Medicine
Dr. Samar
•
Feeding oral or enteral tube feeding preferred to parenteral
rout less complication, enhance GIT integrity.
•
Food: small amount frequent interval every (1 – 4) hours to
avoid hypoglycemia.
•
Salt should be restricted and the micronutrients supplements
may be essential.
Treatment:
o
Fluids & electrolytes before feeding.
o
Vitamins supplement.
o
Worm blanket to rise core of temperature.
Refeeding aim:
Prevent further deterioration and correct life threatening
abnormalities.
!
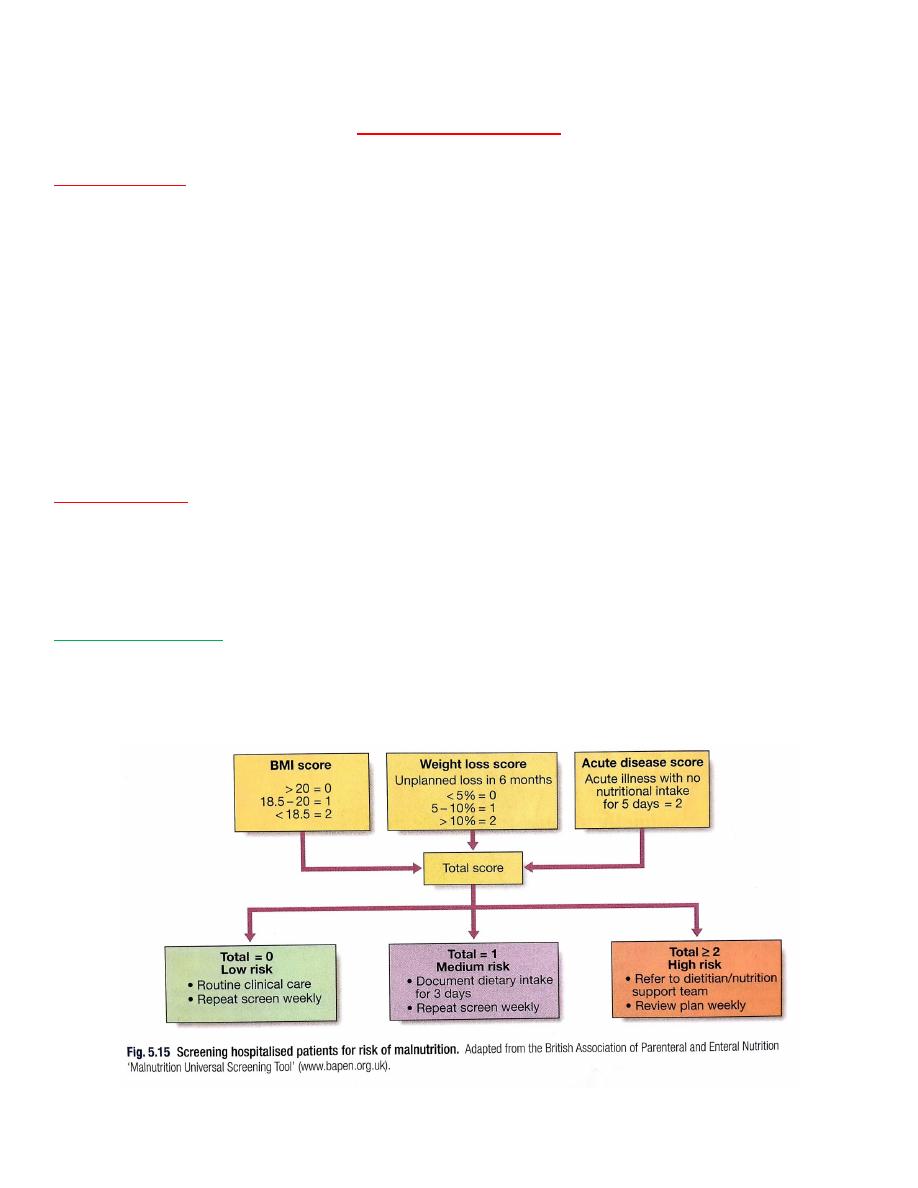
Malnutrition in the hospital:
➢Elderly.
➢Poor appetite and poor dental health.
➢Concurrent illness.
➢Nil by mouth.
➢Impaired immunity, apathic, affect on cooperation and
response to the treatment.
➢Delayed wound healing after surgery with increased risk of
post-operative infection.
Nutrition Support Of Hospital Patient:
Normal Diet:
▪ Encourage to eat normal and adequate diet: inadequate food
due to inability, culture, religious, arthritis stroke, immobility
in bed or poor oral health.
▪ Regular food chart for patients who are in risk of under-
nutrition quantities.
Dietary Supplement:
Patient unable to achieve sufficient nutrition intake by
normal diet alone.
Drinks, high energy and protein content: in carton with
flavored products or made in the hospital kitchen from milk
products and eggs.
Enteral Tube Feeding:
❖
Unable to swallow normally.
❖
Acute stroke.
❖
Throat surgery.
❖
Long neurological problems.
❖
Short term: fine-bore nasogastric tube.
❖
Continuous infusion, bolus technique.
❖
Long term: PEG (percutaneous endoscopic gastrostomy).
Parenteral Nutrition:
•
IV feeding: if enteral feeding is impossible.
•
Peripheral venous cannula: low osmolality.
•
Peripheral inserted cannula: 20 cm cannula in mid-arm vein.
•
Peripheral inserted central catheter: 60 cm antecubital fossa,
the distal end lies in a central vein allowing hyperosmolar
solutions to be used.
•
Central line: the subclavian rout is preferred to the internal
jugular vein due to lower infection rates. Hyperosmolar
solutions can be used without difficulty. Lines need to be
handled with strict aseptic technique, and a single lumen tube
is preferred to prevent the infection.
•
The solution contains: amino acids, lipid emulsion,
electrolytes, trace elements and vitamins.
Blood monitoring:
➢Daily: urea, electrolytes and glucose.
➢Twice weekly: liver function tests, calcium, phosphate and
magnesium.
➢Weekly: full blood count, zinc & triglycerides.
➢Monthly: copper (Cu), selenium (Se) & manganese.
If the patient develops fever or other features of septicaemia, it
should be assumed to be a line infection and blood culture
should be taken.
Refeeding complications (Syndromes):
▪ Fluid over load.
▪ Electrolytes imbalance.
▪ Glucose intolerance.
▪ Cardiac arrhythmia.
▪ Death.
▪ GIT dysfunction.

Ethical and legal considerations:
❖
Competent adult patient give consent for the invasive
procedures.
❖
Patient wishes.
❖
Family view.
Printed By: Ahmed Riyadh