Echinococcosis
By
Dr. Ameer kadhim Hussein.
M.B.Ch.B. FICMS (Community Medicine).
Introduction
Species under genus Echinococcus are small tapeworms of
carnivores with larval stages known as hydatids
proliferating asexually in various mammals including
humans.
There were five morphologically distinct species in this
genus including:
E. granulosus, E. multilocularis, E. oligarthus, E. vogeli
and Echinococcus shiquicus.

Ehinococcosis due to Echinococcus
granulosis
(Cystic echinococcosis or cystic
hydatid disease)
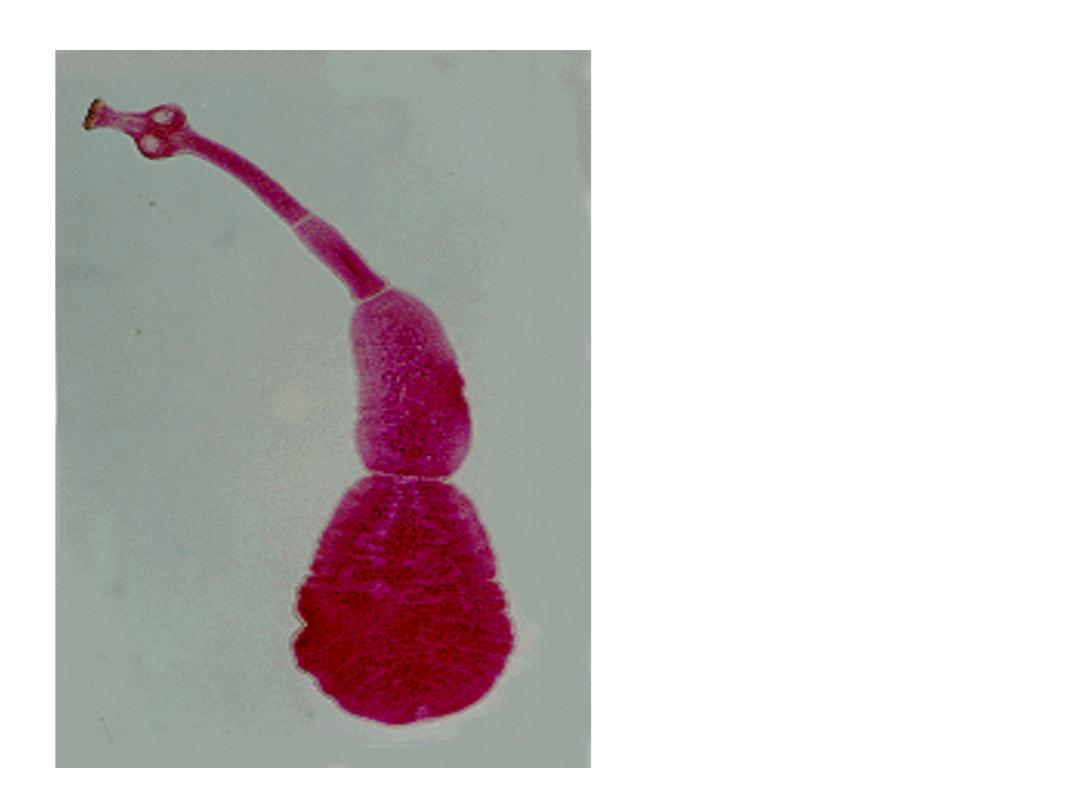
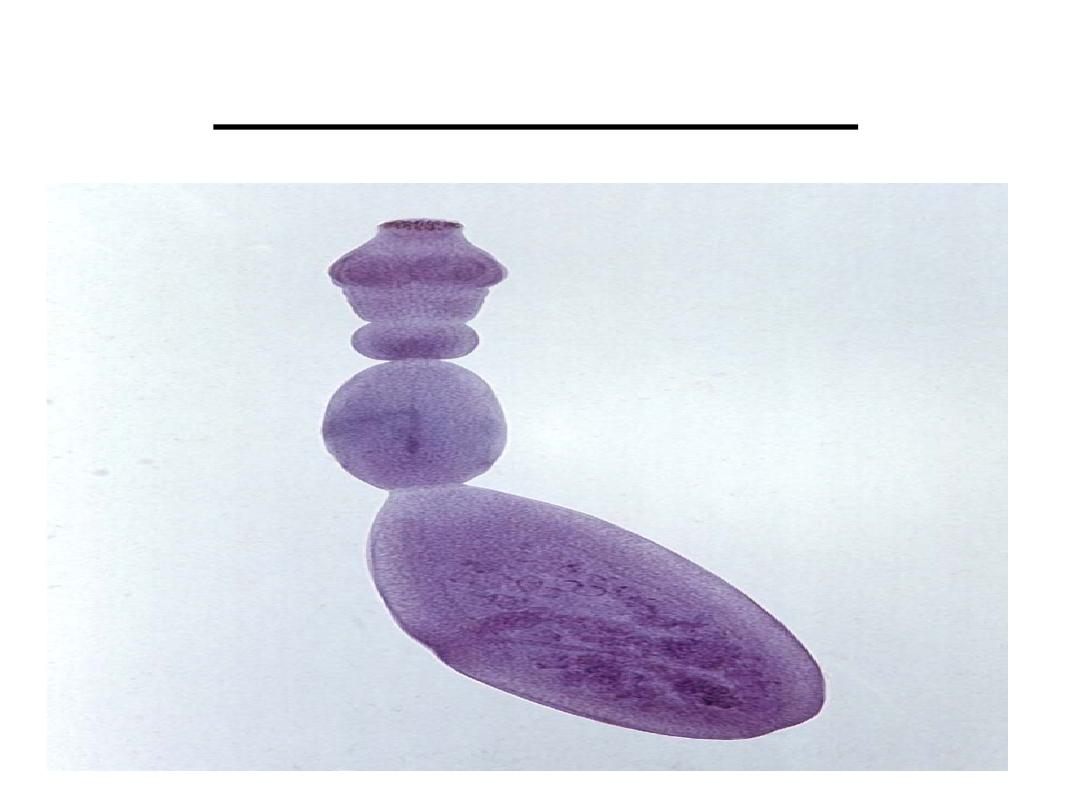
Echinococcus
granulosus
Identification
It is larval stage of the tape worm Echinococcus granulosus.
It is the most common Echinococcus cause hydatid disease.
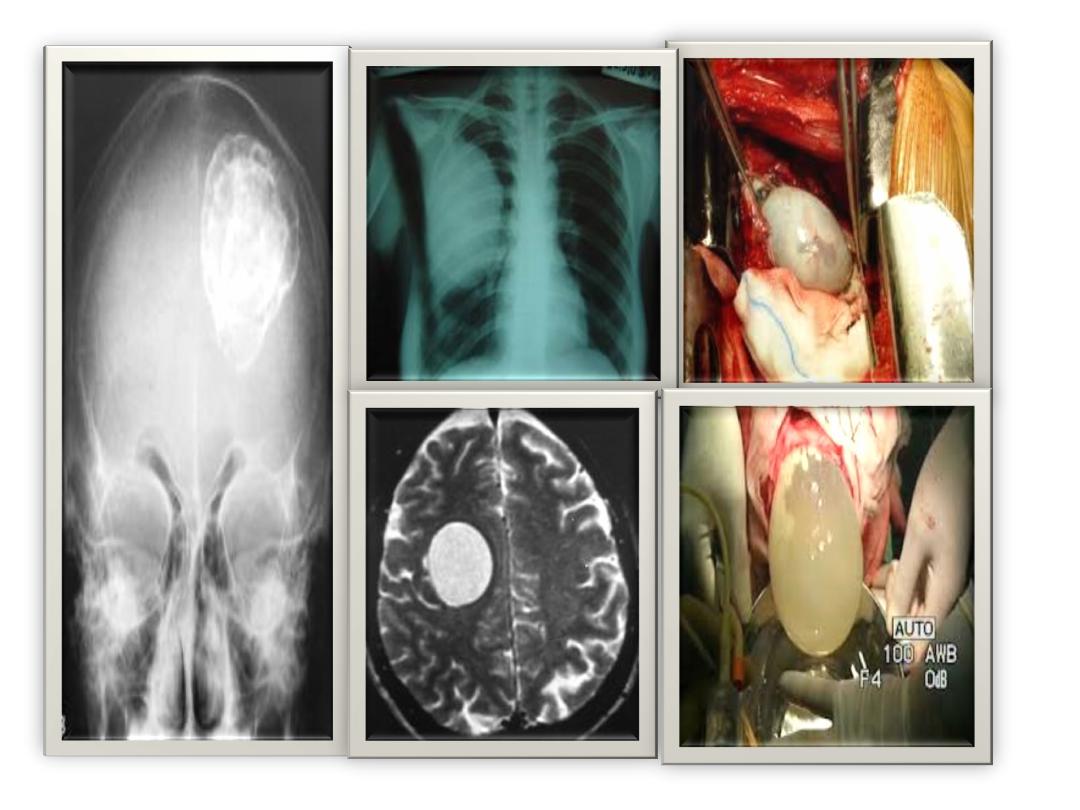
Hydatid cysts enlarge slowly and required several years for
development.
The cyst range from (1-15 cm) in diameter but may be larger.
Infections may be asymptomatic until cysts cause noticeable
mass effect.
Signs and symptoms vary according to cyst location, size, type
and numbers.
Infectious agent:
Echinococcus granulosus, a small tapeworm of dogs and
other canids.
Occurrence:
All continents except Antarctica depend on close
association of humans and infected dogs especially
common in grazing countries where dogs eat viscera
containing cysts. In endemic regions, human incidence
rates for cystic echinococcosis can reach greater than 50 per
100 000 person-years, and prevalence levels as high as 5%–
10% may occur in parts of Argentina, Peru, East Africa,
Central Asia and China.
Reservoir:
The domestic dog and other canids which are definitive
hosts for echinococcus granulosus which may harbor
thousands of adult tapeworms in their intestines without
sign of infection. Intermediate hosts include sheep, goats,
pigs, horses and other animals. Humans also regard as
intermediate host.
Incubation period:
12 months to years depending on number and location of
cysts and how rapidly they grow.
Period of communicability:
Not directly transmitted from person or from one intermediate
host to another. Infected dogs begin to pass eggs (5-7) weeks
after infection. Most canine infections resolve spontaneously
by 6 months however some adult worms may survive up to 2-
3 years. Dogs may become infected repeatedly.
Susceptibility:
Children who are more likely to have close contact with
infected dogs and less likely to have adequate hygienic habits
so have more risk of infection.
Mode of transmission:
Human infection often take place directly with hand to mouth
transfer of eggs after association with infected dogs or
indirectly through contaminated food, water, soil or fomites.
In some instances flies have dispersed eggs after feeding on
infected feces.
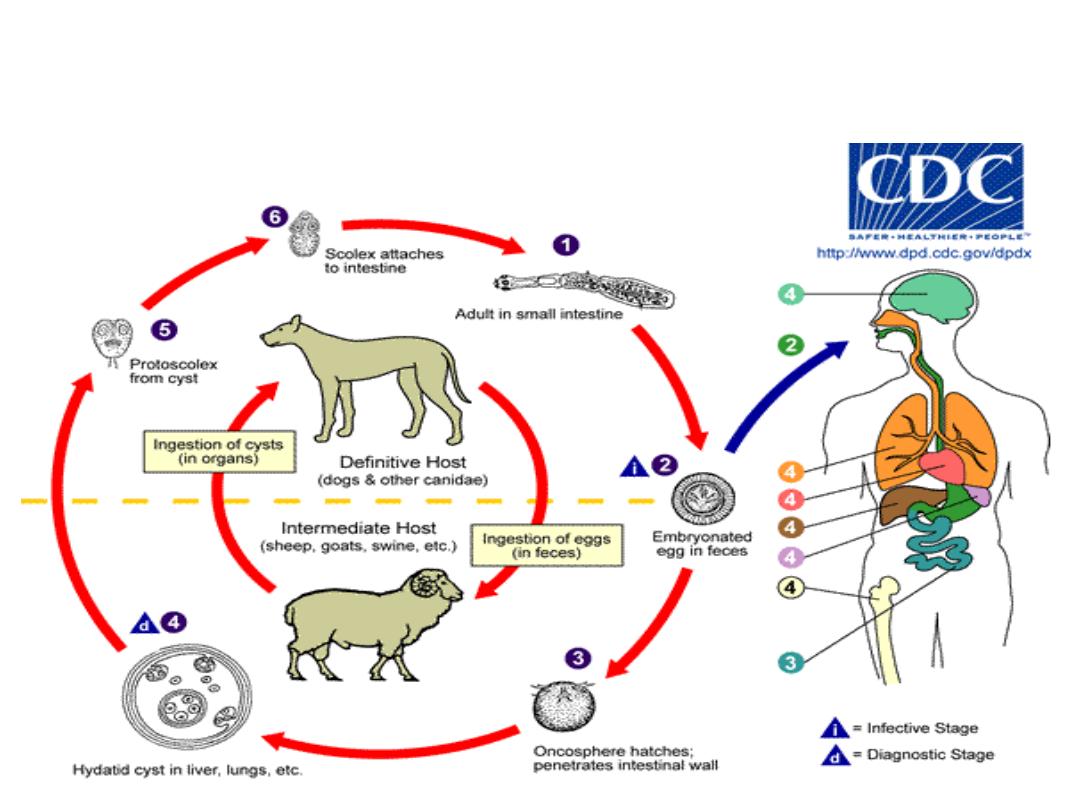
Life cycle of Echioncoccus granulosus
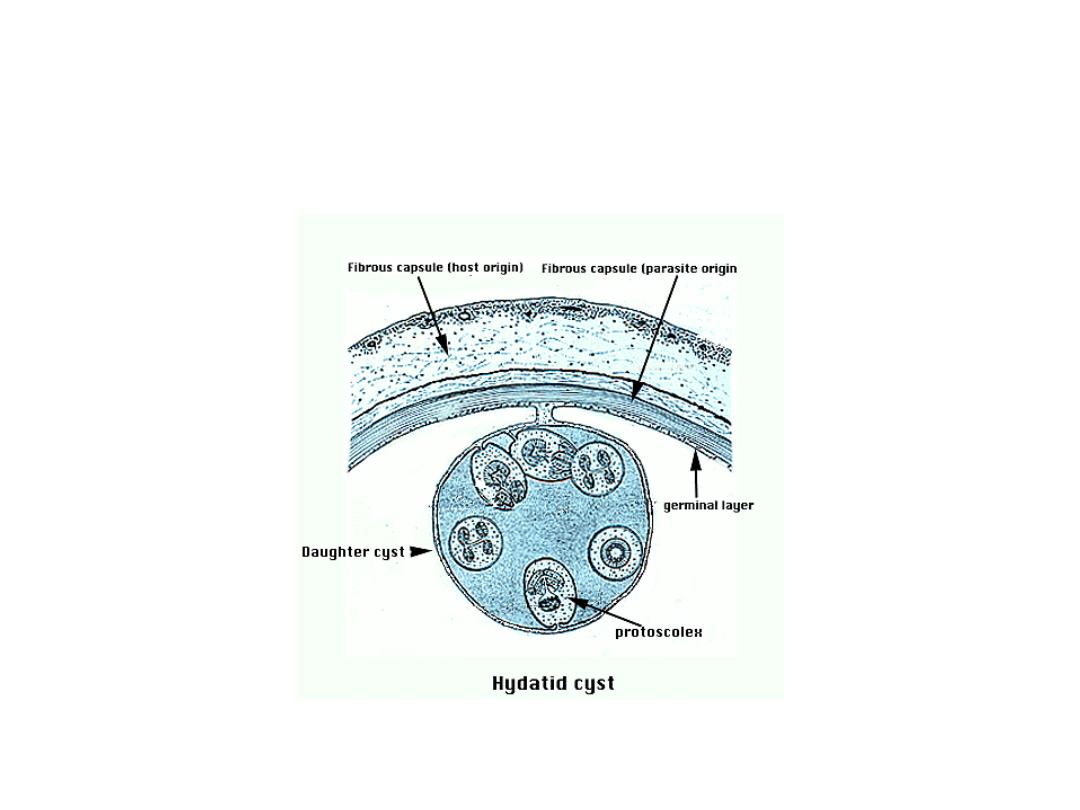
Cyst layers and contents
Methods of control
a. Preventive measures:
1
. Avoid ingestion of raw vegetables and water that may have been
contaminated with feces of infected dogs. Application of hygiene
practices such as hand washing and washing of fruits and vegetables.
Educate those at high risk to avoid exposure to dog feces and
possibly infected dogs.
2.Interrupt transmission from intermediate to definitive hosts by
preventing access of dogs to potentially contaminated and uncooked
viscera. Disposal of viscera should be by incineration or by deep
burial.
3. Periodically treat high risk dogs and all dogs in high risk area.
4. Field and laboratory personnel must observe strict safety
precautions to avoid ingestion of tapeworm eggs.
Control patient, contacts and immediate
environment
1. Report to local health authority.
2. Isolation, concurrent disinfection, Quarantine and
immunization of contacts : Not applicable.
3. Investigation of contacts and source of infection:
Examine families for suspected cysts by using ultrasound,
chest x-ray and other imaging techniques. Check dogs in
and around houses for infection.
Determine beliefs, practices and behaviors increase risk of
infection.
Specific treatment:
must be based on WHO classification of liver cysts usually
surgical intervention is a common treatment.
Other cysts types treated by percutaneous techniques such
as PAIR ( Puncture, Aspiration, Injection, re-aspiration).
Treatment with mebendazole and albendazole has proved
successful and may be preferred treatment in many cases.
If primary cyst ruptures praziquentel and Protoscolicidal
agent reduce risk of secondary cysts.
Other cyst types may not need sugical, percutaneous or
medical intervention and can follow for long time by (wait
and watch).
Echinococcosis due to
Echinococcus multilocularis
(Alveolar echinococcosis)
Echinococcus multilocularis

Identification:
A highly invasive destructive disease caused by the larval stage
of echinococcus multilocularis.
Lesions usually found in the liver but because their growth is
not restricted by a thick laminated cyst wall they may expand to
periphery to produce solid tumor like masses. Metastases can
result in secondary cysts and larval growth in other organs.
Clinical manifestations depend on the size and location of cysts
but are often confused with hepatic carcinoma and cirrhosis.
The disease is often fatal although spontaneous cure and
calcification has been observed.
Diagnosis is often based on histopathology. Sero-diagnosis
using purified E. multilocularis antigen is highly sensitive and
specific.
Staging and classification system recently proposed by
WHO named PNM is based on:
a. Hepatic location of the parasite (P).
b. Extra – hepatic involvement of neighboring organs (N).
c. Metastases (M).
Infectious agent: Ehinococcus multilocularis.
Occurrence: Distribution is limited to areas of the
Northern Hemisphere (China, Turkey, Canada, Central
Europe, Russia …etc). The disease is usually diagnosed
in adults.
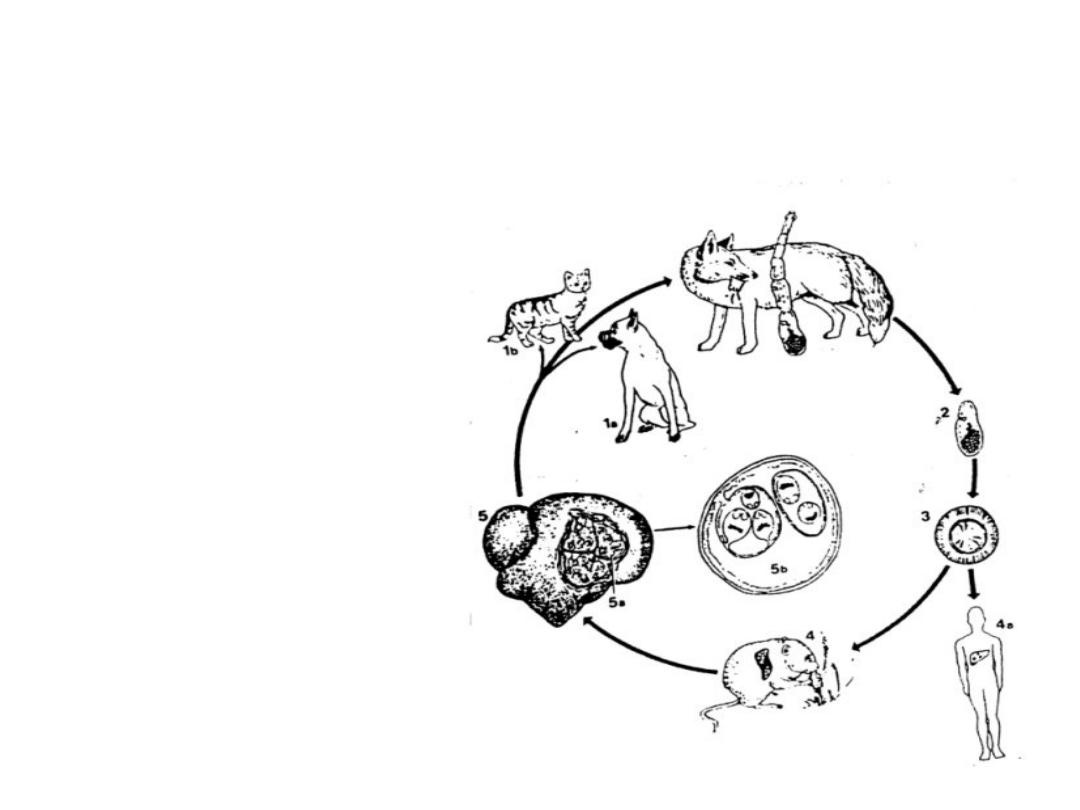
Life Cycle of E. multilocularis
The life cycle is
basically the same
of E.
granulosus
except there are
different definitive
and intermediate
hosts.
Reservoir:
adult tape worms are largely restricted to wild animals such as foxes
and E. multilocularis is commonly maintained in nature of fox-
rodent cycles. Dogs and cats can be sources of human infection if
hunting wild intermediate hosts such as rodents.
Mode of transmission:
Ingestion of eggs passed in the feces of canidae and felidae that have
fed on infected rodents . Fecally soiled dog hair, and environmental
fomites also serve as vehicles of infection.
Incubation period, period of communicability,
Susceptibility and methods of control: as for E.
granulosus.

Radical surgical excision is less often successful and must
be followed by chemotherapy.
Mebendazole or albendazole use for a limited period after
surgery or long term for inoperable patients which may
prevent progression of the disease.
Pre-surgical chemotherapy is indicated in rare cases.

Echinococcosis due to
E. Vogeli and E. Oligarthrus
(polycystic and unicystic echinococcosis)

This disease occurs in the liver, lungs and other viscera.
Symptom vary depending on cyst size and location. This
species is distinguished by its rostellar hooks. This species is
unique in that the germinal membrane proliferate externally to
form new cysts and internally to form septae that divide the
cavity into numerous microcysts.
Brood capsules containing many protocolices develop in the
microcysts.
The causal agents are E. vogeli and E.oligarthrus occur in
Central and South America.
Immuno-diagnosis using purified antigen of E. Vogeli does not
always allow differentiation from alveolar echinococcosis.
Albendazole has been used for chemotherapy.

Summary
Human echinococcosis is a parasitic disease caused
by tapeworms of the genus
Echinococcus
.
The 2 most important forms of the disease in humans
are cystic echinococcosis (hydatidosis) and alveolar
echinococcosis.
Humans are infected through ingestion of parasite
eggs in contaminated food, water or soil, or through
direct contact with animal hosts.
Echinococcosis is often expensive and complicated to
treat, and may require extensive surgery and/or
prolonged drug therapy.

Summary
Prevention programmes involve deworming of dogs,
improved food inspection and slaughterhouse hygiene,
and public education campaigns; vaccination of lambs is
currently being evaluated as an additional intervention.
More than 1 million people are affected with
echinococcosis at any one time.
WHO is working towards the validation of effective
cystic echinococcosis control strategies by 2020.