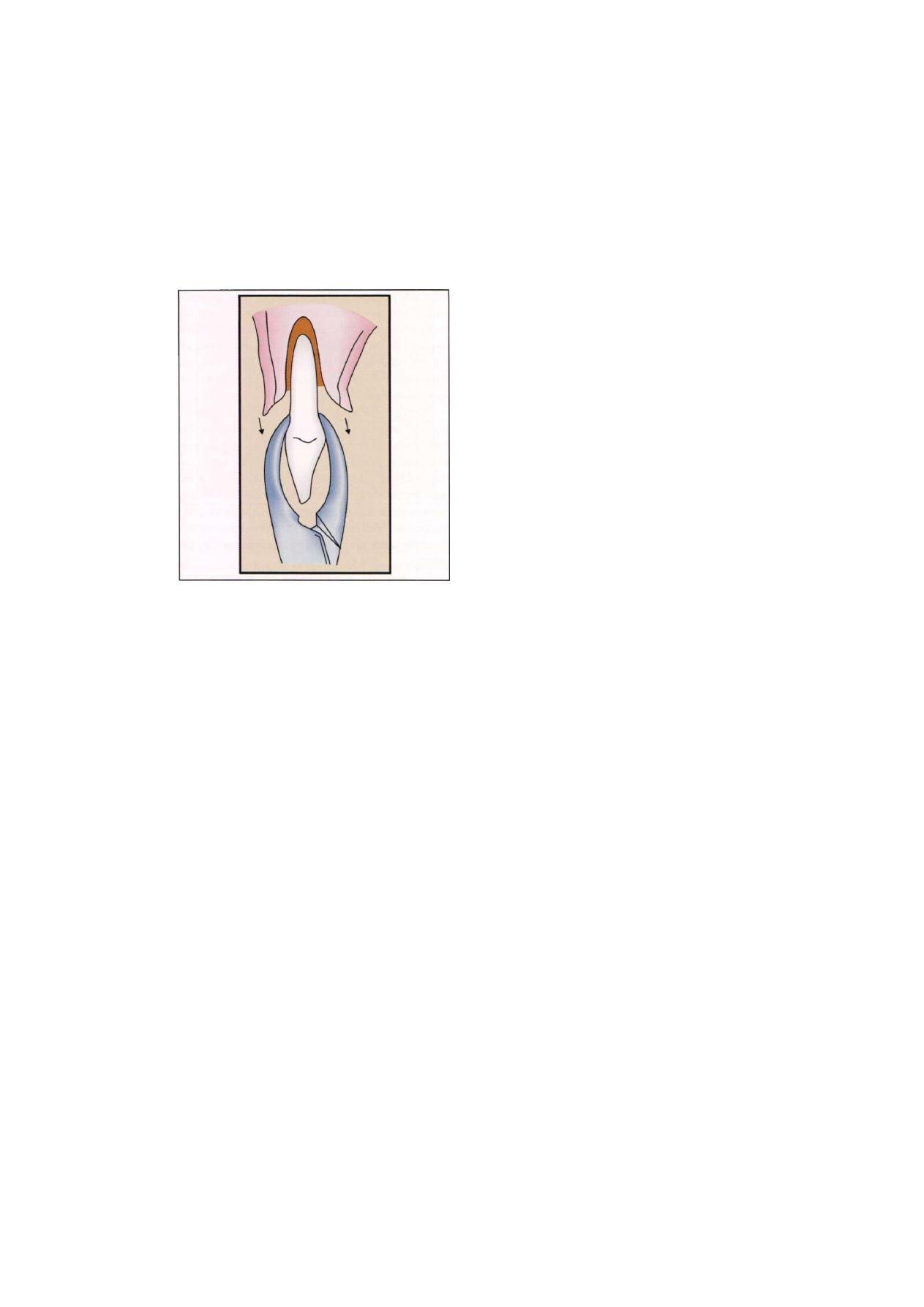
Intra-alveolar Extraction (Simple Exodontia)
51
F i g u r e 6.9: Tractional force
is directed toward the thinnest and therefore weakest
bone. The surgeon uses slow, steady force to displace
the tooth bucally. The motion is deliberate and slow and
gradually increases in force. The tooth is moved again
toward the opposite direction with slow, deliberate, strong
pressure. As the alveolar bone begins to expand, the
forceps are reseated apically with a strong deliberate
motion, which causes additional expansion of the
alveolar bone and further displaces the center of the rota-
tion apically. Buccal and lingual pressures continue to
expand the alveolar socket. For some teeth rotational
motions are then used to help expand the tooth socket
and the periodontal ligament attachment.
Beginning surgeons have a tendency to apply
inadequate pressure for insufficient amounts of time.
Three factors must be reemphasized: first, the forceps
need to be seated apically as far as possible and reseated
periodically during the extraction; second, the forces
applied in the buccal and lingual directions should be
slow, deliberate pressures and not jerky wiggles; and third,
the force should be held for several seconds to allow
the bone to expand. It must be remembered that teeth
are not pulled but rather gently lifted from the socket
once the alveolar process has been sufficiently expanded.
Step
5:
Removal of the Tooth from the Socket
Once the alveolar bone has expanded sufficiently and
the tooth has been luxated, a slight tractional force,
usually directed buccally, can be used. Tractional forces
should be minimized, since this is the last motion that
is used once the alveolar process is sufficiently expanded
and the periodontal ligament completely severed.
It is useful to remember that luxation of the tooth
with the forceps and removal of the tooth from the bone
are separate steps in the extraction. Luxation is directed
toward expansion of the bone and disruption of the
periodontal ligament. The tooth is not removed from
the bone until these two goals are accomplished. The
surgeon should realize that the major role of the forceps
is not to remove the tooth but rather to expand the bone
so that the tooth can be removed.
For teeth that are malopposed or have unusual
positions in the alveolar process, the luxation with the
forceps and removal from the alveolar process will be
in unusual directions. The surgeon must develop a sense
for the direction the tooth wants to move and then be
able to move it in that direction. Careful preoperative
assessment and planning help to make this determination
during the extraction.
ROLE OF THE OPPOSITE HAND
When using the forceps and elevators to luxate and
remove teeth, it is important that the surgeons opposite
hand play an active role in the procedure. For the right-
handed operator, the left hand has a variety of functions.
It is responsible for reflecting the soft tissues of the cheeks,
lips, and tongue to provide adequate visualization of the
area of surgery. It helps to protect other teeth from the
forceps, should they release suddenly from the tooth
socket. It helps to stabilize the patient's head during the
extraction process. In some situations large amounts of
force are required to expand heavy alveolar bone, and
therefore the patient's head requires active assistance in
52
Exodontia Practice
being held steady. The opposite hand plays an important
role in supporting and stabilizing the lower jaw when
mandibular teeth are being extracted. It is often necessary
to apply significant pressure to expand heavy mandibular
bone, and such forces can cause discomfort and even
injury to the temporomandibular joint unless they are
counteracted by a steady hand. Finally, the opposite hand
supports the alveolar process and provides tactile
information to the operator concerning the expansion
of the alveolar process during the luxation period. In
some situations it is impossible for the opposite hand
to perform all of these functions at the same time, so
the surgeon requires an assistant to help with some of
them.
ROLE OF ASSISTANT DURING EXTRACTION
For a successful outcome in any surgical procedure, it
is essential to have a competent assistant. During the
extraction the assistant plays a variety of important roles
that contribute to making the surgical experience
atraumatic to the patient.
The assistant helps the surgeon to visualize and gain
access to the operative area. The assistant reflects the
soft tissue of the cheeks and tongue so that the surgeon
can have an unobstructed view of the surgical field. Even
during a closed extraction the assistant can reflect the
soft tissue so that the surgeon can apply the instruments
to loosen the soft tissue attachment as well as adapt the
forceps to the tooth and tooth root in the most effective
manner.
Another major activity of the assistant is to suction
away blood, saliva, and the irrigating solutions used dur-
ing the surgical procedure. This prevents fluids from accu-
mulating and makes proper visualization of the surgical
field possible. Suctioning is also important for patient
comfort, since most patients are unable to tolerate an
accumulation of blood or other fluids in their mouths.
During a surgical procedure it is almost impossible for
the assistant to suction too much.
During the extraction the assistant should also help
to protect the teeth of the opposite arch, which is
especially important when removing lower posterior
teeth. If traction forces are necessary to remove a lower
tooth, occasionally the-footh releases suddenly and the
forceps strike the maxillary teeth and sometimes fracture
a tooth cusp. The assistant should hold either a suction
tip or a finger against the maxillary teeth to protect them
from an unexpected blow.
During the extraction of mandibular teeth the assistant
may play an important role by supporting the mandible
during the application of the extraction forces. A surgeon
who uses his or her own hand to reflect the soft tissue
may not be able to support the mandible. If this is the
case, the assistant plays an important role in stabilizing
the mandible to prevent temporomandibular joint
discomfort. Most often the surgeon stabilizes the
mandible which makes this role less important for the
assistant.
The assistant also provides psychological and
emotional support for the patient by helping to alleviate
patient anxiety.
DIRECTIONS TO MOVE TEETH FOR
EXTRACTION
Exodontia is an art that must be learned and the operator
gaining experience will begin to appreciate the feel of
each tooth as it moves and so exploit the line of least
resistance. There are however, several rules for each tooth
based on the root form and the local bony anatomy of
the alveolus.
MAXILLARY TEETH
Bone in the maxilla has a higher proportion of cancellous
to cortical structure than the mandible and as a result
is generally less dense than mandibular bone. The
alveolar bone is thinner on its buccal or labial surface
by comparison with the thicker palatal side. Therefore,
the normal direction of tooth displacement is bucally.
However, the buccal plate is buttressed in the first moral
region by the zygomatic process of maxilla. The number
and shape of roots affects the way in which a root is
removed (Figure 6.10).
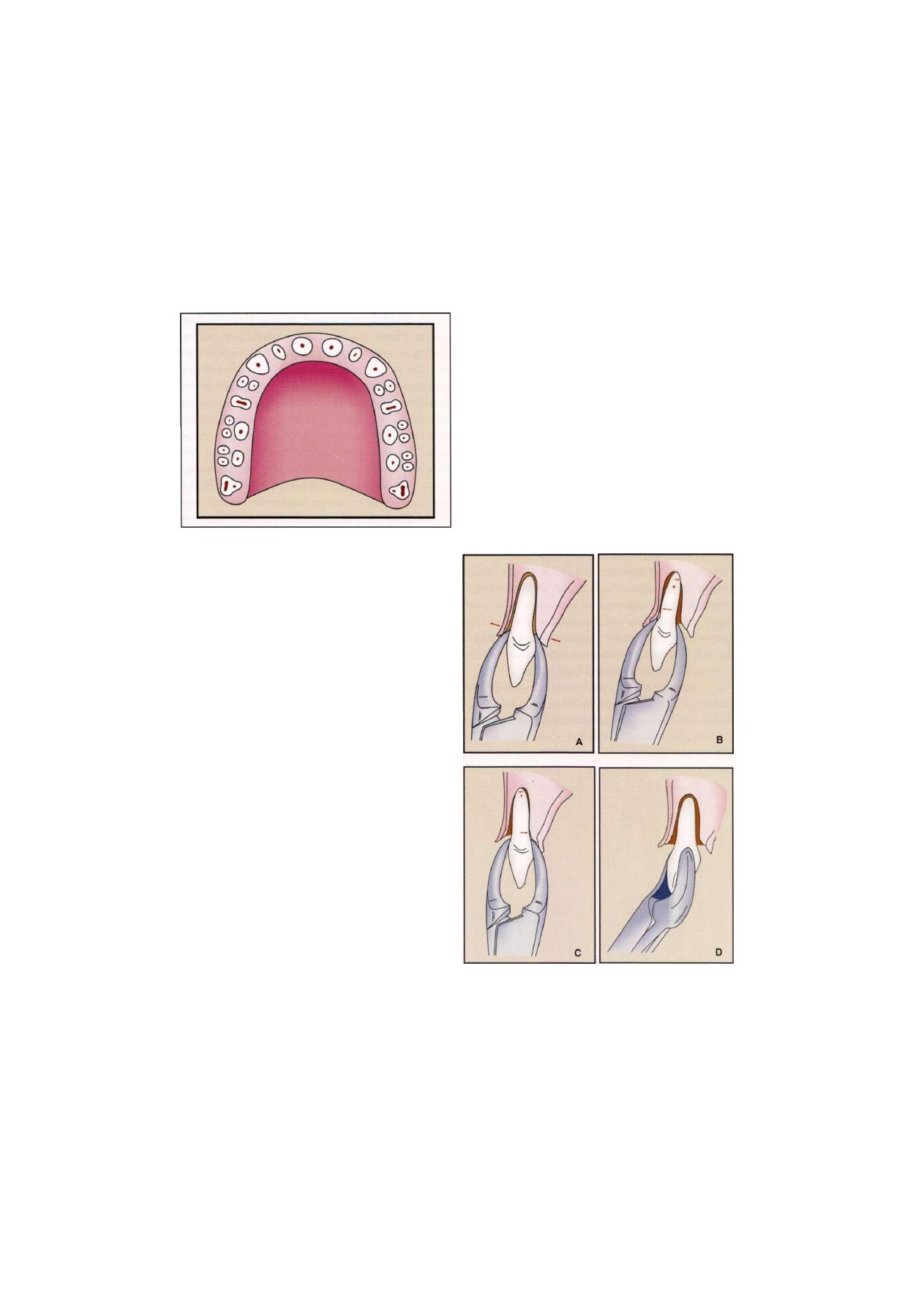
Intra-alveolar Extraction (Simple Exodontia)
53
F i g u r e 6.10: Diagrammatic representation of maxillary
alveolus with number of roots
This section describes specific techniques for the
removal of each tooth in the mouth. In some situations
several teeth are grouped together—for example, the
maxillary anterior teeth—since the technique for their
removal is essentially the same.
MAXILLARY TEETH
In the correct position for extraction of maxillary left
or anterior teeth, the left index finger of the surgeon
should reflect the lip and cheek tissue, and the thumb
should rest on the palatal alveolar process. In this
way the left hand is able to reflect the soft tissue of
the cheek, stabilize the patient's head, support the
alveolar process, and provide tactile information to
the surgeon regarding the progress of the extraction.
When such a position is used during the extraction of
a maxillary molar, the surgeon can frequently feel with
the left hand, the palatal root of the molar becoming
free in the alveolar process before realizing it with the
forceps or extracting hand. For the right side, the index
finger is positioned on the palate and the thumb on
the buccal aspect.
Maxillary incisor teeth: The maxillary incisor teeth
are extracted with the upper incisor forcep.The maxillary
incisors generally have conical roots with the lateral ones
being slightly longer and more slender. The lateral incisor
is more likely also to have a distal curvature on the apical
one-third of the root, so this must be checked radio-
graphically before extraction. The alveolar bone is thin
on the labial side and heavier on the palatal side, which
indicates that the major expansion of the alveolar process
will be in the buccal direction. The initial movement is
slow, steady, and firm in the labial direction, which
expands the crestal buccal bone. A less vigorous palatal
force is then used, followed by a slow, firm, rotational
force. Rotational movement should be minimized for the
lateral incisor especially if a curvature exists on the tooth.
The tooth is delivered in the labial-incisal direction with
a small amount of tractional force (Figure 6.11).
F i g u r e 6 . 1 1 : Extraction of maxillary central incisor
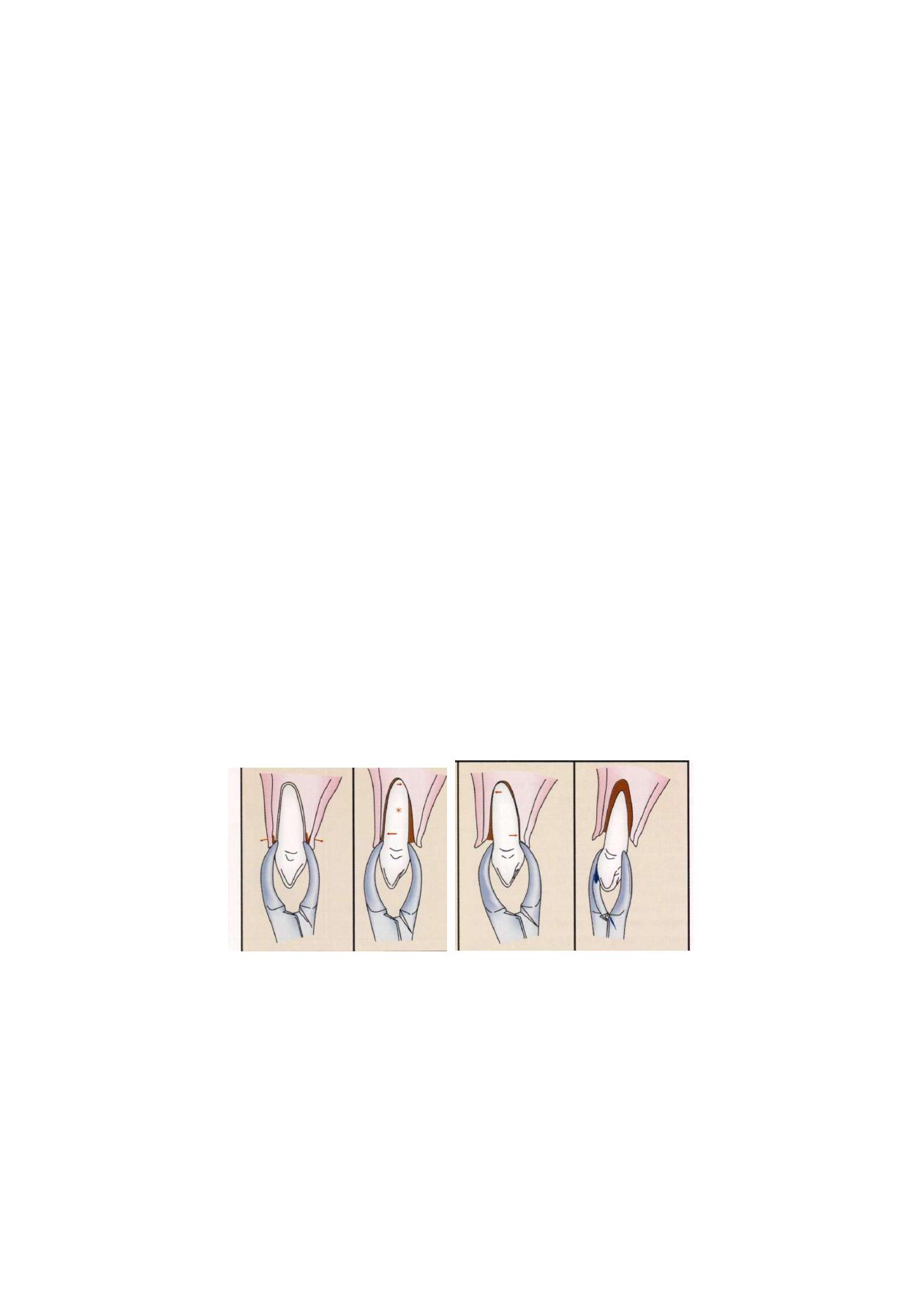
54
Exodontia Practice
Maxillary Canine
The maxillary canine is usually the longest tooth in the
mouth. The root is oblong in cross-section and usually
produces a bulge on the anterior surface of the maxilla
called the canine eminence. The result is that the bone
over the labial aspect of the maxillary canine is usually
quite thin. In spite of the thin labial bone, this tooth can
be difficult to extract simply because of its long root.
Additionally, it is not uncommon for a segment of labial
alveolar bone to fracture from the labial plate and be
removed with the tooth.
As with all extractions, the initial placement of the
beaks of the forceps on the canine tooth should be as
far apically as possible. The initial movement is to the
buccal aspect with return pressure to the palatal. As the
bone is expanded and the tooth mobilized, the forceps
should be repositioned apically. A small amount of
rotational force may be useful in expanding the tooth
socket especially if the adjacent teeth are missing or have
just been extracted. After the tooth has been well luxated,
it is delivered from the socket in a labial-incisal direction
with labial tractional forces (Figure 6.12).
If during the luxation process with the forceps, the
surgeon feels a portion of the labial bone fracture, a
decision must be made concerning the next step. If the
palpating finger indicates that a relatively small amount
of bone has fractured and is attached to the canine tooth,
the extraction should continue in the usual manner with
caution-taken not to tear the soft tissue. However, if the
palpating finger indicates that a relatively large portion
of labial alveolar plate has fractured, the surgeon should
stop the surgical procedure at this point. Usually the
fractured portion of bone is attached to periosteum and
therefore is viable. The surgeon should use a thin
periosteal elevator to raise a small amount of mucosa
from around the tooth down to the level of the fractured
bone. The canine tooth should then be stabilized with
the extraction forceps, and the surgeon should attempt
to free the fractured bone from the tooth with the
periosteal elevator as a lever to separate the bone from
the tooth root. If this can be accomplished, the tooth
can be removed and the bone left in place attached to
the periosteum. Normal healing should occur. If the bone
becomes detached from the periosteum during these
attempts, it should be removed, because it is most likely
non-vital and may actually prolong wound healing. This
procedure can be used whenever alveolar bone is
fractured during extraction.
Maxillary First Premolar
The maxillary first premolar is a single-rooted tooth in
its first two thirds with a bifurcation into a buccal and
lingual root usually occurring in the apical one-third to
one half. These roots may be extremely thin and are
subject to fracture especially in older patients in whom
bone density is great and bone elasticity is small. Perhaps
F i g u r e 6.12: Extraction of maxillary canine
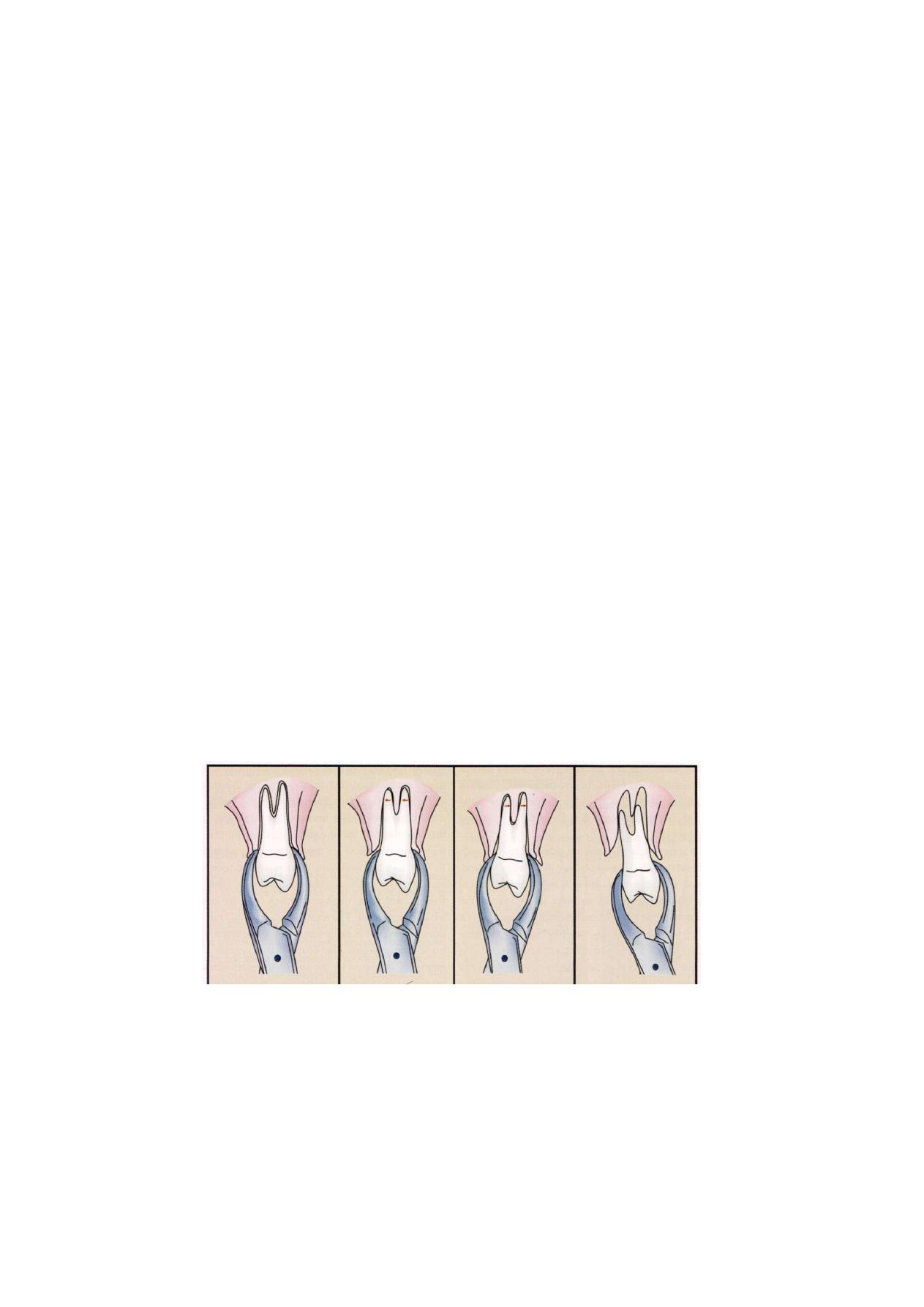
Intra-alveolar Extraction (Simple Exodontia)
55
the most common root fracture when extracting teeth
in adults occurs with this tooth. As with other maxillary
teeth, the buccal bone is relatively thin when compared
with the palatal bone.
The forceps of choice once again is the upper
premolar forceps. Because of the bifurcation of the tooth
into two relatively thin root tips, extraction forces should
be carefully controlled during removal of the maxillary
first premolar. Initial movements should be buccal. Palatal
movements are made with relatively small amounts of
force to prevent fracture of the palatal root tip, which
is harder to retrieve. When the tooth is luxated buccally,
the most likely tooth root to break is the labial. When
the tooth is luxated in the palatal direction, the most
likely root to break is the palatal root. Of the two root
tips, the labial is easier to retrieve because of the thin,
overlying bone. Therefore, buccal pressures should be
greater than palatal pressures. Any rotational force should
be avoided. Final delivery of the tooth from the tooth
socket is with tractional force in the occlusal direction
and slightly buccal (Figure 6.13).
Maxillary Second Premolar
The maxillary second premolar is a single-rooted tooth
for the root's entire length. The root is thick and has
a blunt end. Consequently, the root of the second
premolar fractures rarely. The overlying alveolar bone
is similar to that of other maxillary teeth in that it is
relatively thin toward the buccal with a heavy palatal
alveolar palate.
The forceps are forced as far apically as possible so
as to gain maximal mechanical advantage in removing
this tooth. Since the tooth root is relatively strong and
blunt, the extraction requires relatively strong movements
to the buccal, back to the palate, and then in the buccal-
occlusal direction with a rotational, tractional force
(Figure 6.14).
Maxillary Molar
The maxillary first molar has three large and relatively
strong roots. The buccal roots are usually relatively close
together, and the palatal root diverges widely toward
the palate. If the two buccal roots are also widely
divergent, it becomes difficult to remove this tooth by
closed, or forceps, extraction. Once again the overlying
alveolar bone is similar to that of other teeth in the
maxilla; the buccal plate is thin and the palatal cortical
plate is thick and heavy. When evaluating this tooth
radiographically, one should note the size, curvature,
and apparent divergence of the three roots. Additionally,
F i g u r e 6.13: Extraction of maxillary first premolar
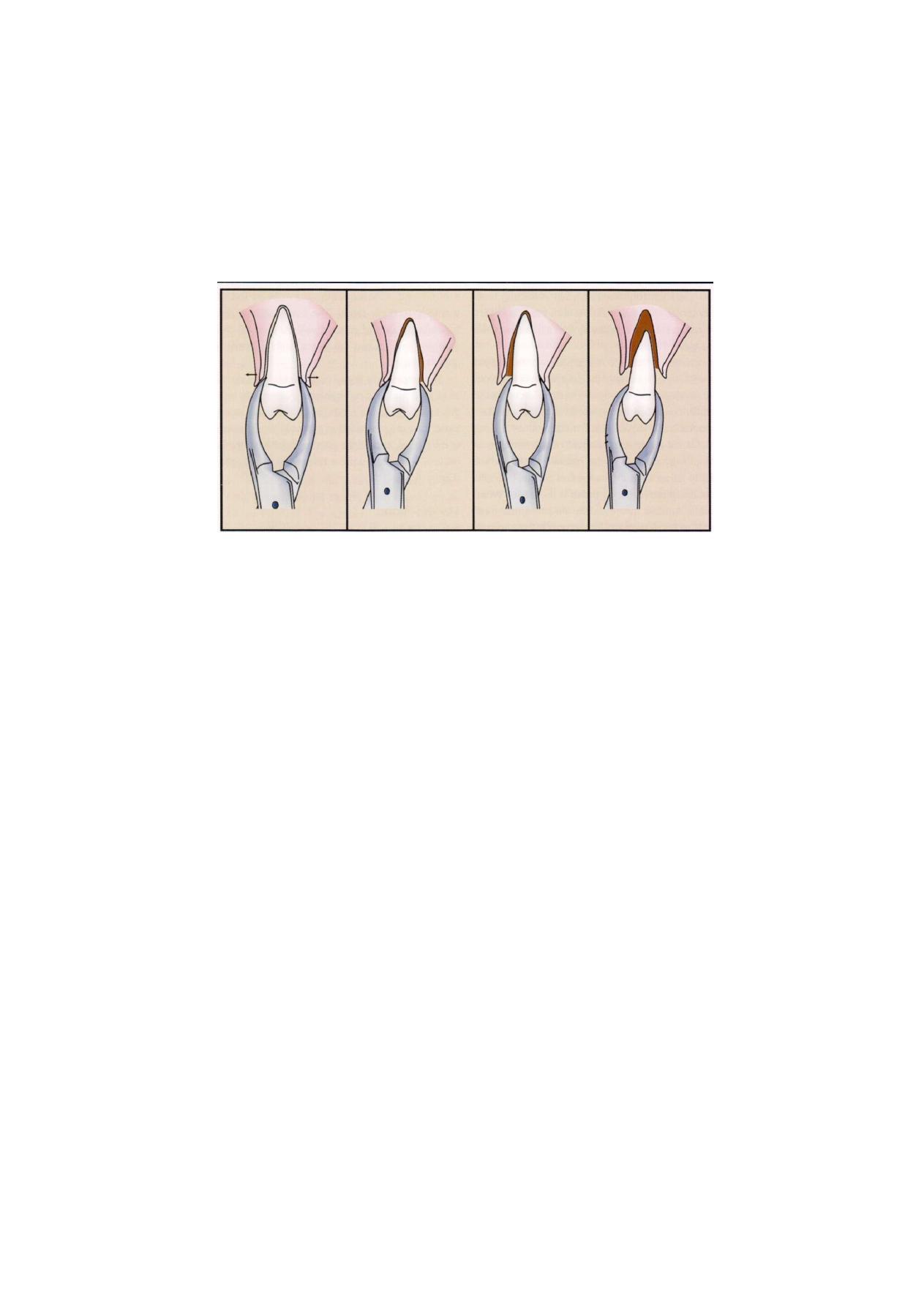
56
Exodontia Practice
Figure 6.14: Extraction of maxillary second premolar
the dentist should look carefully at the relationship of
the tooth roots to the maxillary sinus. If the sinus is in
close proximity to the roots and the roots are widely
divergent, there is increased likelihood of sinus
perforation caused by removal of a portion of the sinus
floor during tooth removal. If this appears to be likely
after preoperative evaluation, the surgeon should
strongly consider a surgical extraction.
The forceps usually used for extraction of the
maxillary molars are the paired forceps. These forceps
have tip projections on the buccal beaks to fit into the
buccal bifurcation. Cow horn forceps are useful if the
crown of the molar tooth has large caries or large
restorations.
The upper molar forceps are adapted to the tooth
and seated apically as far as possible in the usual fashion.
The basic extraction movement is to use strong buccal
and palatal pressures with stronger forces toward the
buccal than toward the palate. Rotational forces are not
useful for extraction of this tooth because of its three
roots. As was mentioned in the discussion of the
extraction of the maxillary first premolar, it is preferable
to fracture a buccal root than a palatal root, because
it is easier to retrieve the buccal roots. Therefore, if the
tooth has widely divergent roots and the dentist suspects
that one root may be fractured, the tooth should be
luxated in such a way as to prevent fracturing the palatal
root. One must minimize palatal force, since this is the
force that fractures the palatal root. Strong, slow, steady,
buccal pressure expands the buccal cortical plate and
tears the periodontal ligament fibers that hold the palatal
root in its position. Palatal forces should be used but
kept to a minimum (Figure 6.15).
The maxillary second molar's anatomy is similar to
that of the maxillary first molar except that the roots tend
to be shorter and less divergent with the buccal roots
more commonly fused into a single root. This means
that the tooth is more easily extracted by the same
technique described for the first molar.
The erupted maxillary third molar frequently has
conical roots and is usually extracted with third molar
forceps, which are universal forceps used for both the
left and right sides. The tooth is usually easily removed,
since the buccal bone is thin and the roots are usually
fused and conical. The erupted third molar is also
frequently extracted by the use of elevators alone. It is
important to visualize the maxillary third molar clearly
on the preoperative radiograph, because the root
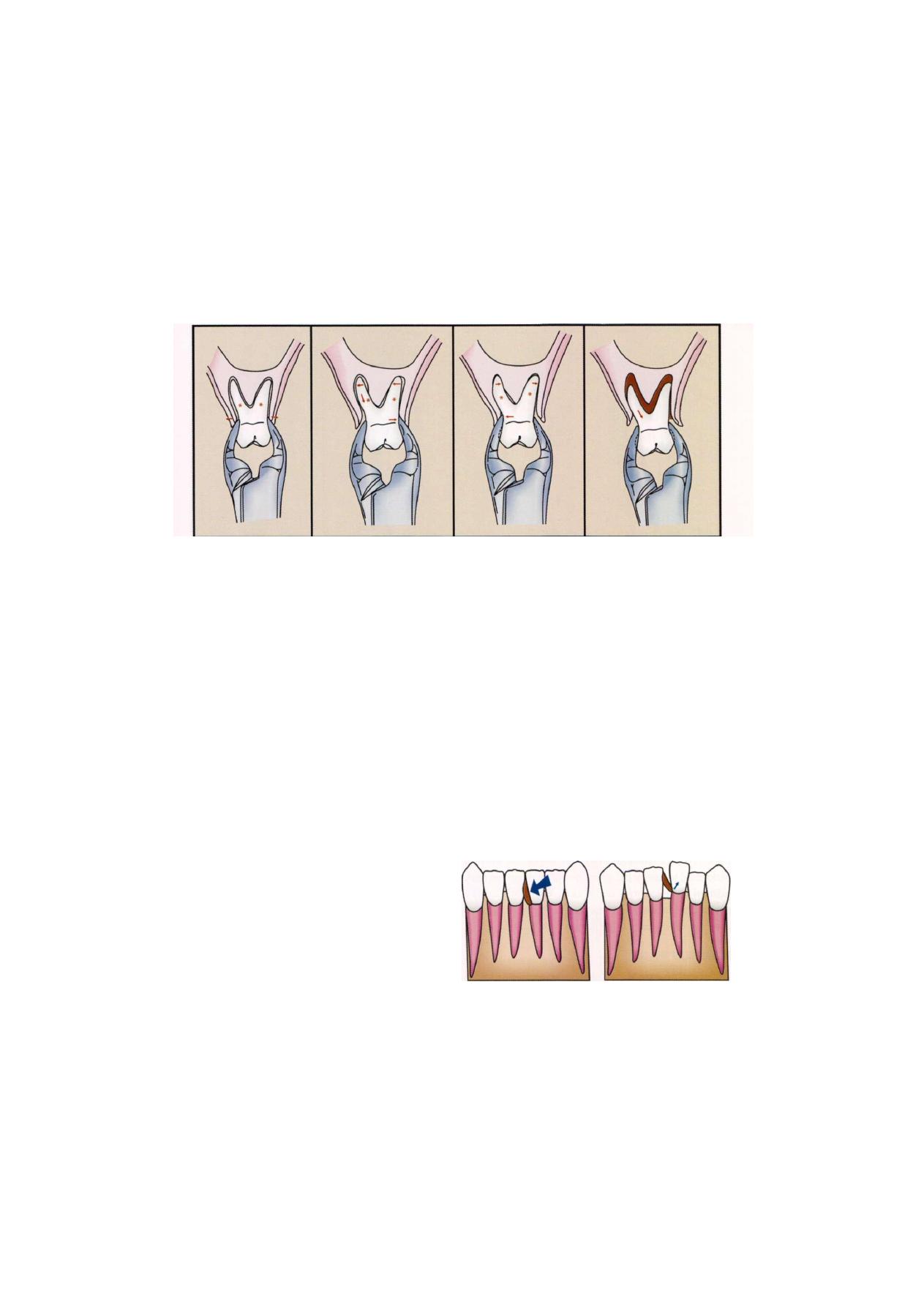
Intra-alveolar Extraction (Simple Exodontia)
57
F i g u r e 6.15: Extraction of maxillary molar
anatomy of this tooth is quite variable and often small,
dilacerated, hooked roots exist in this area. Retrival
of fractured roots in this area can be very difficult.
MANDIBULAR TEETH
The mandible has a more ratio of cortical to cancellous
bone than maxilla. Consequently the alveolar bone
supporting lower teeth is more dense and less readily
deformed. Making the displacement of mandibular teeth
more difficult. Buccal and lingual cortices tend to be of
similar thickness in the anterior mandible. Distally in
molar region buccal cortical plate is thickened by external
oblique ridge. Therefore, incisors canine and premolars
requires strong buccal force and molars require strong
lingual pressure.
MANDIDULAR ANTERIOR TEETH
The mandibular incisors and canines are similar in shape
with the incisors being shorter and slightly thinner and
the canine roots being longer and somewhat heavier.
The incisor roots are more likely to be fractured, since
they are somewhat thin and therefore should be removed
only after adequate pre-extraction luxation. The alveolar
bone that overlies the incisors and canines is quite thin
on the labial as well as the lingual sides. The bone over
the canine may be somewhat thicker especially on the
lingual side.
The usual forceps employed to remove these teeth
is the lower anterior forceps. The forceps beaks are
positioned onto the teeth and seated apically with strong
force. The extraction movements are generally in the
labial and lingual directions with equal pressures both
ways. Once the tooth has become luxated and mobile,
rotational movement may be used to expand the alveolar
bone further. The tooth is removed from the socket with
fractional forces in a labial-incisal direction (Figure 6.17).
STORIES TECHNIQUE
If the extraction of multiple anterior teeth is indicated,
straight elevator is inserted both the lower incisors and
rotated. This will loosen both the adjacent teeth and
facilitate the extraction (Figure 6.16).
Figure 6.16: Stobie's technique for extraction of adjacent teeth
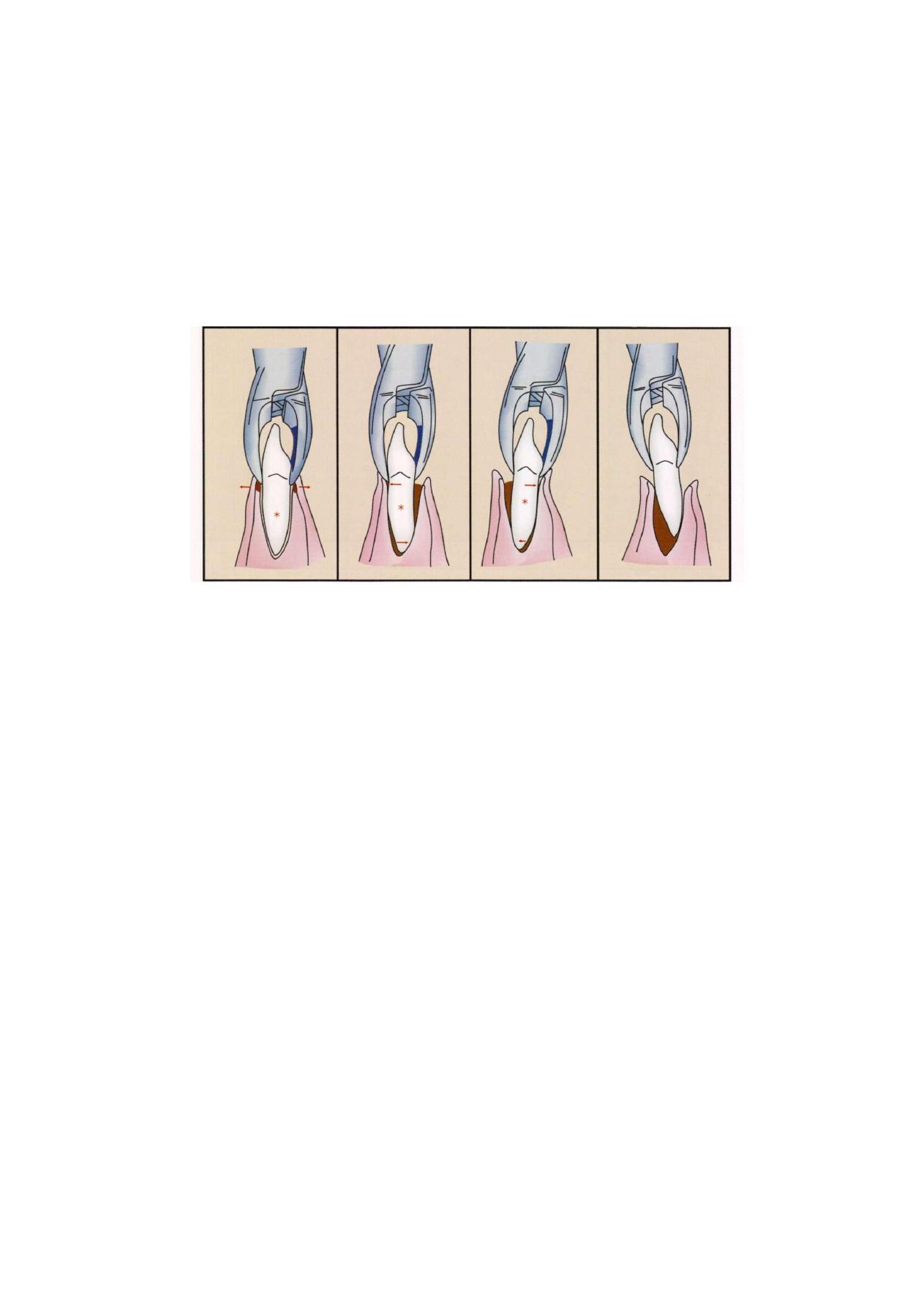
58
Exodontia Practice
F i g u r e 6.17: Extraction of mandibular anterior tooth
MANDIBULAR PREMOLARS
The mandibular premolars are among the easiest of all
teeth to remove. The roots tend to be straight and conical,
sometimes slender. The overlying alveolar bone is thin
on the buccal aspect and somewhat heavier on the lingual
side.
The forceps usually chosen for extraction of the
mandibular premolars are the lower premolar forceps.
The forceps are forced apically as far as possible with the
basic movements being toward the buccal aspect,
returning to the lingual aspect, and finally rotating. Rota-
tional movement is used more when extracting these teeth
than any others except the maxillary central incisor. The
tooth is then delivered in the occlusal-buccal direction.
Careful preoperative radiographic assessment must be
performed to assure the operator that no root curvature
exists in the apical third of the tooth. If such a curvature
does exist, the rotational movements should be reduced
or eliminated from the extraction procedure (Figure 6.18).
MANDIBULAR MOLARS
The mandibular molars are usually two-rooted with roots
of the first molar more widely divergent than those of
the second molar. Additionally, the roots may converge
at the apical one-third, which increases the difficulty of
extraction. The roots are generally heavy and strong.
The overlying alveolar bone is heavier than the bone
on any other teeth in the mouth. The combination of
relatively long, strong, divergent roots with heavy
overlying buccal and lingual bone makes the mandibular
first molar the most difficult of all teeth to extract.
The forceps usually used for extraction of the
mandibular molars are mandibular forceps. The forceps
are adapted to the root of the tooth in the usual fashion,
and strong apical pressure is applied to set the beaks
of the forceps apically as far as possible. Strong buccal
and lingual motion is then used to expand the tooth
socket and allow the tooth to be delivered in the buccal-
occlusal direction. The lingual alveolar bone around the
second molar is thinner than the buccal plate so the
second molar can be more easily removed with stronger
lingual than buccal pressures (Figure 6.19).
If the tooth roots are clearly bifurcated, the cow horn,
forceps can be used. These forceps are designed to be
closed forcefully with the handles, thereby squeezing
the beaks of the forceps into the bifurcation. This creates
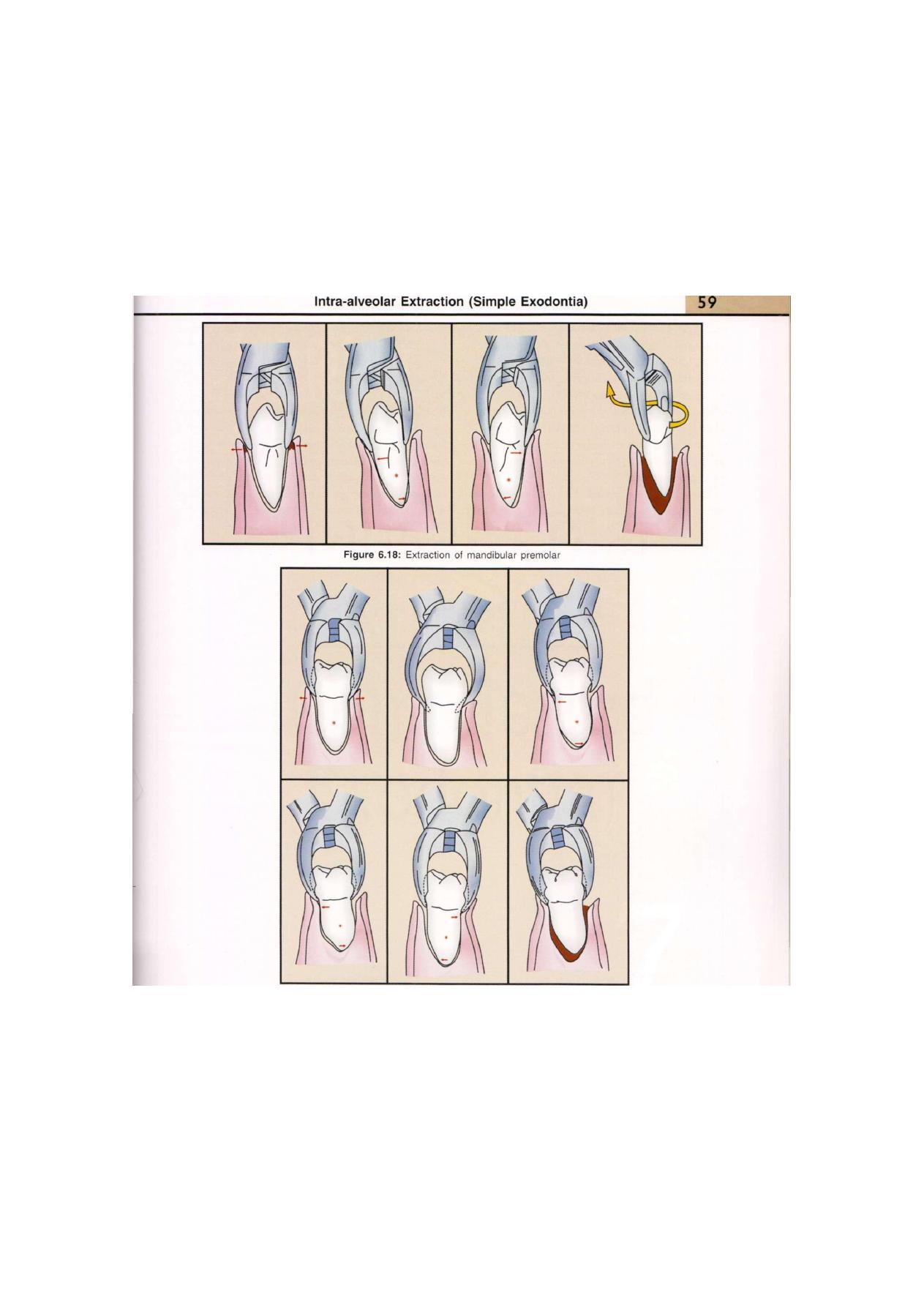
Figure 6.19: Extraction of mandibular molar

60
Exodontia Practice
force against the crest of the alveolar ridge on the buccal
and lingual aspects and literally forces the tooth superiorly
directly out of the tooth socket. If initially this is not
successful, the forceps are given buccal and lingual
movements to expand the alveolar bone, and more
squeezing of the handles is performed. Care must be
taken with these forceps to prevent damaging the
maxillary teeth, since the lower molar may actually pop
out of the socket and thus release the forceps to strike
the upper teeth.
Erupted mandibular third molars usually have fused
conical roots. Since there is not usually a bifurcation,
the short-beaked, right-angled universal forceps is used
for extraction. The lingual plate of bone is definitely thinner
than the buccal cortical plate, so most of the extraction
forces should be delivered to the lingual aspect. The third
molar is delivered in the lingual-occlusal direction. The
erupted mandibular third molar that is in function can
be a deceptively difficult tooth to extract. The dentist
should give serious consideration to using the straight
elevator to achieve a moderate degree of luxation before
applying the forceps. Pressure should be gradually
increased, and attempts to mobilize the tooth should be
made before final strong pressures are delivered.
Transalveolar
Extraction
(Complicated
Exodontia)

62
Exodontia Practice
Exodontia or tooth extraction is painless removal of a
whole tooth or tooth-root, with minimal trauma to the
investing tissues, so that the wound heals uneventfully
and no postoperative prosthetic problem is created.
DEFINITION OF COMPLETE EXODONTIA
Complex extractions are defined as those extractions,
not involving impaction, which cannot be removed by
a simple application of elevators and forceps.
PETERSON
Complex extractions are retrieval of tooth root and teeth
which are likely to fracture for some other reason and
have an obstacle to extraction.
The surgical removal of tooth is the method used for
recovering roots that were fractured during routine
extraction or teeth that cannot be extracted by close
method of extraction. This chapter discusses the
technique for surgical removal of teeth, with different
principles involved.
FACTORS THAT COMPLICATE THE
EXTRACTION PROCEDURE
Factors that complicate the extraction procedure from
simple to complicated extraction are as follows. These
factors can be evaluated clinically and radiographically
before going for extraction of any tooth.
1. Crown
2. Roots
3. Bone
4. Diminished access
5. Adjacent/non-adjacent teeth
6. Adjacent vital structures
7. Prosthetic concerns
CROWN
In cases where crown is destroyed by caries, complex
restorations, fixed prosthesis, etc. the nature of the
coronal portion of the tooth may prevent the application
of instruments and therefore the application of forces.
Crowns may get crushed or shattered when gripped by
the forceps (Figure 7.1). Teeth which have lost their
crowns due to caries or fracture should be evaluated for
necessity to undergo open extraction.
F i g u r e 7 . 1 : Badly carious tooth
ROOTS
All those roots that result in unfavorable path of removal
or increased resistance are enumerated as under:
a. Multiple roots
b. Bulbous roots
c. Root canal treated teeth
d. Hypercementosis
e. Ankylosed teeth
f. Divergent roots
g. Dilacerated roots
Multiple Roots
In teeth that have multiple roots individual roots may
have different long axes. It is essential to apply the forces
along the long axes of the tooth and hence it is necessary
to remove each root along its long axis. Hence, there
might be a need for transalveolar extraction of that tooth
(Figure 7.2).
Bulbous Roots
In teeth that have bulbous roots there is mechanical
obstruction to retrieval of the root. Inspite of expansion
of the socket there might not be enough space for delivery
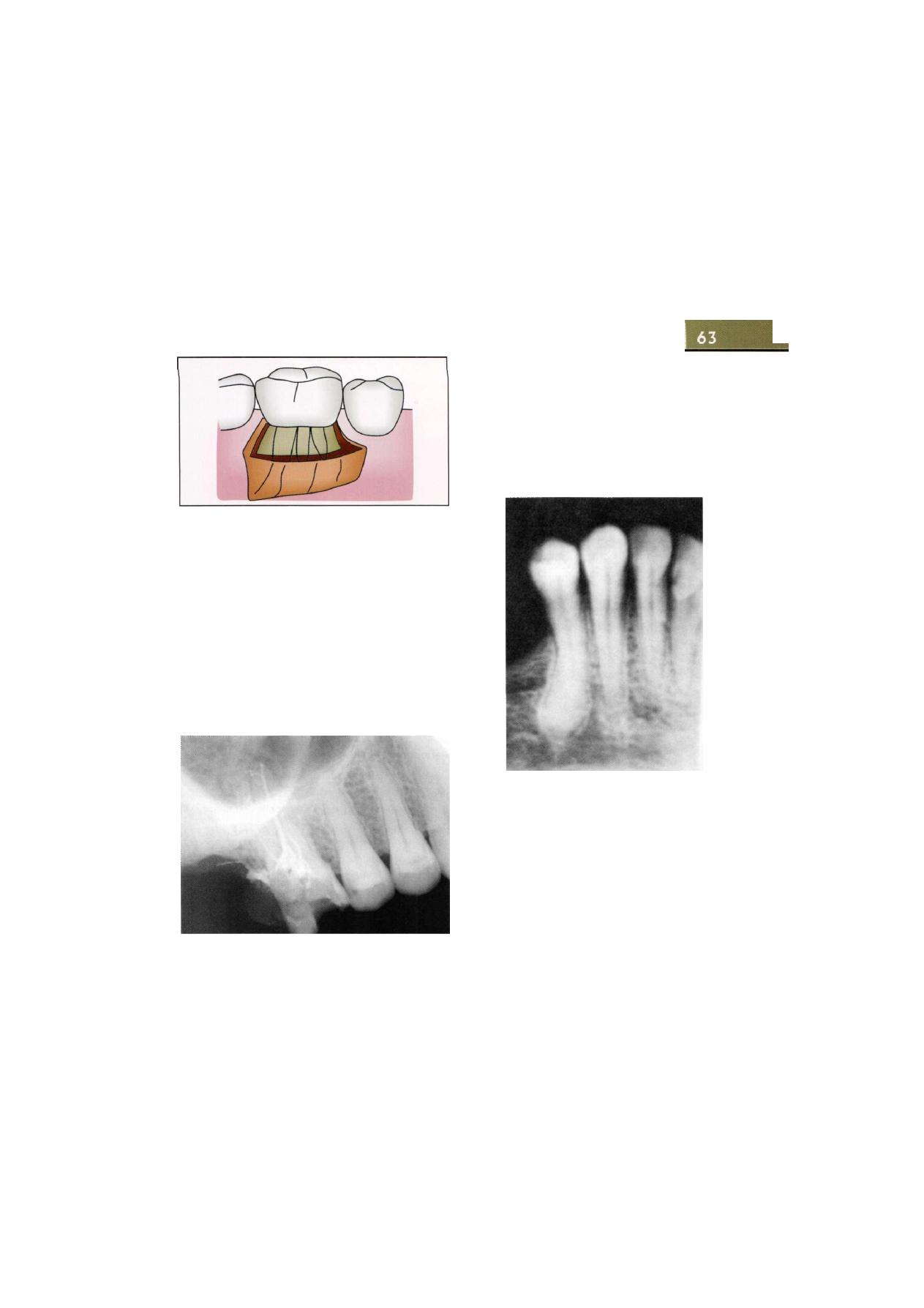
Transalveolar Extraction (Complicated Exodontia)
F i g u r e 7.2: Multiple roots
of the root from the socket. Hence, such teeth should
be considered for open extractions.
Root Canal Treatment
Teeth become brittle following root canal treatment
mainly because of two reasons, viz. cutting of the tooth
structure for endodontic treatment and because of
dehydration of dentin following cessation of blood supply.
The dentin becomes dessicated and hence, becomes
brittle. Thus the tooth may crush during application of
extraction forces due to either reduced bulk of the tooth
or brittleness of the remaining tooth structure (Figure 7.3).
accelerated elongation of tooth, tooth repair and Paget's
disease. It is difficult to remove the root in such cases
through the available root socket because of smaller
diameter of the socket at the cervical level. Due to
difficulty in delivery of the root the operator might use
increased forces which may cause root/bone fracture.
Such roots require thorough radiographic evaluation and
extractions by open technique (Figure 7.4).
F i g u r e 7.3: Root canal treated tooth
Hypercementosis
Hypercementosis occurs because of continuous deposi-
tion of cementum forming large bulbous roots especially
in apical region. It occurs in chronic inflammation,
F i g u r e 7.4: Hypercementosis
Ankylosis
In this condition tooth is fused to alveolar bone. There
is no intervening periodontal ligament. During extraction
tooth is delivered from socket after severing of perio-
dontal ligament. Hence, in ankylosed tooth delivery of
tooth from socket is not possible. If excessive force is
applied fracture of root or alveolar bone will occur. This
condition is diagnosed using radiographs. On radio-
graphic examination there is no periodontal ligament
seen surrounding the root and there is bony union of
tooth. On clinical examination dull tone is heard when
tooth is percussed and no mobility can be felt when
luxation of the root is attempted (Figure 7.5).
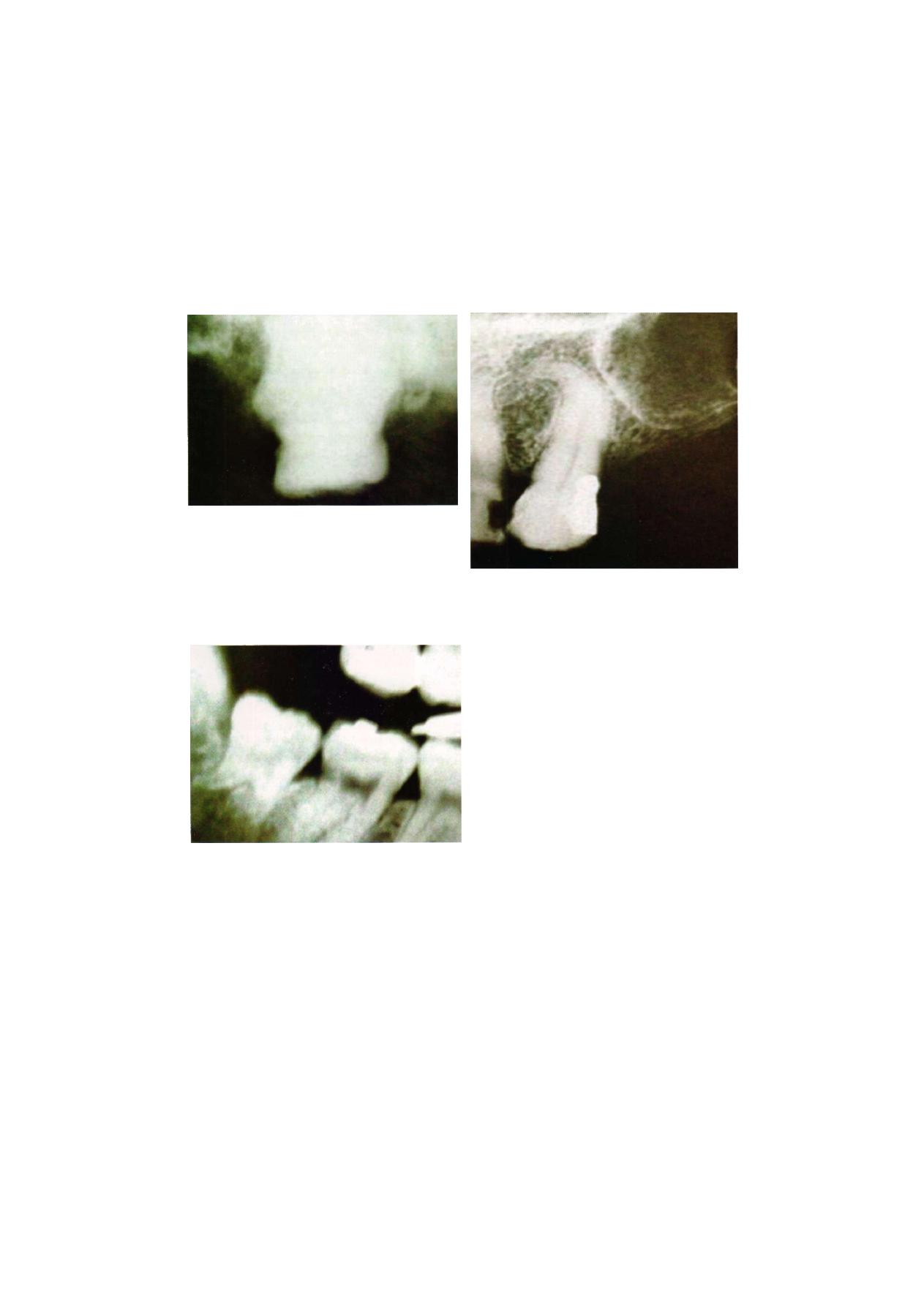
Exodontia Practice
F i g u r e 7.5: Ankylosed tooth
Divergent Root
It occurs in some multirooted teeth; especially maxillary
molars. Due to non-parallelism of long axes of the roots
there is increased difficulty to extract tooth in one piece.
Hence, transalveolar extraction needs to be carried out
to extract the tooth uneventfully (Figure 7.6).
F i g u r e 7.6: Divergent root
Dilacerated Roots
In dilacerated roots there is hooking of root to alveolar
bone. Hence, there is an increased resistance to delivery
of tooth while normal extraction forces are applied
and it is difficult to deliver the tooth from the socket
without fracture of the root at the point of hooking
(Figure 7.7).
F i g u r e 7.7: Dilacerated roots
BONE
The points to be considered are as follows:
a. Periodontal health
b. Increased bone density
c. Increased bone bulk
Periodontal Health
The periodontal health determines firmness of tooth and
hence, difficulty of extraction. In case the periodontal
health is weak, the tooth will be mobile and hence, will
be easily delivered from the socket. Conversely, in case
of teeth with good periodontal health more is the
difficulty while extracting the teeth. In cases such as long
standing tooth, para-functional habits like bruxism,
clenching there is an increase in the width of periodontal
ligament. Hence, it becomes difficult to shear the
periodontal ligament from bone and tooth, and the
delivery of the tooth becomes difficult.
Increased Bone Density
In cases of bruxism and localized osteitis there is a significant
increase in bone density chiefly on buccal cortical plate.
The extraction depends chiefly on expansion of buccal
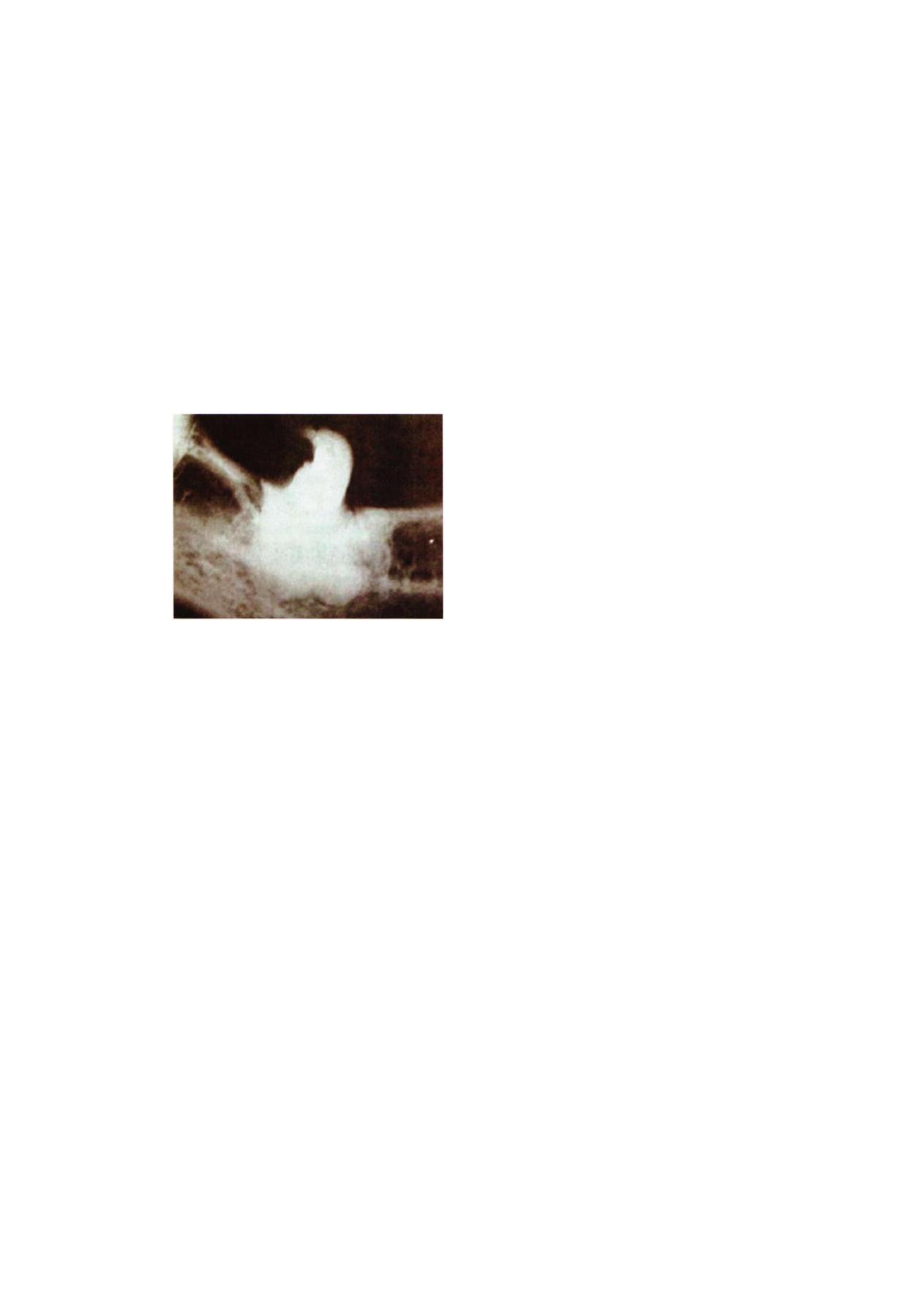
Transalveolar Extraction (Complicated Exodontia)
65
cortical plate. In cases of increased bone density expansion
of socket is difficult and hence, there is difficulty in
extraction of the tooth. This necessitates use of trans-
alveolar method of extraction (Figure 7.8).
F i g u r e 7.8: Increased bone density around the tooth
Increased Bulk
Increase in bulk of bone occurs due to presence of bony
exostosis on the buccal or lingual cortical plate. This
increases the difficulty in socket expansion and therefore
extraction of the concerned tooth.
DIMINISHED ACCESS
Diminished access results chiefly from trismus resulting
from infection of sub-masseteric space, oral submucous
fibrosis, scleroderma. In case of sub-masseteric space
infection trismus is the hallmark due to inflammation and
spasm of Masseter muscle. Scleroderma or systemic
sclerosis is a condition wherein there is progressive fibrosis
of skin and various organs of the body. Oral manifesta-
tions are that lips become thin, firm and partially fixed
leading to microstomia. Gingiva becomes firm. The
reduced mouth opening is due to involvement of
temporomandibular joint tissues. This makes dental care
difficult. Due to decreased oral opening, application of
instruments along long axes of teeth is difficult and
sometimes impossible. This results in inability to apply
correct forces. Difficulty is much more in posterior teeth
than anterior.
ADJACENT TEETH
In case of highly carious, heavily restored, endo-
dontically treated adjacent teeth there are chances of
fracture of the teeth due to either wrong application
of elevator force or transmitted force. In case of
periodontally compromised teeth there are chances of
inadvertent extraction of the adjacent tooth causing
grevious injury due to wrong application of force or
transmitted forces. A long maxillary molar or canine has
dense bone surrounding it with strong periodontal
attachment due to the increased functional load that
it bears. This causes difficulty in socket expansion and
extraction. In case of maxillary molar, the maxillary sinus
may have expanded to include roots of the molar.
Extraction may result in removal of part of sinus floor
and formation of oroantral communication. In divergent
roots these chances increase.
PROXIMITY TO VITAL STRDCTURES
The vital structures that could be in close proximity
to the teeth are inferior alveolar bundle, lingual
nerve, maxillary sinus. In case of inferior alveolar nerve,
risk of nerve injury during extraction of mandibular third
molar is mainly during elevation of a mesioangular tooth.
If the nerve is close to the apices of the tooth it might
come in the arc of rotation and get compressed causing
neuropraxia. In case of lingual nerve, due to its supra-
periosteal course close to the 3rd molar, there are chances
of damage during raising of mucoperiosteal flap. In
addition, in cases of difficult extraction, due to trauma
to the surrounding soft tissue during the extraction, the
lingual nerve might get damaged. The maxillary
sinus when close to the apices of maxillary molars carries
the risk of formation of an oro-antral communication.
Hence, when tooth is in close proximity to the vital
structures, it is essential to consider open extractions
(Figure 7.9).
/
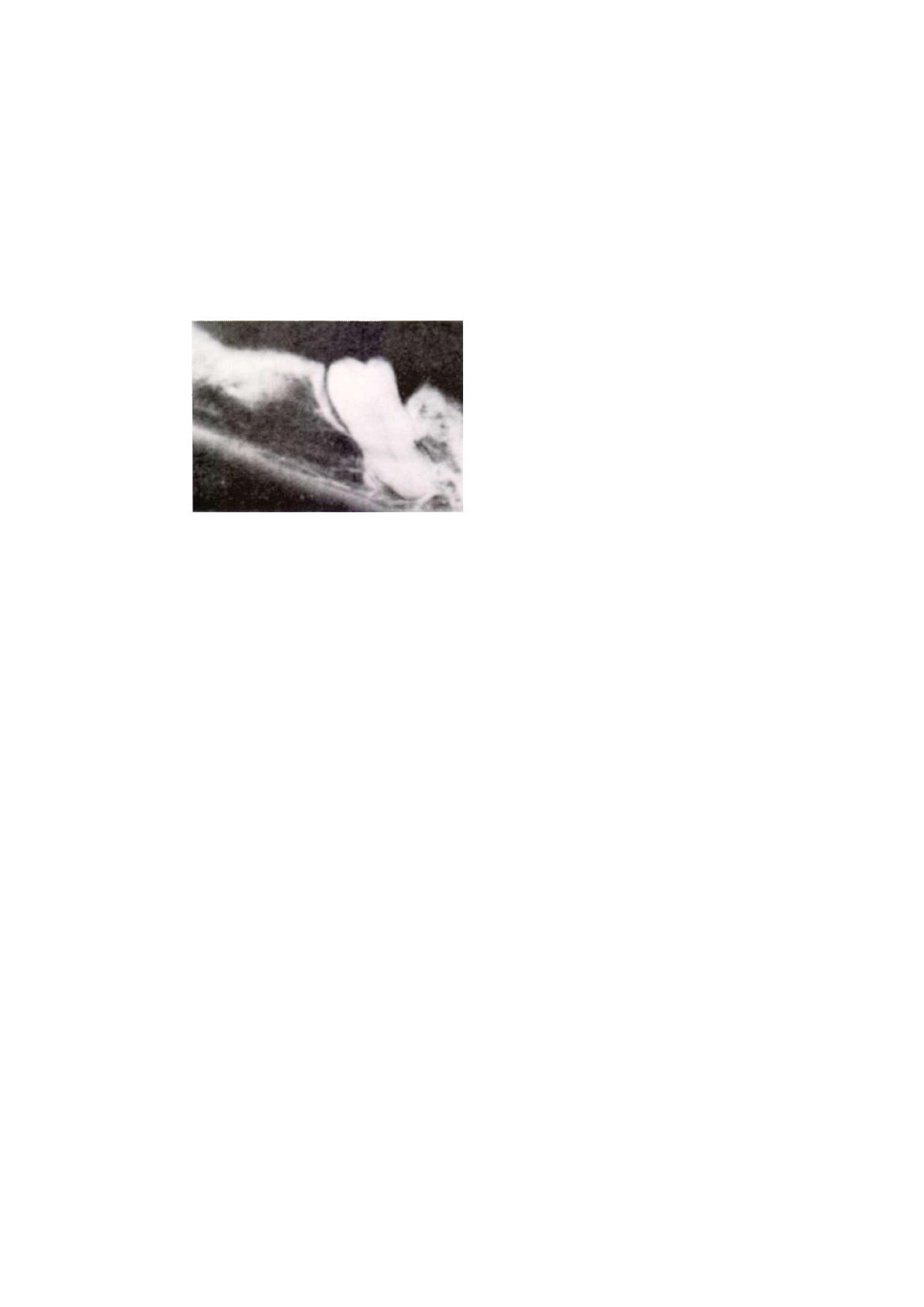
66
Exodontia Practice
F i g u r e 7.9: Tooth in close proximity to inferior
alveolar nerve
PROSTHETIC CONCERNS
These include preservation of alveolus. When intra-
alveolar extraction will cause more bone loss than
transalveolar extraction, it is more prudent to opt for open
extraction rather than try to perform a closed extraction.
The next concern is maintaining correct alveolar contour.
In case there is a existing bony undercut due to
proclination of teeth, and an alveoloplasty is essential
before prosthetic rehabilitation can be done, then
performing an open extraction and performing an
alveoloplasty at the same time is advisable. The third
concern is preservation of attached gingiva of the
adjacent teeth which might get damaged due to excessive
trauma to the surrounding soft tissues due to overzealous
attempt to perform a difficult extraction and will lead
to loss of attached gingiva, pocket formation.
Once all these parameters are evaluated the following
technical observations are taken in to consideration:
1. Basic steps such as severing periodontal ligament,
expanding alveolus, and applying traction don't
work.
2. Correct application of forceps not possible or inspite
of correct application of forceps correct delivery of
forces not possible.
3. Need to alter ability to apply the correct force and
achieve the treatment objective
Following are the technical goals to be achie-
ved at the time of complicated exodontia:
1. To improve the mechanical advantage
2. To reduce resistance
3. To correct an inadequate path of withdrawal.
1. Improved access: This is done by raising a
mucoperiosteal flap and adequate bone removal
2. Improved mechanical advantage: This is achieved by
bone removal and preparation of purchase point.
3. Reduce resistance: This is achieved by removal of
bone support and sectioning of teeth (Odontectomy)
4. Correct path of removal: This is achieved by removal
of bone and sectioning of teeth.
Following are the principles involved during
the surgical removal of teeth:
1. Flap design
2. Bone removal
3. Sectioning teeth
4. Wound closure.
PRINCIPLES OF FLAP DESIGN
INCISION
A gingival margin incision which divides the mandibular
interdental papillae will permit the insertion of a periosteal
elevator and the reflection of either the buccal or lingual
mucoperiosteum or both. If necessary, the papillae can
be divided from one side molar around to the other
without the operator encountering any sizeable vessel.
Similarly, an incision along the crest of the mandibular
edentulous ridge will also permit buccal and lingual
mucoperiosteal flaps to be raised. Such flaps are
described as envelope flaps.
If required the incision can be extended backwards
into the retromolar region and then distobucally up the
external oblique ridge and anterior border of the coronoid
process. No vessel of a size requiring formal ligation will
be encountered until this upwards extension of the
incision reaches a point just below the level of the occlusal
surface of the upper 3rd molar. Here the buccal artery
and long buccal nerve lie side by side and cross the

Transalveolar Extraction (Complicated Exodontia)
67
anterior border of the coronoid from medial to lateral
on the superficial aspect of the buccinator muscle. The
deep facial vein runs either with the artery and nerve
or a little higher up.
By dividing the interdental papillae or by incising
along the edentulous ridge, depending upon whether
teeth are present or not. And then raising flaps, the outer
and palatal aspects of the maxillary alveolar process can
be exposed in a similar fashion. Again no sizeable vessel
will be cut while making these incisions.
A second incision can be added which starts at one
end of the crestal incision and is carried towards the
buccal sulcus. The second incision can be a straight one
which leaves the first at an obtuse angle, or with the
edentulous ridge the crestal incision can be continued
in a curve onto the buccal aspect of the alveolar process.
In the dentulous patient the oblique relieving incision
should include an interdental papilla at the corner to
locate the flap on replacement. This two-sided, or
triangular, flap is easy to retract and allows sufficient
access for many small dentoalveolar procedures to be
carried out, and is easy to suture. The addition of a
second buccal incision at the other end of the crestal
incision so creating a three sided quadrangular flap
increases still further the degree of surgical access. By
curving the sulcus ends of the incisions along the bottom
of the sulcus in a direction away from the center of the
flap the length of these relaxing incisions can be increased.
This permits the reflection of the tissues to a higher level
in the case of the maxilla or a lower one in the case
of the mandible.
It is a basic principle of flap design that the base of
the flap should be as wide as is practical to ensure a
good blood supply. However, where teeth are standing,
the angle at the gingival margin should be no more than
around 100° or a narrow V shaped strip will be left which
will have an inadequate blood supply at its tip.
In order to raise the flap along the gingival margin
of the teeth the papillae needs to be divided
interdentally. A No. 15 scalpel blade on a No. 3 handle
is held parallel to the long axis of the teeth with the
back of the blade interproximally and the cutting tip
used to incise vertically downwards, first the distal
attachment of the papilla then the mesial attachment
so dividing it like a wedge of cake. The blade may then
be passed along the gingival crevice to divide the next
papilla, but if this is done it should not cut the periodontal
fibers below the alveolar crest. Often as the flap is
reflected it will separate readily from the alveolar bone
and the neck of the tooth so that the connecting incisions
are not essential. In the edentulous jaw, however, the
attachment of the mucoperiosteum to the crest of the
ridge is particularly strong and not only the crestal incision
be made firmly down to bone but reflection of the flap
may need the assistance of the knife to cut the tough
fibrous connections and to free it from the adjacent bone.
The use of excessive force with a periosteal elevator may
tear the flap, either at this narrow zone of strong
attachment, or at the sulcus end of a two limbed incision.
It is important to design the incision so that a complete
interdental papilla is present at each end of a three-sided
flap, because this facilitates suturing through each
interdental space. Bringing together the buccal and
lingual papillae in this way produces excellent healing
without clinically detectable increase in the depth of the
gingival crevices. If such an incision is made in the
experimental animal and the healing studied, a small
down growth of epithelium will be found at the depth
of the gingival crevice. The extent is microscopic, and
not detectable clinically.
Recommendations have been made from time to time
that the marginal gingiva should be avoided when
outlining a flap, in order to prevent injury to epithelial
attachment. Those who follow this advice make a
horizontal incision 2-3 millimeters away from, and
parallel to, the gingival margin. Unfortunately the strip
of gingiva which is left covers the margin of the alveolar
bone. Should the excision of bone be carried too close
to the concealed socket margin while, for example,
removing an unerupted upper canine, the crestal
alveolar bone may be damaged. Loss of the marginal
bone will not be repaired and permanent damage to
\
Exodontia Practice
68
the tooth attachment will result. Retention of such a
strip of gum also reduces surgical access with the result
that it becomes traumatized both during the operation
and when suturing, so producing necrosis with
breakdown of the suture line. In addition, at the end
of the operation, a bone cavity, such as the socket of
a tooth or a cyst cavity, may lie close to the line of closure
so that the wound edges are not adequately supported,
Again the suture line will tend to break down and the
flap fall into the underlying bony defect.
'In general incision lines should be planned so that
at the end of the operative procedure there is still an
untouched zone of bone at the cavity margin to support
the edge of the flap that has been reflected. This will
provide a broad area of contact through which the
process of healing can reattach the wound margin and
develop an adequate degree of early wound strength
to resist any tension during movement of the face and
jaws in the period immediately after the removal of the
sutures.
Mucoperiosteal flaps are relatively thin and do not
possess layers which can be closed separately, of necessity
any surgically created bone cavity forms a dead space
and creates a hematoma. It is important to seal this
effectively from the mouth and the possible ingress of
infection. Failure to achieve primary wound healing for
this or other reasons leads to exposure of the underlying
clot, leaving a cavity which will be repaired slowly by
'secondary intention'.
As alveolar wounds cannot be closed in layers a valve-
like closure is the best that can be achieved. Sitting the
incision so that there is a zone of intact bone between
the cavity margin and the line of the soft tissue wound
provides for such a valve-like closure. Where unavoidably
the incision line crosses the cavity, eversion of the wound
edge by mattress sutures creates an additional zone of
tissue contact, but not as secure a closure as one
supported on bone.
Provided incisions are confined to the mucoperio-
steum of the alveolar process or the palate, that is the
masticatory mucosa, the sutured wound is subject to
little tension. The sulcus tissues in contrast are elastic
and the wound edges contract away from one another,
though normally not so as to create a significant tension
in the sutured wound. Incisions made in the sulcus
radially or at right angles to the outer aspect of the jaw
are not subject to muscular pull and are readily closed
with little risk of wound dehiscence during healing. On
the other hand, horizontally aligned incisions in the sulcus
in some parts of the mouth are subject to tension during
movements of the jaws, lips and cheeks and are best
avoided. If such an incision is necessary, special care
is required in its closure to avoid wound breakdown.
For example, the design of flap often used when an
apicectomy is performed upon an anterior tooth is a
semilunar one with the convexity towards the gingival
margin. The incision for such a flap should not approach
closer to the gingival margin than one third of the depth
of the sulcus. Such a flap suffers from all of the dis-
advantages mentioned above. If the incision approaches
closer to the gingival margin, the remaining strip of gum
may slough, because its blood supply may be inadequate,
particularly after sutures have been passed through it.
Furthermore, it is not always easy to predict how large
the surgical cavity may be at the end of the operation,
particularly if a small cyst is to be dealt with during the
apicectomy, and the flap may be inadequately supported
at its margin. Finally the suture line will be under tension.
This can be seen as soon as the sutures are inserted
because the wound edges will gape between the sutures.
Some operators attempt to overcome this problem by
using horizontal mattress sutures, but there is a danger
with such a small wound that they will be drawn too
tight and strangulate the wound margin, particularly on
the gingival side. A three-sided flap which includes the
gingival margin of the tooth to be operated upon and
its interdental papillae is more satisfactory.
The problem of tension from muscular activity is
encountered again when horizontal incisions are made
either to 'deglove' the chin or to expose the anterior part
of the maxilla during a Le Fort I level osteotomy. Such
incisions should be made so that a generous skirt of
Transalveolar Extraction (Complicated Exodontia)
sulcus mucosa is left on the gingival aspect. In the case
of the mandible the incision should be carried out on
the labial aspect of the sulcus and then obliquely
downwards through the mentalis muscles to provide a
sufficient thickness of tissues on the gingival side to hold
sutures, A continuous horizontal mattress suture line will
bring the deeper tissues together and evert the wound
margin, but should not be drawn excessively tight, nor
should large bites of tissue be taken at each horizontal
step or the wound edge will be strangulated and slough.
The epithelial edges are coadapted by oversewing with
a continuous plain suture.
INSTRUMENTATION
In general incisions in the perioral tissues are made with
a No. 15 blade. The scalpel handle is held at an acute
angle with the proposed incision line but with the flat
of the blade at right angles to the surface. This way much
of the length of the cutting edge will be employed in
making the incision and it will be deepened progressively
down to the level of the tip of the blade. If the knife
is held with the blade vertically in the tissues they will
tend to bunch up ahead of the blade and a ragged cut
will result. Where mucoperiosteum is being incised, the
tissues are held steady by the underlying bone and a
clean cut is easily produced. Where soft tissues unsup-
ported by bone are being cut they must be stretched
gently at right angles to the line of incision, for example
on the inner aspect of the lip. Where thick tissues are
to be divided, such as those over the anterior border
of the coronoid process, the incision can be deepened
progressively by a succession of passages of the knife.
This way the direction of the cut can be controlled,
divided vessels identified and picked up with artery
forceps and damage to any important structures avoided.
If an attempt is made to divide the full thickness in one
sweep of the knife the operator will be tempted to plunge
the scalpel blade in at right angles to the surface so
bunching up the tissues as described above or resorting
to a sawing motion, all of which will result in a ragged
incision. \
In order to incise the periosteum cleanly, a degree
of pressure onto the bone must be maintained as the
blade is advanced. After a short while this will blunt the
edge of the blade. Incising over an unerupted tooth will
also damage the scalpel edge and a new blade should
be fitted before further incisions are made.
Loose connective tissue can be broken down by
pushing the ends of the closed blades of a pair of scissors
into the tissue then opening them. Performed with care
this type of blunt dissection will permit vessels and nerves
which are passing through such tissue to be displayed.
The excessive use of blunt dissection, however, is a bad
habit which will cause unnecessary tissue damage, untidy
wounds and imprecise surgery. Scissors can be used as
an alternative to a scalpel to divide sheets of soft tissue,
usually thin muscles and sheets of connective tissue and
mostly in a direction across the fibres. They are also used
to divide loose connective tissue to avoid excessive blunt
dissection.
Periosteum is raised from the bone with periosteal
elevators. These may have a thin rounded edge or a
sharpened edge flush with one surface and the end may
be curved to enable it to be applied closely to curved
bone surfaces. A blade end set at an angle to the handle
like a hockey stick is used in cleft palate surgery and
angled Warwick James' root elevators may be used as
substitutes for such periosteal elevators to raise the edges
of palatal incisions.
Large bi-angled spoon excavators also form excellent
miniature periosteal elevators when it is necessary to raise
soft tissues from bone in a confined space such as a cyst
cavity.
The fibers of most tendinous insertions lie almost
parallel with the surface and a periosteal elevator
advanced from the bone to the edge of the insertion
will slip up over the surface of the tendon. The muscle
insertion should be approached from the side.
FLAP REFLECTION
Flaps are raised by dissecting parallel to the surface at
the junction of tissue layers. Where these have similar
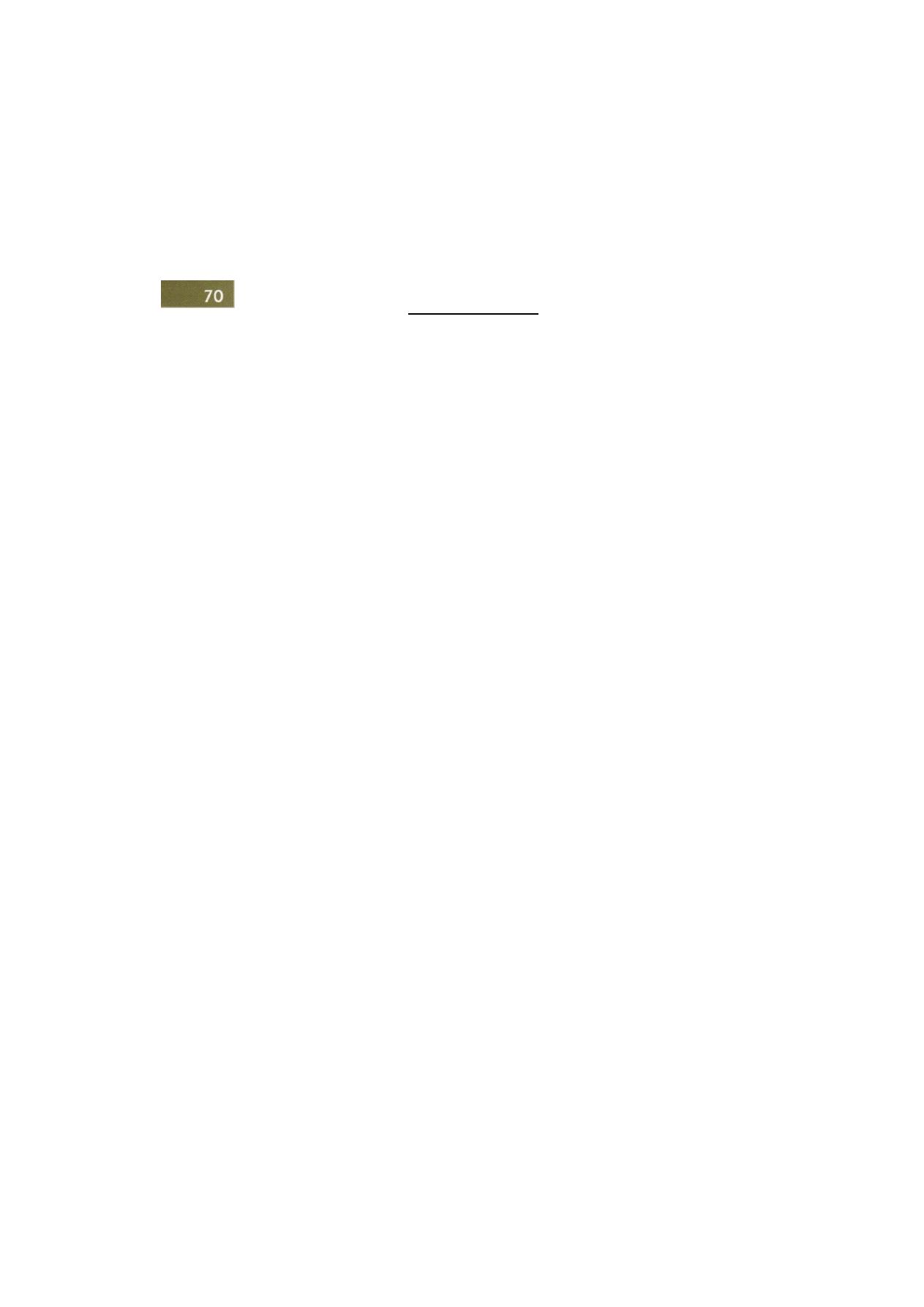
Exodontia Practice
l
mechanical properties, such as the junction of soft tissue
layers sharp dissection is used. Mostly dental surgeons
are intent upon exposing the mandible and maxilla so
that flaps are raised subperiosteally. This is done by blunt
dissection with a periosteal elevator, making use of the
well-defined plane of mechanical discontinuity between
the soft tissues and the hard bone. The attachment of
the periosteum to bone varies in strength from place to
place. The interdental papillae are firmly attached to the
cribriform surface of the tops of the interdental septa.
In the edentulous jaw this cribriform bone forms a narrow
continuous strip along the crest of the ridge. Connective
tissue fibers and vessels which pass from bone to
periosteum resist separation by the periosteal elevator
and it may be necessary to cut them with a scalpel. The
surface of the bone beyond the alveolar process can be
exposed by further elevation of periosteum and overlying
soft tissues, but a sufficient mesiodistal length of flap
needs to be developed to permit adequate retraction and
comfortable access to the bone at the operation site. On
the outer aspect of the body of the mandible several
structures are encountered which require special
attention. Foremost of these is the mental nerve. As the
periosteum is reflected in the region of the apices of the
mandibular premolar teeth, care should be taken until
the foramen is found. Gentle use of the periosteal elevator
will preserve the mental nerve and vessels inside their
conical sleeve of periosteum.
Special care should be taken where the patient is
edentulous. If the alveolar process is atrophic the mental
foramen will be relatively close to the crest of the ridge.
Indeed where resorption has been extreme the nerve may
emerge on the crest of the residual ridge and can be
seen radiating outwards beneath the mucosa.
Anterior to and below the mental foramen there are
the origins of the depressor labii and depressor anguli
oris muscles and the insertion of the platysma muscle.
These add only a marginally stronger attachment of the
soft tissues to the mandible. In contrast, the origin of
the mentillis muscle below the incisors requires a
substantial effort. Indeed the periosteum is firmly attached
over the whole mental eminence.
The attachment of the buccinator to the mandible
is easily disrupted, but it should not be raised unless the
additional access is definitely required. Once the edge
of the muscle has been separated edema of the buccal
space is facilitated producing a greater degree of facial
swelling postoperatively. As the body of the mandible
is uncovered buccal to the second molar it should be
remembered that the facial artery and vein lie
immediately external to the periosteum at this point.
More posteriorly the insertion of the masseter needs
to be separated to expose the outer aspect of the
mandibular angle. This requires little effort until the
posterior border of the ramus and the lower border of
the angle are reached. However, the tough, inelastic
periosteum may need to be incised by a few gentle strokes
across the inner surface to permit adequate retraction
of the muscle to allow work on the underlying bone.
The shape of the mandible makes surgical access to
its inner aspect awkward and this difficulty is increased
by strong muscle origins. The genial muscles can be
detached only by cutting through their origin, close to
the tubercles and of course if complete detachment is
necessary, they should be reattached. The sublingual
arteries enter the mandible through a single foramen just
above the tubercles and if divided they must be ligated
or the bleeding from them arrested with coagulation
diathermy. The mylohyoid origin extends from the third
molar region to the midline and is not at all easy to
separate from the bone, mainly because the muscle
slopes downwards and the periosteal elevator more easily
perforates the thin lingual periosteum and slips over the
surface of the muscle rather than lifting it from the bone.
It may be detached, if this is necessary, by hooking a
narrow, curved elevator beneath the posterior border
and detaching it from below upwards. This should be
done with care and it may damage the mylohyoid nerve
producing a transient patch of cutaneous anesthesia on
the point of the chin. Naturally in the elevation of the
mucoperiosteum on the lingual aspect of the 3rd molar
region the lingual nerve must be safeguarded. Even the
exposure of no more than the lingual aspect of the

Transalveolar Extraction (Complicated Exodontia)
7
alveolar process requires care because, except in the 3rd
molar region, the mucoperiosteum is thin and easily torn.
Any tear in the lingual periosteum will permit blood to
spread into the lax tissues of the floor of the mouth
forming a bulky hematoma.
As the outer surface of the maxilla above the alveolar
process is uncovered few obstacles are encountered. The
buccinator attachment is barely noticed and there is only
little resistance from the levator anguli oris. In contrast
the depressor septi muscles form a fleshy zone over the
central Incisors which requires some care during flap
reflection. Once the anterior bony aperture of the nose
is reached the reflection of the periosteum into the nasal
aspect of the maxilla impedes further mobilization of the
soft tissues. Caution should be exercised high on the
anterolateral aspect of the maxilla to identify and preserve
the infraorbital nerve. This is done by elevating the soft
tissues with a swab enclosed finger. Behind the zygomatic
buttress or zygomaticoalveolar crest on the posterolateral
aspect of the rnaxilla again the periosteum should be
raised gently. It is easily stripped from the bone but care
is necessary to avoid unnecessary damage to the
posterior superior dental artery as it enters the bone.
Exploration high up on the back of the maxilla leads
to its disruption and the onset of a brisk ooze. While
the hemorrhage is usually on a small scale. It can be
troublesome in this corner where visibility is bound to
be poor. Also a breach in the periosteum will release
the buccal pad of fat creating an even greater impediment
to vision. The mucoperiosteum of the hard palate is
normally raised by incising the interdental papillae or
by making an incision around the crest of the edentulous
ridge. The palatal mucoperiosteum is tightly attached at
the margin of such a flap so care must be taken not to
use a tooth as a fulcrum for the periosteal elevator when
it is raised. Initial elevation of the margin may be
facilitated by using the spoon-shaped end of a curved
Warwick James elevator. The mucosa is also tightly
attached to the median palatal suture and tethered to
the contents of the incisive fossa. Normally a generous
length of the curvature of the upper dental arch is needed
to form a useful flap. However, redially placed relieving
incisions can be made to limit the amount of mucosa
which is raised to gain access to the surgical site. These
should be short so as not to cut the greater palatine
neurovascular bundle. Division of the palatine artery
leads to a brisk hemorrhage which is best controlled by
elevation of the posterior margin of the cut, the appli-
cation of hemostat and underrunning the vessel with a
resorbable stitch which is then tied to form a ligature.
In order to raise the full width of the palate elevation
is started at a premolar interdental papilla on each side
and separation is carried up to and around the incisive
fossa structures. The nasopalatine nerves and vessels are
divided as they enter the deep surface of the flap and
rarely cause trouble either with hemorrhage or post-
operative loss of sensation. Posteriorly the greater
palatine neurovascular bundles in the adult emerge
opposite the second molars and must be preserved with
care. Damage to both can result in death of the flap.
Damage to one may result in cyanosis of the edge of
the flap.
Access just to the centre of the palate can be made
by a midline incision. The mucosa is thin, as well as tightly
adherent on either side of the midline, but can be raised
with care and retracted to expose the underlying bone.
A V shaped extension about the incisive fossa anteriorly
increases access if this is necessary, but should not extend
so far laterally as to divide the palatine vessels. Further
reflection of the mucosa can be achieved by a V shaped
cut at the posterior end but the thickness of the mucosa
at this site makes such an extension less helpful. In making
a posterior V shaped cut the incisions should not be
carried on to the soft palate nor should they be made
so as to endanger the greater palatine vessels.
TYPES OF FLAPS
• Envelope flop: In this type of flap, only crevicular
incisions are given and mucoperiosteal flap is raised
(Figure 7.10).
• Three cornered/triangular flap: In this type of flap,
in addition to the crevicular incisions, one release
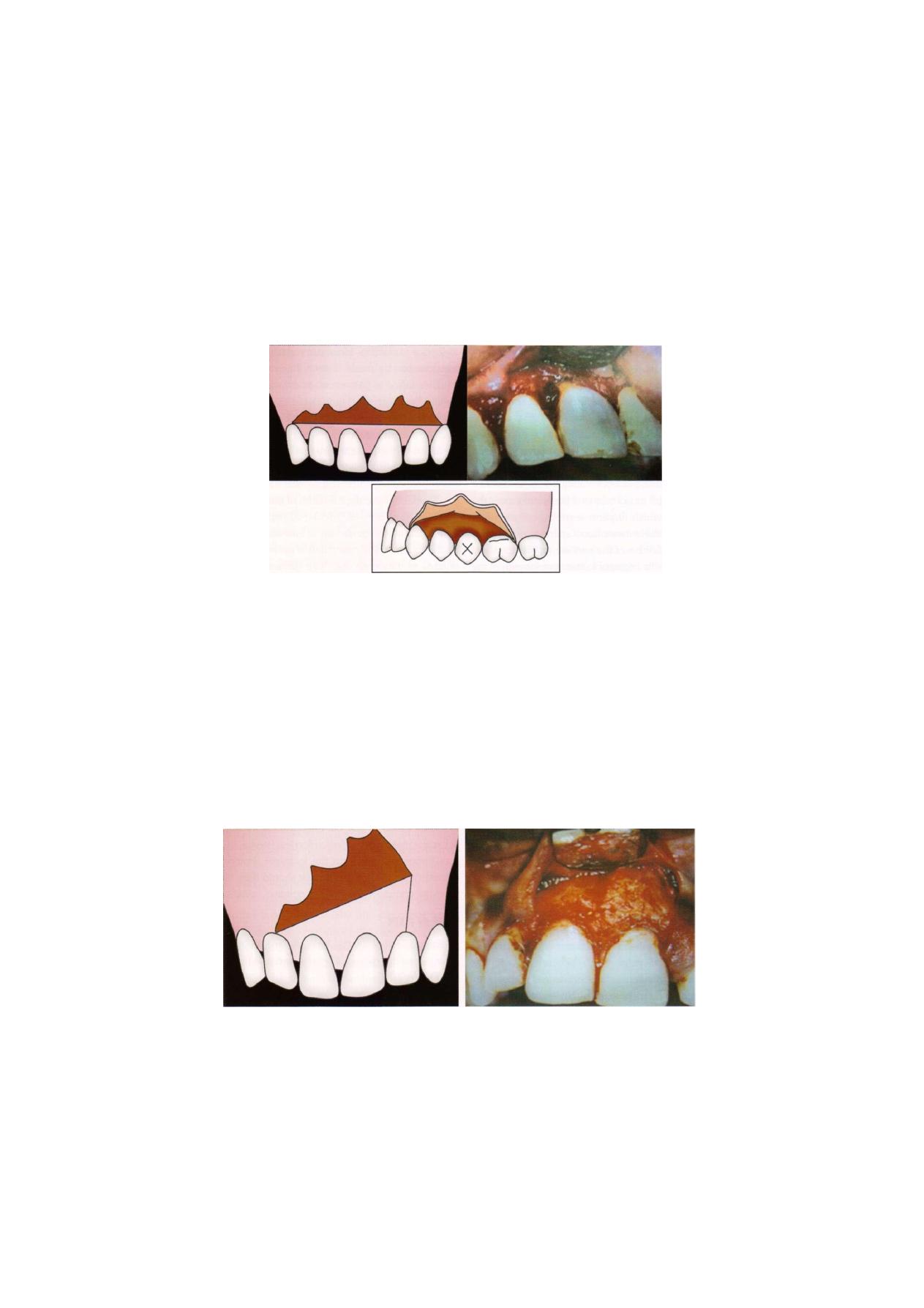
\
Exodontia Practice
F i g u r e 7.10: Envelop flap
incision usually anteriorly is given, such that the flap
has two edges and three angles (Figure 7.11).
Four cornered flap: In this flap there are two releasing
incisions in addition to the crevicular incision.
Thus this flap has three edges and four angles (Figure
7.12).
The release incisions should lie on the mesio-
buccal or distobuccal line angle of the tooth and on
sound bone (Figure 7.13).
Release incisions on the facial aspect of crown don't
heal properly due to tension and sometimes results
in vertical clefting of bone.
• Incisions that cross gingival papilla damages the
papilla unnecessarily and increased chances of
localized periodontal problems.
INCISIONS (FIGURES 7.14A TO C)
• They play a vital role in health of flap and post-
operative healing.
• They should be made over intact bone.
• They should lie at least 6-8 mm beyond the
anticipated bony defect so that it lies on sound bone.
If incision lies over bony defect—it will tend to collapse
into the defect and result in wound dehiscence and
delayed healing.
F i g u r e 7 . 1 1 : Triangular flap
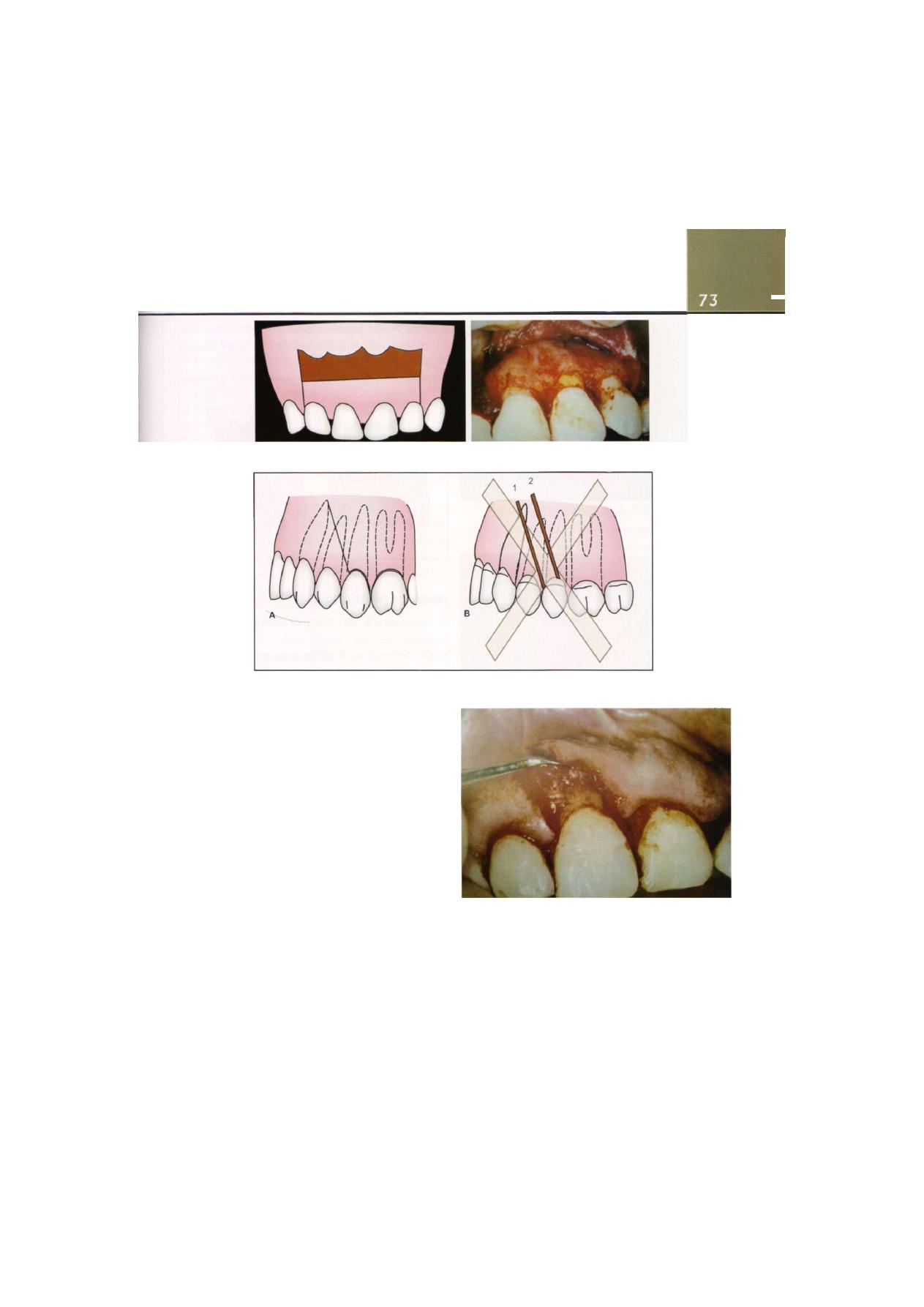
Transalveolar Extraction (Complicated Exodontia)
F i g u r e 7.12: Four cornered flap
F i g u r e 7.13: Mesiobuccal or distobuccal line angle of tooth
Firm pressure should be applied while placing
incisions.
Periosteum should be incised simultaneously.
A single stroke, without breaking continuity, must be
used to avoid ragged borders. Avoiding ragged
borders affects healing. Smooth borders lead to
primary healing, ragged lead to secondary healing
and scarring.
Blade should be changed if more than one flap is
to be raised because there is blunting of the blade
on contact with the periosteum and bone. Hence,
for clean incisions, while raising a second flap, one
should change the blade.
Reflection of flap begins at papilla with sharp end
of elevator.
Then broad end is used, it is inserted at middle corner
of flap.
F i g u r e 7.14A: Reflection of mucoperiosteal flap
Dissection is carried out with pushing stroke
posteriorly and apically.
This facilitates easy, rapid and atraumatic reflection
of mucoperiosteum.
\

\
Exodontia Practice
F i g u r e 7.14B: Lower anterior region with flap reflection
F i g u r e 7.14C: Palatal flap reflection
PREVENTION OF FLAP NECROSIS (BLOOD SUPPLY OF FLAP!
(FIGURE 7.151
1. Flap should be wider at base than apex to provide
unimpeded blood supply to all parts of the flap
Necessary to avoid ischemic necrosis of flap and
dehiscence (Figure 7.15).
2. Releasing incisions should converge at free end.
3. Length should not be more than the width. In
maxillofacial surgery, length of the flap is usually half
the breadth.
4. Base should not be excessively twisted/stretched,
grasped with sharp instruments that might damage
the blood supply of flap.
F i g u r e 7.15: Base at flap broader than open
PREVENTION OF FLAP DEHISCENCE
• Approximate flap margins over sound, healthy
bone.
• Gentle handling of tissues is necessary to maintain
the vitality of the tissues.
• Tensionless suturing to prevent necrosis of the flap
margins and dehiscence___
• Dehiscence causes bone exposure which causes
severe pain, bone loss and increased scarring
AVOID VITAL STRUCTURES
• Mental nerve: In premolar region use envelope flap
as far as possible. As flap is reflected care should be
taken until mental foramen is found. Gentle use of
periosteal elevator will preserve mental nerve in its
conical sleeve of periosteum. In edentulous arch with
ridge resorption- mental foramen will be close to the
ridge crest.
• Lingual nerve comes in mandibular 3rd molar
surgeries. A lingual flap if raised should be subperio-
steal as the nerve lies in the supraperiostael plane.
• Facial artery: releasing incisions at lower 1st molar
site should be curved at its lower edge to avoid the
facial artery.

Transalveolar Extraction (Complicated Exodontia)
7
• Greater palatine vessels: damage to these vessels is
avoided by avoiding a palatine flap. Controlling
bleeding from greater palatine artery is very difficult.
• If anterior palatine flap is raised, nasopalatine nerves
and vessels can be easily incised at the level of the
foramen. Bleeding can be controlled easily. In
addition nerve can regenerate quickly and the
temporary numbness does not bother the patient.
CLOSURE
• Achieves approximation of flap margins.
• Accurate apposition of flap—primary healing.
• Tensionless sutures: If sutures are tight they might cut
through or compromise blood supply causing necrosis
and dehiscence of flap.
• Suture tightness judged by avoiding tissue blanching
but knot should be tight.
Functions of Sutures
1. Coapt wound margins: If space between margins is
less, primary healing will result which will be rapid
and complete.
2. Hemostasis: Sutures play a role in hemostasis in
oozing socket but not in case of profuse bleeding.
Profuse bleed—chances of hematoma due to conti-
nuity of bleeding in underlying tissues. In Oozing
socket, bleed is controlled due to tamponade.
However, sutures should not be tight.
3. Holding soft tissue flap over bone. Bone that is bare
is very painful. It becomes non-vital and requires
longer time to heal.
ADVANTAGES OF LONG FLAPS
• Adequate visualization.
• Healing by first intention- rest on sound bone.
• Flaps not to overextend in vertical direction to avoid
vital structures.
AVOIDING BUTTON HOLED FLAPS
• In chronic sinus cases sometimes need to include sinus
in the tissue flap to avoid button holing of the flap.
BONE REMOVAL
• "Bone belongs to the patient and tooth to the
surgeon"
• Unnecessary bone removal must be avoided
• Bone removal is divided into removal before tooth
delivery and bone removal after tooth delivery.
• Bone removal before tooth delivery.
1. Removal of buccal cortical plate (l/3rd of retained
root surface to be exposed): Before delivery.
Buccal bone removal done for adequate visuali-
zation of tooth root. It improves access and brings
root in full view which can be removed by hand
instruments or rotory instruments. Rotory
instruments are preferred because hand instru-
ments chisel and mallet may strike root and
fracture root with bone at same level and there
is need for more bone removal. Also the sensation
is unacceptable under local anaesthesia. With bur
avoid cutting into root. Round burs are preferred
over straight fissure for bone removal because
cooling is easier and faster and visualization is
good.
2. Guttering of buccal bone: In this trough created bet-
ween bone and tooth on buccal and/or mesial or
distal aspect and height of alveolus is maintained.
3. Postage stamp method: Buccal cortical bone is
removed upto l/3rd height of root. This technique
is also used for retained apical l/3rd of root (Figure
7.16).
F i g u r e 7.16: Bone removal: Postage stamp method
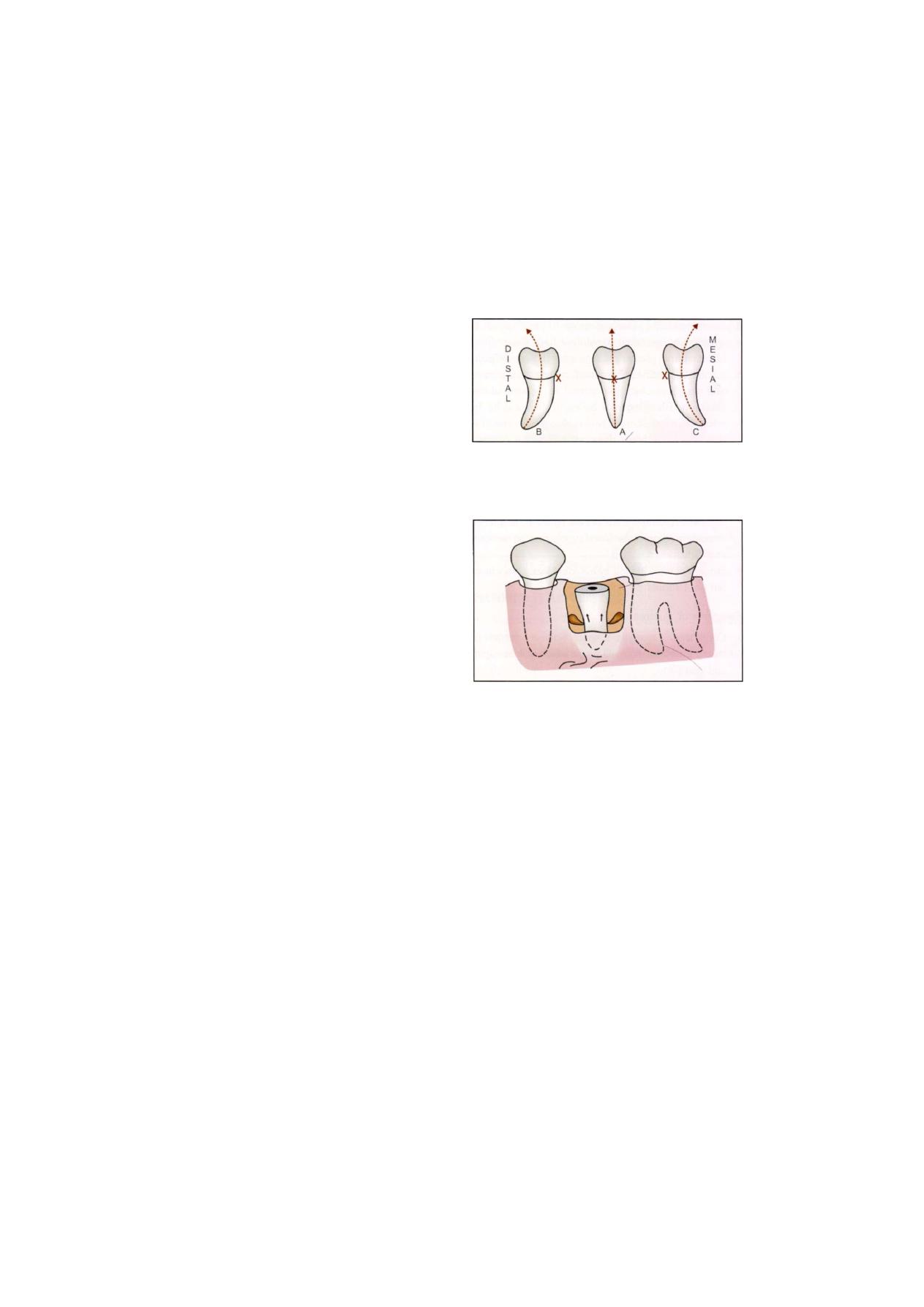
76
Exodontia Practice
• Use of coupland chisel for bone removal can be done
under local anesthesia because it involves use of hand
pressure for bone cutting.
• Use of chisel and mallet can be done under general
anesthesia.
• Two vertical cuts, one anterior and one posterior
and one horizontal cut connecting both the vertical
cuts.
• Bevel of chisel should face bone that is to be cut—
faces mesially for distal cut and vice versa and
occlusally for horizontal cut.
• Bone removal after tooth delivery is performed to
achieve the following:
1. To smoothen sharp bone margins.
2. Reduce size of clot by reducing size of socket.
3. Recontour the residual alveolar ridge for prosthetic
rehabilitation.
TOOTH SECTIONING
• Also known as odontectomy. Fragments can be
removed easily one by one, we can section crown
from root, separate cusps, separate roots or perform
a combination.
Advantages:
1. Individual sections with different paths of with-
drawal can be removed easily.
2. Splitting of roots better with burs because of
definite control over splitting, although it is more
time consuming.
3. Creation of space by bur: If space is not created
between divergent roots they will still impact
against each other on elevation.
APPLICATION OF ELEVATORS
• "GIVE ME A LEVER AND A SECURE FULCRUM
AND I WILL MOVE THE WORLD"
• It will depend on configuration of root and direction
in which it must be moved for its delivery (Figure
7.17).
F i g u r e 7.17: Diagrammatic representation showing correct
method of application of elevator in curved root
• Straight roots can be elevated from any side (Figure
7.18)
F i g u r e 7.18: Diagrammatic representation of application
of elevator in straight root
• In curved roots elevator to be applied on convex side.
If applied on concave side root will get forced against
bone- further fracture of root (Figure 7.19).
In multirooted tooth with roots curved in same
direction, elevator applied on convex aspect of whole
root complex.
Multirooted teeth with roots having conflicting lines
of withdrawal:
1. Divergent
I
recurved root pattern: Roots should be
separated before application of elevator to convex
surface of each. Occasionally elevator can be applied
to unfavorable surface in case of infected root /
resilient bone / bone loss without fracture of root and
if space has been created between the two roots
(Figure 7.20).
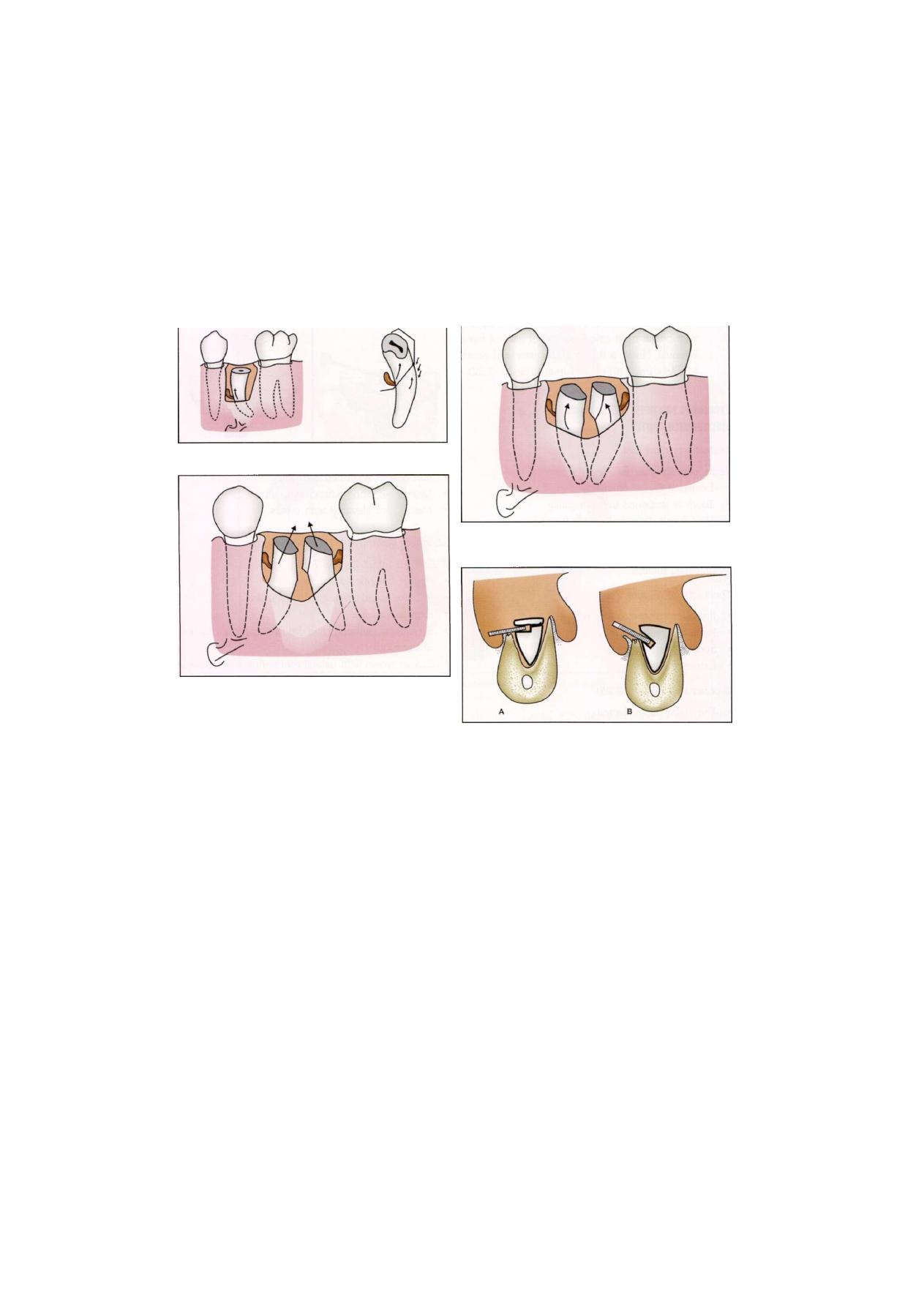
Transalveolar Extraction (Complicated Exodontia)
F i g u r e 7.19: Application of elevator on greater curvature
of root
F i g u r e 7.20: Root sectioning and removal of root
2. Convergent root
I
cprved roots: elevator is applied
to convex surface (Figure 7.21)
• Elevators should be applied with modest and
controlled force.
• Sometimes it is essential to make more secure place
for application of elevators. This is done by drilling
notch in side of root which is more apically at its
depth. This will resist root fracture when elevation
is attempted. Round bur is used at an angle of 45
degrees to long axis of tooth (Figure 7.22).
/
TECHNIQUE FOR OPEN EXTRACTION OF SINGLE ROOTED TOOTH
1. Provide adequate visualization and access by raising
a flap.
2. Determine need for bone removal
• Reset extraction forceps under direct visua-
lization—extract.
F i g u r e 7 . 2 1 : Root sectioning and application of elevator
in curved roots
F i g u r e 7.22: Preparation of purchase point
• Grasp a bit of buccal/Ungual bone: Iimprove
mechanical advantage—grasp tooth root. Small
amount of buccal/lingual bone is removed. This
is alveolar purchase technique.
• Use straight elevator in a shoehorn pattern forcing
it down the periodontal ligament space with a
wiggling motion to expand the periodontal
ligament space and allow small straight elevator
to enter as a wedge and displace root occlusally.
• Proceed with bone removal over area of the
tooth. Bone removal in mesiodistal direction same
as width of tooth and in vertical direction. Then
extract with elevator or forceps. Heavy elevator
'crane pick' can be used.
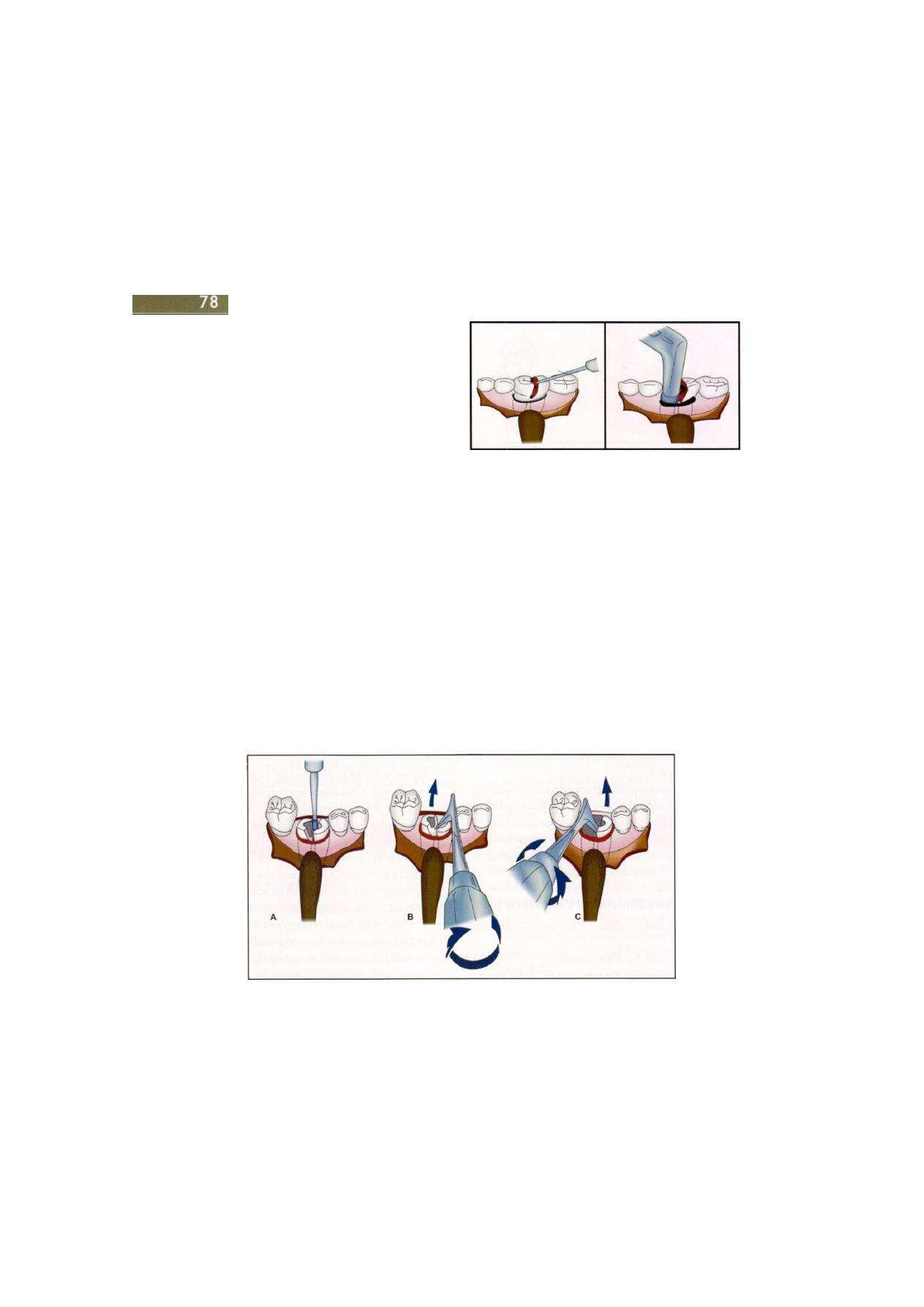
Exodontia Practice
• If still difficult to elevate, prepare a purchase point
with bur at most apical portion of area of bone
removal. Notch is 3 mm in diameter and depth
to allow insertion of instrument (Figure 7.22).
TECHNIQUE FOR OPEN EXTRACTION OF
MULTIROOTED TOOTH
Mandibular First Molar
Technique
l
(Figure
7.23)
• Envelope flap is reflected.
• Tooth is sectioned buccolingually.
• Mesial and distal halves are formed.
• Sectioned tooth is treated as two single rooted teeth.
• Luxated with straight elevators and extracted with
universal forceps.
Technique 2 (Figure 7.24)
• If crown lost previously; reflect flap.
• Remove crestal bone.
• Section the two roots.
• Extract individually.
Technique 3 (Figure 7.25)
• Triangular flap reflected.
• Sufficient buccal bone removed to expose bifurcation.
F i g u r e 7.23: Vertical split of crown and its removal
• Mesial root sectioned with burs.
• Distal root along with crown extracted.
• Mesial root elevated with cryers.
Maxillary Molars with Divergent Roots
If crown is intact (Figure 7.26):
• Reflect mucoperiosteal flap.
• Remove small amount of crestal bone.
• Expose furcation.
• Separate mesiobuccal and distobuccal roots from rest
of the tooth.
• Extract crown with palatal root with bucco-occlusal
pressure.
• Palatal root with crown are delivered along long axis
of palatal root.
• Avoid palatal force to prevent palatal root fracture.
F i g u r e 7.24: Sectioning of mesial and distal roots and its removal

Transalveolar Extraction (Complicated Exodontia)
F i g u r e 7.25: Another method of sectioning and removal of tooth
• Elevate buccal roots one by one using straight / cryer
elevator. Avoid too much apical force to avoid sinus
perforation. Apply maximum force mesiodistally.
Crown is missing/fractured
• Divide the three roots.
• Extract them individually.
• First extract buccal roots, then extract palatal root.
SOCKET TOILET
• Removal of tooth/root does not complete the
procedure.
• Progress of healing and after-pain depends on socket
toilet.
• Irrigate with copious amounts of normal saline in the
socket and apical portion of flap where it joins bone
because it is a common place for debris collection.
If not irrigated may delay healing or cause sub-
periosteal abscess.
• Remove infected granulation tissue using a curette.
SUTURING
Incisions are closed and the tissues held in contact with
one another to permit healing by first intention by the
use of sutures. Hemostasis should be secured always
before the wound is closed. While the act of suturing
the wound will arrest a slight ooze from the surfaces which
the stitches bring together this cannot be relied upon.
If bleeding continues after the wound has been closed
a hematoma will form. This may either take the form
of a clot which creates a dead space in the tissues.
Hematomas increase the volume of the tissues, expand
flaps from the underside impairing their blood supply
and creating tension at the suture line. The tissues within
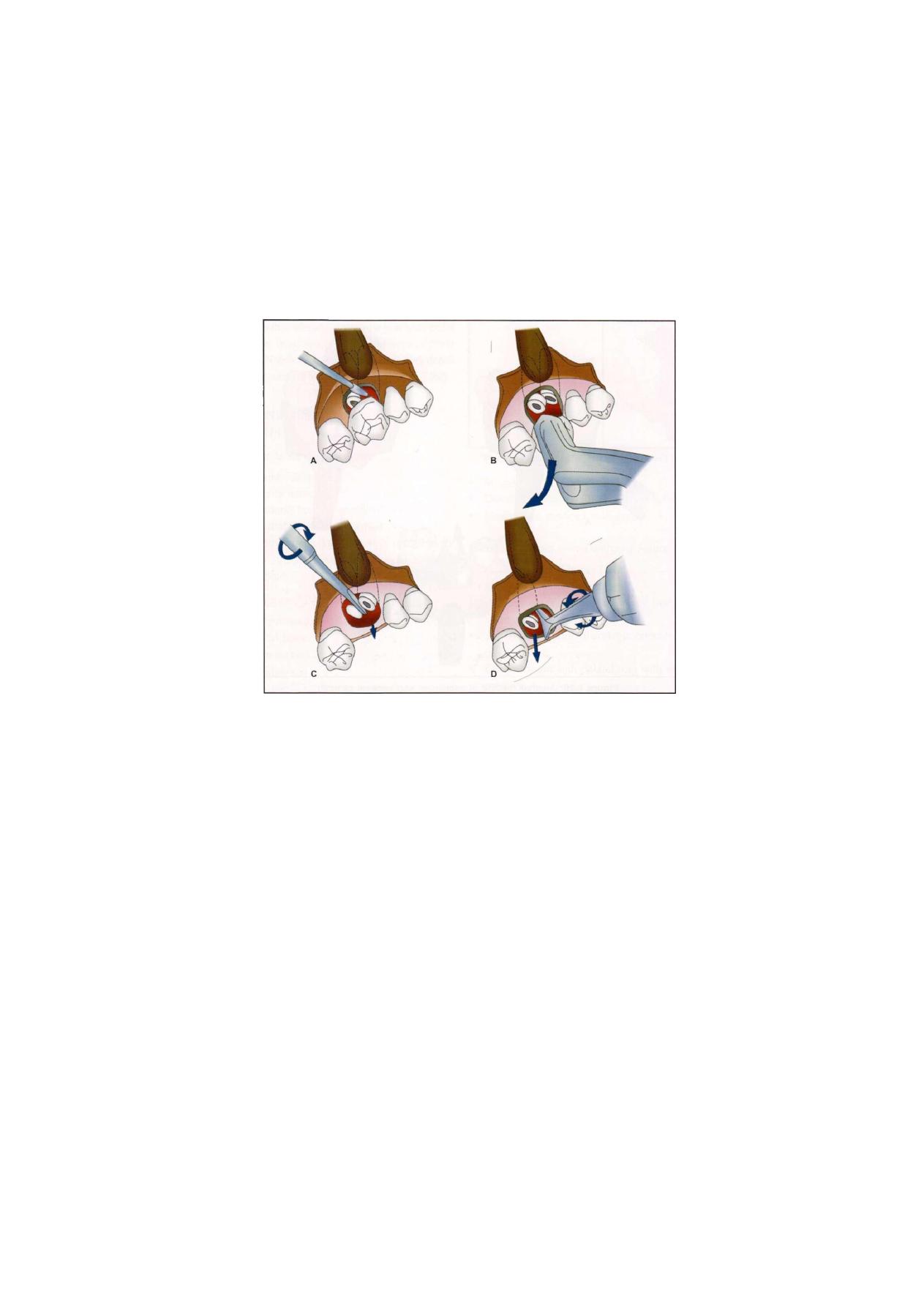
Exodontia Practice
F i g u r e 7.26: Method of sectioning and removal of maxillary molar
the bite of the sutures are also excessively compressed
and necrose so that the suture cuts out and the wound
opens, the so-called 'burst' suture line. Secondary
infection will follow. Hemostasis therefore must precede
wound closure.
The cheapest sutures are undoubtedly those made
from eyed needles and a suitable length of suture material
cut from a reel. However, most suture materials and
needles are difficult to sterilize, The needles are also
difficult to clean after use and become blunt and work
hardened so that they snap.
Modern sutures are prepared commercially and
sterilized by gamma radiation. The needles are eyeless,
with the end shaped as a tube into which the suture thread
is swaged. These 'atraumatic' sutures pass through the
tissues with minimal effort and damage.
Needles may be either round bodied or cutting.
Cutting needles are flattened on two or more aspects
behind the needle point to raise sharp edges which aid
penetration of tough tissues. Round-bodied needles dilate
a hole for the thread so that delicate tissues are less likely
to tear and the stitches cut out. The thread also fits tightly
in the hole to make a water-tight suture line. Large
needles may be handheld, but small needles such as are
required for suturing in the mouth are held in needle
holders. There should be a portion of the needle shank
which has flattened surfaces which may be held by the
needle holder and which prevent the gripped needle from
rotating. It is a fault of some modern needles that this
necessary flattening of the surface may not be present.
Needles are also either straight or have varying
degrees of curvature. Suturing in a limited space is

Transalveolar Extraction (Complicated Exodontia)
facilitated by a curved needle so that the point can be
readily seen and grasped after rotating it through the
tissues. A half circle needle is usually chosen. These are
22 and 25 mm in length measured around the curve,
and are well suited to relatively thin layers of tissue and
the small 'bites' required to close them. Suture material
of 2 metric (3/0) silk or polyglycolate is usually used
in the mouth.
The sutures may be either absorbable or non-
absorbable and monofilament or braided. The
traditional absorbable suture material is catgut and
despite the appearance of new synthetic materials it is
still widely used. Catgut is prepared from the collagenous
adventitia of lambs intestines and is prepared either plain
and simply stranded, twisted and sterilized with gamma
irradiation or treated with chromate, i.e. chromic gut.
to increase its tensile strength and delay absorption.
However, synthetic polymers the polyglycolate and the
polyglactin suture materials, are stronger and less irritant
to the tissues. Unfortunately if uncoated these sutures
may be difficult to knot securely and will spontaneously
untie unless the surgeon is familiar with their behavior.
Polyglactin sutures are coated with polyglactin 370
and calcium stearate (Vicryl-Ethicon) which reduces
drag.
In general, non-resorbable materials creates little
tissue reaction but because they are not destroyed by
the tissues are only used where they can be removed
or buried deeply in situations where permanent support
from the sutures is required and where subsequent
infection of the foreign material is unlikely. They may
be either monofilament or braided. Braided materials
are generally more flexible and are easy to knot and
so are more suitable for suturing the mucous membrane
of the mouth. Natural fibers, such as silk, with their slightly
roughened surfaces hold knots better than smooth
surfaced artificial fibers. However, a braided thread will
act as a wick for moisture and accumulate debris and
microorganisms which can irritate the wound. To prevent
this, braided sutures are often coated and made water
repellent with wax or silicone.
Monofilament synthetic polyesters such as poly-
propylene or polyamide (nylon) will not absorb and
conduct liquids in this way but are more difficult to knot
as they have an intrinsic springiness. Therefore only
4-0 or finer gauge monofilaments are used in the mouth.
As elsewhere in the body, catgut or other absorbable
material is used for buried sutures although these are
not often required during operations performed through
the mouth. Absorbable sutures are also used for mucosal
flap closure when operating on young children to avoid
the need for suture removal, or in all age groups for
suturing the inside of lips and cheek or the floor of mouth
where postoperative oedema may make the sutures cut
in to a degree that they are difficult to remove. Sizes
3/0 (3 metric) to 6/0 (6 metric) of catgut are chosen,
dependent upon the tissues to be sewn.
Needle holders with narrow beaks are required to
hold small, curved needles without flattening their
curvature. The handles should be sufficiently long that
the holding fingers do not obstruct the surgeon's view.
Modern eyeless needles are difficult to hold without
a ratchet type needle holder and this can be a dis-
advantage in awkward corners of the mouth.
However, they are less highly tempered than the eyed
needles and much less likely to snap if accidently bent.
The needle holder is clamped on to the needle at a
position about two-thirds of the distance from its tip. If
the needle is held correctly in this manner the length
between the jaws of the needle holder and the point
is sufficient to allow the needle to be inserted about
2-3 mm from the wound edge, and rotated through the
tissues so that enough of the pointed end emerges from
the wound to be gripped and drawn through. The flap
is controlled with either toothed dissecting forceps or a
skin hook and the edge everted as the needle is passed.
The needle point enters at right angles to the surface
and it should penetrate completely through a muco-
periosteal flap to obtain the maximum grip, but emerge
near the bottom of the soft tissue incision ensure that
there is no dead space,'left after it has been tied. Eversion
of the first side of the flap enables the curved needle

Exodontia Practice
to travel through the tissue obliquely away from the
incision to enclose a slightly larger bite on the deep aspect
than at the surface.
In general the needle should be drawn out of the
first side of the wound before the point is engaged in
the other. Now the second side is everted with toothed
forceps or a skin hook and the needle inserted from the
underside of the flap. The needle is inserted into this
side of the wound at the same depth that the thread
emerges from the first side. Now, once the needle
has penetrated into the second side the forceps or skin
hook is detached from the edge of the flap and pressed
against the surface of the tissues just beyond the hidden
point of the needle. This action pulls the superficial tissues
over the point so that the needle emerges closer to the
wound edge than it would otherwise. This way again
the needle embraces a greater width of tissue deeper
in.
Now when the stitch is tied the wound edges are
everted slightly. Eversion of the wound edges increase
the area of contact and so improves the early strength
of the healing wound. As the scar contracts a flat surface
results. The distance of the needle punctures from the
edge of the flap should be less than the depth to which
the stitch penetrates into the tissues, particularly with
mucoperiosteal flaps or one edge will overlap the other
as the knot is tied. Overlapping will also result if unequal
depths of flap are embraced by the stitch. Excessive depth
of bite in relation to width, on the other hand. Results
in excessive eversion and gaping of the approximated
wound at the surface.
In the mouth, one side of the wound often constitutes
the flap and has been freely elevated from the bone and
the other side remains attached to the bone almost up
to the incision. The edges of the fixed margin, however,
will have been raised for a sufficient distance to permit
penetration of the full thickness of the flap by the needle.
Suturing from loose to fixed flap usually enables finer
repositioning and reduces the chance of the suture tearing
through the fixed thin tissue layers. However, comfortable
suturing is important to good technique and to this end
it is preferable, where appropriate, to sew from the edge
further from the operator to the nearer one.
A knot is now tied, either by hand or with instruments.
If the knots are tied by hand more thread is wasted than
when instrument tying is employed, particularly where
the knots have to be formed towards the back of the
mouth. The technique of instrument tying therefore will
be described. Furthermore, it is easier to see what is
happening if instruments are used in the confined space
of the mouth.
The needle is drawn out of the second side of the
wound and the thread pulled through until a length of
about 4 cm remains protruding from the entry puncture.
The needle is taken from the needle holder with the index
finger and thumb of the left hand. The excess suture is
taken up into the palm of the left hand, using third and
fourth fingers and the thread grasped again with finger
and thumb about 8 cm from the wound. The beaks of
the needle holder are brought across the front of the
thread and rotated in a circle to pick up two loops of
the thread. The short end is now gripped at its end with
the needle holder and the loops slide off the beaks onto
the thread by rotating the needle holders so that the beaks
point towards the left and by drawing on the long end
with the left hand. The short end is given a short
downwards jerk which tumbles the loops into a slip knot,
which is positioned just beyond the tips of the beaks and
with the short length emerging from under the loops.
By drawing on the long thread the knot may be made
to slide down onto the tissues at the exit puncture. The
short end should not be pulled as if this is done an
unstable knot will result. Tension upon the long end also
results in a short end which needs minimum trimming
subsequently. The short end will emerge between the
loops and the tissues and the knot will not slip while
the long end only is under tension. As this first knot is
tightened the left hand moves away from the operator's
body and across the wound.
To form the second throw of the knot the needle
holder beaks are brought across the long thread from
behind and the points rotated downwards, away and

Transalveolar Extraction (Complicated Exodontia)
83
to the right to pick up a single loop. The short end is
again clamped but should not be pulled upon. The loop
is drawn off the needle holder beaks and the knot
tightened by traction upon the long end only with the
left hand. Final tightening is accomplished by drawing
the long thread towards the operator and the short end
away, across the wound. A third throw will prevent any
chance of a knot slipping, particularly if a synthetic suture
is being tied, or of the knot untying as it absorbs moisture
from the saliva in the case of catgut. The loop is formed
as for the first throw, but only one loop is picked up.
The left hand travels away from the operator and across
the wound to tighten the knot. The thread ends are held
up and cut off by the assistant.
It is essential to close a wound with the correct suture
tension, sufficient to keep the edges of the wound firmly
together, but no more. Slight edema of the soft tissue
margins can be anticipated postoperatively and
allowance must be made for this, particularly when
suturing the inside of the cheek or lips or the floor of
the mouth. If a suture is too tight it will cut into the tissues
and produce scars at right angles to the healed incision,
or stitch marks. Permanent suture scars depend more
upon the tension of the sutures than upon the length
of time before they are removed. To avoid irritation of
the healing wound the knot should be manipulated so
that it lies over the puncture point to one side of^the
wound. If an angled incision is used the apex between
the two edges is correctly positioned first. Then the next
two sutures are inserted at each mid-point between the
ends of the wound and the first suture. The remaining
sutures are interspaced at regular intervals.
Interrupted sutures are used for most oral surgical
procedures though where long incisions are to be
closed,continuous sutures are used. Where a continuous
suture has been inserted the thread is drawn after the
last penetration of the needle leaving a short loop on
the other side of the wound. The mid point of this loop
is grasped with the needle holder as the knot is tied,
instead of the usual short end.
Mattress sutures, which may be either horizontal or
vertical in design, embrace a greater volume of the tissue
which increases the grip upon the wound margin. In the
case of the former, the needle is introduced through one
wound edge and passed out through the other in the
usual manner. Then the needle is re-inserted about
3 mm further along the wound from the point of its
emergence, carried back through both wound edges and
tied. The vertical mattress suture is made by inserting
the needle 4-5 mm from the wound margin and through
the tissues in a deep bite. The needle is then re-introduced
close to the wound margin and taken through more
superficially in line with the previous direction of insertion,
but of course in the opposite direction. The suture is then
tied on the side of its original insertion. A vertical mattress
will coadapt the wound margins where there is a small
degree of tension and at the same time ensure eversion
of the wound edges.
Absorbable sutures can be inserted to close layers
below the skin surface, to ensure complete closure of
a wound in depth, to reconstitute sheets of muscle or
fascia and to eliminate potential dead spaces. The part
of the suture which will persist longer than the rest and
be likely to form a nidus for infection is the knot. If it
lies under the outer suture line the bulk may affect the
soundness of closure. For both these reasons the knot
should be buried on the deep aspect of the suture line.
The needle is inserted from the deep side of the layer
to be sutured and reinserted from above downwards
on the other side of the wound. When the knot is tied
it will slip through between the approximated tissues.
The removal of sutures should be performed with
care. They should be swabbed gently with chlorhexidine
then each knot gripped in turn with non-toothed forceps.
The external part of the suture is raised and the thread
cut below the knot and flush with its point of emergence.
In order to avoid a strain upon the healing wound the
suture is drawn out across the wound. This draws the
deep part of the suture out of the opposite puncture
creating tension towards the wound rather than away
from it. This prevents dehiscence of the healing wound
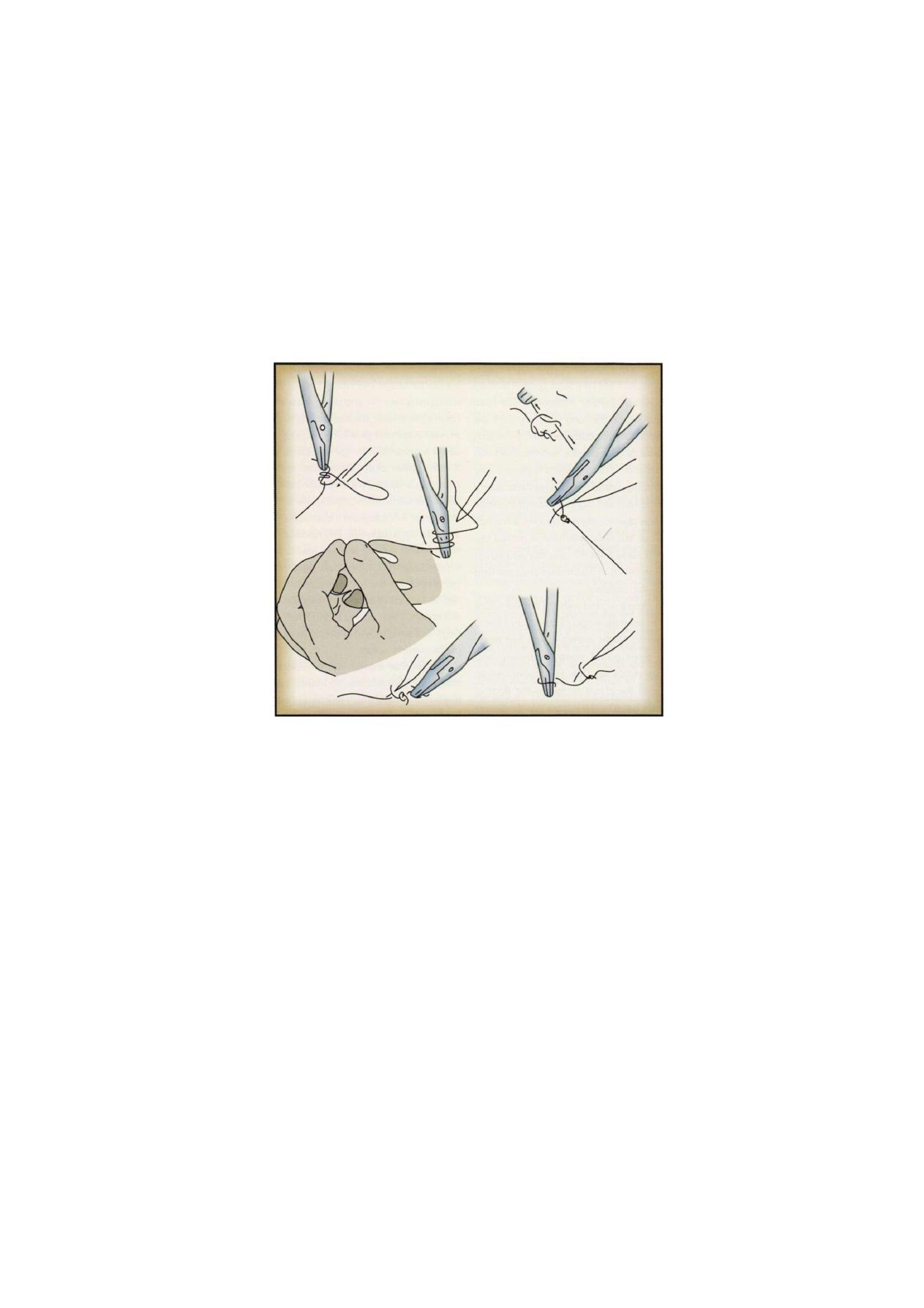
84
Exodontia Practice
F i g u r e s 7.27: Suturing techniques
and also draws only the previously buried part of the
stitch through the wound. Never cut through a stitch in
such a way that part of the contaminated external loop
is drawn through the wound. Above all, avoid cutting
the suture in two places so that part of the suture is left
in the tissues. As the suture is divided some compression
of the tissues is released and the retained segment retreats
into the depths of the tissue. Even if some micro-
organisms have travelled along the suture material they
do not produce a clinical infection in the ordinary way
because a suture creates a wound which is drained at
both ends. Leave a cut segment buried in the suture track
and allow the puncture points to close so that there is
no longer drainage and a stitch abscess will result.
Functions of sutures are:
1. Coapt wound margins.
2. Hemostasis—oozing socket but not in case of
profuse bleeding.
3. Holding soft tissue flap over bone.
4. Maintaining blood clot within socket—use of
gelfoam, oxidized cellulose.
If flaps are snugly in position and bleeding is
controlled, sutures are unnecessary.
AFTER CARE
• Maintenance of oral hygiene, especially at site of
sutures.
• Avoid accumulation of irritants, plaque and food
debris which will lead to infection and breakdown
of flap.
Chapt
2 J
The Root Piece
Removal
(The Fractured
Root)

86
Exodontia Practice
A decision must be made whether to leave or remove
a residual root. These requires anticipating whether the
root fragment will remain asymptomatic or whether it
will become infected and cause pain, perhaps lead to
an abscess and a discharging sinus, develop a cyst or
interfere with a denture. Occasionally mandibular roots
may even sink towards the lower border creating greater
problems in their removal.
If the root breaks after the tooth has become mobile
the missing piece should be recovered for it is almost
certain to become infected and cause pain. Conversely
when the apex of a tooth with a vital pulp snaps off before
the main body of the tooth has been loosened, the
fragment is likely to be enclosed by the bone of the
healing socket, and remain asymptomatic, and its
removal can be deferred if necessary. Perhaps the only
absolute indication for root removal is for patients for
whom unpredictable local infection may become major
risk such as those who have rheumatic or congenital heart
disease or who are immunosuppressed.
IMPORTANT FACTORS FOR CONSIDERATION
The following factors need to be determined before
decision to be made for removal of root piece.
THE AMOUNT OF ROOT RETAINED
When only apical 3rd or less of the root tip is retained
it may be left. More often the socket heals satisfactorily
and the root remains in the bone. However, sometimes,
as time passes, the alveolus resorbes and eventually the
root comes to the surface and may cause chronic
discomfort or an acute infective episode. Late removal
may be surgically easy, but may result in deficiency in
the edentulous alveolus. Generally, root tips should be
removed in patients below 50 years of age at the time
of fracture, while in older patients, their general condition
and the bone resorption rate should be considered.
THE SITE OF FRACTURED ROOT
i. Roots in the close proximity to anatomical spaces
such as maxillary sinus and inferior dental canal
should be left at the time of fracture and elective
surgical removal can be considered later.
ii. If the root is in close proximity to an adjacent tooth,
as in cases of displaced or dilacerated roots, and
causes damage to the adjacent healthy tooth, then
the root tip is better left alone.
iii. The palatal root of the maxillary 3rd molars,
particularly when the tooth is rotated, may be in
the position where access to it can only be achieved
by removal of the 2nd molar. Hence it is better
-to leave such a root piece.
REASONS FOR EXTRACTION
i. When a tooth is extracted for orthodontic purpose
no root should be left behind as it may prevent
movement of adjacent teeth into this space.
ii. When there is periapical radiolucency present, the
root as well as the periapical granuloma should be
removed, or else it may develop into a cyst.
Radiographic evaluation is mandatory.
AGE AND GENERAL MEDICAL CONDITION OF THE PATIENT
Very young, very elderly and certain nervous individuals
may tolerate extraction of the tooth under local anesthesia
but not the entire procedure of trans alveolar extraction.
It is rather wise to stop the operation and make other
arrangements for root removal than causing distress to
the patient.
CIRCUMSTANCES OF THE FRACTURE
If the tooth has been luxated before the fracture occurred,
the periodontal membrane may have been torn and any
blood supply to the root may have been cut off. Such
root then acts as a foreign body which may give rise
to a septic socket or chronic infection in the bone. Such
roots should therefore be removed.
TECHNIQUE FOR REMOVAL OF
SMALL ROOT TIPS
When the apical 3rd of the root fractures, initial
attempts should be made by the closed technique and

The Root Piece Removal (The Fractured Root)
87
if unsuccessful, then by open technique. Whatever
technique is chosen 3 basic requirements are of
importance -Excellent light for illumination of field, Good
suction for isolation of area and Good assistance.
THE CLOSED TECHNIQUE
It is a technique that does not require reflection of
mucoperiosteal flap and removal of bone. The technique
is most successful when the tooth has been well luxated
and mobile before the root tip fractured. However, if
the tooth was not well mobilised before fracture, closed
technique is less likely to be successful. It may not be
successful when the roots are hypercemented, dilacerated
or when there is a bony interference.
Forcep Removal
The narrow bladed forceps i.e. root forceps, are
invaluable for the removal of sizeable retained roots if
used with care as follows:
a. Always ensure that the blades are inserted beneath
the gingival which may have to be elevated locally
first.
b. Always obtain a grip on an identified root rather than
just grip the alveolus blindly.
c. Press the forceps well down over the root. In the
mandibular molar region a small amount of alveolar
bone may have to be included.
d. In the maxilla, apply the palatal forcep blade between
the palatal and one buccal root and the outer blade
buccal to the other buccal root where retained molar
roots are being tackled.
e. Apply a firm continuous force with a strong grip to
expand the alveolus, at the same time moving the
root only through a small arc while maintaining an
apically directed pressure. Rapid rocking movements
although popular are likely to fracture the roots.
f. This approach is likely to remove one mandibular
root or in the maxilla two roots, making the removal
of the remaining one easier.
After a root has been recovered, verify that the
removal is complete by fitting the tip to the previously
extracted portion of the tooth. If this precaution is
neglected, the surgeon may discover that he has failed
to retrieve the whole of a missing root. Indeed all teeth
should be inspected carefully after extraction because
some have an extra root and if this is fractured and
retained, its absence may be overlooked by a casual
glance at the tooth.
Endodontic files may help removal of root tips in
certain situations. After proper visualization of the root
canal is achieved, an endodontic file of an appropriate
size is selected and screwed into the root canal at the
fragment, until it firmly engages the root tip. The shank
of the file is gripped with the needle holder, which is
used as a lever to lift the root fragments from the socket.
If the file pulls out of the root canal, a larger size file
should be fitted into the canal and the technique
attempted again. The endodontic files are not useful for
removing root tips with non-visible canals, hypercemen-
ted roots, bony interferences and dilacerated roots that
prevent proper access to the root canal.
A technique that is similar in concept to the
endodontic file technique involves the use of the dental
drill with a small round bur to drill into the tooth root.
There may be sufficient friction between the bur and the
tooth to permit the root to be removed when the drill
is removed from the socket. This technique is more useful
for larger root fragments than for smaller root tips.
Root tips can also be removed with a straight elevator.
This technique is indicated more often for the removal
of larger root tips than for smaller root tips. Straight
elevator is forced into the periodontal ligament space,
where it acts like a wedge to deliver the tooth fragment
towards the occlusal plane. However care should be
taken to avoid strong apical pressure which may force
the root into the underlying tissues. This is more likely
to occur in maxillary premolar and molar area where
the tooth can be displaced into the maxillary sinus.
There are a number of other maneuvers which will
enable the operator to remove a fractured root without
resorting to a surgical procedure. However, too much
time should not be spent in this way and if success is

88
Exodontia Practice
not soon achieved the attempt should be abandoned
and a flap reflected.
In certain cases one complete root of a multirooted
tooth is fractured off and retained. With care it may be
possible to place a sharp pointed elevator in the empty
socket and rotate it to remove first the inter-radicular
septum and then the root. This is often a successful
method for removing lower molar roots but is less
successful in the maxilla. The distobuccal root from an
upper molar may be extracted in this way provided only
gentle pressure is used with an elevator inserted in the~
mesial socket. Unfortunately the mesial root is difficult
to remove through the distal socket, as the root curvature
is unfavorable for the application of an elevator from
the distal aspect. Mesiobuccal roots can be elevated by
introducing a Coupland chisel or straight Warwick James
elevator up the mesial periodontal membrane in order
to turn the root downwards and backwards.
Elevators should not be used to remove the palatal
root of an upper molar. The buccal wall of the socket
does not form a satisfactory fulcrum and can be crushed
by the elevating force. Furthermore there is always the
danger of forcing the root into the antrum. The palatal
root must be seen clearly, which usually implies the
removal of both the buccal roots and, if necessary,
some surrounding bone which can be done with a bur.
Then gentle dislocation with a narrow Coupland's chisel
or rotation with upper root forceps should deliver the
root.
Sometimes a root apex is heard to fracture after the
tooth has been loosened with forceps and it may be
possible to see the apex clearly with the aid of a sucker.
A probe or a thin root canal reamer or file can be
introduced into the root canal and the loose apex is
withdrawn with its aid.
So-called apical elevators are usually too thick to use
to dislodge the apical third of a tooth root from its socket,
but a stout, bi-angled spoon excavator may enter the
periodontal space and topple it out. However, the
movement will be a tilting one, pushing the sharp
fractured edge on the other side of the root against the
socket wall. This may be sufficient to prevent the operator
dislodging it out of the socket. A narrow groove cut
around the end of the root with a rose-head bur may
be sufficient to overcome this obstruction.
Used with discretion, these maneuvers can neatly
remove a number of small retained fragments but again
it must be emphasized that unless success is achieved
early, further attempts will prove frustrating and time
consuming. It is then much quicker to raise a flap, cut
away some buccal bone and tease out the fragment with
-a^fine elevator. Indeed if socket surgery is performed
without caution, it can lead to roots being forced into
the maxillary sinus or the inferior dental canal.
Where immediate simple measures have failed to
deliver a root, a formal surgical removal is essential. This
should not be undertaken without clinical reappraisal
and adequate radiographs to localize the root fragments
and identify the features which might explain the
problem.
THE OPEN TECHNIQUE
If the closed technique is unsuccessful, the surgeon should
attempt open technique. There are two main open
techniques for removing tooth tips.
1. A soft tissue flap is reflected with a periosteal elevator
and retracted with a right angled retractor. Bone is
then removed with a chisel or bur to expose the buccal
surface of the tooth root. The root is bucally delivered
with a straight elevator. The flap is repositioned and
sutured.
2. Open window technique (a modification of the open
technique without removal of the buccal plate). A
soft tissue flap is reflected in the usual fashion and
the apex area of the tooth fragment is located. A bur
is then use to remove the bone overlying the apex
of the tooth, exposing the root fragment. An
instrument is then inserted into the window, and the
root is displaced out of the socket. This approach
is especially indicated when the buccal crestal bone
must be left intact. An important example is the
removal of premolars root tips for orthodontic

89
The Root Piece Removal (The Fractured Root)
purposes, especially in adults.There should be no
hesitation to reflect a flap whenever this is necessary
to see the retained root clearly. It is also essential to
remove adequate bone to enable unimpeded
elevation of the fragment along the appropriate line
of withdrawal. This will avoid much frustration from
repeated premature attempts to dislodge the root.
In the edentulous jaw the incision is made along the
crest of the ridge or if adjacent teeth are standing, the
incision is made along their gingival margins. The flap
must be ample in length and vertical depth in order to
provide adequate access for surgical manipulations
without damage to the soft tissues.
BONE REMOVAL
What constitutes adequate bone removal can be learned
only by experience but, within reason, it is better to
remove rather too much bone than too little.
Bone is usually cut away from the buccal aspect of
a root because this not only improves the access but
brings the fragment into full view. The socket wall can
be removed either with a hand chisel or gouge, a mallet
and chisel, or a drill.
In general a bur in a dental drill is preferable to a
chisel or gouge for the removal of bone around a buried
root because if a hammer and chisel are used inexpertly
the edge of the chisel may strike the root it self and
fracture the root. Furthermore, most conscious patients
undergoing surgery under local anesthesia find the
sensation produced by a mallet and chisel objectionable.
When using a bur, care must be taken not to damage
the adjacent teeth or to cut into the root fragment itself
to a degree that fracture when elevation is attempted.
Burs are also used to separate divergent or curved
roots. A tapered fissure bur is best for this purpose.
Separation of roots with a bur may take longer time than
splitting them apart with an osteotome but is more
certain. If the roots are shattered by the splitting blow
their removal may be made more difficult. What is more
important is a space is created between the root ends
by the bur cut permitting curved or divergent roots to
move towards one another as they are elevated. If the
roots are split apart the split surfaces may still impact
against one another as elevation is attempted.
If the operation is performed under a general
anesthesia it may be convenient for the operator to use
chisels and a mallet instead of a hand piece and bur.
Two vertical cuts are made, one on either side or parallel
to the side of the root. For the more mesial cut the bevel
of the chisel should face distally and for the distal one-
mesially. This way the remaining bone edges are not
crushed. A third cut is made horizontally and joining the
other two cuts at a suitable distance from the socket
margin so as to expose at least a third of the length of
the retained root fragment. The cuts should just penetrate
the cortical bone and care should be taken not to damage
the adjacent teeth, nor should the chisel strike the root
as the third cut is made or it will be fractured. A curved
Warwick James elevator is inserted to lever the tooth
from the socket.
Alveolar bone may also be conserved during the
removal of small apical fragments. Instead of removing
the whole length of the lateral wall of the socket to reach
the root tip a window is cut in the bone overlying the
apical part of the socket and access gained to the root
in this way. It may be delivered laterally through the
opening or it can be dislodged into the socket and
retrieved from this aspect if it is a fresh socket.
THE APPLICATION OF AN ELEVATOR
The configuration of the root and direction in which it
must be moved for its delivery will determine the correct
site of application of the elevator. Roots may be straight
or curved and the only way to establish the shape of
a particular root is by radiography. The operator should
always try to identify the reason why the root fractured
during the original extraction. Was the impediment during
the original extraction of the tooth relieved by the fracture
leaving a readily removable root or does the obstruction
still exist.
Theoretically, an elevator can be applied to any side
of a straight root in order to apply the necessary

9
Exodontia Practice
dislocating force. However, if a root is curved the elevator
must engage its convex aspect. If it is applied incorrectly
to the concave side of the root it will not displace it from
the sockeTbut will produce a further fracture of the
fragment.
When dealing with multistoried teeth the roots of
which all curve in the same general direction, the elevator
may be applied to the convex aspect of the whole root
complex. However if the lines of withdrawal of the apices
conflict, because of a divergent or curved root pattern,
then the roots must be separated before applying an
elevator against the convex surface of each in turn.
Occasionally the application of an extraction force to
unfavorable roots in infected or resilient bone will result
in successful delivery without fracture, but in the vast
majority of cases, the unorthodox approach will lead
to further fragmentation or to crushing of the socket wall
and the formation of a dry socket. Even in the absence
of a suitable preoperative radiograph, an experienced
operator can often feel whether he is applying pressure
to the correct aspect of the root, for on sensing the
slightest resistance he will alter the position of the
instrument so that the edge of the blade engages a more
appropriate side of the root. Nevertheless, it is obviously
more satisfactory to avoid guesswork, and obtain the
relevant information about root pattern from a
radiograph. The elevating force should always be modest
and controlled as the application of excessive force will
result in further fractures of the tooth fragment or even
a fracture of the jaw. A fractured jaw is most likely to
occur during the removal of deeply embedded roots in
a thin mandible. There are times when, after adequate
surgical exposure of the socket, a systematic search for
the root tip proves abortive. Alternative possibilities for
its location should then be considered, namely
dislodgement into the soft tissues, deflection into the
antrum from upper posterior teeth, displacement into
the inferior dental canal or lingual pouch from lower
posterior teeth, loss into the mouth or on to the surgery
floor. Some patients refuse to have a retained root
removed. When this happens the issue should not be
pressed, but an entry should be made in the case notes
to this effect.
POLICY FOR LEAVING ROOT (TIP)
FRAGMENTS
When a root tip has fractured and the closed approach
of removal has been unsuccessful and the open approach
may be extensively traumatic, the surgeon may consider
leaving the root in place. As with any surgical approach,
the surgeon must balance the benefits of surgery against
the risks of surgery.
CONDITIONS FOR LEAVING ROOT TIPS IN THE SOCKET
Three conditions must exist for a tooth root to be left
in the alveolar process.
1. First the root fragment must be small, usually not more
than 4 or 5 mm in length.
2. The root must be deeply embedded in bone and not
superficial. This prevents subsequent bone resorption
from exposing the root and interfering with the
prosthesis that will be constructed over the edentulous
area.
3. The tooth involved must not be infected, and there
must be no radiolucency around the root apex.
The 3 risks involved on removal of root tips: The risk
is considered to be greater than the benefit if one of the
following conditions exists.
1. Removal will cause excessive destruction of the bony
tissue.
2. Removal of the root endangers the vital structures,
most commonly the inferior alveolar nerve, either at
the mental foramen area or along the course of the
canal. If surgical retrieval of a root may result in a
permanent or even a prolonged temporary anesthesia
of the inferior alveolar nerve, the surgeon should
seriously consider leaving the root tip in place.
3. Attempts at recovering the root tip can displace the
root into the tissue spaces or into the maxillary sinus.
The roots most often displaced into the maxillary sinus
are those of the maxillary molars.

The Root Piece Removal (The Fractured Root)
4. If the preoperative radiograph shows that the bone
is thin over the roots of the teeth and that the
separation between the teeth and the sinus is small,
the surgeon will choose to leave a small root fragment
rather than risks displacing it into the maxillary sinus.
Likewise, roots of the mandibular second and third
molars can be displaced into the submandibular space
during attempts to remove them.
ROOTS IN EDENTULOUS JAWS
• Difficult to judge the position of the root piece. There
are no teeth. Hence it is difficult to determine the
location without any guideline
• Insert a short needle in anesthetized gingiva and take
a radiograph just before the operation
• Better to retrieve the root fragment through outer
aspect of jaw, rather than alveolar crest to preserve
the alveolar height.
PROTOCOL WHEN LEAVING REHIND THE ROOTS
If the surgeon decides to leave a root tip in place, a strict-
protocol must be observed. The patient must be informed
that, in the surgeon's judgment, leaving the root in
position will do less harm than surgery. In addition,
radiographic documentation of the root tips presence
and position must be obtained and retained in the
patient's record. The fact that the patient was informed
of the decision to leave the root tip in position must be
recorded in the patient's record. Also the patient must
be recalled for several routine periodic follow-ups over
the year to trace the fate of this root. The patient should
be asked to contact the surgeon immediately if any
problems develop in the area of the retained root.
Chapter
Pediatric
Exodontia

94
Exodontia Practice
The general principles of exodontias remain the same
whether applied to adults or to children. However, in
the child we are dealing with a developing organism
in both its physical and its psychological aspects.
Techniques, therefore, must be modified to conform to
the needs of this growing patient. Some factors to be
considered in oral surgery for children as compared to
adults are:
1. The oral cavity is small and there is greater difficulty
in gaining access to the field of operation.
2. The jaws are in the process of growth and
development and the dentition is in a continuous state
of change, with the eruption and resorption of primary
teeth and eruption of permanent teeth taking place
simultaneously. Any interference with the growth
centers in the jaw or premature extraction of primary-
teeth may lead to malformations of the jaw, the
permanent teeth or both.
3. The bone structure of a child contains a higher
percentage of organic material, which makes it more
pliable than adult bone and not as likely to fracture.
LOCAL ANESTHESIA
It is unfortunate that many practitioners refer children
to the oral surgeon for extractions under general
anesthesia without first making an effort to perform the
extraction themselves under local anesthesia. The general
practitioner or pedodontist should instruct parents that
general anesthesia is the method of choice.
We have found that many children can be handled
under local anesthesia, provided that parents cooperate
and there are no other contraindications. The child should
be told in simple words what is going to be done. He
should never be told an untruth: a child can be
disappointed only once and his confidence is lost forever.
It is safer to tell the child that he will experience slight
discomfort like a scratch or mosquito bite than to promise
complete painlessness and not be able to abide by our
promise.
If a child complains of pain during an injection or
operation, believe him. reconsider the situation, reinject
if necessary, but never submit him to pain by force. A
great percentage of even the more difficult and frightened
children can be persuaded to take a local anesthetic. When
elective surgery is to be done, it is best to see the patient
at least once prior to the operation. This gives the operator
time to talk to the patient and presents an opportunity
to establish rapport. This visit will permit discussion of
the procedure with the child and parents. By taking time
to explain what needs to be done, the dentist can keep
apprehension and fear to a minimum.
PREPARATORY MEASURES
It is mandatory to obtain permission from a parent or
guardian of a child before any type of anesthesia, local
or general, is to be used. The consent should be in written
form and should include the type of anesthesia to be
used and the operation to be performed. In an
emergency, a telephone call will suffice, but it should be
confirmed by a written statement as soon as possible.
It is a safe precaution to note the number of the telephone
and the name of the person giving the oral consent on
the record of the patient, preferably in the presence of
an assistant who can act as a witness.
Children seem to tolerate local anesthetics better after
a moderate food intake, about two hours prior to the
operation. If it is felt that the child might require a general
anesthetic, the parents should be told not to give the child
food or fluids for at least six hours prior to the procedure.
Appointments for extraction should be made
whenever possible in the early morning when the child
is well rested. The office appointment should be scheduled
so that the child does not have to wait because he tends
to become restless.
The instruments on the tray should be covered
with a towel and out of sight of the patient. We have
found it best to place the instruments on a tray behind
the patient. A display of needles, knives, forceps
and other instruments upsets not only a child but any
patient. There is never a need to load syringes in front
of patients; to do so only loads to further fear and
apprehension.

95
Pediatric Exodontia
Premedication has proven invaluable and an operator
should not hesitate to use it. Immediately before the
operation, the child should be sent to empty the bladder
and bowels whether local or general anesthesia is used.
Clothing should be loosened and protected with a
gown or a protective apron. We prefer linen aprons, as
rubber or plastic coverings make patients perspire more
freely and this makes any patient, including a child, more
uncomfortable. Relatives and friends should be sent out
of the operating room unless it is felt that their presence
may be of benefit in handling the child. The child's position
should be adjusted for comfort and support and should
be slightly reclining.
ANESTHESIA TECHNIQUE
Some clinicians advise the use of topical anesthetics before
injection. It is difficult to determine how effective they
are. They certainly have a psychological value, but they
do not substitute for a good injection technique. If they
are used at all they should be used properly.
1. The mucous membrane should be dried to avoid
dilution of the topical anesthetic solution,
2. The topical anesthetic should be held in contact with
the surface for at least 2 minutes, allowing at least
another minute for it to act. One of the errors made
in the use of topical anesthetics is the operator's
failure to permit sufficient time for the topical agent
to produce any effect before he injects. It is wise
to wait at least four minutes after the topical
anesthetic is applied before starting the injection.
3. A topical anesthetic should be selected which does
not cause local necrosis at the site of application.
No irritation has been found from the use of
Xylocaine (lidocaine) ointment.
4. A sharp, fine needle with a relatively short bevel
should be used, attached to a smoothly working
syringe. We feel disposable needles should be used,
for they assure both sharpness and sterility. Their
use eliminates the possibility of transferring infection
from one patient to another by means of a
contaminated needle.
5. The tissues should be stretched if loose, as they are
in the mucobuccal fold: they should be compressed
if densely attached, as they are on the hard palate.
The use of tension and pressure helps produce a
certain degree of anesthesia and thus lessens the
pain associated with the introduction of the needle.
If the tissue is loose, we prefer to pull the tissue over
the needle as we are advancing it.
6. When using an infiltration technique the anesthetic
solution should be deposited slowly. Rapid injection
tends to accentuate the pain. If more than one tooth
in the maxilla has to be anesthetized, the operator
can enter the initially anesthetized area and. by
changing the direction of the needle to a more
horizontal position, can gradually advance the
needle and deposit the anesthetic solution. The
palatal side may be anesthetized by injecting a few
drops anterior to the greater palatine foramen,
which can be found on a line connecting the last
erupted upper molars. When anesthesia is necessary
in the incisal region of the maxilla we have found
it best to give the anesthetic on the labial and then
pass the needle from this anesthetized area through
the interdental papilla between the centrals and
gradually deposit the anesthetic solution as the
needle is advanced. This technique seems to
produce less pain than if the needle is inserted in
or around the incisive papilla.
7. The vasoconstrictor should be kept at the lowest
possible concentration e.g.. with 2 per cent
Xylocaine, not more than 1:100,000 epinephrine
should be used.
8. The symptoms of anesthesia should now be
explained to the child. Numbness, tingling, a feeling
of swelling may otherwise frighten a child who has
not been forewarned.
9. Enough time (5 minutes) should be allowed to lapse
before any operation is started. If tingling and
numbness in the lower lip do not occur in 5 minutes
following an inferior dental block, the injection
should be considered a failure and repeated.

96
Exodontia Practice
10. Aspirating syringes should be used to prevent
intravascular injection of the anesthetic solution to
keep toxic, allergic and hypersensitivity reactions at
a minimum.
TYPES AND LOCATION OF INJECTION
In anesthetizing the maxillary primary molars or
permanent premolars, the needle should penetrate the
mucobuccal fold and be inserted to a depth that
approximates that of the apices of the buccal roots of
the teeth. The solution should be deposited adjacent to
the bone. The maxillary permanent molars may be
anesthetized with a posterior superior alveolar nerve block
or by local infiltration.
Labial infiltration commonly is used to anesthetize the
primary anterior teeth. The needle is inserted in the
mucobuccal fold to a depth that approximates that of
the apices of the buccal roots of the teeth. Rapid deposition
of the solution in this area is conrraindicated because it
produces discomfort during rapid expansion of the tissue.
The innervation of the anterior teeth may arise from the
opposite side of the midline. Thus, it may be necessary
of deposit some solution adjacent to the apex of the
contralateral central incisor.
The infraorbital block injection is an excellent technique
that may be used in place of local infiltration of the anterior
teeth. All ipsilateral anterior maxillary teeth are
anesthetized by this block. The needle is inserted
anywhere in the mucobuccal fold from the lateral incisor
to the first primary molar and is advanced next to bone
to a depth that approximates the infraorbital foramen.
The foramen is readily palpated as a notch on the
infraorbital rim of the bony orbit. The solution is deposited
slowly.
The tissues of the hard palate are innervated by the
anterior palatine and nasal palatine nerves. Surgical
procedures involving palatal tissues usually require a nasal
palatine nerve block or anterior palatine anesthesia. These
nerve blocks are painful, and care should be taken to
prepare the child adequately. These injections are not
usually required for normal restorative procedures. If it
is anticipated that the rubber dam clamp will impinge
on the palatal tissue, however, a drop of anesthetic
solution should be deposited into the marginal tissue adja-
cent to the lingual aspect of the tooth. A blanching of
the tissue will be observed.
MANDIBULAR TOOTH ANESTHESIA
The inferior alveolar nerve innervates the mandibular
primary and permanent teeth. This nerve enters the
mandibular foramen on the lingual aspect of the mandible.
The position of the foramen changes by remodeling more
superiorly from the occlusal plane as the child matures
into adulthood. The foramen is at or slightly above the
occlusal plane during the period of the primary dentition.
In adults, it averages 7 mm above the occlusal plane.
The foramen is approximately midway between the
anterior and posterior borders of the ramus of the
mandible.
For the inferior alveolar nerve block, the child is
requested to open his or her mouth as wide as possible.
Mouth props may aid in maintaining this position for the
child. The ball of the thumb is positioned on the coronoid
notch of the anterior border of the ramus, and the fingers
are placed on the posterior border of the ramus. The
needle is inserted between the internal oblique ridge and
the pterygomandibular raphe. The barrel of the syringe
overlies the two primary mandibular molars on the
opposite side of the arch and parallels the occlusal plane.
The needle is advanced until it contacts bone, aspiration
is completed, and the solution is deposited slowly.
Occasionally, the inferior alveolar nerve block is not
successful. A second try may be attempted: however, the
needle should be inserted at a level higher than that of
the first injection. Care must be taken to prevent an
overdose of anesthetic.
The long buccal nerve supplies the molar buccal
gingiva and may provide accessory innervation to the
teeth. It should be anesthetized along with the inferior
alveolar block. A small quantity of solution is deposited
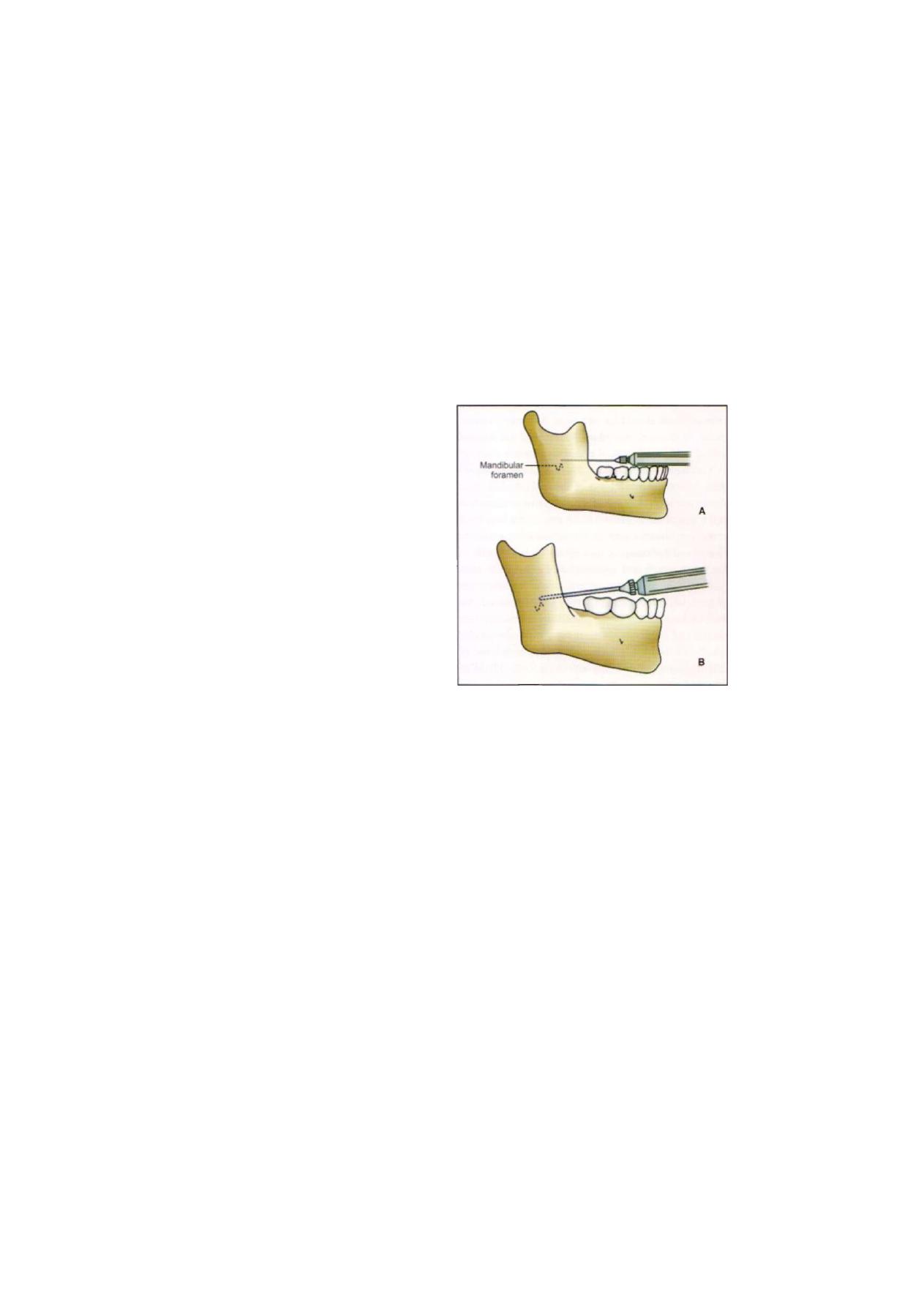
Pediatric Exodontia
97
in the mucobuccal fold at a point distal and buccal to
the most posterior molar.
Local anesthesia in children does not differ to a great
extent from that in adults. The lesser density of bone
hastens the diffusion of the local anesthetic through the
compact layers of the bone. On the other hand, the
smaller size of the jaws reduces the depth to which the
needle has to penetrate in certain block anesthesia. One
will find that, with the exception of the inferior dental
block, no other blocks are necessary in children.
The bone density is such, especially in the region
of the tuberosity that anesthetic solutions easily pass
through the cortex without the dentist having to a deeper
injection. Deep injections in this area may be followed
by a hematoma due to injury of the adjacent pterygoid
plexus, or. what is more likely, an injury of the posterior
superior alveolar artery or of its external gingival branch,
which runs downward and forward along the postero-
lateral wall of the maxilla close to the periosteum. This
is an unpleasant accident but it cannot always be avoided.
A hematoma, once noticed, can be controlled by packing
tightly compressed sponges behind and lateral to the
tuberosity intra-orally while applying pressure from the
outside against this pack with ice-cold compresses.
Mental and infraorbital blocks are usually unnecessary.
They often lead to transient nerve injuries
and hematomas which are painful. The block of the
greater palatine foramen often causes a sensation of
choking.
In terminal infiltration the puncture is made in the
mucobuccal (labial) fold, slightly gingival to the deepest
point, and the needle penetrates toward the bone in the
direction of the apex of the particular tooth. One should
consider the length of the root of each particular tooth
as seen on the roentgenogram.
Permanent molars require block injection; so do
multiple extractions or larger operations involving the
lower jaw. In making an inferior nerve block injection,
one has to bear in mind that the ascending ramus in
the child is shorter and narrower anteroposteriorly than
in the adult. The anteroposterior width may be estimated
by palpation through the skin. The lesser height of the
ramus has to be compensated for by inserting the needle
a few millimeters nearer to the occlusal plane than in
adults (Figures 9.1 A and B).
F i g u r e s 9.1 A and B: Difference in inferior alveolar nerve
block techniques
As mentioned earlier, the child should be informed
of the subjective signs such as tingling, numbness and
a feeling of swelling in the lip and tongue, either before
or preferably after the anesthesia has been administered.
Testing for anesthesia should be done carefully with
slowly increasing pressure of an explorer or other in-
strument, keeping in mind that anesthesia in the
superficial tissues does not necessarily mean anesthesia
of the deeper tissues.
The long buccal nerve should not be anesthetized until
definite signs of numbness in the respective side of the
lip appear, as the child might give misleading information
because he is confused by the tingling or numbness of
the mucosa of the lip. The long buccal nerve should be
anesthetized by terminal infiltration in the mucobuccal
fold of the respective tooth.

Exodontia Practice
EXTRACTION OF PRIMARY TEETH
INDICATIONS
In considering the advisability of extraction of primary
teeth, one should always keep in mind that age per se
is not an acceptable criterion in determining whether a
primary tooth should be removed. A primary second
molar, for example, should not be removed just because
a child is 11 or 12 years of age. unless there is a special
indication. For some patients the second premolars are
ready to erupt at 8 or 9 years of age while in other cases
these same teeth do not show sufficient root development
at the age of 12. A primary tooth that is firm and intact
in the arch should never be removed unless a complete
clinical and radiographic evaluation has been made of
the entire mouth and especially of the particular area.
Occlusion, arch development, size of teeth, amount
of root, resorption of the primary tooth involved, the
state of development of the underlying permanent suc-
cessor and adjacent teeth, presence or absence of
infection all of these factors must be considered in
determining when and how a primary tooth should be
removed.
With the above considerations in mind, indications
for extraction of primary teeth are as follows:
1. If the teeth are decayed beyond possible repair; if
decay reaches down into the bifurcation or if a sound
hard gingival margin cannot be established.
2. If infection of the periapical or interradicular area has
occurred and cannot be eradicated by other means.
3. In cases of acute dentoalveolar abscess with cellulitis.
4. If the teeth are interfering with the normal eruption
of the succeeding permanent teeth.
5. In cases of submerged teeth.
CONTRAINDICATIONS
Contraindications to extraction, except for the
considerations mentioned above, are more or less the
same as in adults. Many of these contraindications are
relative and may be overcome with special precaution
and premedication.
1. Acute infectious stomatitis, acute Vincent's infection
or herpetic stomatitis, and similar lesions should be
eliminated before an extraction is contemplated.
Exceptions to this are conditions such as acute
dentoalveolar abscesses with cellulitis, which demand
immediate extraction.
2. Blood dyscrasias render the patient susceptible to
postoperative infection and hemorrhage. Extractions
should be performed only after adequate consultation
with a hematologist and proper preparation of the
patient.
3. Acute or chronic rheumatic heart disease, congenital
heart disease and kidney disease require proper
antibiotic coverage.
4. Acute pericementitis, dentoalveolar abscesses and
cellulitis should be treated as will be explained later,
when and if indicated, with preoperative and
postoperative antibiotic medication.
5. Acute systemic infections of childhood contraindicate
elective extractions for the child because of a lowered
resistance of the body and the possibility of secondary
infection.
6. Malignancy, if suspected, contraindicates dental
extractions. The trauma of extraction tends to enhance
the speed of the growth and spread of tumors. On
the other hand, extractions are strongly indicated if
the jaw or surrounding tissues are to receive radiation
therapy for malignancy: this is done to avoid the risk
of an infection in the bone which has been exposed
to radiation.
7. 7eeth which have remained in irradiated bone should
be extracted only as a last resort and only after the
consequences have been fully explained to the
parents. If the teeth must be removed, consultation
with the radiologist who gave the irradiation might
be wise. Infection of the bone will follow extractions
in most cases even after antibiotic therapy, owing to
the avascularity which follows the radiation. The
infection is followed by a slowly progressing osteo-
myelitis which is very painful and which cannot be
controlled except by wide resection of the whole

99
Pediatric E x o d o n t i a
irradiated bone. It is. therefore, very dangerous to
remove teeth after exposure to radiation.
8.
Diabetes mellitus
poses a relative contraindication.
Consultation with the physician is a wise precaution
to make certain that the child is under control. In con-
trolled cases of diabetes, one does not observe more
infections than in normal children and there-fore
antibiotics are not a prerequisite to extraction. It is
important that the diabetic child retain his
diet in the same qualitative and quantitative
composition after an operation. Changes in these
respects may change the sugar and fat metabolism
of the child.
INDICATIONS FOR EXTRACTION OF PERMANENT
FIRST MOLARS
When making a decision about the fate of permanent
first molars, the following considerations should be kept
in mind. If a permanent first molar is removed before
the permanent second molar has erupted through the
gingiva, the chances that this second molar will move
mesially and occupy the space of the extracted first molar
are very good. If. on the other hand, the permanent
second molar has erupted through the gingiva at the time
of the loss of the permanent first molar, the second molar
will probably tilt forward into the space of the first molar,
causing conditions favoring periodontal disease and
orthodontic problems such as closing-of the bite.
The procedure in practice, therefore, should follow
the rule that when the second molar has not yet broken
through and one or two first molars are diseased beyond
repair, they should be removed. But if three first molars
are diseased beyond repair, all four first molars should
be removed with the expectation that a more symmetrical
dentition will result.
In cases in which the second molars have broken
through, every attempt should be made to save the first
molars. If extraction is necessary, only the destroyed teeth
should be removed and space maintainers should be
inserted.
EXTRACTION TECHNIQUE FOR PRIMARY TEETH
Armamentarium
Many dentists choose to use the same surgical instruments
for their child patients as they routinely use for their adult
patients. Most pediatric dentists and oral and maxillofacial
surgeons, however, prefer the smaller pediatric extraction
forceps, for the following reasons:
1. Their reduced size more easily allows placement in
the smaller oral cavity of the child patient.
2. The smaller pediatric forceps are more easily concealed
by the operator's hand.
3. The smaller working ends (beaks) more closely adapt
to the anatomy of the primary teeth.
The choice of the proper instrumentation can also
depend on special considerations unique to the child and
the adolescent. The use of cow horn mandibular forcep
is contraindicated for primary teeth, owing to the potential
for injury to the developing premolars. Great care must
also be given to the routine use of elevators and forceps
adjacent to large restorations such as metal crowns and
especially restorations adjacent to erupting single-rooted
teeth that may easily become dislodged with the slightest
force (Figures 9.2A and B).
Figures 9.2A and B: Pediatric extraction forceps

100
Exodontia Practice
General Considerations
The technique used to perform extractions in the child
patient is similar to the manual extraction technique used
in the adult. T h e greatest difference is in patient
management. It is essential that the dentist take the time
to describe the ensuing p r o c e d u r e completely a n d
accurately to the child. A few children require general
anesthesia for the surgical procedure to be accomplished.
The choice of proper local anesthesia-sedation-general
anesthesia technique d e p e n d s on the psychological
constitution of the child and the extent and nature of
the surgical procedure. The appropriate local anesthetic
technique for each type of tooth is described earlier in
this chapter.
A number of aspects of the extraction procedure
should be performed with every extraction. The dentist
should consult with the child and the parents prior to
surgery in order to prepare them for the upcoming
procedure. The dentist should provide any preoperative
needs, such as prescriptions or any dietaiy restrictions,
that might be necessary as a result of the planned sedative
techniques. T h e entire surgical p r o c e d u r e a n d the
expected postoperative recovery course should also be
described. This allows the parents to prepare for any
special postoperative arrangements, such as the need for
a soft diet or child care support. As noted before, the
dentist should perform a thorough review of the patient's
medical history, looking especially for medical conditions
that might complicate treatment.
There is no other type of dental treatment in which
the principles of tell. show, and do are more important
than during extractions. The dentist should be sure to
obtain profound anesthesia because once the patient has
felt pain, it may be difficult to regain the child's confidence
to a level in which he or she will behave in a manner
that allows completion of the procedure.
Just prior to the actual extraction, the dentist should
place the balls of the index finger and thumb in the
area of the extraction and demonstrate to the child the
types of pressures and movements that he or she will
encounter during the extraction. This digital pressure
should be firm enough to rock the child's head from
side to side in the headrest.
The dentist should be placed in the position in which
he or she can easily control the instrumentation, have
good visual access to the surgical site, and control the
child's head. The non-dominant hand of the dentist is
then placed in the patient's mouth. The role of the
nodominant hand is to help control the patient's head:
to support the jaw being treated: to help retract the cheek,
lips, and tongue from the surgical field; and to palpate
the a l v e o l a r process a n d adjacent teeth during the
extraction. Once the proper operator and nondominant
hand positions are established, the actual extraction
technique may begin. Variations in technique for individual
teeth are discussed later in this chapter, but the general
principles apply to all extractions are same.
After the tooth is removed from its socket, the surgical
site is evaluated visually and with the use of a curette.
The curette should be used as an extension of the dentist's
finger to palpate and evaluate the extraction site. No
attempt should be made to scrape the extraction site.
If a p a t h o l o g i c lesion such as a cyst or periapical
granuloma is present at the apex of a permanent tooth
socket, it should be gently e n u c l e a t e d . A g g r e s s i v e
manipulation of a curette in a primary tooth socket is
contraindicated owing to the potential for damage to the
succeeding tooth bud. The operator should palpate both
the facial and palatal or buccal and lingual aspects of the
surgical site to feel for any bone irregularities or alveolar
expansion. Any bone sharpness should be conservatively
removed with the use of either a rongeur or a bone file.
Digital pressure should be able to return the alveolus to
its presurgical configuration if gross e x p a n s i o n has
occurred.
MAXILLARY MOLAR EXTRACTIONS
Primary maxillary molars differ from their permanent
counterparts in that the height of contour is closer to the
cementoenamel junction and their roots tend to be more
divergent and smaller in diameter. Because of the root
structure and potential weakening of the roots during

P e d i a t r i c E x o d o n t i a
101
the eruption of the permanent tooth, root fracture in
primary maxillary molars is not uncommon.
The extraction is completed using a maxillary universal
forceps. Palatal movement is initiated first, followed by
alternating buccal and palatal motions with slow contin-
uous force applied to the forceps. This allows expansion
of the alveolar bone so that the primary molar with its
divergent roots can be extracted without fracture.
EXTRACTION OF MAXILLARY ANTERIOR TEETH
The maxillary primary and permanent central incisors,
lateral incisors, and canines all have single roots that are
usually conical. This makes them much less likely to
fracture and allows for more rotational movement during
extraction than is possible with multirooted teeth.
MANDIBULAR MOLAR EXTRACTIONS
When extracting mandibular molars, the dentist must give
special care to the support of the mandible with the
nonextraction hand so that no injury to the temporo-
mandibular joints is inflicted. The mandibular forceps are
used to extract the tooth with the same alternating buccal
and palatal motions used to extract maxillary primary
molars.
EXTRACTION OF MANDIBULAR
ANTERIOR TEETH
The mandibular incisors, canines, and premolars are all
single-rooted. Because of this fact, one must take great
care that the forceps do not place any force on adjacent
teeth because they can become easily dislodged. This
also enables the dentist to use rotational movements in
the extraction process. Then slow, continuous force applied
in alternating labial and lingual movements enables these
teeth to be removed easily.
MANAGEMENT OF FRACTURED
PRIMARY TOOTH ROOTS
Any dentist who extracts deciduous molars occasionally
has the opportunity to treat root fractures. Once the root
has fractured, the dentist must consider the following
factors. Aggressive surgical removal of all root tips may
cause damage to the permanent tooth buds. On the other
hand, leaving the root may increase the chance for
postoperative infection and may increase the theoretical
potential of delaying permanent tooth eruption, although
most primary root tips will resorb. A common-sense
approach is best. If the tooth root is clearly visible and
can be removed easily with an elevator or root tip pick,
the root should be removed. If several attempts fail or
if the root tip is very small or is situated very deep within
the alveolus, the root is best left to be resorbed, most
probably by the erupting permanent tooth. In some cases,
the root tips do not resorb but are situated mesially and
distally to the succeeding premolar and do not impede
its eruption. The patient and parents should be notified
that a root fragment has been retained, and they should
be assured that the chance of unfavorable sequelae is
remote.
If the preoperative evaluation indicates that a root
fracture is likely or that the developing succedaneous tooth
may be dislodged during the extraction, an alternative
extraction technique should be used. In these cases, the
crown should be sectioned with a fissure bur in a
buccolingual direction so that the detached portions of
the crown and roots can be elevated separately.
If sufficient resorption of the roots has occurred,
extractions may be very simple. On the other hand, if
a tooth, especially a molar, has to be removed prema-
turely, the roots may have undergone little or irregular
resorption, and this situation can make these extractions
difficult. It must be borne in mind that the crown of the
succeeding tooth is situated in close relationship to the
roots of the primary tooth. The widespread roots of the
primary molars surround the crowns of the permanent
teeth, and we may dislodge, if not extract, the forming
tooth if great care is not exercised during the extraction.
The permanent tooth will offer little opposition because
of the lack of development of its roots. Not infrequently
the resorption of a primary molar root occurs halfway
between the apex and the cemento-enamel junction.

2
Exodontia Practice
This weakens the root considerably and fractures of such
roots are not uncommon. Good radiographs are of great
importance and should be studied carefully before the
extraction is planned. If such a root is broken, the question
arises whether it should be removed immediately or
whether an attitude of watchful waiting should be taken.
The decision hinges upon the skill of the operator and
the accessibility of the root tip. If the tip can be removed
without trauma to the bud of the permanent tooth, it
should be elevated with small spear-point elevators.
Occasionally it is desirable to elevate a mucoperiosteal
flap and remove buccal bone to approach such a tip.
The commercial elevators are usually too heavy and large.
We prefer an instrument which has been ground into
a point from a straight root tip elevator.
If a permanent tooth bud is moved during an
extraction, it should be carefully pushed into its original
position and the socket closed with one or two sutures.
Some operators cover the bud with Gelfoam. Should
a permanent tooth bud be erroneously extracted, it
should be reinserted immediately without disturbing the
tooth follicle or dentinal papilla. Care should be taken
to orient the tooth in the socket in the proper buccolingual
position, and the socket should be closed by sutures. Pulp
tests should be made of the tooth after eruption.
If an already erupted permanent tooth with an
insufficiently formed root has been dislodged during the
removal of a primary tooth, it should be reinserted and
immediately splinted. After healing, pulp tests should be
made, although the radiographic findings of further root
development and of eventual narrowing of the root canal
are proof that the vascular supply has been reestablished.
Chapter

Exodontia Practice
Exodontia is a minor procedure that can be safely
performed in dental office provided the patient is healthy
and the procedure is not dramatically invasive. It might
require some special attention in situation where the
host is compromised either due to underlying systemic
disease or certain prevailing condition like pregnancy,
which render them susceptible to complications.
Knowledge regarding the patient's medical condition is
of utmost importance in patient management. One
should always keep the following words in mind "Dentist
should not be concerned only with the treatment of teeth
in patients but also the treatment of patients who have
teeth". Good pre-operative assessment endeavors to
anticipate and prevent trouble. Hence before any
extraction it is a clever practice to take a thorough medical
history and it is truly said time spent in taking thorough
history is never wasted. Certain systemic conditions needs
special mention like cardiac diseases (e.g. Hypertension),
respiratory disorders (e.g. asthma), endocrine disorders
(e.g. Diabetes mellitus. thyroid dysfunction), disorders
of hemostasis (e.g. hemophilia, thrombocytopenia)
patients on long-term steroids, antiplatelets, anticoagulant
drugs, pregnancy, etc. Exodontia can be relatively or
strictly contraindicated in such systemic conditions.
Criteria of fitness for a procedure are not absolute but
depends on factors such as the. type of procedure,
duration of procedure, degree of trauma and stress,
health of patient, degree of urgency of the procedure,
skill of the operator, etc. Although care of the medically
compromised patient is a complex problem requiring
specialties in the field, its occurrence is so common
that the practitioners and students must be acquainted
with these condition in order to have the competence
necessary to recognize and prevent problems
associated with exodontia. In this chapter the commonly
encountered systemic conditions, preoperative
assessment and relevant investigations to be performed,
special precautions to be taken pertaining to extraction
of teeth, anesthetic considerations, careful use of
drugs and indication, contraindications if any are
disscussed.
List of condition commonly encountered and needs
special mention.
• Diabetes
• Hypertension
• Infective endocarditis
• Heart failure
• Artificial valves/transplants
• Thyroid dysfunction
— Hyperthyroidism
— Hypothyroidism
• Disorders of hemostasis
— Hemophilia.
— Patients on anticoagulants, antiplatelet drugs.
• Patients on long-term steroids.
• Pregnancy
• Epilepsy
• Asthma
• Patients undergoing radiotherapy
DIABETES
Diabetes mellitus is a group of metabolic disorders
characterized by hyperglycemia resulting from defects
in insulin secretion, insulin action or both. There can be
a low output of insulin from the pancreatic beta cells,
or the peripheral tissue may resist insulin. Types of
diabetes includes insulin dependent (type I immune
mediated or idiopathic) and non-insulin dependent
(type II), Gestational diabetes mellitus. Other specific
types include, Genetic defects in beta cell function.
Genetic defect in insulin action, diseases of exocrine
pancreas, endocrinopathies. drug induced infectious
associated with other genetic syndromes.
Type I diabetes is the result of progressive destruction
of the beta cells in the islets of Langerharis. which leads
to severe insulin deficiency. Symptoms of diabetes
become apparent when approximately 80-85% of the
beta cells are destroyed. Develops most often in children
and young adults before the age of 25 years.
The etiology of type II diabetes is not established.
The principle underlying defects are insulin resistance
i.e. the reduction in biological effect of insulin on glucose

Exodontia for Medically Compromised Patients
metabolism, beta cell failure which includes delayed
insulin secretion after nutrient stimulation, inability to
compensate for insulin resistance, metabolic inhibition
of beta cell function by chronic hyperglycemia.
Clinical features of diabetes can be divided into early
and late. Early features usually includes confusion and
behavioral change, constipation, itching, increased thirst
and urination (polydipsia and polyuria), polyphagia,
unexplained weight loss, undue tiredness, tingling or
numbness in the extremities, burning feet. Late features
include abdominal pain, coma, dehydration, hyperven-
tilation, muscle wasting, nausea, paraesthesia, renal
failure, shock, vomiting.
Laboratory diagnosis can give some definite clue, a
person can be said as having diabetes if there are
symptoms of diabetes and random plasma glucose
concentration > / = 200 mg/dl. Fasting plasma glucose
> / = 126 mg/dl, 2 hours plasma glucose > / = 200
mg/dl during glucose tolerance test.
Complications of diabetes can be varied and classified
as acute and chronic. Acute complication include mainly
hypoglycemia and hyperglycemia. Hypoglycemia is seen
usually in patients treated with insulin and is due to
imbalance between food intake and insulin therapy.
Hypoglycemic coma is the main acute complication. It
is usually of rapid onset and is usually a result of failure
to take food, overdose of insulin, alcohol consumption.
Hyperglycemic coma is usually has a slow onset over
many hours with deepening drowsiness, signs of
dehydration, acidosis. Long standing diabetes can lead
to a variety of complication. Chronic complication of
diabetes mainly includes large blood vessel disease, small
vessel disease (microangiopathy) and increased
susceptibility to infection.
Diabetics are considered to be at increased risk of
preoperative morbidity and mortality because of the
involvement of their vital organs the autonomic nervous
system in the natural course of the disease. Poor
metabolic control results in dangerous acute metabolic
complications due to surgical stress. The infection that
develops in them tends to become virulent which further
worsens the metabolic state, thus establishing a vicious
cycle.
Hyperglycemia leads to impaired wound healing,
deficient formation of granulation tissue, with poor tensile
strength of collagen. The fibroblast formation takes longer
time than non-diabetics and there is a deficient capillary-
growth into the wound. The chemotactic, phagocytic and
bactericidal activity of the neutrophil is deficient. There
is impaired humoral host defense mechanism and
abnormal complement function. Hence metabolic
assessment and management of diabetes must begin
early and maintenance of euglycemia (atleast < 200
mg%) during peri-operative period will reduce the
morbidity and mortality to a very large extent.
Surgical procedure causes a considerable metabolic
stress in the non-diabetic and more so in a diabetic. The
stress response to surgery is mediated by neuroendocrine
system essentially by stimulating the adreno-medullary
axis. The neuroendocrine system comes into play to
maintain fuel requirements by glycogenolysis and
gluconeogenesis through stress hormones catecho-
lamines, glucagon. Cortisol, and growth hormone. In a
non-diabetic there is enough insulin secretion to utilize
the fuel produced by the stress hormones and thus
glucose homeostasis is maintained. Whereas this com-
pensatory elaboration of insulin is less possible in Type
II diabetic and cannot occur in Type I diabetic necessita-
ting supplementation of insulin in peri-operative period.
The pre-operative evaluation is necessary to know
the metabolic, nutritional, electrolyte, cardiac, pulmonary
and renal functions as well as the autonomic and
peripheral nervous system status. If the cardiac disease
is suggested by history and physical examination, the
tests to detect the presence of ischemic heart disease can
be helpful in preoperative assessment of the patient.
CARE PERTINENT TO EXODONTIA
Exodontia is a minor surgical procedure and is usually
elective unless performed in emergency depending on
the merit of individual case. It is important to determine
disease status, associated disorders and drug therapy.
Exodontia Practice
Physician consent should be obtained regarding the
planned surgical procedure including drug administra-
tion. Before performing any kind of procedure the dentist
should make use of stress reduction protocol. Stress
increases the amount of secreted Cortisol and endogenous
epinephrine which induces hyperglycemia. So the
procedure should be short, stress free and atraumatic.
Once every measure to reduce the anxiety of patient
is made, other most important concern is avoiding
hypoglycemia. Additional consideration should be given
to maintenance of normal dietary habits. Exodontia can
interfere with normal pattern of food intake and can
interfere with diabetic control, so the insulin dosage must
be adjusted accordingly. It is best to give oral glucose
just before appointment. The essential requirement is to
avoid hypoglycemia but to keep hyperglycemia below
levels that may be harmful because of delayed wound
healing or phagocytic dysfunction.
Appointments should be early to mid-morning after
a normal breakfast and normal antidiabetic treatment
because levels of endogenous corticosteroids are higher
in morning and stressful procedure are tolerated better.
Antibiotic prophylaxis varies depending on the state of
patient's metabolic control. Prophylactic antibiotic
coverage is indicated because of following reasons like
defective leukocyte function, decreased chemotaxis and
phagocytosis secondary to hypoglycemia, decreased
bactericidal activity, cellular immunity and vascular stasis,
higher infection rates and impaired healing. Local
anesthesia can be used safely. Epinephrine level in local
anesthesia has no significant effect on blood sugar but
excessive quantities of epinephrine should be avoided
to prevent elevation of blood glucose levels by stimulation
of sympathetic receptor system. Conscious sedation can
be used safely as well. Autonomic neuropathy in diabetes
can cause orthostatic hypertension hence supine position
should be slowly raised upright in the dental chair.
SYSTEMIC HYPERTENSION
Hypertension is a persistently raised blood pressure
resulting from raised peripheral arteriolar resistance, but
the definition of in terms of blood pressure, of what is
hypertension is arbitrary. In general the blood pressure
rises with age. When either or both systolic or diastolic
pressure are persistently raised and on remeasurement
with systolic pressure over 140 and diastolic over
90 mmHg, it is generally regarded as hypertension. About
one-third of the people with hypertension are unaware
of it, and those under treatment only one-third are fully
compliant. In more than 90% the cause is unknown and
it is then termed essential hypertension which becomes
more frequent as the age advances, and appears to be
related to genetic influence, obesity and various other
factors. About 40% of hypertensive patients have raised
levels of circulating catecholamines, epinephrine or nor-
epinephrine and may therefore have abnormal
sympathetic activity. Hypertension can be secondary to
defined causes such as renal disease, endocrine disorders,
pregnancy, oral contraceptives, certain drugs like cocaine,
amphetamine, immunosuppressives, glucocorticoids,
mineralocorticoids. etc. can raise the blood pressure. Some
nonsteroidal anti-inflammatory drugs like indomethacin
can impair the efficacy of the antihypertensive agents.
CARE PERTINENT TO EXODONTIA
It is important to determine status of hypertension,
associated disorders and physician's consent of any
planned surgical treatment regimen. Knowledge of drugs
administered with their potential to interact with
vasoconstrictors, other drug regimens and associated
systemic disorders. Implement strict stress reduction
protocol. Small, late morning appointments are preferred,
as endogenous epinephrine levels peak during morning
hours and adverse cardiac events are most likely in the
early morning.
Compliance and effectiveness of the medical therapy
should be confirmed by blood pressure recordings
(average of 2 recordings) at several short appointments
prior to and at the time of surgery. Patients with a
sustained blood pressure > 160/95 mm Hg are not
considered well controlled and exodontia should be
delayed until medical control is established.

Exodontia for Medically Compromised Patients
A risk in the administration of local anesthesia for
the hypertensive patient is the inclusion of epinephrine
and its sympathomimetic effect on cardiac beta-2
receptors. The current dosages of a local anesthetic
solution for a patient with poorly controlled hypertension
is two 1.8 ml cartridges (for a total dose of 3.6 ml) with
1:100.000 epinephrine per appointment. If lengthy
procedures are anticipated, the epinephrine should be
diluted to as ratio of 1:200.000. The side effects of
absorbed epinephrine must be weighed against the
benefits. Many clinical situations will contraindicate the
use of epinephrine. The apprehensive sweating, or
nervous patient likely has increased levels of endogenous
epinephrine. Because plasma levels of epinephrine
are dose dependent, administration of epinephrine
would be contraindicated for hypertensive patient.
The type of injection that is administered (block vs.
infiltration) as well as vascularity of the area where the
local anesthetic is being deposited is also an important
factor.
Barbiturates, narcotics and phenylephrine are
contraindicated in patients on mono-amine oxidase
inhibitors.
INFECTIVE ENDOCARDITIS
Infective endocarditis is a rare but dangerous, potentially
lethal infection, predominantly affecting heart valves.
Platelets and fibrin deposits accumulate at sites where
there is turbulent blood flow over damaged valves
(nonbacterial thrombotic endocarditis). These sterile
vegetations can thereafter readily be infected during
bacteremias resulting in infective endocarditis. Infective
endocarditis results from two main predisposing factors—
bacteremia and a cardiac lesion where there is turbulent
blood flow. Viridans streptococci such as Strep, mutans
and Strep, sanguis are most common causative
organisms. Others implicated include particularly
Staphylococcus aureus and enterococci. Viridans
streptococci have complex attachment mechanisms,
which may enable them to adhere to the endocardium.
The most common type of bacteremia implicated in
patients with infective endocarditis involves Viridans
streptococci, which are present in enormous numbers
in the mouth. Viridans streptococci proliferate where
oral hygiene is lacking and proliferate into the blood
stream in large numbers particularly in during tooth
extraction. Oral bacteremia after a tooth extraction are
generally transient and last for less than 15 min. but
may last even for one hour.
The signs and symptoms are highly variable. In the
previously healthy patient who acquires endocarditis due
to Viridans streptococci the picture is likely to be that.
3 or 4 weeks after a dental operation, there is insidious
onset of the low fever and mild malaise pallor or light
pigmentation of the skin, joint pains and hepatospleno-
megaly. The main effect of endocarditis are progressive
heart damage, infection or embolic damage of many
organs, especially the kidneys. Release of emboli can
have effects ranging from loss of a peripheral pulse to
sudden death from stroke. Embolic phenomenon
include hematuria, cerebrovascular occlusion, petechiae.
purpura of skin and mucous membrane, splinter
hemorrhage under the fingernails. Roth spots are small
retinal hemorrhages: Osier's nodes are small tender
vasculitic lesions of the skin.
CARE PERTINENT TO EXTRACTION
Prophylaxis should be given for dental procedures that
disturb the bacteria in periodontal sockets, since this
provides a g o o d chance of precipitating infective
endocarditis in a susceptible patient (Table 10.1). In a
survey of nearly 5000 cases of infective endocarditis
attributable to dental treatment, it was found to have
followed dental extractions in 95%. Role of antibiotic
prophylaxis is a subject of controversy but a word of
caution is that antibiotic prophylaxis is essential, where
appropriate. The current recommendations are,
therefore, that antibiotic prophylaxis is mandatory for
extraction. The surgical procedure should be minimally
invasive and atraumatic as far as possible.

Exodontia Practice
Table 1 0 . 1 : Possible prophylactic antibiotic regimens
against infective endocarditis
Recommending authority
Regimen
U K : B r i t i s h S o c i e t y for 1 9 9 2
A n t i m i c r o b i a l C h e m o t h e r a p y
E u r o p e a n c o n s e n s u s 1 9 9 5
A m e r i c a n H e a r t A s s o c i a t i o n 1 9 9 7
( a ) A m o x i c i l l i n : 3 g 1 h b e f o r e
t r e a t m e n t
( b ) C l i n d a m y c i n : 6 0 0 m g 1 h
b e f o r e t r e a t m e n t
( a ) A m o x i c i l l i n : 3 g 1 h b e f o r e
t r e a t m e n t
( b ) C l i n d a m y c i n : 3 0 0 - 6 0 0 m g
1 h b e f o r e t r e a t m e n t
( a ) A m o x i c i l l i n : 2 g 1 h b e f o r e
t r e a t m e n t
( b ) C l i n d a m y c i n : 6 0 0 m g 1 h
b e f o r e t r e a t m e n t
HEART FAILURE
Heart failure is when the pumping action of the heart
is insufficient to meet body's demands. Lack of tissue
and organ perfusion results. The most common cause
of heart failure is ischemic heart disease. Left-sided heart
failure results in damming of blood back from the left
ventricle to the pulmonary circulation with pulmonary
hypertension and pulmonary edema. Lying down
worsens pulmonary congestion, edema and dyspnea
(orthopnea). It also makes respiration less efficient, and
cyanosis likely, because the abdominal viscera move the
diaphragm higher and reduce the vital capacity of the
lungs. Coughing is another typical consequence. The
sputum is frothy and. in severe cases, pink with blood.
In the more advanced stages of left-sided heart failure
there is inadequate cerebral oxygenation, leading to
symptoms such as loss of concentration, restlessness and
irritability or. in the elderly, disorientation. Right-sided
heart failure causes mainly congestion of the systemic
and portal venous systems, affecting primarily the liver,
gastrointestinal tract, kidneys and subcutaneous tissues.
It thus presents with peripheral (dependent) edema and
fatigue. The liver is usually enlarged due to passive
congestion, causing abdominal discomfort and. in severe
cardiac failure, raised portal venous pressure also leads
to escape of large amounts of fluid into the peritoneal
cavity (ascites). Most patients suffer bi-ventricular failure,
since failure of one side of the heart usually leads to
failure of the other. The pulse may become rapid and
irregular, particularly if there is atrial fibrillation, and. in
extreme cases, patients are cyanotic, polycythemic,
dyspneic at rest and edematous with pulmonary edema
and distension of neck veins -(raised jugular venous
pressure). Heart failure is usually progressive, but may
cause few symptoms until activity becomes limited with
breathlessness (dyspnea), cyanosis and dependent
edema (usually swollen ankles). Sacral or ankle edema
are common dysrhythmias and sudden death may
result.
CARE PERTINENT TO EXTRACTION
It is dangerous to lay any patient with left-sided heart
failure supine. It will severely worsen dyspnea. The dental
chair should be kept in a partially reclining or erect
position. Extraction may precipitate dysrhythmias, angina
or heart failure. Anxiety must be minimized and pain
control must be fully effective. For patients with poorly
controlled or uncontrolled cardiac failure (worsening
dyspnea with minimal exertion, dyspnea at rest, or
nocturnal angina).medical attention should be obtained
before any dental treatment. Appointments should be
short. Patients are best treated in the late morning.
Endogenous epinephrine levels peak during morning
hours and cardiac complications are most likely in the
early morning. Late morning appointments are recom-
mended. An aspirating syringe should be used to give
a local anesthetic. Epinephrine may, theoretically,
increase hypertension and precipitate dysrhythmias.
Blood pressure tends to rise during oral surgery under
local anesthesia, and epinephrine can theoretically
contribute, but this is usually of little 'practical impor-
tance'. Effective analgesia must be p r o v i d e d .
Bupivacaine should be avoided as it is cardiotoxic.
Otherwise, local anesthesia can usually safely be used
providing that consideration is given to the underlying
cause of the cardiac failure. Epinephrine containing local
anesthetics should not be given in large doses to patients
taking beta blockers. Interactions between epinephrine
and the beta blocker may induce hypertension if
excessive doses of the local anesthetic are given.

Exodontia for Medically Compromised Patients
Supplemental oxygen should be readily available.
Cardiac monitoring may be desirable.
Medication such as diuretics may cause orthostatic
hypotension, and therefore patients should be raised
slowly to the upright position. NSAlDs other than aspirin
should be avoided in those patients taking ACE inhibitors
since they increase the risk of renal damage. Patients
being treated with digoxin for atrial fibrillation or congestive
heart failure are more prone to ECG changes such as ST
segment depression during dental extractions under local
anesthesia than other cardiac patients. Erythromycin and
tetracycline should be avoided as they may induce digitalis
toxicity by impairing gut flora metabolism of the digitalis.
Some drugs may complicate treatment, such as digitalis
(vomiting). ACE inhibitors (coughing) or itraconazole
(cardiac failure). Conscious sedation can usually safely
be used. However, consideration must be given to the
underlying cause of the cardiac failure.
ARTIFICIAL HEART VALVES AND TRANSPLANTS
Currently used prosthetic heart valves (synthetic or
porcine) are composed of teflon or teflon like material
to diminish the possibility of adhesions. The danger of
clumps of bacterial colonies collecting on these valves
increases after a bacteremia induced secondary to dental
procedures. So such patients are highly susceptible to
endocarditis, therefore physician's consult for antibiotic
pre-medication is important. The management challenge
is most difficult because of the need to avoid altering
the cardiac output and the physiologic or pharmacologic
compensation mechanisms.
TREATMENT CONSIDERATIONS
Patients who have received a mechanical or bio-pros-
thetic artificial heart valve are at high-risk for endocarditis.
The overall risk for prosthetic valve endocarditis is
1-2% per patient year. Infections due to it are of 2 types
that occurring early within 2 months of valve replacement
which is caused by Staphylococci. Streptococci and
gram negative bacilli. Other occurring late, i.e. 2 months
of v a l v e replacement, caused by Streptococci
predominantly, antimicrobial prophylaxis is mandatory
in these patients. Such patients are maintained on life-
long immunosuppressive therapy which creates an
increased potential for infection. Steroids suppress the
adrenal glands and supplemental corticosteroid therapy
is necessary. When the patient is stable post-operatively.
the condition and recent history must be assessed to
determine if urgent dental care only should be provided
in the first 6 months with necessary antibiotics, monitoring,
concern for coagulopathies and adrenal suppression.
After 6 months, if the patient is stable, the evalua-
tion of the patient's recent history and medical
consultation should reveal what dental extraction is
generally possible with considerations for adrenal
suppression and the potential for infection owing to
immunosuppression.
A significant increase in heart rate is observed in such
patients after administration of 2% lidocaine with
1:80.000 epinephrine, but not after the administration
of 3% mepivacaine with 1:100.000 epinephrine and
prilocaine with felypressin. This suggests that without,
or with, low concentrations of epinephrine should be
used. Such patients should receive antibiotic premedi-
cation orally parenteraly. Local (topical) measures for
hemostasis should be used.
Lab investigation should be carefully evaluated.
PT and aPTT should be adjusted to within 150 % of
the normal/control value, i.e. 11 and 35 sec. respectively.
BT should be under normal range.
HYPERTHYROIDISM
Hyperthyroidism is associated usually, with a diffuse goiter
due to autoimmune disease(graves disease, primary
hyperthyroidism) when there are thyroid-stimulating
autoantibodies against thyroid TSH receptor (TRAbs)
and thyroid microsomal antibodies (TMAbs) sometimes,
with a hyperfunctioning (toxic) multinodular goiter or
nodule due to one or more thyroid adenomas producing
excess thyroxine. 90% of the swellings are benign rarely
with thyroiditis, thyroid hormone overdosage, or ectopic
thyroid tissue.

110
Exodontia Practice
Clinical features include anorexia, vomiting or
diarrhea, weight loss, anxiety and tremor sweating and
heat intolerance cardiac disturbances, particularly in elder
patients. These includes tachycardia, dysrhythmias
(especially atrial fibrillation) or cardiac failure exoph-
thalmos, eyelid lag and eyelid retraction. Thyrotoxic
periodic paralysis comprises attacks of mild to severe
weakness, during which serum potassium levels are
generally low. Myasthenia gravis may occasionally be
associated.
CARE PERTINENT TO EXTRACTION
Patients with untreated hyperthyroidism can be difficult
to deal with as a result of heightened anxiety irritability.
The sympathetic overactivity may lead to fainting. Local
anesthesia is the main means of pain control. The risk
from epinephrine exacerbating symphathetic overactivity
is only theoretical.Conscious sedation is frequently
desirable to control excessive anxiety. Benzodiazepines
may potentiate antithyroid drugs, and therefore nitrous
oxide, which is morerapidly controllable, is probably
safer. Povidone-iodine and similar compounds are best
avoided. Carbimazole occasionally causes agranulo-
cytosis, which may cause oral or oropharyngeal ulceration.
Otherwise the treated thyrotoxic patient presents no
special problems in dental treatment. However, after
treatment of hyperthyroidism the patient is at risk from
hypothyroidism, which may pass unrecognized.
HYPOTHYROIDISM
Hypothyroidism may be primary (due to thyroid
disease)or secondary (to hypothalamic or pituitary
dysfunction).The common causes of hypothyroidism are
thyroid loss from surgical removal of too much thyroid
tissue in a previously hyperthyroid patient or destruction
by irradiation of the neck or thyroid gland autoimmune
disease (Hashimoto's thyroiditis), associated with
autoantibodies to thyroglobulin and thyroid microsomes.
Clinical features includes weight gain, lassitude, dry
skin, myxoedema. loss of hair, cardiac failure or ischemic
heart disease, bradycardia, anemia, neurological or
psychiatric changes, hypotonia, cerebellar signs of ataxia,
tremor, and dysmetria. polyneuropathy, cranial nerve
deficits, entrapment neuropathy (e.g. carpal tunnel
syndrome), myopathic weakness, dementia, apathy,
mental dullness, irritability, sleepiness, hoarseness,
hypothermia and may be complicated by coma.
CARE PERTINENT TO EXTRACTION
The main danger is of precipitating myxoedema coma
by the use of sedatives (including diazepam or
midazolam), opioid analgesics (including codeine), or
tranquilizer. These should, therefore, be either avoided
or given in low dose. Local anesthesia is satisfactory for
pain control. Conscious sedation can be carried out with
nitrous oxide and oxygen. Diazepam or midazolam may
precipitate coma. Associated problems may include
hypoadrenocorticism, anemia, hypotension, diminished
cardiac output and bradycardia. Occasional associations
include hypopituitarism and other autoimmune disorders
such as Sjogren's syndrome. Povidone-iodine and
similar compounds are best avoided.
PATIENT ON EXOGENOUS STERIODS
Corticosteriods are frequently used to suppress inflam-
mation, and for immunosuppression, and occasionally
to replace missing hormones like in Addison's disease
or after adrenalectomy. Corticosteriods act by binding
to cytoplasmic receptors, to produce alterations in
regulatory protein synthesis. One regulatory protein,
lipocortin (macrocortin). a member of the annexin
superfamily of proteins, inhibits phospholipase A2 and
so prevents metabolism of arachidonic acid to leuko-
trienes. prostaglandins and thromboxanes involved in
inflammation. Glucocorticoids also increase beta-
receptor synthesis, reduce microvascular permeability,
reduce cytokine production and mast cells and eosino-
phils. Anti-inflammatory mechanisms involve the
glucocorticoid receptors, the glucocorticoid-responsive
genes, and the release of anti-inflammatory molecules
such as lipocortin-1, IL-IO. IL-1 ra. and nuclear factor-
KB. Corticosteroids induce the transcription of the gene
Exodontia for Medically Compromised Patients
to decreas the pro-inflammatory cytokine secretion. As
a consequence, the immune system is 'blocked'.
Corticosteroids have a negative feedback control on
hypothalamic activity and A C T H production and there
is, thus, suppression of the hypothalamic-pituitary-
adrenocortical axis (HPA) and the adrenals may become
unable to produce a steroid response to stress. Cortico-
steroids are an essential part of the body's response to
stresses such as trauma, infection, general anesthesia or
operation. At such times there is normally an enhanced
adrenal corticosteroid response related to the degree of
stress. In patients given exogenous steroids, the enhanced
adrenal corticosteroid response may not follow. When
the adrenal cortex is unable to produce the necessary
steroid response to stress, acute adrenal insufficiency
(adrenal crisis) can result, with rapidly developing
hypotension, collapse and possibly death. Suppression
of the H P A axis becomes deeper if corticosteroid
treatment has been prolonged and/or the dose of steroids
exceeds physiological levels (more than about 7.5 mg/
day of prednisolone). Adrenal suppression is less when
the exogenous steroid is given on alternate days or as
a single morning dose (rather than as divided doses
through the day). Corticotrophin (ACTH) has been used
in the hope of reducing adrenal suppression, but the
response is variable and unpredictable. However, adrenal
function may even be suppressed for up to 1 week after
cessation of steroid treatment lasting only 5 days. If
steroid treatment is for longer periods, adrenal function
may be suppressed for at least 30 days and perhaps
for 2-24 months after the cessation of treatment. Patients
on. or who have been on. corticosteroid therapy within
the past 30 days may be at risk from adrenal crisis, and
those who have been on them during the previous 24
months may also be at risk, if they are not given
supplementary corticosteroids before and during periods
of stress such as operation, general anesthesia, infection
or trauma. Patients who have used systemic cortico-
steroids should be warned of the danger and should
carry a steroid card indicating the dosage and the
responsible physician. However, the frequency and
extent of the adrenocortical suppression (and the need
for supplementary corticosteroids before and during
periods of stress is unclear and has been questioned.
Although the evidence for the need for steroid cover
may be questionable, medicolegal and other
considerations suggest that one should act on the side
of caution and fully inform and discuss with the patient
take medical advice in any case of doubt give a steroid
cover unless confident that collapse is unlikely.
CARE PERTINENT TO EXTRACTION
Dentoalveolar or maxillofacial surgery may result in stress
and a Cortisol response. Minor operations under local
anesthesia may be covered by giving the usual oral
steroid, dose in morning and giving oral steroids 2-4 h
pre- and postoperatively (25-50 mg hydrocortisone or
20 mg prednisolone or 4 mg dexamethasone) or by
giving IV 25-50 mg hydrocortisone immediately before
operation. Intravenous hydrocortisone must be
immediately available for use if the blood pressure falls
or the patient collapses. Corticosteroids given by
intramuscular injection are more slowly absorbed and
reach lower plasma levels than when given intravenously
or orally. Patients may also require special management
as a result of diabetes, hypertension, poor wound healing,
or infections. Aspirin and other nonsteroidal anti-
inflammatory agents should be avoided as they may
increase the risk of peptic ulceration. Susceptibility to
infection is increased by systemic steroid use. In addition
to careful aseptic surgery, prophylactic antimicrobials may
be indicated.
PATIENTS RECEIVING WARFARIN THERAPY
Warfarin is an anticoagulant which inhibits synthesis of
the vitamin K-dependent coagulation factors II, VII, IX
and X. Indications for anticoagulation are increasing, and
dentists will be consulted by patients taking warfarin .The
activity of warfarin is expressed using the international
normalized ratio (INR). INR = (patient PT/mean normal
P T )
I S I
or log INR = ISI (log observed PT ratio), where
ISI denotes the International Sensitivity Index of the
2
Exodontia Practice
thromboplastin used at the local laboratory to perform
the PT measurement. The ISI reflects the responsiveness
of a given thromboplastin to reduction of the vitamin
K-dependent coagulation factors. The more responsive
the reagent, the lower the ISI value. A normal
coagulation profile has an INR of 1.0. The desirable
INR range for patients depends on the condition being
treated. Patients receiving treatment for deep vein
thrombosis have a lower target range than those with
prosthetic heart valves. The risk of bleeding increases
exponentially as the INR rises. Gingival bleeding can
indicate a raised INR. Oral surgery can be completed
safely with an INR from 1.5 to 2.5. With appropriate
local measures to reduce bleeding, teeth may be removed
by simple extraction with an INR of 2-4. However dentists
should still be cautious before they remove teeth where
the INR exceeds 3 (Table 10.2). The possibility of
postoperative bleeding in patients taking warfarin
concerns dentists. However, before deciding if warfarin
therapy should be interrupted the risk of perioperative
or postoperative bleeding must be balanced against the
risk of thromboembolism.
CARE PERTINENT TO EXTRACTION
Before extraction a thorough medical history should be
obtained including details of any condition likely to be
treated with warfarin. The dentist should also consider
possible drug interactions with warfarin. Medications
including antibiotics such as metronidazole, herbal
remedies and alcohol may unpredictably alter the INR.
If an interaction is considered likely or if the effect of
any prescribed medication is not known, the dentist
should consult the doctor supervising the patient's
anticoagulant therapy. The INR should be checked
before surgery.
In most cases of dento-alveolar oral surgery, including
simple extraction of teeth, bleeding can be controlled
in a reasonable time by minimizing the extent of surgery
to one site or quadrant, and using firm sutures or firm
postoperative packs over the wound. Preferably surgery
should be performed in the morning to facilitate
postoperative observation.
Where the operative site is infected the use of
antibiotics should be restricted to a preoperative
prophylactic dose and postoperative antibiotics should
be discontinued as soon as reasonable. Prolonged use
of broad spectrum antibiotics should be avoided as it
may change the effectiveness of warfarin by altering gut
microflora compromising availability of vitamin K. Aspirin
and non-steroidal anti-inflammatory drugs may also
increase the risk of bleeding.
Local anesthetics should be given cautiously avoiding
venepuncture. To avoid the needles becoming barbed
and tearing tissues, they should be used once only for
each mucosal or skin puncture. Local vasoconstriction
may be encouraged by infiltrating a small amount of
local anesthetic solution with 1:100 000 or 1:200 000
adrenaline close to the surgery site
PATIENTS TAKING ASPIRIN
Aspirin irreversibly impairs platelet aggregation and is
used long-term in the prevention of cardiovascular events
and stroke in patients at risk. In large doses, aspirin may
also cause hypoprothrombinemia. Even small doses of
Table 10.2: Range of International Normalised Ratio
Type of Suboptimal Suboptimal Normal target Normal target May be normal Out of range
treatment range range INR range INR range target with
mechanical
heart valve
<1.5 1.6-1.9 2.0-2.5 2.5-3.0 3.1-3.5 3.5
Simple extraction Safe Safe Safe Local measures Local measures Not advised
Multiple extraction Safe Safe Local measures Local measures Local measures Not advised
Single bony impaction
Exodontia for Medically Compromised Patients
113
aspirin prolong the bleeding time, impair platelet
adhesiveness. Aspirin may worsen bleeding tendencies
if there are other anticoagulation medications other
bleeding disorders, such as uremia. Patient taking
even one 80 mg aspirin have platelet functions altered
for upto a week until new. unaffected platelets are
produced.
CARE PERTINENT TO EXTRACTION
In patients with no other cause for a bleeding tendency
and receiving up to 100 mg aspirin daily, in general, for
uncomplicated forceps extraction of 1-3 teeth. Suturing
and packing the socket with resorbable gelatin sponge,
oxidized cellulose, or microfibrillar collagen can be
carried out if necessary. In patients with no other cause
for a bleeding tendency and receiving doses of aspirin
higher than 100 mg daily, if there is concern, the current
value of the bleeding time should be established. If it
is over 20 min. surgery should be postponed.
PATIENTS ON HEPARIN
Heparin is a natural product, abundant in granules of
the mast cells that line the vasculature. It is released in
response to injury. Heparin is also used as a parenteral
anticoagulant, given subcutaneously or intravenously for
acute thromboembolic episodes or for hospitalization
protocols that include significant surgical procedures, to
prevent deep venous thrombosis and pulmonary emboli.
Heparin is a sulphated glycosaminoglycan originally
obtained from liver. Heparin acts immediately on blood
coagulation to block the conversion of fibrinogen to fibrin,
mainly by inhibiting the thrombin-fibrinogen reaction via
its binding to and catalysing antithrombin III. which then
inhibits the serine proteases of the coagulation cascade
to inactivate thrombin. Heparin also acts on activated
factors IX-XII and increases platelet aggregation but
inhibits thrombin-induced activation. The anticoagulant
effect of standard or low molecular weight heparin has
an immediate action on blood clotting, which is usually
lost within 6 h of stopping it. The prothrombin, activated
partial thromboplastin (APTT) and thrombin times (TT)
are prolonged. Most patients are monitored with the
APTT and are maintained at 1.5-2.5 times the control
value (the therapeutic range). Large doses of heparin
can prolong the INR. Platelet counts should also be
monitored if heparin is used for more than 5 days, since
it can cause thrombocytopenia. Autoimmune thrombo-
cytopenia is possible within 3-15 days, or sooner if there
has been previous heparin exposure. Heparin is available
as standard or unfractionated heparin, or low-molecular-
weight (LMW) heparins. The latter, such as certoparin.
interact with factor Xa. but do not affect standard blood
test results.
CARE PERTINENT TO EXTRACTION
For uncomplicated forceps extraction of 1-3 teeth, there
is usually no need to interfere with anticoagulant
treatment involving heparin or low-molecular-weight
heparins or antiplatelet drugs. Heparin has an immediate
effect on blood clotting but acts for only 4-6 h and no
specific treatment is therefore needed to reverse its effect.
The effect of heparin is best assessed by the APTT.
Withdrawal of heparin is adequate to reverse anticoagu-
lation where this is necessary. In an emergency, this can
be reversed by intravenous protamine sulphate given in
a dose of 1 mg per 100IU heparin, but a medical opinion
should be sought first. Where heparin has been stopped,
any surgery can safely be carried our after 6-8 h. Low-
molecular-weight heparin may have little effect either
on the APTT or on postoperative bleeding, despite their
longer activity (Up to 24 h). However, the advice of the
hematologist should be sought before surgery.
HEMOPHILIA
Common forms of hereditary bleeding disorders caused
by clotting factor deficiencies of factor VIII, IX. or XI.
Hemophilia A (factor VIII deficiency), which affects about
80% of hemophiliacs, and hemophilia B (factor IX
deficiency) have identical clinical manifestations,
screening test abnormalities, and X-linked genetic
transmission. Specific factor assays are required to
distinguish the two. Hemophilia may result from gene

Exodontia Practice
mutations: point mutations involving a single nucleotide,
deletions of all or parts of the gene, and mutations
affecting gene regulation. About 50% of cases of severe
hemophilia A result from a major inversion of a section
of the tip of the long arm of the X chromosome. Because
factor VIII and factor IX genes are located on the X chro-
mosome, hemophilia affects males almost exclusively.
Daughters of hemophiliacs will be obligatory carriers,
but sons will be normal. Each son of a carrier has a 50%
chance of being a hemophiliac, and each daughter has
a 50% chance of being a carrier. Rarely, random
inactivation of one of the two X chromosomes in early
embryonic life will result in a carrier's having a low factor
VIII or IX level to experience abnormal bleeding.
A patient with a factor VIII or IX level < 1% of normal
has severe bleeding episodes throughout life. Minor
trauma can result in extensive tissue hemorrhages and
hemarthroses, which, if improperly managed, can result
in crippling musculoskeletal deformities. Bleeding into
the base of the tongue, causing airway compression,
may be life threatening and requires prompt, vigorous
replacement therapy. Patients with factor VIII or IX levels
about 5% of normal have mild hemophilia. They rarely
have spontaneous hemorrhages: however, they will bleed
severely (even fatally) after surgery if not managed
correctly. Occasional patients have even milder
hemophilia with a factor VIII or IX level in the 10 to
30% of normal range. Such patients may also bleed
excessively after surgery or dental extraction.
Typical findings in hemophilia are a prolonged PTT.
a normal PT and a normal bleeding time. Factor VIII
and IX assays determine the type and severity of the
hemophilia. Because factor VIII levels may also be
reduced in VWD. VWF antigen should be measured in
patients with newly diagnosed hemophilia A. particularly
if the disease is mild and a family history cannot be
obtained. After transfusion therapy, about 15% of
patients with hemophilia A develop factor VIII antibodies
that inhibit the coagulant activity of further factor VIII
given to the patient. Patients should be screened for
factor VIII anticoagulant activity (e.g. by measuring the
degree of PTT shortening immediately after mixing the
patient's plasma with equal parts of normal plasma and
after incubation for 1 h at room temperature), especially
before an elective procedure that requires replacement
therapy.
CARE PERTINENT TO EXTRACTION
Hemophiliacs should avoid using aspirin. There should
be judicious use of other NSAIDs. which have a lesser,
more transient effect than aspirin on platelet function.
All drugs should be given orally or IV: IM injections can
cause large hematomas. Fresh frozen plasma contains
factors VIII and IX. However, unless plasma exchange
is performed, sufficient whole plasma cannot be given
to patients with severe hemophilia to raise factor VIII
or IX concentrations to levels that effectively prevent or
control bleeding. For hemophilia A. the treatment of
choice is viral inactivated or recombinant factor VIII
concentrate. For hemophilia B. the treatment of choice
is a highly purified viral inactivated factor IX concentrate.
In hemophilia A. the factor VIII level should be raised
transiently to about 0.3 U (30%) to prevent bleeding
after dental extraction.
In hemophilia B. the plasma factor IX level rises to
only half of that expected from the units of factor IX
listed on the bottle. This may reflect binding of infused
factor IX to vascular endothelium.
An antifibrinolytic (-aminocaproic acid 2.5 to 4 g
postoperative qid for 1 week or tranexamic acid 1.0
to 1.5 g postoperative tid or qid for 1 week) should
be given to prevent late bleeding after dental extraction.
Treatment of bleeding in hemophiliacs who develop a
factor VIII inhibitor is difficult, and a specialist should
be consulted. Patients with a low initial antibody titer
may be given a large dose of factor VIII to overcome
the inhibitor and temporarily raise plasma factor VIII
concentration. If this does not control the bleeding, further
factor VIII infusion will usually be futile because of the
rapid rise in antibody titer. The factor VIII antibodies
responsible for inhibitor activity are heterogeneous and
in some patients do not inhibit or only minimally inhibit

Exodontia for Medically Compromised Patients
porcine factor VIII. Thus, a high-purity porcine factor
VIII preparation controls bleeding in such patients.
Prothrombin complex concentrate, which contains factor
IX and variable amounts of an activity that bypasses
the role of factor VIII in coagulation, has also been used
to manage serious bleeding in patients with a high-titer
inhibitor, but it may also induce hypercoagulability and
a paradoxical thrombotic event. The factor VIII inhibitor-
bypassing material in prothrombin complex concentrate
may be factor IXa. Recombinant factor Vila in repeated
high doses (e.g. 90 ugkg) controls bleeding in some
patients with a factor VIII inhibitor without inducing a
hypercoagulable state. Long-term control of inhibitors
in hemophilia A is achieved in most patients by inducing
immune tolerance through continuous exposure to factor
VIII.
PREGNANCY
Pregnancy is a major event in any women's life and
is associated with physiological changes affecting especially
the endocrine, cardiovascular and hematological systems
and often attitude, mood, behavior. Knowledge of
physiologic changes from non-gravid woman to gravid
woman is of utmost importance to dental surgeon. The
hormonal and physiologic changes during gestation
results in alteration of major organ system.
The dental surgeon who treats a gravid woman
should be aware that he she is treating two patient, the
unborn child the second one. In most instances surgery
can be performed safely with proper consultation. Most
experts agree that elective surgical procedures should
be delayed until after delivery. Physiologic changes are
due to hormonal release, anatomic changes or both.
The normal period of pregnancy is approximately
38 weeks - 9 months. For clinical purposes, the gestation
period is usually divided into trimesters (period of 3
months), because each trimester presents different
considerations in medical and dental management.
Trimester approach is safe for mother and child because
it accounts the period of greater risk of harming the
developing fetus or embryo. The embryonic period
spanning weeks 2 through 8 post conception, is the time
of active organogenesis and therefore greater suscepti-
bility to teratogens. The concern of doing procedure
during the first trimester is two-fold. First, the developing
child is at greatest risk posed by teratogens during
organogenesis, and second during the first trimester it
is known that as many as one in five pregnancies undergo
spontaneous abortion. The current recommendation is
that necessary procedures be done during second
trimester. By the second trimester, organogenesis is
completed, and the risk to the fetus is low. The mother
has also had time to adjust to her pregnancy, and the
fetus has not grown to a potentially uncomfortable size
that would make it difficult for the mother to remain
still for long periods. The positioning of the pregnant
patient is important, especially during the third trimester.
As the uterus expands with the growing fetus and
placenta, it comes to lie directly the inferior vena cava,
femoral vessel, and the aorta. If the mother is positioned
supine for a procedure the weight of the gravid uterus
could apply enough pressure to impede blood flow
through the major vessels and cause a condition called
supine hypotension. In this condition, the blood pressure
drops secondary to the impeded blood flow, which
causes a syncopal or near syncopal episode. This situation
is easily remedied by proper positioning of the patient
on her left side and elevating the head of the chair to
avoid compression of major vessels.
CARE PERTINENT TO EXTRACTION
Detailed information of pregnancy state is obtained and
non urgent treatment should be delayed to the post-
partum period. If patient is unsure regarding her preg-
nancy refer to physician. In case of emergency situation
inquire about last menstrual period cycle.The fetus is most
susceptible to harmful effect of teratogens, carcinogens
and maternal stress during first and third trimester.
Certain procedures when clinically indicated may be
defered to 2nd trimester. Important points to be stressed
before doing any extraction procedure is the stress of

6
Exodontia Practice
surgery, stress of anesthesia, ionizing radiations, drugs.
It is generally accepted that dental radiographs and
minor procedures like exodontia under local anesthesia
expose fetus to minimal risk. Gynecological consultation
should be taken before performing exodontia. Risk
benefit ratio of delaying treatment is made on time of
presentation and progress of disease. Beyond first
trimester, gravid patient should not placed in supine
position because enlarged gravid uterus compress the
vena cava and decrease in cardiac output as low as 30%
results in supine hypotension syndrome of pregnancy.
Compression of vena cava increases venous stasis and
enhances risk of clot formation. Sign and symptoms
includes light headedness. tachycardia, loss of
consciousness. The appropriate and desired position is
left lateral position with right buttock and hip elevated
to approximately 15 degrees. Local anesthesia should
be preferred over general anesthesia.
Procedure like extraction of tooth have the potential
to escalate into bacteremia and sepsis, with resulting
serious fetal complications making antibacterial treatment
and prophylaxis important in pregnant patient.
Obstetrician's consult if doubtful about the teratogenic
effects of a medication.
Drugs which can be safely administered include
Acetaminophen or its combination with oxycodone
(opiod analgesic) for mild to severe pain control.
Beta-lactam antibiotics like Penicillin. Amoxicillin.
Cephalosporin.
Drugs contraindicated are estolate form of erythro-
mycin base because it increases risk of cholestatic
hepatitis.
Tetracyclines have increased effect on developing
tooth and bones. Chloramphenicol. Metronidazole have
carcinogenic effects. Narcotics causes respiratory
depression in fetus and mother.
NSAIDs in 3rd trimester prolongs pregnancy and
labor. It causes anti- and post-partum hemorrhage,
increased chances of oral clefts and other defects,
increased chances of fetal mortality.
EPILEPSY
It is a brain disorder which manifests as chronic, sudden,
often recurrent, paroxysmal, discharge of the cerebral
neurons, resulting in episodic disturbances of conscious-
ness and autonomic nervous system. Convulsive or
involuntary muscle movements called as seizures /fits.
It affects about 1-2% of general population, but more
prevalent in young and handicapped patients. Epilepsy
is characterized by seizures of any type that are chronic
and recurrent. In addition to seizures, there may be other
features, such as headache, changes in mood or energy
level, confusion, and memory loss. The main types of
epilepsy are generalized seizures (grand mal (tonic-clonic)
and petit mal) - when consciousness is typically lost and
petit mal. Partial seizures, which include simple seizures
during which the person remains alert, but there are
abnormal movements or sensations. In complex seizures
abnormal movement or sensation is accompanied by
changes in consciousness. Generalized seizures are the
most dramatic but partial complex seizures are the most
common.
CARE PERTINENT TO EXTRACTION
Epileptics can have good and bad phases, and exodontia
should be carried out in a good phase, when attacks
are infrequent. Various factors can precipitate attacks.
Those who have infrequent seizures, or who depend
on others (such as those with a learning impairment),
may fail to take regular medication and thus be poorly
controlled. Drugs can be epileptogenic or interfere with
anticonvulsants, or can themselves be changed by
anticonvulsant therapy and may. therefore, be contra-
indicated. One should have comprehensive knowledge
of patient's seizure history and medications. Avoidance
of situations likely to provoke a seizure and PAS complex
by strictly implementing stress reduction protocol. In acute
attack-situation following steps should be taken, terminate
dental therapy and position the patient supine on the
floor, if unconscious.
Protect the patient from injury by passive restraint
in the event of a seizure. Remove him/her from any

Exodontia for Medically Compromised Patients
proximity to sharp edges, a fall or other trauma. Loosen
any tight collar or other clothing.
Lightly restrain, if needed. To prevent any injury to
lips, tongue and to establish a patent airway, following
steps are taken immediately - Turn the patient on his
her side in the dental chair with the head extended. A
well padded tongue blade available is kept in between
teeth. Supplemental O2 may be necessary in worse
conditions. Local anesthetics readily cross the blood-
brain barrier. At low (therapeutic/non-toxic) levels, no
CNS effects are clinically significant. At higherjtoxic/
overdose) levels, a generalized tonic-clonic episode is
seen. Patients on valproic acid may have a prolonged
bleeding time, thus bleeding time should determined
prior to surgery.
ASTHMA
Asthma is a chronic inflammatory disease characterized
by reversible airway obstruction. This disorder is typified
by bronchial edema caused by hypersensitivity to either
known or unknown stimuli and which results in airway-
narrowing. This process is also associated with increased
mucin secretion and diminished ciliary action, further
compounding obstruction.
Asthma is broadly classified by the principle stimuli
that incite an acute episode rather than specific etiologic
parameters. Some classification systems divide asthma
into 2 basic groups: allergic, or extrinsic asthma versus
idiosyncratic or intrinsic asthma.
Other proposed classification systems for chronic
asthma are based on disease severity according to the
frequency of acute attacks. This classification system
divides asthma into mild intermittent, mild persistent,
moderate persistent and severe persistent categories.
Furthermore, such classification based on severity lends
itself nicely to specific treatment approaches for each
category,
Regardless of the various classification systems. The
etiology of asthma is both poorly understood and poorly
defined. Asthma is an inflammatory process associated
with bronchial hyper-responsiveness, bronchial lumen
decreases in diameter because of edema, mucus
production, and hypertrophy of the bronchial wall.
Typical symptoms of asthma include wheezing, chest
tightness, cough, and dyspnea. The frequency and the
severity of asthma symptoms vary among patients and
within individual patient episodes. Physical evaluation
of the patient may reveal expiratory wheezing with or
without expiratory phase prolongation or tachypnea.
In acute asthma flares, use of the accessory muscles of
respiration is also characteristic. Pulmonary function tests,
primarily spirometry, are necessary to establish or confirm
a diagnosis of asthma and assess its severity.
CARE PERTINENT TO EXTRACTION
Optimal asthma control is desirable before dental
treatment. The dentist must also remember that some
medications used in dentistry may have specific
implications in the treatment of a patient with asthma.
Aspirin, as well as other nonsteroidal anti-inflammatory
medications, should be avoided in aspirin-sensitive
persons with asthma because they could trigger an acute
asthma attack. In general, nonsteroidal anti-inflammatory
medications, including aspirin, should be used with
caution in all persons with asthma because these
medications inhibit cyclo-oxygenase and preferentially
generate leukotrienes. Opiates, which cause respiratory,
depression and which can induce histamine release,
should also be avoided. Macrolide antibiotics (e.g.
erythromycin), which alter cytochrome P450. may result
in elevated serum methyl xanthine (theophylline) levels.
In addition, sulfite preservatives, as those found in some
local anesthetics (i.e.. those with vasoconstrictors, such
as levonordefrin and epinephrine), can precipitate asthma
attacks. Other concerns for the dentist include the
requirement of steroid supplementation-before stressful
or perceived stressful dental procedures-in patients with
severe asthma who are on a long-term regimen of
systemic corticosteroids. Proper preparation of the
asthmatic patient before dental therapy may enhance
Exodontia Practice
the dentist's ability to emergently manage an acute
asthmatic attack. Patients should be advised to bring
their short-acting beta agonist inhaler medications to
the dental appointment.
PATIENTS RECEIVING RADIOTHERAPY
Radiotherapy is often used to treat oral cancer. It can
be used alone or as adjuvant to surgical procedure aiming
to treat oral cancer. Many oral complications can follow
radiotherapy involving oral cavity and salivary glands.
Radiotherapy to tumors of the mouth, naso and
oropharynx is especially liable to damage the salivary
glands, depress salivary secretion and result in saliva of
a higher viscosity but lower pH. Salivary secretion
diminishes within a week of radiotherapy in virtually all
patients and the saliva becomes thick and tenacious.
Infections are predisposed to by xerostomia. Caries, oral
candidosis and acute ascending sialadenitis are typical
consequences. Some salivary function may return after
many months.
CARE PERTINENT TO EXTRACTION
Before radiotherapy meticulous oral hygiene should be
implemented. Neglected and unsaveable teeth in the
radiation path should be extracted. An interval of at least
2 weeks between extracting the teeth and starting
radiotherapy is desirable but the time interval permitted
between extractions and radiotherapy is invariably a
compromise because of the need to start radiotherapy
as soon as possible. No bone should be left exposed
in the mouth when radiotherapy begins since, once the
blood supply is damaged by radiotherapy, wound healing
is jeopardized.
After radiotherapy oral hygiene and preventive dental
care should be continued. If extractions become
unavoidable, trauma should be kept to a minimum,
raising the periosteum as little as possible, ensuring that
sharp bone edges are removed, suturing carefully and
giving prophylactic antibiotics in adequate doses from
48 h preoperatively and continued for 4 weeks at least.
Clindamycin 600 mg tds is an appropriate antibiotic since
it penetrates bone well.

Exodontia Practice
General anesthesia (GA) has been one of the far-reaching
inventions of medical science. The use of general
anesthesia in dentistry began in 1844 when Connecticut
dentist Horace Wells first used the chemical compound
nitrous oxide, commonly known as laughing gas. to
relieve pain during a dental procedure. Two years later,
his former partner. William Thomas Morton, introduced
the use of ether as a general anesthetic at a public
demonstration.
Though general anesthesia is an expensive
component of a surgical procedure, recent economic
development in India has widened the scope for
extraction of teeth under general anesthesia. Various
anesthetic agents are available and readers are advised
to refer to appropriate general anesthesia textbook.
It is imperative to understand that though dental
extraction is classified as a minor surgical procedure,
the morbidity and mortality from general anesthesia
still remains same to a large extent. Any complication
from the procedure is there for not well tolerated by
patient. Fortunately most complications are minor but
occasionally respiratory and cardiac arrests will occur.
Proper case selection and precautions can only reduce
these complications but cannot eliminate it from
happening.
INDICATIONS FOR GENERAL ANESTHESIA
1. Anxious patient.
2. Difficult procedure (e.g. very low lying third molar).
3. Pediatric dental extraction in a non-cooperative child.
4. Extraction in people with special needs, e.g. cerebral
palsy, learning difficulties.
CONTRAINDICATIONS FOR GENERAL
ANESTHESIA
Cardiovascular and respiratory diseases are the most
common limiting factors for GA. A detailed questionnaire
is provided to go through when a patient is planned for
G A . Any significant medical problem needs to be
investigated and discussed with the anesthetist. Amount
of exercise tolerance gives a good indication of fitness
for general anesthesia. Finally it is the individual
anesthetist's skill and acute care facilities, which
determines the patient selection.
One of the common reasons for cancellation in day
case procedure is due to non-fasted patients. Patient
needs to be nil by mouth for eight hours. All regular
medication needs to be checked by the anesthetist to
advise on taking them on the day of the operation. Use
of chewing gums or drinking tea/coffee with milk will
stimulate gastric secretion which can regurgitate leading
to aspiration pneumonia which can be fatal.
Dental extractions under GA are routinely carried out
in developed countries. The assessment of these patients
is mainly carried out using American Society of
Anesthesiologists (ASA) grading. Medical co-morbidity
increases the risk associated with anesthesia and surgery.
ASA accurately predicts morbidity and mortality (Table
11.1). In general fifty percent of patients presenting for
elective surgery are ASA grade 1. This number is very
likely to be large in maxillofacial surgery as the age group
of people who have wisdom teeth removed are in a
younger age group and are generally fit and healthy.
Operative mortality for these patients is less than 1 in
10,000.
Table 1 1 . 1 : ASA predicts mortality and morbidity
Any contraindication for extraction under local
anesthesia (apart from those which indicates GA) will
also apply to GA for. e.g. bleeding disorders unless
corrected.
ASA Definition Mortality
Grade (%)
I Normal healthy individual 0.05
II Mild systemic disease that does
not limit activity 0.4
III Severe systemic disease that limits
activity but is not incapacitating 4.5
IV Incapacitating systemic disease
which is constantly life-threatening 25
V Moribund, not expected to survive
24 hours with or without surgery 50

CONSENT
Obtaining an informed consent is an important and
recommended practice of modern day surgery. Though
it is not something routinely carried out in Indian
circumstances due to difference in practice of surgery.
With the increasing health awareness and publicity of
medicolegal issues, informed consent should be incor-
porated in routine practice by explaining the importance
of it to patients.
The extent of warning should involve routine
complications like numbness of tongue and lip following
third molar removal. It is advisable to cover the risks
of GA either separately by the anesthetist or as a team.
It is always advisable to discuss the possible outcomes
and change of plans intraoperatively. for example, it is
advisable to include the adjacent tooth on the extraction
list if it is radiographically carious and found to be beyond
restoration clinically once adjacent tooth is extracted. It
is not a good idea to wake the patient to inform the
changes.
GENENRAL ANESTHESIA AND
CONSIDERATIONS FOR INTRAORAL
PROCEDURE
All intraoral procedures have limited access and presence
of endotracheal tube can only make it more difficult.
The two clinical exercise which should be part of a clinical
assessment for GA are mouth opening and neck exten-
sion. Poor mouth opening is not only a surgical difficulty
but also anesthetic. When there is trismus secondary to
infection and suspected airway compromise as well, the
team should be ready to carry out emergency tracheo-
stomy if needed. The use of fiberoptic guided intubation
technique is more safe and can avoid emergency
tracheostomy. Patients with reduced neck extension
should be discussed with anesthetist before hand.
Technically, blind nasal intubation is more difficult
than placing oro-endotracheal tube. Where good access
is needed, surgeon needs to inform the anesthetist the
requirement of nasoendotracheal intubation. Where
simple extractions are planned, oral intubation using
Portex
K
cuffed oral endotracheal tube-PDT which are soft
and specially engineered for maxillofacial surgery can
be used. They provide enough maneuvering for retraction
using tongue retractors. It is always a good idea to inform
the anesthetist when their position is changed for access.
Laryngeal mask airways are alternative airway
devices which are successfully used in short general
anesthesia. They can be used when there is adequate
access is available and the procedure is short and patient
does not have any contraindication for laryngeal mask
airway like morbidly obese patients or procedures close
to oropharynx.
POSITIONING FOR GENERAL ANESTHESIA
The patient needs to be kept comfortable and any soft
tissue damage by pressure needs to be avoided. These
injuries will be severe as most often they go unnoticed
till patient is awake. Soft cushioning jelly pads are
routinely used. This has a major significance especially
when the routine short procedure is prolonged due to
any complication. Catheterization is not routinely
required.
The layout for anesthetist and his equipment,
operating lights, scrub nurse, operator and assistant needs
to be planned before hand as moving anesthetic machine
or operating table is cumbersome and will delay the
procedure. It is important to move the operating light
whenever patient or operator's position is changed.
POSITIONING OF THE OPERATOR
The positioning of the operator varies individually but
in general it is better to stand on the side of the operation
to enhance access and visibility. Most of the extraction
forceps are designed for patients sitting in a dental chair:
therefore operators need to use non-conventional use
of forceps for patients in supine position during general
anesthesia. For example, the author finds lower anteriors
are some times better accessed from 12 O' clock position
with an upper anterior forceps.

Exodontia Practice
IDENTIFYING THE RIGHT TOOTH
Marking the site of surgery is an integral part of preparing
the patient for theater. Though it is not widely used,
marking the tooth is suggested by some. It is imperative
for the actual surgeon to do an oral examination just
before the surgery. The assistant has to be equally vigilant
to avoid any wrong tooth extraction. Charting the whole
mouth before extraction is a very useful safety technique,
especially when multiple extractions are planned. Marking
the tooth to be extracted on the OPG (which should have
patients name and date of exposure and sides correctly
oriented) and writing it on the board is a safe practice
and reduces the intraoperative confusion, delays and
medicolegal issues. Before applying the forceps or
elevator, the surgeon must re-check the notes. The
importance of preoperative examination cannot be
emphasized enough as symptoms cannot be elicited once
the patient is anesthetized. This also gives an opportunity
to check if the symptoms have resolved or changed
warranting change of treatment plan.
In certain situations where complete clinical
examination is not possible, examination needs to be
carried out along with whole mouth charting. There
should be low threshold for extracting teeth in these
patients as restoration on a later date may not be possible
and further GA may be needed to complete the
extractions. It is important to plan restoration at the same
time where possible to avoid unnecessary distress to
patient.
SURGICAL CONSIDERATIONS FOR GENERAL ANESTHESIA
Surgical procedures under GA need to be planned to
avoid any unnecessary delay or cancellation of
procedures. All equipment needs to be checked and
availability of instruments should be confirmed. Any
special need or equipment should be informed prior hand
to theatre staff. The most important thing is the skill of
the surgeon. He should be skilled enough not only to
carry out the procedure but also to handle any
complications like fractured roots, root in the antrum or
an oro-antral fistula.
Extraction under GA is usually complicated by the
fact that area of airway maintenance by anesthetist and
operating site are very close to each other and co-
ordination between the two is crucial. Standard two towel
draping is recommended. Many surgeons prefer not to
prepare the skin or oral cavity prior to surgery but using
a mouthwash on the ward preoperatively is recom-
mended.
Local anesthesia ( L A ) is mainly used to obtain
adequate postoperative pain control and long acting
agents like bupivacaine is preferred. They usually contain
adrenaline for its hemostatic property. Local anesthesia
is also shown to avoid any tachycardia due to stimulation
of nerve fibers but presence of adrenaline can cause
immediate tachycardia and therefore should be told to
anesthetist prior to injection. Care should be taken not
to dislodge the anesthetic tube while operating especially
where advanced anesthetic machines, which have
sensitive alarms, are not available.
The airway must be protected from any copious
irrigation, fractured tooth, filling and any other debris.
Relying on the endotracheal cuff is not sufficient and
the anesthetist routinely places a throat pack. At the end
of the procedure all extracted teeth and fractured crowns
and fillings, roots, instruments, swabs and needles must
be accounted for. If it is not. immediate bronchoscopy
should be arranged where facilities available or an urgent
chest and abdominal X-ray should be arranged. It is the
surgeon's duty at the end of the procedure to remove
the throat pack and the team needs to record it. You
forget to take it out only once.
Obtaining good access to carry out the procedure
is very prudent. It is advisable to use a mouth prop on
the non-operating side to keep the mouth open. The
tongue needs to be retracted with out damaging the floor
of the mouth mucosa. They should also retract the throat
pack which should be placed beyond oropharynx to
avoid entanglement to high speed burs leading to soft
tissue injury. Cheek retractors need to be in place and
should be held by hand rather than the surgeons gown
to avoid any accidental injury to cheek.

Extraction Under General Anesthesia
It is recommended that surgeon informs the
anesthetist about the proceedings of the surgery so that
they can plan the anesthesia. This will avoid unnecessary
prolongation of the anesthetic time due to muscle
relaxants and other drugs given for longer periods than
needed.
Placing immediate dentures and loose intraoral packs
can be difficult especially if they are ill fitting. They are
potential to obstruct the airway. It is advisable to place
them in when patient is more alert in the recovery when
local anesthetic is still working and tissues haven't swollen.
Small pressure packs used to press on the extraction
socket can come off and obstruct the airway. A long pack
sufficiently hanging outside the mouth which is easily
retrievable should be used and removed once bleeding
has stopped.
Most of the time extraction under general anesthesia
is carried out due to some special needs and stopping
bleeding from their extraction sockets when they are
awake can be very difficult and some times may need
another anesthesia. It is ideal to put sutures and obtain
good homeostasis to avoid an unpleasant complication
of post extraction hemorrhage in a non co-operative
patient. When in doubt, place surgicel in the socket
and horizonthal mattress suture to compress the
socket.
POSTOPERATIVE INSTRUCTION
It is important to provide postoperative instructions
prior to surgery so that patient can make necessary
arrangement and also he will not be in a state to receive
any instruction after a GA in the initial hours. The
language of choice should be the one patient is comfor-
table with.
COMPLICATIONS OF EXTRACTION UNDER
GENERAL ANESTHESIA
Complications of extraction in general are covered in
a different chapter but specific complications arising
mainly under GA are covered here.
Inadvertent force while carrying out extraction under
GA is not uncommon and can result in various compli-
cations. Fractured mandibles are mainly associated
following removal of third molars. Should this happen
the surgeon should proceed directly to fixing the fracture
and fully explain the situation to the patient post-
operatively. It is easy to forget the traction on temporo-
mandibular joint while applying the force. This is only
felt after patient has recovered from anesthesia and can
be very uncomfortable, some times more than the pain
at the surgical site. Supporting the mandible, applying
mouth prop and applying controlled, guided force
reduces the risk of such damage. On completion of treat-
ment, before taking the throat pack out the operator must
ensure that mandible can come to centric occlusion to
rule out TMJ dislocation unless patient is intubated orally.
Soft tissue injury is not uncommon under GA. Most
commonly the angle of the mouth is injured due to
injudicious retraction or friction from the instruments.
Poor access and visibility contributes to the problem.
Copious amounts of skin lubricants/ moisturizing cream
should be applied to lips preoperatively and also
postoperatively. Care should be taken as instruments can
get very slippery due to lubricant coat.
It is important to make sure that autoclave instruments
are cool before being used. Surgical gloves do not
conduct heat well and can give false low temperature
leading to tissue trauma. Eyes should be covered at all
the time as they are exposed to sharp material and high
velocity rotary instruments. Use of cautery for dental
extraction is rare but if needed bipolar cautery is more
advisable to prevent soft tissue injury.
POSTOPERATIVE INSTRUCTIONS
Patient information for removal of teeth under
GA
1. You may not have anything to eat or drink (including
water) for eight (8) hours prior to the appointment.
2. A responsible adult must accompany the patient to
the office, remain in the office during the procedure,
and drive the patient home.

Exodontia Practice
3. The patient should not drive a vehicle or operate any
machinery for 24 hours following the anesthesia
experience.
4. Contact lenses, jewelry, and dentures must be
removed.
POSTOPERATIVE INFORMATION
1. The surgical area will swell and will be more swollen
on the 2nd or 3rd postoperative day.
2. Stiffness of the muscles may cause difficulty in opening
your mouth for a few days
3. You may develop sore throat and ear ache which
are temporary.
4. The corners of the mouth may become dry and crack.
Your lips should be kept moist with cream or ointment.
5. There may be a slight elevation of temperature for
24 to 48 hours. If temperature continues, notify us.
Further information may be added as per- post-
operative instruction following extraction under LA.

26
Exodontia Practice
The healing of wounds is one of the most interesting
of the many phenomena which characterize the living
organism. The ability of damaged tissue to repair itself
is a response of life itself, and within this very process
may lie the final understanding of nature. It is said that
an unhealed wound will eventually result in the death
of the organism. Therefore, wound healing must be
considered one of the primary survival mechanisms from
birth onward. It should be clearly understood that the
healing of a wound is not an isolated, solitary phenom-
enon but actually a very complex series of biologic events.
Classic reviews of this dynamic process are those of Arey
in 1936 and of Schilling in 1968.
Repair of tissue is generally considered to be a phase
of the inflammatory reaction, since it cannot be separated
from the preceding vascular and cellular phenomena
occurring in response to an injury. Healing of all tissues
after injury has an essentially identical pattern, but this
healing may be modified considerably, depending upon
numerous intrinsic and extrinsic factors.
Oral wounds are common, some being sustained
accidentally and others being inflicted by the dentist for
a specific purpose. The unusual anatomic situation of
the oral cavity, the teeth protruding from the bone, the
constant inflammation present in the gingival tissues, the
presence of countless microorganisms in a warm, moist
medium of saliva contribute to modify the healing reac-
tion of the various wounds. It is. these reparative
phenomena and their alterations from the basic pattern
which are discussed in this chapter.
HEALING OF THE EXTRACTION WOUND
A thorough understanding of the phenomenon of
healing of extraction wounds is imperative to the dentist,
since vast numbers of teeth are extracted because of pulp
and periapical infection as well as various forms of
periodontal disease, and there is an ever-present
possibility of complications in the healing process.
A number of careful scientific studies have been carried
out, both on the experimental animal and in the human
being, dealing with undisturbed as well as complicated
extraction wound healing. The healing of an extraction
wound does not differ from the healing of other wounds
of the body, except as it is modified by the peculiar
anatomic situation, which exists after the removal of a
tooth. The healing process to be described here is a
composite of the various studies reported in the literature
and. while minor variations in the time sequence have
been described, the uncomplicated healing of an
extraction wound in the human may be expected to parallel
that described later. Normal human biologic variation
precludes the establishment of a day-to-day timetable
for such healing wounds, the healing process can only
be described as an "average" sequence of events.
IMMEDIATE REACTION FOLLOWING EXTRACTION
After the removal of a tooth, the blood which fills the
socket coagulates, red blood cells being entrapped in
the fibrin meshwork. and the ends of the torn blood
vessels in the periodontal ligament become sealed off.
The hours after tooth extraction are critical, for if the
blood clot is dislodged, healing may be greatly delayed
and may be extremely painful.
Within the first 24 to 48 hours after extraction, a
variety of phenomena occur which consist principally
of alterations in the vascular bed. There are vasodilatation
and engorgement of the blood vessels in the remnants
of the periodontal ligament and the mobilization of
leukocytes to the immediate area around the clot. The
surface of the blood clot is covered by a thick layer of
fibrin, but at this early period visible evidence of reactivity
on the part of the body in the form of a layering of
leukocytes here is not particularly prominent. The clot
itself shows areas of contraction. It is important to
recognize that the collapse of the unsupported gingival
tissue into the opening of a fresh extraction wound is
of great aid in maintaining the clot in position (Figures
12.1A and B).
FIRST-WEEK WOUND
Within the first week after tooth extraction, proliferation
of fibroblasts from connective tissue cells in the remnants
of the periodontal ligament is evident, and fibroblasts
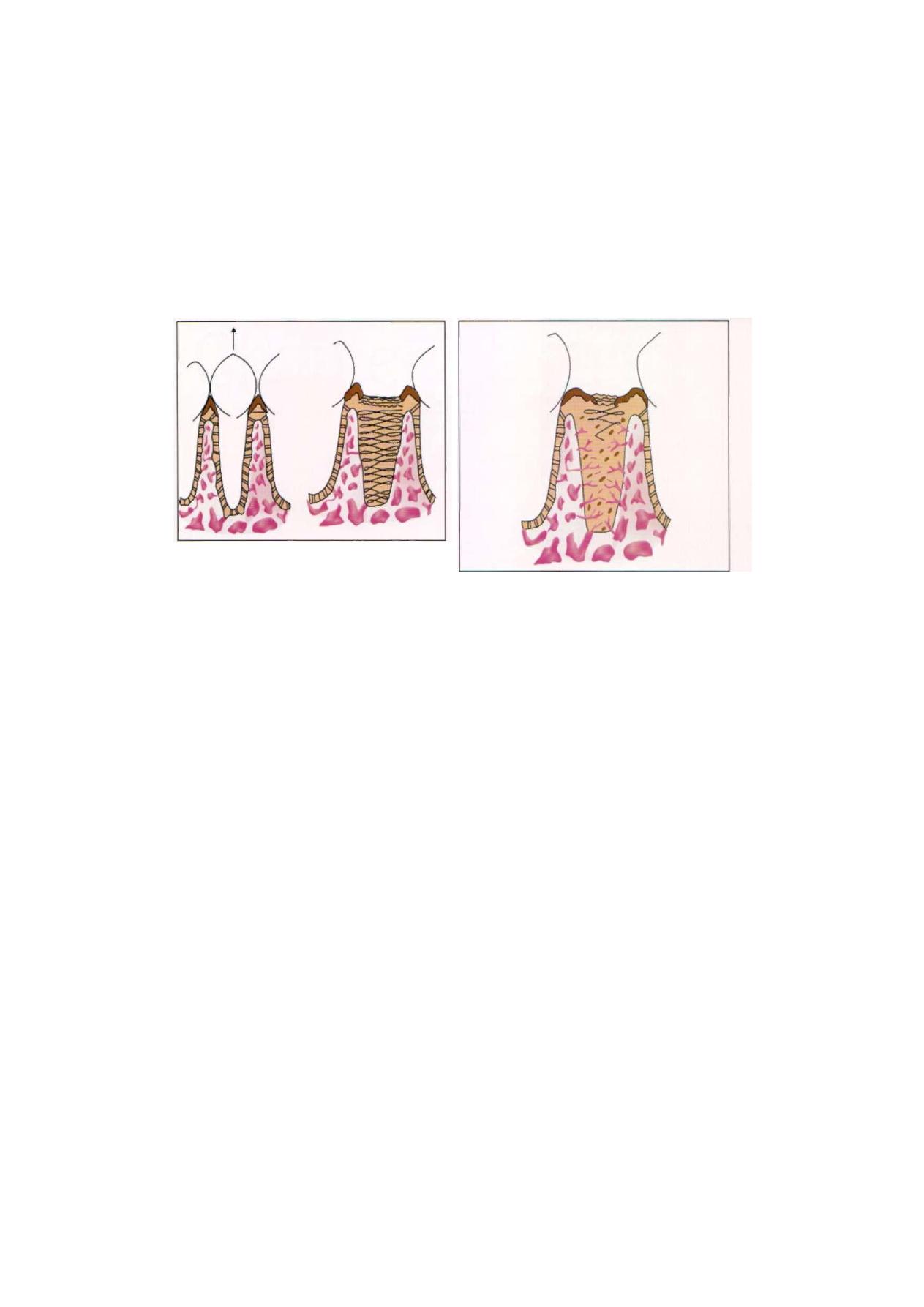
Healing of Extraction Socket
F i g u r e s 12.1 A and B: Tooth socket immediately after
extraction
have begun to grow into the clot around the entire
periphery. This clot forms an actual scaffold upon which
cells associated with the healing process may migrate.
It is only a temporary structure, however, and is
gradually replaced by granulation tissue. The epithelium
at the periphery of the wound exhibits evidence of
proliferation in the form of mild mitotic activity even
at this time. The crest of the alveolar bone which makes
up the margin or neck of the socket exhibits beginning
osteoclastic activity. Endothelial cell proliferation signaling
the beginning of capillary in growth may be seen in the
periodontal ligament area.
During this period, the blood clot begins to undergo
organization by the in growth around the periphery of
fibroblasts and occasional small capillaries from the
residual periodontal ligament. Remnants of this perio-
dontal ligament are still visible, but as yet there is no
evidence of significant new osteoid formation, although
in some cases it may have just commenced. An extremely
thick layer of leukocytes has gathered over the surface
of the clot, and the edge of the wound continues to exhibit
epithelial proliferation (Figure 12.2).
SECOND-WEEK WOUND
During the second week after extraction of the tooth,
the blood clot is becoming organized by fibroblasts
Figure 12.2: First week extraction wound
growing into the clot on the fibrinous meshwork. At this
stage, new delicate capillaries have penetrated to the
center of the clot. The remnants of the periodontal
ligament have been gradually undergoing degeneration
and are no longer recognizable as such. Instead, the
wall of the bony socket now appears slightly frayed. In
some instances, trabeculae of osteoid can be seen
extending outward from the wall of the alveolus.
Epithelial proliferation over the surface of the wound
has been extensive, although the wound is usually not
covered, particularly in the case of large posterior teeth.
In smaller sockets, epithelialization may be completed.
The margin of the alveolar socket exhibits prominent
osteoclastic resorption. Fragments of necrotic bone
which may have been fractured from the rim of the
socket during the extraction are seen in the process of
resorption or sequestration (Figure 12.3).
THIRD-WEEK WOUND
As the healing process continues into the third week,
the original clot appears almost completely organized
by maturing granulation tissue. Very young trabeculae
of osteoid or uncalcified bone are forming around the
entire periphery of the wound from the socket wall. This
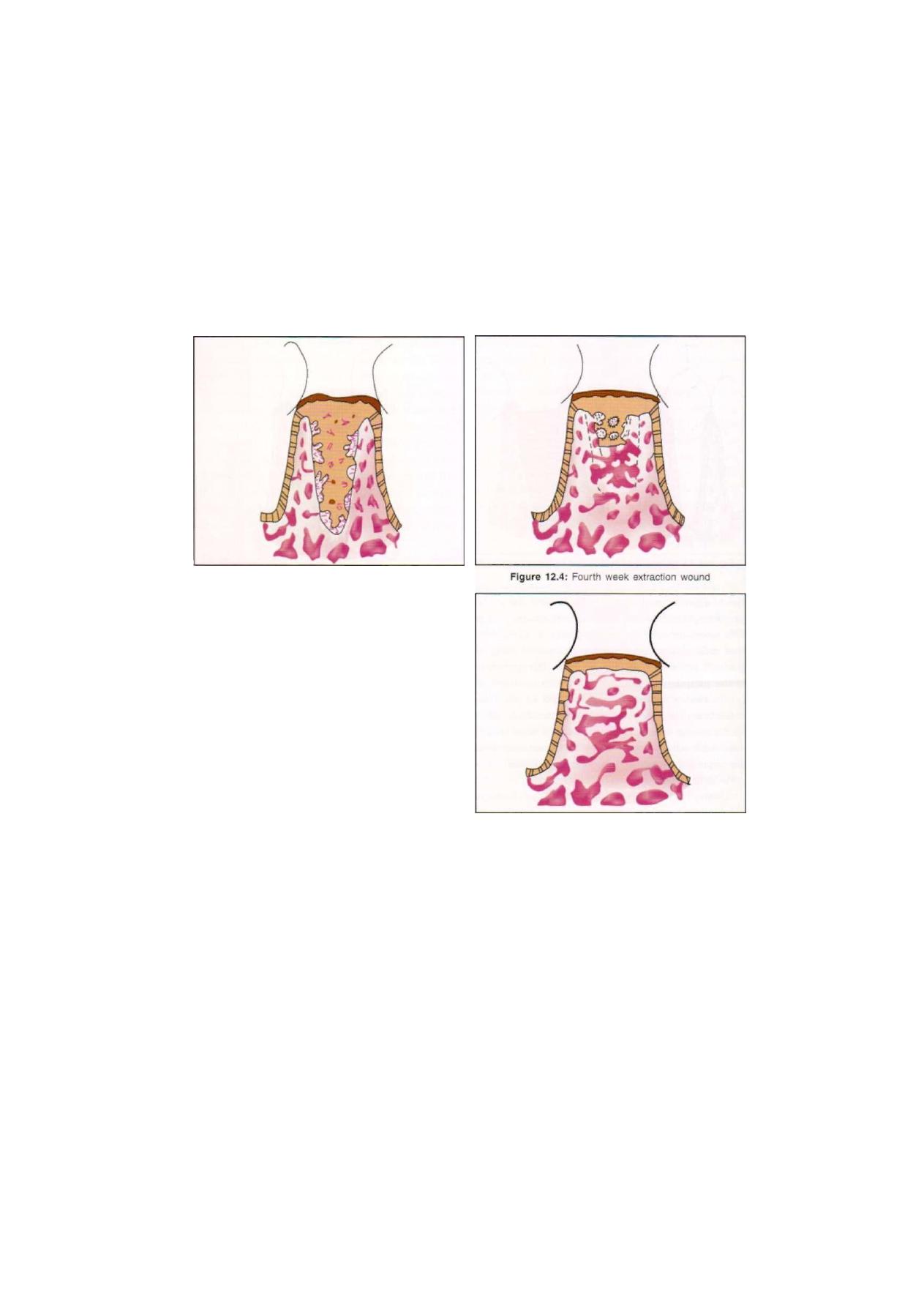
Exodontia Practice
F i g u r e 12.3: Third week extraction wound
early bone is formed by osteoblasts derived from
pluripotential cells of the original periodontal ligament
which assume an osteogenic function. The original
cortical bone of the alveolar socket undergoes remodeling
so that it no longer consists of such a dense layer. The
crest of the alveolar bone has been rounded off by
osteoclastic resorption. By this time the surface of the
wound may have become completely epithelized (Figure
12.4).
FOURTH-WEEK WOUND
During the fourth week after the extraction, the wound
begins the final stage of healing, in which there is contin-
ued deposition and remodeling resorption of the bone
filling the alveolar socket. However, this maturative
remodeling will continue for several more weeks. Much
of this early bone is poorly calcified, as is evident from
its general radiolucency on the roentgenogram.
Roentgenographic evidence of bone formation does not
become prominent until the sixth or eighth week after
tooth extraction. There is still roentgenographic evidence
of differences in the new bone of the alveolar socket
and the adjacent bone for as long as four to six months
after extraction in some cases. Because the crest of
alveolar bone undergoes a considerable amount of
F i g u r e 12.5: Healed extraction socket
osteoclastic resorption during the healing process and
because the bone filling the socket does not extend above
the alveolar crest, it is obvious that the crest of the healed
socket is below that of the adjacent teeth. Surgical
removal of teeth, during which the outer plate of bone
is removed, nearly always results in loss of bone from
the crest and buccal aspects, producing in turn a smaller
alveolar ridge than that after simple forceps removal of
teeth. This may be of considerable significance in the
preparation of a prosthetic appliance (Figure 12.5).
130
Exodontia Practice
No surgical procedure is guaranteed to be free of
complications and tooth extraction is no exception.
Whilst the risk of certain adverse events can be minimized
with forethought at the assessment stage and careful
execution of the surgery, some of the problems that
arise are totally unpredictable.
Any deviation from the normal procedure is called
as complication. Complication at the time of exodontias
can occur at the time of giving anesthesia (anesthetic
complications), at the time of removal of tooth (intra-
operative complication) or after removal of tooth
(postoperative complications). In this chapter we will
discuss intraoperative and postoperative complications.
LOCAL COMPLICATIONS
IMMEDIATE
• Failure of local anesthesia
• Failure to move the tooth
• Fracture of the tooth or root being extracted
• Fracture of the alveolus (including maxillary
tuberosity)
• Oro-antral communication
• Displacement of the tooth or a root into the tissues.
Loss of a tooth or part of a tooth into the pharynx
and then to the lung
• Fracture or subluxation of an adjacent tooth
• Collateral damage to surrounding soft tissues
• Hemorrhage
• Dislocation of the temporomandibular joint
• Fracture of the mandible
• Damage to branches of the trigeminal nerve.
DELAYED
• Excessive pain
• Swelling
• Trismus
• Hemorrhage
• Localized osteitis (dry socket)
• Acute osteomyelitis
• Infection of soft tissues
• Oro-antral fistula
• Failure of the socket to heal
• Nerve damage
• Osteomyelitis
• Osteoradionecrosis.
LOCAL COMPLICATIONS
IMMEDIATE COMPLICATIONS
Failure of Local Anesthesia
Failure of local anesthesia is usually the result of either
inaccurate placement of the anesthetic solution, too small
a dosage, or not waiting long enough for the anesthesia
to act before commencing surgery. Both patient and
operator need to know that the anesthetic is working
satisfactorily before the extraction can proceed procedure
starts. A simple test of adequate numbness is to push
a blunt probe firmly into the gingival crevice around
the tooth for extraction. Whilst the patient will feel the
transmitted pressure from the probe there should be
no sensation of sharpness or pain. An additional caution
is to tap the tooth with a mirror handle as occasionally
there is possibility of periodontitis, and therefore would
be painful to extract, is not detected using the probe
test. If anesthesia cannot be secured by using
conventional techniques of infiltration or regional block,
intraligamental, intraraosseous or intrapulpal injections
may be indicated, provided that the cause of the failure
is not local infection around the tooth. Local anesthetic
should not be injected to infected tissues because of the
risk of spreading the infection.
Failure to Move Tooth
If the tooth does not yield to reasonable displacing forces
applied with forceps or elevators, this normally indicates
that either the bone texture is dense and inelastic, or that
the root shape is obstructing its path of withdrawal. To
apply forceps using even greater force is likely to result
in fracture of the tooth or exhaustion of both the operator
and the patient. The cause of the obstruction should be
findout by taking a radiograph before proceeding to lift

131
Complications of Tooth Extraction
a mucoperiosteal flap and remove bone and/or divide
the tooth as indicated.
Fracture of Tooth
The causes of crown or root fracture are:
• Excessive force applied to the tooth
• A tooth weakened by caries or large restorations.
• Inappropriate application of force resulting from
failure to grasp enough of the root mass or using
forceps with blades too wide to make two point
contacts on the root
• Haste due to impatience or frustration
• Unfavorable root anatomy.
Tooth fracture is an inconvenience, but need not be
a disaster, and it happens to even the most experienced
dentists. The key to managing this potential problem
is to reassess the situation and decide whether to
proceed, or abort the extraction attempt and refer the
patient for oral surgical advice. Inspection of the
fractured tooth shows the likely size and position of the
retained root. If there is no pre-operative radiograph
that shows the whole of the root structure then one
should be taken at this stage. When only the crown has
been removed, it may be possible to reapply root forceps,
but this is unlikely to be productive unless there is a
reasonable amount of root accessible above alveolar
bone level, and the root has already shown signs of
loosening. When the root itself has fractured, retrieval
of the retained portion normally requires a surgical
approach. The operator must assess whether this surgical
task is feasible cooperation of the patient, the facilities
available and his or her level of experience.
Ideally all roots should be removed but some apical
fragments may be difficult or hazardous to pursue
because of the proximity of the inferior dental nerve
or the antral floor. Such small apices are best left in situ
and rarely cause symptoms. In general, a root fragment
of a vital tooth, less than 5 mm in length, can normally
be safely left in the jaws of healthy patients. Larger root
fragments and those with necrotic pulps or periapical
radiolucent areas should be removed, unless the risk of
so doing outweighs the potential gain. If it is decided that
the root can be safely retained, then the patient must
be informed of this eventuality along with a suitable
explanation, and both the retention of the root apex and
the information given to the patient should be recorded
in the clinical notes.
Fracture of Alveolar Bone
Fracture of alveolar bone is a common complication
of tooth extraction, and examination of extracted teeth
reveals alveolar fragments adhering to a number of
tooth. This may be due to the accidental inclusion of
alveolar bone within the forceps blades or to the
configuration of roots, the shape of the alveolus, or to
pathological changes in the bone itself. The extraction
of canines is frequently complicated by fracture of the
labial plate, especially if the alveolar bone has been
weakened by extraction of the lateral incisor-and/or the
first premolar prior to the removal of the canine. If these
three teeth are to be extracted at one visit, the incidence
of fracture of the labial plate will be reduced if the canine
is removed first.
It is advisable to remove any alveolar fragment which
has lost over one-half of its periosteal attachment, by
gripping it with hemostatic forceps and dissecting off
the soft tissues with a periosteal elevator.
Fracture of Maxillary Tuberocity
Fracture of maxillary tuberocity occasionally, during the
extraction of an upper molar, the supporting bone and
maxillary tuberocity is felt to move with the tooth. This
accident is usually due to the invasion of the tuberocity
by the antrum, which is common when an isolated
maxillary molar is present, especially if the tooth is
overerupted. Pathological germination between an
erupted maxillary second molar and an unerupted
maxillary third molar is a rare predisposing cause. When
fracture occurs the forceps should be discarded and a
large buccal mucoperiosteal flap raised. The fractured
tuberosity and the tooth should then be freed from the
palatal soft tissues by blunt dissection and lifted from

132
Exodontia Practice
the wound. The soft-tissue flaps are then approximated
with mattress sutures which evert the edges and are left
in situ for at least 10 days.
If this complication occurs in one maxilla the patient
should be warned that it is liable to complicate a similar
extraction performed on the other side of the mouth.
Only if a preoperative radiograph reveals the possibility,
it is possible to reduce the risk of fracture of the tuberosity
by extracting the tooth by careful dissection.
Fracture of an adjacent or opposing tooth during
extraction can be avoided. Careful preoperative
examination will reveal whether a tooth adjacent to that
to be extracted is either carious, heavily restored, or
in the line of withdrawal. If the tooth to be extracted
is an abutment tooth, the bridge should be divided with
a diamond disk before extraction. Caries and loose or
overhanging fillings should be removed from an adjacent
tooth and a temporary dressing inserted before the
extraction. No force should be applied to any adjacent
tooth during an extraction, and other teeth should not
be used as a fulcrum for an elevator unless they are
to be extracted at the same visit.
Opposing teeth may be either chipped or fractured
if the tooth being extracted yields suddenly to
uncontrolled force and the forceps strike them. Careful
controlled extraction technique prevents this accident.
Under general anesthesia, teeth other than the one
being extracted may be damaged by the injudicious use
of gags and props. The presence of heavily restored
or loose teeth, crowns or bridges should be noted and
brought to the attention of the anesthetist. Such teeth
should be avoided when props or gags are inserted.
If possible mouth gags should not be used. Gags and
props must either be placed under direct vision, or, if
inserted by an anesthetist standing behind the patient,
should be guided into place by the operator.
Fracture of the Mandible
Fracture of the mandible may complicate tooth extraction
if excessive or incorrectly applied force is used, or
pathological changes have weakened the jaw. Excessive
force should never be used to extract teeth.
The mandible may be weakened by senile osteo-
porosis and atrophy, osteomyelitis, previous therapeutic
irradiation, or such osteodystrophies as osteitis defor-
mans, fibrous dysplasia. Unerupted teeth, cysts,
hyperparathyroidism, or tumors may also predispose
to fracture. In the presence of one of these conditions,
extraction should be attempted only after careful clinical
and radiographic assessment and the construction of
splints preoperatively. The patient should be informed
before operation of the possibility of mandibular fracture,
and should this complication occur treatment must
be instituted at once. If a fracture occurs in the dental
surgery, extra-oral support should be applied and the
patient referred immediately to a hospital where facilities
for treatment exist.
Dislocation of an Adjacent Tooth
Dislocation of an adjacent tooth during extraction is an
avoidable accident. Improper application of elevator
may lead to this type of complication. During elevation
a finger should be placed upon the adjacent tooth to
support it and enable any force transmitted to it to be
detected.
Dislocation of the Temporomandibular Joint
Dislocation of the temporomandibular joint occurs
readily in some patients and a history of recurrent
dislocation should never be disregarded. This
complication of mandibular extractions can usually be
prevented if the lower jaw is supported during extraction.
The support given to the jaw by the left hand of the
operator should be supplemented by that given by the
anesthetist or an assistant pressing upwards with both
hands beneath the angles of the mandible.
Dislocation may also be caused by the injudicious
use of gags. If dislocation occurs it should be reduced
immediately. The operator stands in front of the patient
and places his thumbs intra-orally on the external oblique
ridges lateral to any mandibular molars which are

Complications of Tooth Extraction
133
present and his fingers extra-orally under the lower border
of the mandible. Downward pressure with the thumbs
and upward pressure with the fingers reduce the
dislocation. If treatment is delayed muscle-spasm may
make reduction impossible, except under general
anesthesia. The patient should be warned not to open
his mouth too widely or to yawn for a few days
postoperatively, and an extra-oral support to the joint
should be applied and worn until tenderness in the
affected joint subsides.
OROANTRAL PENETRATION
The incidence of oroantral communication after tooth
extraction is probably high but as the number of patients
with residual fistulae is small, the ability of the alveolar
tissues to heal spontaneously is marked.
Predisposing causes of oroantral communications are:
1. The relationship of unerupted teeth and of the roots
of standing teeth to the maxillary sinus. Submerged
premolars or upper first molars at extraction are likely
to produce communication with the antral cavity Tooth
shape anomalies which may produce their own
physical problems of surgical removal. Excessive
deposition of cementum around the roots of the
upper premolar and molar teeth often leads to root
fracture at the time of extraction. Hypercementosis
occurs in relation to lone standing teeth or when teeth
have chronic excessive occlusal loads. Generalized
hypercementosis may be idiopathic in origin, but that
accompanying Paget's disease or even acromegaly
may give insight to the underlying generalized bone
disease. In advanced disease the increase in root size
can be gross and must produce surgical difficulties on
extraction. In a patient with previously undiagnosed
established Paget's disease the writer has
seen excessive extraction force subluxate all the molar
teeth in one quadrant together with their grossly
hypercementosed roots and supporting alveolar bone.
Encroachment of such roots and the altered bone
on the maxillary sinus may distort the anatomical cavity
but produce no other special features.
2. Where the sinus has extended into the alveolus
especially each side of a longstanding molar tooth or
posteriorly enlarged tuberosities.
3. Bulbous or curved roots or bony sclerosis leading to
excessive force being used for an extraction.
4. Loss of periapical bone due to the presence of a
granuloma or an apical periodontal cyst.
5. Dental elevators incorrectly applied either 'blind' or
using vertical instead of transalveolar forces.
6. Surgical procedures performed for the removal of
lesions such as cysts or neoplasm lying in the maxillary
sinus.
Healing of Oroantral Penetrations
An oroantral penetration does not necessarily become
a permanent fistula as a small perforation will often heal
spontaneously. The main factor favoring healing is an
adequate thickness of bone between the sinus and the
mouth, ensuring that the socket is of sufficient depth
to encourage fibrous repair to take place and so keep
antral or oral epithelium separate. Similarly, the smaller
the diameter of the bony deficiency the better is healing.
Infection in or around the socket, or raised air pressures
on one or other side of the wound are detrimental.
When these conditions are satisfactory it can be expected
that granulation tissue, then callus, will seal the wound
and allow it to epithelialize on both the sides.
On occasions the extraction of a maxillary molar will
be accompanied by a fragment of the smooth concave
antral floor, attached between its roots, which may retain
some antral lining confirming the presence of an
oroantral communication. A mouthwash or later a drink
may come down the nose, a free-flow of air and bubbling
between the mouth and nose may be noticed, or
difficulty experienced in smoking or blowing against
resistance. No attempt to prove the presence of a fistula
by probing or other means should be made.
The following measures will assist healing:
Socket Edge Reduction and Simple Suturing
Reflection of the buccal mucosa and reduction of the
bony outer wall of the socket with rongeurs to eliminate

134
Exodontia Practice
part of the buccal root spaces will allow the mucoperios-
teum to fall medially. It may then be sutured to the
palatal side of the socket with horizontal mattress sutures.
This technique does not close the socket opening but
reduces it and helps support clot formation.
Use of a Supporting Pack or Protective Dental Palate
Placing any non-resorbable dressing into the socket
means that healing must occur by secondary intention.
Hemostatic substances such as oxidized cellulose
'Surgical' (Ethicon) or 'Oxycell' (Parke-Davis) are
similarly to be avoided if possible. However, where
support of the clot is required, a short length of 1.5
cm ribbon gauze is folded and soaked in an antiseptic
agent such as Whitehead's varnish or bismuth-iodoform-
paraffin paste (BIPP). It is suspended across ^the socket,
and held in place by prepared loops of sutures crossing
from the palatal buccal mucosa. All packs should be
sutured to the wound edge to prevent their loss. They
are kept in position for 2 weeks and then removed.
A protective dental plate worn for a limited period
may partly prevent food particles being forced into the
socket. When taking impressions for the appliance, the
socket must be adequately protected by a layer of gauze
to prevent impression material being forced into the
sinus. These supportive measures are no substitute for
a good surgical technique but may be sufficient to
prevent a permanent communication.
Nose Blowing and Mouth Washing
Restriction of nose-blowing to avoid raising the air
pressure in the antrum and of mouth-washing to protect
the clot is advised until healing is complete. A suitable
prophylactic antibiotic cover will help to prevent infection.
TREATMENT OF THE ESTABLISHED
OROANTRAL FISTULA
Exposure of the antral cavity to the mouth for any length
of time will expose the sinus to salivary secretions and
contamination with food debris. This will induce chronic
irritative changes in its lining and hence infection, which
will disturb the normal ciliary action and mucous flow
which transfers foreign bodies to the medial antral wall.
Early closure of such a communication is vital, but there
are contraindications to immediate surgery.
The first is the degree of soft tissue damage that has
accompanied the extraction. Macerated and edematous
oral tissue prevents early closure and a decision to leave
the fistula for 3 or 4 weeks may have to be taken,
whereas with minimal trauma to the mucoperiosteum
closure can be performed in the first 48 hours.
The second is infection of the antrum. The success
of all surgical attempts to close an oroantral fistula
depends largely on having a clean sinus with a healthy
mucosa. Wherever there is a history of a previous
chronic sinus infection, the antrum must be radiographed
to assess the state of the lining, including chronic mucosal
thickening or cavity obliteration. Where there is a history
of longstanding disease with chronic mucopurulent nasal
discharge, closure of the fistula must be combined with
an intranasal antrostomy to provide drainage in the
postoperative period.
Where the sinusitis is related to the creation of the
defect and is of shorter duration it may be treated
conservatively, unless widespread polypoidal changes
in the mucosa make it unlikely that it can be improved
by simple measures. Indeed polyps may make irrigation
impossible or uncomfortable.
Fistulae that have been open for weeks will frequently
show a localized hyperplastic polypoidal change imme-
diately surrounding the defect, and metaplastic change
to squamous epithelium may have occurred. This can
be treated by local removal of the affected sinus mucosa
at the time of attempted surgical closure.
Conservative treatment consists of daily antral lavage
through the socket, enlarged if necessary to give suffi-
cient access to allow the patient to perform the irrigation
with warm saline using a bulb syringe. Over 4-6 weeks
the infection should resolve and the communication may
even have closed spontaneously. After this time
epithelialization of the tract will have occurred. Any
attempt at permanent closure must be delayed until the
infection is settled.

135
Complications of Tooth Extraction
Buccal Mucoperiosteal Flap
This surgical approach was first described by Von
Rehrmann (1936).
Most patients will prefer the surgery to be completed
under general anesthesia, though it can be performed
satisfactorily under local anesthesia. Nasotracheal in-
tubation through the nostril of the opposite side gives
an unimpeded intraoral approach and permits a nasal
antrostomy to be performed where necessary. Alternati-
vely, an oral tube taped to the opposite angle of the
mouth is acceptable. Hemostasis and visibility are much
improved by the use of a local vasoconstrictor subject
to agreement with the anesthetist. This is introduced
along the anterolateral wall of the sinus and behind the
zygomatic buttress, being infiltrated freely to separate
fascial planes. A further reduction in bleeding can be
produced by tipping the table to raise the head.
As in all procedures for closure of an established fistula,
the excision of the partially or wholly epithelialized fistulous
tract is imperative. An incision is made with a no. 11 blade.
2 mm outside and encircling the fistulous tract. This should
pass either down to underlying bone or through the bony
defect and into the sinus cavity. The excised tubular tract
is then grasped with fine curved artery forceps and
removed, and as a precautionary measure sent for
histopathological examination. This procedure must lay
bare bone and connective tissue to which the advanced
cheek mucosa and periosteum can unite. It is vital that
where necessary further mucosa is removed palatally to
expose about 3 mm of the bony edge so that the line
of repair will be supported on bone.
From the anterior and the posterior limit of the
excised fistula two divergent buccal incisions pass up
into the vestibule. They are made with the scalpel blade
pressed hard on to bone, to cut through mucosa,
connective tissue and periosteum to a level well above
the attached gingiva. The funnel shape allows the flap
to be advanced palatally between the standing teeth.
The posterior limb is the shorter of the two, and can
be quite short when placed further back in the buccal
sulcus, particularly in elderly patients who have alveolar
resorption. A longer posterior limb will not only make
control of hemorrhage more difficult by involving the
branches of the maxillary artery as they pass forward on
the outside of the lateral antral wall, but the scalpel will
leave the bone surface, and therefore the periosteum,
as it passes into the soft tissues above. Where it is not
possible to make the divergent limbs of equal length,
sufficient laxity is obtained by extending the anterior
incision in a curve forward and upward over the apices
of the teeth. The mucoperiosteal pedicle flap may then
be advanced down and back to meet the palatal mucosa.
A coronal view of the maxilla and the oral soft tissue
shows that the mucosal and periosteal layers separate
at the vestibular fornix so that the mucosa descends to
the cheek while the periosteum continues upwards,
following the anterolateral and buccal aspects of the
maxillary bone above. The flap cannot be advanced
in a palatal direction without sectioning the rigid fibrous
periosteum and so freeing the more elastic mucosa and
submucosal connective tissues to be drawn across the
ridge. To do this the incisions must extend beyond the
vestibular height to allow the flap to be everted and
so expose the periosteum beyond the reflection of the
mucosa. A horizontal cut through the periosteal layer
alone, made in one stroke high up and adjacent to the
maxilla enables the flap to be advanced easily mainly
from its anterior edge over the crest of the alveolar ridge
to a point well palatal to the fistula. IrTits final position
it must lie without tension with the suture line resting
on bone. Sufficient laxity may be provided by digital
stretching after it has been undercut.
The leading alveolar edges of the buccal flap are
trimmed to fit accurately into the area already provided
by excision of the fistula. The advanced pedicle must
also closely contact the adjacent teeth as it passes across
the arch. The edge of the palatal mucosa may be slightly
elevated to allow eversion of the raw edges of the wound
with horizontal mattress sutures. To complete the
procedure the entire incision is repaired with interrupted
sutures and the buccal vertical limbs of the incision are
also loosely closed. All sutures are, unless resorbable,

136
Exodontia Practice
removed after 10 days. As there is a hematoma within
the sinus cavity over the mucoperiosteum that has been
advanced, every effort should be made to prevent
infection. This is done by prescribing the antral regime.
A disadvantage of this repair is the local reduction
in sulcus depth caused by drawing the cheek across the
sulcus. It is most marked in the first week following
surgery. Some 40% of oroantral communications closed
using this method still had sulcus reduction at about
6-8 weeks, but had minimized at 6 months.
Palatal Mucoperiosteal Flap
When the oro antral fistula is related to the palatal side
of the ridge or where buccal procedures have failed
usually because of considerable ridge resorption, a
palatal pedicle flap based on the greater palatine artery
may be lifted and rotated across the arch perhaps to
be attached to the buccal tissues.
The palatal mucosa is firmly fused to periosteum from
which separation is difficult. This makes the palatal flap
thick and inelastic so that it must be made longer than
would appear necessary. Even so, only limited rotation
can be safely performed without twisting the palatine artery
and thus devitalizing the flap. Rotation posterior to the
second molar is not recommended though it may be
used for closing an oro antral or oronasal communication
on the contralateral side of the mouth in this position.
The fistula is dissected out and the mucosa cut back to
expose 4 mm of bone all round the defect. The palatal
margin of the excised fistula is made to coincide with the
lateral edge of the palatal flap. An incision is made along
the mid palatal line from just anterior to the junction of
hard and soft palate and curved laterally toward the
affected side, when it has reached the canine and lateral
incisor region. It then passes back about 4 mm palatal
to the crest of the edentulous ridge or the gingival margin
of the fistula when excised.
The flap is lifted and detached from the palate
anteroposteriorly until it can be rotated laterally to lie
without tension over the fistula. This maneuver can be
helped by removing a small notch bucally. After it has
been trimmed to fit the defect accurately it is sutured
to the recipient area with horizontal mattress sutures
and interrupted sutures secure the line of closure
supported on bone.
The denuded bone anteriorly is then covered by
ribbon gauze soaked in an antiseptic solution. The sutures
are retained for 10 days and the pack for 3 weeks. The
uneven palatal surface regains a very nearly normal
appearance in about 2 months.
The Palatal Island Flap
This plastic procedure dissects out an island of palatal
mucosa but retains its connection to the greater palatine
artery (Brosch 1950). Variations of this technique have
been described by Millard (1962) and Moore and Chong
(1967). By dissecting the greater palatine neurovascular
bundle back to the palatal foramen, some extension can
be provided and the flap can be transferred as a well-
nourished full thickness flap to a palatal or buccal site.
Twisting of the exposed artery is reduced by virtue of
its length but care with manipulation of the vascular
supply is imperative.
Bridge Flap
Other forms of local flap have been used but offer no
greater degree of certainty or ease of procedure than
those already discussed. In the edentulous maxilla a local
bridge of tissue in an area adjacent to a fistula may be
mobilized and moved back to cover it (Kazanjian 1949;
Schuchardt 1953). After excision of the fistulous tract
incisions are placed transversely across the line of the
arch. The length of the bridge of mucoperiosteum is
somewhat limited at its palatal end by the palatine artery
which may not be preserved. It can however be extended
buccally sufficiently to elevate and lift it over the fistula
without tension. It is then sutured to the undisturbed edge
of the mucoperiosteum on the distal edge of the defect.
The bridge must be wider than the bony defect and broad
enough for its margins to be well seated on bone. It
follows therefore that the size of the fistula must be
accurately measured before the incisions for the bridge

137
Complications of Tooth Extraction
are made. The denuded bone of the donor area will
granulate under a pack and later epithelialize.
Gold Foil Technique
It is an attractive conservative measure because it requires
the minimal surgical intervention, can be completed easily
under local anesthesia, and preserves the full depth of
the sulcus. It is advocated primarily for the manage-
ment of very large fistula or those repaired by one of
the other techniques described which have failed
subsequently, and where an immediate, simple, trouble-
free protection for the sinus is required. As for all other
methods it can only be used when the maxillary sinus
is free of infection.
The fistulous tract is excised, or curetted to take away
the epithelial lining and bring the underlying defect into
view when any diseased bone is removed. A linear incision
along the crest of the ridge is extended 1.5 cm anterior
and; posterior to the defect and the oral mucoperiosteum
reflected from around the area for about 5 mm
surrounding the defect. A small oblong piece of gold foil
(24 ct) 35 gauges is placed on the bone to cover the
hole completely, with an overlap of 3 millimeters that
can be tucked under the edges of the mucosal wound
to prevent displacement. The incision is then closed with
interrupted sutures, no attempt being made to oppose
the tissues but leaving an elliptical defect which exposes
the underside of the gold throughout the healing period.
Granulation tissue grows from the wound edges on the
superior antral surface of the inert gold foil and crosses
it to form a bridge. This is said to be complete in most
patients in 3-6 months.
The sutures are removed after 10 days. As healing
progresses the edges of the oral wound recede progressi-
vely to expose the gold foil which in time can be removed
with little difficulty. The oral surface then gradually
epithelializes. The obvious problems are that healing
above the foil cannot be seen and that conventional
repair by one of the other methods may be needed
later.
SUPPORTIVE MEASURES
The postoperative regime will depend on the state of
the antrum found at the surgery and the nature of the
procedure. In general the patient should be advised to
follow the antral regime for the first 10 days after
operation.
DISPLACEMENT OF THE TOOTH OR A ROOT INTO THE TISSDES
This is a rare but potentially serious complication. The
tooth or part of it may be lost under a mucoperiosteal
flap into the lingual pouch through the thin lingual cortex
of bone in the lower third molar region, or into the
infratemporal fossa around the back of the maxillary
tuberosity from the upper molar region. Improper
application of forceps to a tooth or elevating a root
with inadequate access may cause such displacement.
Any root or part of the tooth that is unaccounted for
during extraction should be pursued by taking a further
radiograph of the socket and, if possible, the surrounding
area. The patient should then be referred for further
investigation and management by an oral surgeon.
If a tooth or root is lost from view during the course
of an extraction, it may be in one of the following sites:
• Swallowed into the stomach or inhaled into the lung.
If either of these is suspected the patient should be
sent to hospital for abdominal and chest radiographs.
• Pushed into the antrum.
• Displaced into a soft tissue space.
• Collected inadvertently by the suction apparatus.
• Still in the socket.
COLLATERAL DAMAGE TO SDRROUNDING SOFT TISSUES
A certain amount of disruption to the gingival tissues
around an extracted tooth is to be expected. Some
attached gingiva may need to be dissected free of small
fragments of alveolar bone but such displaced tissues,
like flaps of mucoperiosteum can be replaced with
sutures. However, the incidence of the following modes
of soft tissue injury can be reduced with care and
forethought:

Exodontia Practice
• Gingival tissue lacerated by the forceps blades. Be sure
to place the blades inside the gingival crevice and not
trap the soft tissue against the tooth. This is a particular
danger on the lingual aspect of lower teeth.
• Lower lip crushed against the lower teeth while
extracting resistant upper molars. This is due to
incorrect angulations of the forceps and is more likely
to happen under general anesthesia or when the
patient's lower lip is also anesthetized. Awareness of
this problem is usually enough to prevent it.
• An elevator that slips off the intended point of
application and stabs the tongue, floor of mouth or
the palate. Elevators should always be held with the
index finger down the shank of the handle towards
the tip to act as a 'stop' in case the instrument slips.
HEMORRHAGE
Tooth extraction is a stringent test of hemostasis and
excessive bleeding from the socket occurs not
infrequently even in patients who have no pathological
hemorrhagic tendency. The bleeding may be at the time
of surgery— primary hemorrhage within a few hours
after surgery when the vasoconstriction of damaged
blood vessels ceases-reactionary hemorrhage, or present
up to 14 days post-operatively as a result of infection—
secondary hemorrhage.
All patients should be asked whether they or any
blood relative have a history of excessive bleeding and
full details obtained about relevant previous incidents
particularly following tooth extraction. If a hemorrhagic
diathesis is suspected then the patient should be referred
for investigation by a hematologist. Diseases causing
excessive bleeding may involve abnormalities of:
• Blood clotting, e.g. hemophilia, or more commonly
the acquired complication of anticoagulant therapy.
• Platelet deficiency (thrombocytopenia). Either
because to rapid destruction or failure of production
of platelet.
• Blood vessels.
Precautions to minimize the risk of hemorrhage
include careful handling of the tissues to avoid
unnecessary trauma. Placing a gauze pack over the
socket for at least 10 minutes with the patient applying
steady pressure by biting gently to encourage a blood
clot to form in the socket, and then instructing the patient
not to disturb the clot by avoiding vigorous mouth rinsing
or chewing.
If hemorrhage becomes a problem at the time of
extraction it is essential to have good suction apparatus
available so that clear vision of the operative field is
possible. Injecting further local anesthetic solution
containing a vasoconstrictor can help substantially to
control soft tissue bleeding whilst a horizontal matters
suture is placed across the margins of the socket. A small
oxidized cellulose gauze (Surgicel-Ethicon) placed into
the superficial part of the socket further stabilizes the
forming blood clot at this site. When persistent oozing
is coming from the cancellous bone, this can be stopped
by smearing bone wax into the relevant spaces in the
bone marrow. If all else fails then packing the socket
with gauze soaked in Whitehead's varnish (compound
iodoform paint) is a reliable solution to the problem
but the pack must be removed 10 days later.
When patients return with post-operative hemor-
rhage it is often amidst a flurry of high anxiety and blood
stained dribbling. Sitting the patient down quietly,
cleaning away the blood clots that have formed in the
mouth but evidently not in the socket, and giving
reassurance while the patient bites on a pack placed
accurately over the bleeding area will do much to tackle
the situation. In some cases this may be enough to stop
the hemorrhage. Normally it is helpful to inject local
anesthetic around the socket and then suture its margins
with or without the placement of a pack. The medical
history should be checked along with any drugs that
are being taken, notably any anticoagulant such as
warfarin, although aspirin and non-steroidal anti-
inflammatory drugs have an anti-platelet action and may
sometimes be the cause of significant hemorrhage. If
it is thought that there could be a systemic rather than
a local reason for the bleeding, it may be appropriate
to refer the patient for further investigation. In the case

Complications of Tooth Extraction
139
of hemorrhage that is not controllable by the above
measures, the patient should be sent directly to hospital
for surgical management which in severe cases requires
blood transfusion.
Most patients who return complaining of post-
operative hemorrhage is accompanied by anxious
relatives or friends and it is essential to separate the
patient from these well-intentioned, but unhelpful,
companions. Until the patient has been taken to the dental
surgery and the persons accompanying him asked to
remain in the waiting room, it will be quite impossible
either to reassure or treat him satisfactorily. After seating
the patient comfortably in the dental chair and covering
his clothes with a protective waterproof apron, the dental
surgeon should examine the mouth in order to determine
the site and amount of hemorrhage. Almost invariably
an excess of blood-clot will be seen in the bleeding area
and this should be grasped in a piece of gauze and
removed. A firm gauze pack should then be placed upon
the socket and the patient instructed to bite upon it. If
tannic acid powder is placed upon the portion of the
pack adjacent to the bleeding socket it will help to arrest
the hemorrhage. In most instances it will be advisable
to insert a suture into the mucoperiosteum, under local
anesthesia, to control the hemorrhage. An interrupted
horizontal mattress suture is best suited to this purpose
and should be inserted across the socket as soon as
possible. The object of suturing is not to close the socket
by approximating the soft tissues over it, but to tense
the mucoperiosteum over the underlying bone so that
it becomes ischemic. In the vast majority of cases, the
bleeding arises not in the bony socket but from the soft
tissues surrounding it and is stopped by the procedure
described above. The patient should be instructed to bite
upon a gauze pack for 5 minutes following the insertion
of a suture. Should these measures fail to control the
hemorrhage, either gelatin or fibrin foam may be tucked
into the socket. After the pack has been placed in situ
and an extra-oral support provided, the patient should
be referred to the nearest hospital for further treatment.
The mouth tastes unpleasant after a dental hemorrhage,
but repeated rinsing promotes bleeding and should be
avoided. The oral cavity should be cleaned carefully with
gauze soaked in cold water, special attention being
paid to the tongue. This simple procedure adds greatly
to the patient's comfort.
DRY SOCKET
Dry socket has "plagued oral surgeons since the practice
of exodontia began". It is one of the most perplexing
post extraction complications.
The term 'Dry socket' was first introduced by
Crawford in the year 1896. Other terms describing the
condition include alveolitis sicca dolorosa, fibrinolytic
osteomyelitis, alveolalgia, osteomyelitis syndrome.
Dry socket is a term generally understood to refer
to the delayed onset of severe pain associated with
breakdown of clot. This has been satisfactorily established
in a normal extraction wound.
Etiopathogenesis
It is the subject of debate with the opinions being divided
into two main schools of thought.
The first opinion, i.e. inability to form the clot based
on the presumption that there is an absolute absence
of blood clot or improper blood clot formation.
Second opinion i.e. dislodgement of clot, assumes
initial formation of blood clot which however, is
subsequently lysed and lost, leaving behind the empty
socket. The loss of blood clot from the extraction socket
is probably the most accepted factor because of various
reasons which lead to dry socket.
In most of the cases the clot is lost from the socket
due to patient's carelessness in following postoperative
instructions particularly vigorous and constant mouth
rinsing, constant drink which have bubbling effect
destroys the clot or weaken the adherence of clot to the
socket wall, making it more vulnerable for dislodgement.
Breakdown of the clot due to fibrinolytic mechanism
should be given due consideration. According to Brin's
hypothesis, the fibrin is lysed by plasmin which is an

140
Exodontia Practice
enzyme, acting at neutral pH. A proenzyme plasminogen
is converted to plasmin by the action of activators or
kinases like bradykinin and kininogens, released from
traumatized mucosa, periosteum, bone marrow, and
concentrate in the endothelial cells of blood vessel. Its
release is promoted by variety of stimuli. It may also
come from body fluid or arises in plasma precursors
which are proactivators. Thus this plasmin breaks down
the fibrin network of clot, making the socket dry.
The recent study has shown that the oral anaerobic
bacteria 'Treponema denticola' which is a normal
habitant of oral cavity has fibrinolytic activity. The
enzymes produced by this microorganism have a
plasmin like activity leading to breakdown of clot and
dry socket even in the absence of mentioned firbrinolytic
mechanism. This organism doesn't produce pus,
swelling or redness, since it is an anaerobic infection.
It explains the foetid odor and bad taste associated with
dry socket.
The degree of fibrinolytic activity of common oral
bacteria such as streptococcus hemolytics, staphylococ-
cus, and bacteroides is probably not sufficient to be the
cause of dry socket.
PREDISPOSING FACTORS
Difficulty during Extraction
If more force is used than average to extract the tooth,
it may damage and devitalize the bone of socket wall,
reducing its resistance to infection from Treponema
denticola like organism and increasing the local release
of plasminogen activators.
Site of Extraction
Mandibular extractions are complicated by dry socket
more frequently than maxillary extractions. The
mandible has much dense bone and is less vascular as
compare to maxilla.
Also lower teeth are more difficult to extract and
gravity ensures the mandibular sockets to become
contaminated with food debris.
Sclerotic Jaw Bones
In sclerotic jaw bones and irradiated jaws blood supply
is reduced leading to improper clot formation which is
vulnerable to lysis leading to dry socket.
Vasoconstrictors
Reduced vascularity due to the action of vasoconstrictors
inhibits the vascular component of the inflammatory
reaction and tends to favor the establishment of
infection.
Patient on Oral Contraceptives
The use of oral contraceptives has a significant role in
increasing the probability of dry socket after tooth
extraction. Increased fibrinolytic activity is suspected as
a causative mechanism.
Diagnosis: The diagnosis of dry socket can be confirmed
by gently passing a small probe in the extracted wound,
a bare bone is felt which is extremely sensitive.
Signs and symptoms: Following signs and symptoms
helps for the correct diagnosis of dry socket.
PAIN
After two to five days patient comes with the complaint
of severe pain which is closely localized to the socket,
it may radiate to the ear of the same side or other parts
of the face, but with or without signs and symptoms
of infection such as fever, swelling and erythema. Pain
is exaggerated by contact with food during mastication
and also by air blow or fluids. The pain becomes dull
after some days due to necrosis of tissue in the socket,
which covers the bare bone.
HALITOSIS
The food debris may have accumulated in the socket
which, with the disintegrating clot, produces a foul taste
and smell. Anaerobic micro-organisms Treponema
denticola could be a etiologic agent that produce foetid
odor.

Complications of Tooth Extraction
141
GINGIVAL MARGIN
It is usually swollen and becomes dusky red. The socket
itself is either devoid of clot or contains a brown, friable,
foamy clot which is easily washed out.
After a period of 7 to 14 days granulation tissue lines
the socket and gradually fills it up, often there is no
frank sequestrum of the bone but from time to time
exuberant granulation forms and small pieces of socket
wall or part of the interradicular space separate and are
discharged with the formation of small amount of pus,
due to superimposition.
Treatment
The treatment of dry socket is directed primarily towards
the relief of pain as well as healing of wound and is
divided into following ways:
Local Therapy
When patient reports within first 48 hours after
extraction, the dry socket should be treated as simple
extraction wound in which the necrotic blood clot is
removed gently and after irrigation, fresh bleeding is
induced under local anesthesia and pressure pack is given
with antibiotic cover.
When patient reports after 48 hours, all necrotic
debris should be removed and the socket irrigated with
a warm sterile isotonic saline solution and diluted solution
of antiseptic like Betadine. After irrigation of wound the
socket is gently packed with ribbon gauze painted with
zinc oxide eugenol paste (with minimum eugenol
contents). The ribbon should not be packed forcefully
or tightly to form and cover the base of bone. The pack
should completely obliterate and isolate the socket from
the oral cavity. Dressing can be changed depending upon
the severity of the pain but generally the second dressing
is not required, as initial healing takes place to cover
the raw bone.
Zinc oxide- eugenol dressing protects the bare bone
from irritants like food, saliva etc. and prevents food
debris from accumulating in the socket. Eugenol being
an obtundent relieves the pain by destroying superficial
nerve ending. It also acts as a mild irritant which
stimulates the healing and doesn't cause bone necrosis.
Bone necrosis chances are more if eugenol is more. ZnO
itself works as an antiseptic agent.
Systemic Therapy
Systemic therapy consists of use of systemic antibiotics
and antianaerobic agent like metronidazole for rapid
recovery with local wound care. Analgesics and anti-
inflammatory drugs should be given for relief of pain
and to minimize the inflammatory response.
CONCLUSION
Thus it should be noted that dry socket can be taken
care like local wound care with a suitable material like
ZnO—eugenol dressing. The role of systemic antibiotics
is very limited or only to the extent of preventing the
superinfection. It should never be considered curative
and the patient should not be put on heavy antibiotic
or multiple drugs which are not required.
NERVE DAMAGE
The following branches of the nerve may be at risk during
tooth extraction.The mental nerve can be damaged by
over-extension of releasing incisions in the depth of the
buccal sulcus in the lower premolar region, or by bone
removal encroaching on the mental foramen just below
and between the premolar apices. The affected area of
sensory loss extends over the ipsilateral lower lip and chin.
If the tooth or root is in an intimate relationship with
the inferior dental nerve, damage can be prevented or
minimized only by preoperative radio-graphic diagnosis
and careful dissection. The mental nerve may be
damaged either during the removal of lower premolar
roots or by acute inflammation in the tissues around
it. If the nerve is protected by a metal retractor during
operation, and bone removal is maximal mesially to a
first premolar root and distally to a second premolar
root, impairment of labial sensation will be avoided
altogether or be minimal and transient.

142
Exodontia Practice
The lingual nerve may be damaged either by a
traumatic extraction of a lower molar in which the lingual
soft tissues are trapped in the forceps, or by being caught
up with the bur during the removal of bone. A metal
retractor should be used to protect adjacent soft tissues
from harm whenever a bur is in use.
EXCESSIVE PAIN, SWELLING AND TRISMUS
Some degrees of swelling and discomfort is to be
expected after any surgical procedure: tooth extraction
is no exception. Suitable analgesic medication prescribed
for the patient before the expected onset of pain,
combined with appropriate post-operative instructions
and reassurance, is normally adequate management of
these symptoms. Careful instrumentation and handling
of the tissues during surgery minimizes post-operative
edema by avoiding unnecessary trauma, but other
causes of swelling, such as hematoma formation or
infection, cannot always be prevented.
TRISMUS
Trismus is an inability to open the mouth to a normal
and is commonly seen following extractions, particularly
lower molars. Inflammation and edema may spread
from this region to affect the powerful jaw closing
muscles, masseter and medial pterygoid, which are then
painful when stretched. Severe and progressive trismus
occasionally follows a few days after an inferior dental
nerve block as the result of the development of a
hematoma in the medial pterygoid muscle. The passage
of the local anesthetic needle through this muscle may
unavoidably pierce a small blood vessel and cause some
bleeding between the muscle fibres. Fibrosis of the
hematoma may result in prolonged limitation of mouth
opening unless active stretching exercises are employed.
Trismus due to edema normally resolves spontaneously
with the inflammation but the patient can be made more
comfortable meanwhile by the application of heat to
the affected area.
One of the common complications of an inferior
alveolar block is post injection trismus. This may be
caused by (1) needle track infection, (2) trauma to the
medial pterygoid muscle, or (3) the development of
myofacial pain dysfunction syndrome.
Occasionally there will be a persistent trismus which
has certain characteristics that differentiate it from the
three conditions referred to above.This condition is not
frequently mentioned in the literature, and to suggest
that a conservative approach to therapy may be as
effective as the more radical procedures that have been
advocated by some clinicians.
Campbell, in describing his personal experience with
the condition, expressed his opinion that forced opening
was unnecessary and harmful and that even stretching
exercises should not be used, as spontaneous remission
would occur after several months.
Brown believed that such delay in treatment was
usually not acceptable to patients and that gentle
stretching exercises supplemented by a forced opening
under an anesthetic in some cases was the treatment
of choice.
Berry quoted some unpublished studies in these
patients which led him to believe that the trismus might
be a form of guarding of a damaged structure.
Therefore, he did not advocate forced opening.
The use of reassurance together with jaw-opening
exercises and physiotherapy, in the form of ultrasound,
as an initial measure in all cases. Complete failure to
respond after a period of 3 or 4 weeks from the
commencement of treatment would appear to indicate
that forcible opening might be necessary, but this should
be undertaken only if the patient is unable to persist
with the more conservative method of therapy.
Etiology
Various views exist as to the cause of this condition.
Campbell believed that the problem was due to a
hematoma in the medial pterygoid muscle. As mentioned
earlier, Berry thought that the condition was a form of
"guarding" of a damaged structure. It is true that this
type of phenomenon may occur in the muscles of mas-
tication. The argument against this is the fact that the
trismus does not disappear even if the patient is paralyzed

Complications of Tooth Extraction
143
under general anesthesia. This condition is the result of
a needle piercing a small artery with resultant hematoma
formation, followed by its organization into a band of
tissue in the vicinity the medial pterygoid, is the most
feasible one.
(1) onset of the condition is usually a few days
following the injection (average time, 3 days); (2) once
the trismus begins, it becomes established in about 24
hours; (3) spontaneous pain is unusual, but forced
opening of the jaw causes discomfort; (4) there appears
to be a "mechanical restriction" of opening. (5) in most
with correct conservative management, the condition
will resolve in less than 4 months.
The application of intra-oral heat by means of short-
wave diathermy or the use of hot saline mouth-baths
gives relief in mild cases, but other patients require the
administration of antibiotics or specialist treatment to
relieve their symptoms.
OSTEOMYELITIS
Osteomyelitis is an established infection within bone
tissue. All tooth sockets are bony wounds open to the
contaminated environment of the mouth, it is surprising
that infections of the jaws are not seen more often
following tooth extraction. The excellent blood supply
of the facial bones as well as the immunological and
anti-bacterial activity of saliva is largely responsible for
this effect.
Intense penetrating bone pain, prolonged healing
of the socket, anesthesia of the lower lip and general
malaise are the symptoms of osteomyelitis which, in the
acute phase, may show signs of spreading infection and
fever. If the infection becomes chronic the main features
are suppuration, an indurated swelling, and patchy
radiolucency seen on radiographs of the affected bone.
Treatment of acute osteomyelitis requires a high dose
of an appropriate antibiotic for an extended period,
normally several weeks. In addition to this, chronic
suppurative osteomyelitis demands surgical debridement
of the affected area to remove any sequestra of dead
bone.
OSTEORADIONECROSIS
Osteoradionecrosis is an extremely serious complication
of radiotherapy to the jaws that can be triggered by
tooth extraction. The effect of radiation on the tissues,
especially bone, is to reduce dramatically their blood
supply, and therefore to increase vulnerability
to
infection and failure of normal healing. All teeth in the
anticipated radiation field that may require extraction
should ideally be removed before the patient has
radiotherapy treatment or within a few weeks of it (the
ischemic post-irradiation effects on bone are slowly
progressive over a period of months). If the opportunity
for this preradiation management has been missed and
a patient who has had radiotherapy needs a dental
extraction in an affected part of the jaws, then this should
be undertaken in hospital by an oral surgeon.
TRAUMATIC ARTHRITIS OF THE TEMPOROMANDIBULAR JOINT
Traumatic arthritis of the temporomandibular joint may
complicate difficult extractions if the lower jaw is not
supported. The risk of this unpleasant condition
occurring can be minimized if the operator uses his left
hand correctly and the anesthetist or an assistant steadies
the mandible by holding it under the angtes. If it is known
that the patient has a history of a previous dislocation
of the temporomandibular joint it is a wise precaution
to get him to hold a dental prop tightly between his
teeth on the contralateral side during a dental extraction.
SWELLING
If the soft tissues are not handled carefully during an
extraction traumatic edema may delay healing. The use
of blunt instruments, the excessive retraction of badly
designed flaps, or a bur becoming entangled in the soft
tissues predispose to this condition. If sutures are tied
too tightly postoperative swelling due to edema or
hematoma formation may cause sloughing of the soft
tissues and breakdown of the suture line. Usually both
conditions regress if the patient uses hot saline mouth-
baths frequently for 2 or 3 days.

144
Exodontia Practice
A more serious cause of postoperative swelling is
infection of the wound. No effort should be spared to
prevent the introduction of pathogenic microorganisms
into the wound. If the infection is mild it will often respond
to the application of heat intra-orally by the use of
frequent hot saline mouth-baths. The patient should be
cautioned against applying heat extra-orally because this
increases the size of the facial swelling. A hot-water bottle
applied to the cheek in an effort to relieve pain is a
common cause of gross swelling of the face. If fluctuation
is present the pus should be evacuated before beginning
antibiotic therapy. Any patient with a postoperative
infection severe enough to warrant antibiotic therapy
is best treated at a hospital with oral surgery facilities,
especially if the swelling involves the submandibular and
sublingual tissues.
Collapse in the dental chair may occur suddenly
and may or may not be accompanied by loss of
consciousness. In most instances these episodes are
syncopal attacks or 'faints' and spontaneous recovery
is usual. The patient often complains of feeling dizzy,
weak, and nauseated, and the skin is seen to be pale,
cold, and sweating. First-aid treatment should be
instituted at once and at no time should such a patient
be left unattended. The head should be lowered by
lowering the back of the dental chair. With some designs
of chair the use of this method may be considerable
delay and in these circumstances the patient's head
should be put between his knees after ensuring that his
collar has been loosened. Care should be taken to
maintain the airway and to ensure that the patient cannot
fall out of the chair. No fluids must be given by mouth
until the patient is fully conscious.
If recovery does not occur within a few minutes of
first-aid measures being instituted, the collapse is
probably not of syncopal origin and oxygen should be
administered and medical aid summoned. Careful note
should be taken of both the type and rate of respirations,
and the rate, volume, and character of the pulse. If
circumstances permit, the blood-pressure should be
recorded at intervals.
If respiratory arrest occurs the skeletal muscles
become flaccid and the pupils are widely dilated. The
patient should be laid flat on the floor and his airway
should be cleared by the removal of any appliances or
foreign bodies and by pulling the mandible upwards and
forwards to extend the head fully. The patient's nostrils
should be compressed between the operator's finger and
thumb, and mouth-to-mouth resuscitation should be
performed so that the chest is seen to rise every 3 or
4 seconds. The efficiency of this form of resuscitation is
greatly enhanced if a airway is available and can be
inserted over the tongue. Whilst he is attempting to
remedy respiratory arrest the dental surgeon must check
the carotid pulse and apex beat at regular intervals, for
cessation of breathing may be quickly followed by cardiac
arrest, which is a more serious emergency.
Unless the circulation can be restored and maintained
within 3 minutes of cardiac arrest occurring, irreversible
brain damage may occur due to cerebral anoxia. The
patient exhibits a pallor and greyness, and his skin is
covered with a cold sweat. The pulse and apex beat
cannot be felt and the heart-sounds cannot be heard.
If the patient is a child, the heart will often start beating
again if the sternum is tapped sharply. When an adult
is being treated the patient should be laid flat on his
back on the floor. The dental surgeon places the
heel of his left hand on the lower third of the patient's
sternum. The operator then places his right hand on
the back of the heel of his left hand and presses
downwards rhythmically at second intervals, with
sufficient force to compress the heart between the
sternum and the vertebral column. If an assistant is
present she should simultaneously treat the respiratory
arrest in the manner described a b o v e . When no
assistance is available the dental surgeon should perform
respiratory and cardiac resuscitation alternately for
periods of 20 seconds.

Index
A
A d v a n t a g e s of long flaps 75
A l v e o l a r process of the mandible 26
A l v e o l a r process of the maxilla 22
A v o i d vital structures 74
facial artery 74
lingual nerve 74
mental nerve 74
B
B o n e removal: postage stamp m e t h o d
75
C
C o m p l e t e e x o d o n t i a 62
Complications of tooth extraction 129
fracture of alveolar b o n e 131
fracture of maxillary tuberocity 131
fracture of the mandible 132
dislocation of an adjacent tooth
132
dislocation of the
temporomandibular joint
132
oroantral penetration 133
fracture of tooth 131
local complications 130
failure of local anesthesia 130
failure to m o v e tooth 130
nose b l o w i n g and mouth washing
134
socket e d g e reduction and simple
suturing 133
use of a supporting pack or
protective dental palate 134
Contraindications of exodontia 34
active infections 35
b l e e d i n g disorders 35
diabetes and hypertension 34
medically c o m p r o m i s e d patients 35
patients on steroid therapy 35
pregnancy 35
D
Dental extraction 2
Directions to m o v e teeth for extraction
5 2
mandibular anterior teeth 57
mandibular molars 58
mandibular premolars 58
mandibular teeth 57
maxillary canine 54
maxillary first premolar 54
maxillary second premolar 55
maxillary molar 55
maxillary teeth 52, 53
Stobie's technique 57
E
Exodontia for medically compromised
patients 103
artificial heart valves and transplants
1 0 9
treatment considerations 109
asthma 117
care pertinent to extraction 117
diabetes 104
care pertinent to exodontia 105
epilepsy 116
care pertinent to extraction 116
heart failure 108
care pertinent to extraction 108
hemophilia 113
care pertinent to extraction 114
hyperthyroidism 109
care pertinent to extraction 110
hypothyroidism 110
care pertinent to extraction 110
infective endocarditis 107
care pertinent to extraction 107
patient on e x o g e n o u s steroids 110
care pertinent to extraction 111
patients on heparin 113
patients receiving radiotherapy 118
care pertinent to extraction 118
patients receiving warfarin therapy
111
care pertinent to extraction 112
patients taking aspirin 112
care pertinent to extraction 113
pregnancy 115
care pertinent of extraction 115
systemic hypertension 106
care pertinent to exodontia 106
Extraction of primary teeth 98
contraindications 98
extraction technique for primary
teeth 99
armamentarium 99
general considerations 100
indications 98
indications for extraction of
permanent first molars 99
Extraction under general anesthesia
119
consent 121
contraindications for general
anesthesia 120
indications 120
F
Factors that complicate the extraction
procedure 62
adjacent teeth 65
b o n e 6 4
increased b o n e bulk 65
increased b o n e density 64
periodontal health 64
crown 62
diminished access 65
prosthetic concerns 66
proximity to vital structures 65
roots 62
ankylosis 63
bulbous roots 62
dilacerated roots 64
divergent root 64
hypercementosis 63
multiple roots 62
root canal treatment 63
Functions of sutures 75
coapt w o u n d margins 75
hemostasis 75
holding soft tissue flap o v e r b o n e
75
G
General anesthesia and considerations
for intraoral procedure 121

146
Exodontia Practice
complications of extraction under
general anesthesia 123
postoperative information 124
postoperative instructions 123
identifying the right tooth 122
positioning for general anesthesia
121
positioning of the operator 121
postoperative instruction 123
surgical considerations for general
anesthesia 122
General principles in exodontia 38
basic requirements 38
a g o o d radiograph 38
adequate anesthesia 38
adequate illumination 38
efficient assistance 38
instruments 38
suction apparatus 38
chair position for forceps extraction
3 9
for a mandibular extraction 40
for a maxillary extraction 39
clinical evaluation 38
interpretation of a preoperative
radiograph 39
patient and surgeon preparation 39
placement of fingers during extraction
of mandibular teeth 42
role of assistant during the
extraction procedure 43
role of opposite hand 42
H
Healing of the extraction w o u n d 126
first-week w o u n d 126
fourth-week w o u n d 128
immediate reaction following
extraction 126
s e c o n d - w e e k w o u n d 127
third-week w o u n d 127
!
Important factors for removal of root
p i e c e 86
a g e and general medical condition
of the patient 86
amount of root retained 86
circumstances of the fracture 86
reasons for extraction 86
site of fractured root 86
Indications of exodontia 32
apical p a t h o l o g y 32
dental caries 32
e c o n o m i c considerations 34
esthetics 34
focal sepsis 34
impactions 33
orthodontic reasons 32
m a l p o s e d teeth 32
serial extraction 32
therapeutic extractions 32
periodontal disturbances 32
prosthetic considerations 32
pulp p a t h o l o g y 32
root fragments 33
supernumerary teeth 33
teeth in relation to bony pathology 33
teeth prior to irradiation 33
tooth in the line of fracture 33
Instrument for providing suction 19
Instrument to hold the mouth open 19
Instrument to hold towels and drapes
in position 19
Instruments for controlling hemorrhage
14
Instruments for elevating
mucoperiosteum 13
Instruments for irrigation 19
Instruments for r e m o v i n g b o n e 15
b o n e file 15
bur and handpiece 16
chisel and mallet 15
R o n g e u r forceps 15
Instruments for suturing mucosa 16
n e e d l e 17
n e e d l e holder 16
suture cutting scissor 17
suture material 18
Instruments to grasp tissue 14
Instruments to incise tissue 12
Instruments to r e m o v e soft tissue from
b o n y defects 16
Instruments used for tooth luxation
(elevators) 10
types 10
a p e x o elevator 11
axio elevator 11
cross bar elevator 11
straight elevator 11
winter cryer elevator 11
Instruments used to extract tooth
(dental forceps) 6
mandibular forceps 9
mandibular anterior forcep 9
mandibular c o w horn forceps
10
mandibular molar forcep 9
mandibular premolar forcep 9
universal forcep 10
maxillary forceps 7
maxillary anterior forcep 7
maxillary Bayonet forcep 9
maxillary c o w horn forcep 8
maxillary molar forcep 8
maxillary premolar forcep 7
maxillary third molar forcep 9
M
Management of fractured primary tooth
roots 101
Maxillary molar extractions 100
extraction of mandibular anterior
teeth 101
extraction of maxillary anterior teeth
101
mandibular molar extractions 101
Mechanical principles of elevators 43
lever principle 43
w e d g e 4 3
w h e e l and axle principle 44
P
Pediatric exodontia 93
anesthesia technique 95
local anesthesia 94
mandibular tooth anesthesia 96
preparatory measures 94
types and location of injection 96
Policy for leaving root ( T I P ) fragments
9 0
conditions for leaving root tips in
the socket 90
protocol w h e n leaving behind the
roots 91
roots in edentulous j a w s 91
Postextraction care 44
Prevention of flap dehiscence 74
Prevention of flap necrosis ( b l o o d
supply of flap) 74
Principles of flap design 66
flap reflection 69
incision 66
instrumentation 69
types of flaps 71
e n v e l o p e flap 71
four cornered flap 72
release incisions on the facial
aspect of crown 72
three cornered/triangular flap 71
Procedure for closed extraction 46
general steps 46
adaptation of the forceps to the
tooth 47
application of forces to the tooth
with the forceps 49

I n d e x
147
loosening of soft tissue
attachment from the tooth 46
luxation of the tooth with a
dental elevator 47
removal of the tooth from the
socket 51
R
R o l e of assistant during extraction 52
R o l e of the opposite hand 51
S
Socket toilet 79
I
Technique for o p e n extraction of
multirooted tooth 78
mandibular first molar 78
maxillary molars with divergent
roots 78
Technique for o p e n extraction of
single rooted tooth 77
Technique for removal of small root
tips 86
application of an elevator 89
b o n e r e m o v a l 8 9
closed technique 87
forcep r e m o v a l 87
o p e n technique 8 8
Tooth sectioning 76
Treatment of the established oroantral
fistula 134
bridge flap 136
buccal mucoperiosteal flap 135
collateral d a m a g e to surrounding
soft tissues 137
dry socket 139
etiopathogenesis 139
excessive pain, swelling and trismus
142
gingival margin 141
treatment 141
g o l d foil technique 137
h e m o r r h a g e 138
nerve d a m a g e 141
osteomyelitis 143
osteoradionecrosis 143
palatal island flap 136
palatal mucoperiosteal flap 136
predisposing factors 140
difficulty during extraction
140
patient on oral contraceptives
140
sclerotic j a w b o n e s 140
site of extraction 140
vasoconstrictors 140
supportive measures 137
swelling 143
traumatic arthritis of the
temporomandibular joint
143
trismus 142
etiology 142
Exodontia Practice
Dr Abhay N Datarkar earned his BDS and MDS degree at Govt.
Dental College and Hospital Rashtra Sant Tukdoji Maharaj Nagpur
University. He also has an honour of being the First Diplomat of
National Board in Central India.
A meritorious student throughout his career, a recipient of Gold
Medal award of Nagpur University and Best student of Nagpur
University award in 1996. He has various scientific presentations and publications
to his credit in various national and international conferences and journals.
He is a natural teacher, excellent academician and a surgeon par excellence.
He is known amongst his colleagues and students for his inestimable calm,
professional competence, unalloyed guidance, elucidatory suggestions and
ineffable surgical wisdom.
Rs. 795.00
JAYPEE BROTHERS
MEDICAL PUBLISHERS (P) LTD.