Fifth Stage
Orthopedics
Dr. Haider – Lecture 4
1
Complications of fractures
There are pathologies other than the loss of bone continuity which either co exist
or originate due to the fracture.
Early diagnosis and aggressive treatment is necessary to minimize disabilities.
Complications:
—
Immediate
—
early
—
Late
Immediate complications
•
Systemic
•
hypovolaemic Shock
•
local
•
1.major vessels injuries
•
2. Muscles and tendons injuries
•
3. Joints injuris
•
4. Visceral injuries
Early complications
•
Systemic
•
ARDS
•
Fat embolism
•
DVT & pulmonary embolism
•
Tetanus
•
Gas gangren
•
Crush syndrome
•
local
•
infection
•
Compartment syndrome
2
Late complications
—
Delayed union
—
Mal union
—
Non union
—
Avascular necrosis
—
Shortening
—
Joint stiffness
—
Sudeck’s astrophy
—
Osteomyelitis
—
Ischemic contracture
—
Myositis ossificans
—
Degenerative arthritis ( osteoarthritis )
Hypovolaemic shock :
—
Commonest cause of death in fractures of major bones Like pelvis or femur
—
Exteral or internal bleeding and veceral injuries are the main causes of shock.
—
Fracture femural shaft = 1 – 1.5 L of blood
—
Fracture pelvic ring = 1.5 – 2 L of blood
—
Treat the cause , start IV fluid and blood , stabilize the fracture.
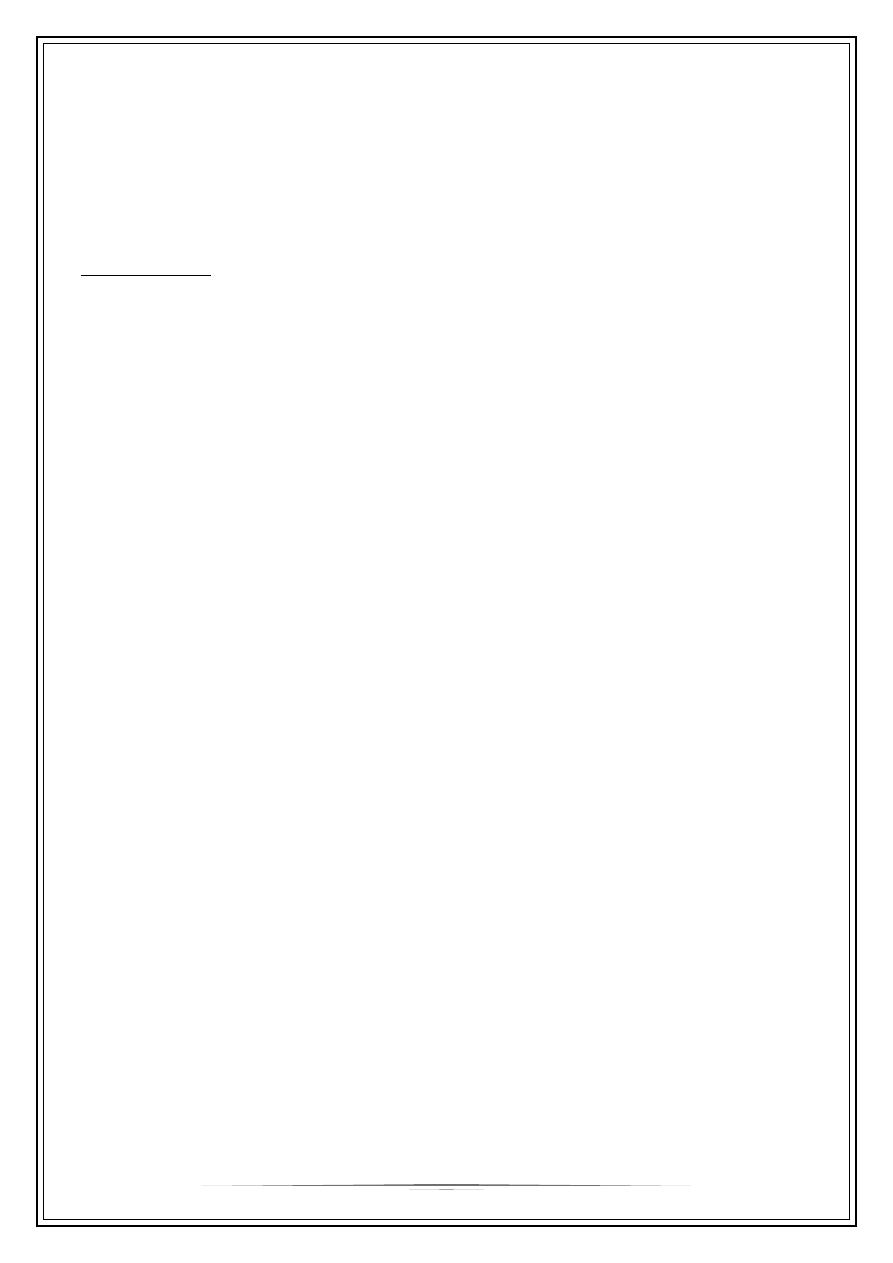
ARDS ( acute respiratory distress syndrome )
The cause is not definite. Hypothesized to be by release of Inflammatory cells and
proteinaceous fluid that accumulate in the alveolar spaces leading to a decrease in
diffusing capacity and hypoxemia. Usually within the first 24 hours after injury.
Clinical features :
-Tachypnea , hypoxia
-X- ray- diffused pulmonary infiltrates
Treatment: is by 100% O2 and assisted
ventilation
•
If not detected early and treated , death may
occurs by multiorgan failure or
cardiorespiratory failure.
3
Fat embolism
It is a life threatening complication of fracture where fat globules occlude the small
blood vessels. Usually occur 48 – 72 hrs from the injury.
Pathogenesis : 3 theories
1. release fat globule from the fractures bone marrow to blood stream.
2. fat can also be released from the adipose tissue.
3. Fat is converted to free fatty acid , which induces toxic vasculitis followed by
thrombosis which obstruct the microvasculature.
Clinical features of fat embolism :
—
Patechial rash of anterior neck, anterior axillary fold or conjunctiva
—
Drowsiness Restlessness Disorientation Coma
—
Tachypnoea Tachycardia , hypoxia
Dx : -Urine: fat globules
-CXR: pulmonary infiltration\Snow storm appearance ( not always )
Treatment of fat embolism:
—
ventelation support
—
heparin
—
corticosteroeds
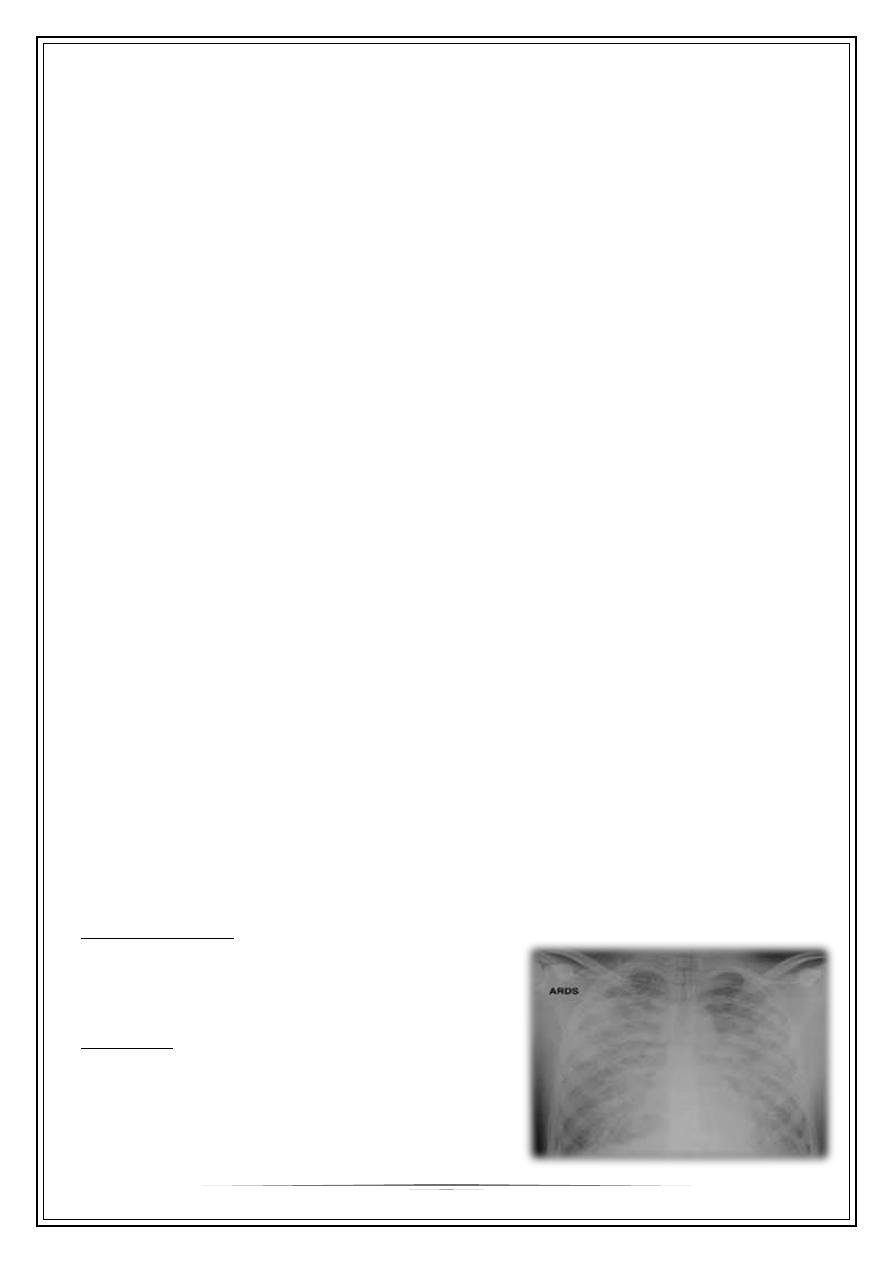
Thrombo-embolism :
Include leg veins thrombosis (DVT ) and pulmonary embolism.
A common complication especially in pelvic and spinal
injuries. Usually 3 – 5 days from the injury .
Pathogenesis : Virchow's triad :
1. Venous blood stasis
2. damage to the blood vessel wall
3. hypercoagulability
Diagnosis :
—
Clinical features leg pain , redness , sweling and pain ,
or feature of pulmonary embolism.
—
D-dimers
—
Doppler ultrasound
—
Venography ( the gold standard )
4
Treatment of thrombo embolism :
—
Prophylaxis : mechanical and chemical ( medications)
—
Therapeutic anticoagulants and thrombolytics
—
Early surgical stabilization to start early movement of the limb and patient.
Tetanus
Is a potentially fatal disease that is preventable by appropriate immunization
—
•caused by clostredium tetani ,
which is anaerobic, gram-positive spore forming bacilli found in faecal matter of
animals and humans.
Risk factors : Deep wounds without exposure to air, Wounds containing ischaemic
tissues, No immunization, Improper sterilization
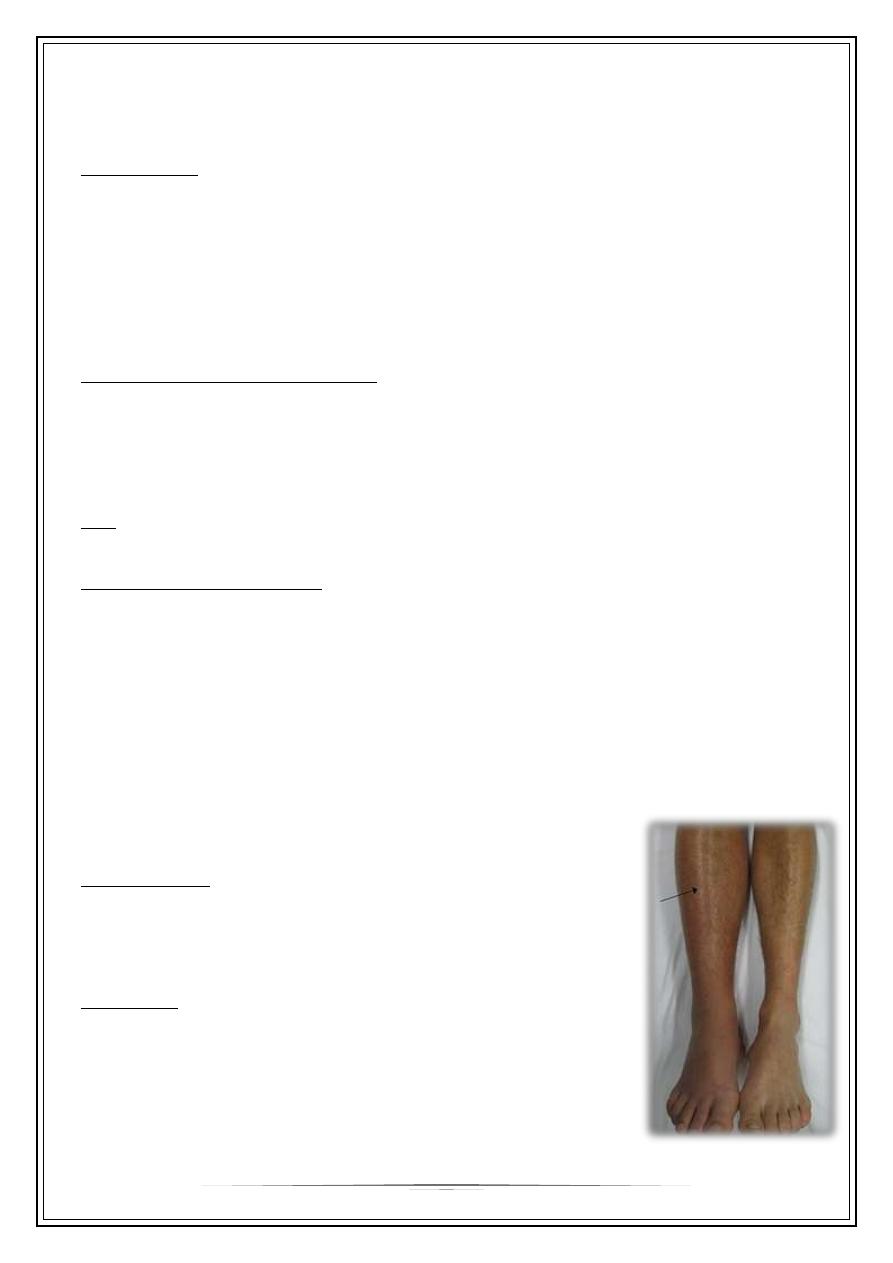
Clinical features :
—
Prodromal symptoms like headache and
restlessness. Trismus or lock jaw
Dysphagia and Neck rigidity.
Rigidity of back muscles (Risus sardonicus)
—
May end with convulsion
—
Sustained spasm of laryngeal and
respiratory muscles may cause asphyxia
and death.
Prevention :
—
Immunization
—
Removal of soil, foreign body and necrotic tissue.
—
Tetanus antitoxin (ATS) is given (250) units
Management :
—
Traheostomy if breathing difficult ( may need ET tube ventilation ).
—
Managed by heavy sedation to avoid spasms and convulsions.
—
During this period adequate nutrition, care of bladder and bowel
5
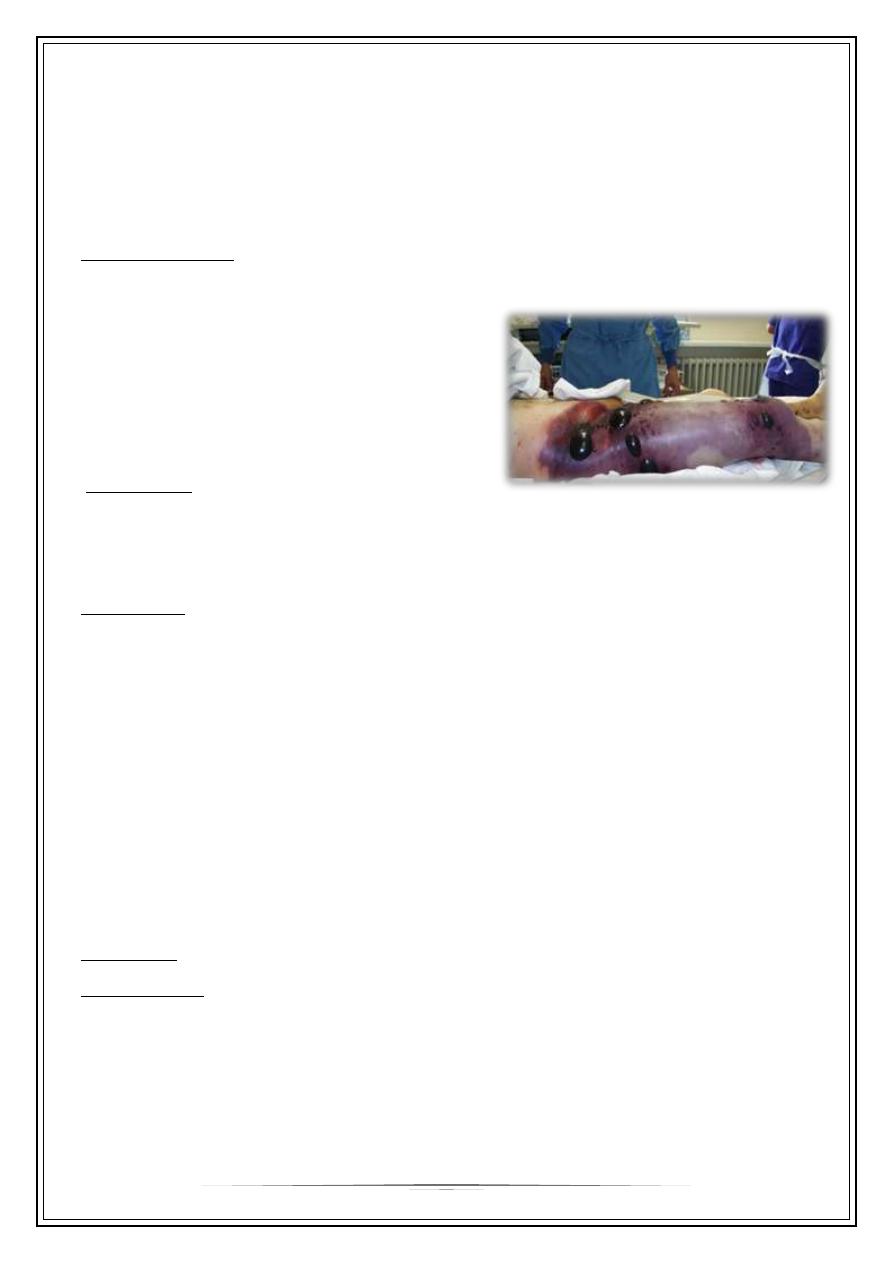
Gas gangren :
Terrifying condition is produced by Clostridium prefrengens , an anaerobic organisms
that can survive and multiply in a dirty wound with dead muscle that has been closed
without adequate debridement.
Toxins produced by the organisms destroy the cell wall and rapidly lead to tissue
necro-
Clinical features :
Appear within 24 hours of the injury with intense pain and swelling around the
wound and a brownish discharge may be
seen. little or no pyrexia but the pulse rate is
increased and a characteristic smell becomes
evident.
Rapidly the patient becomes toxaemic
and may lapse into coma and death.
Prevention :
Deep, penetrating wounds in muscular tissue are dan- gerous; they should be
explored, all dead tissue should be completely excised and, if there is the slightest
doubt about tissue viability, the wound should be left open.
Treatment :
—
The key to life-saving treatment is early diagnosis.
—
General measures, such as fluid replacement and intra- venous antibiotics, are
started immediately.
—
Hyper- baric oxygen has been used
—
The mainstay of treatment is prompt decompression of the wound and removal
of all dead tissue.
—
In advanced cases, amputation may be essential.
Crush syndrome:
Definition : renal failure following extensive crushing injury of muscles.
Pathogenesis:
Crushing of muscles causes entry of myoglobin into circulation. Myoglobin
precipitates in renal tubules causing acute tubular necrosis, metabolic acidosis &
hyperkalemia.
6
Clinical features:
(Appear within 2-3 days of injury) , Oliguria (Scanty urine) , Restlessness , Cardiac
arrhythmia ,Shock
Treatment :
—
As acute renal failure : fluid with diuretics
—
Al kalinazaion of urin by sodium bicarbonates
Infection
Open fractures may become infected; closed fractures hardly ever do unless they
are opened by operation.
Compartment syndrome
A devastating complication of fracture or other kind of injuries .
Definition : An increased pressure within enclosed osteofascial space that reduces
capillary perfusion below level necessary for tissue viability ( especially the nerve
and muscle tissues )
Casues:
—
Trauma ( fracture or crushing injuries )
—
Bleeding disorders
—
Burns
—
Tight wraps and casts
—
Leakage of iv fluid infusion .
Diagnosis :
—
Tense compartment
—
Severe pain out of proportion to the injury
—
Pain to the passive stretch of muscle (the earliest sign)
—
5 Ps : pain , parathesia , palor , pulslessness
,paralysis , poikilothermia ( late signs )
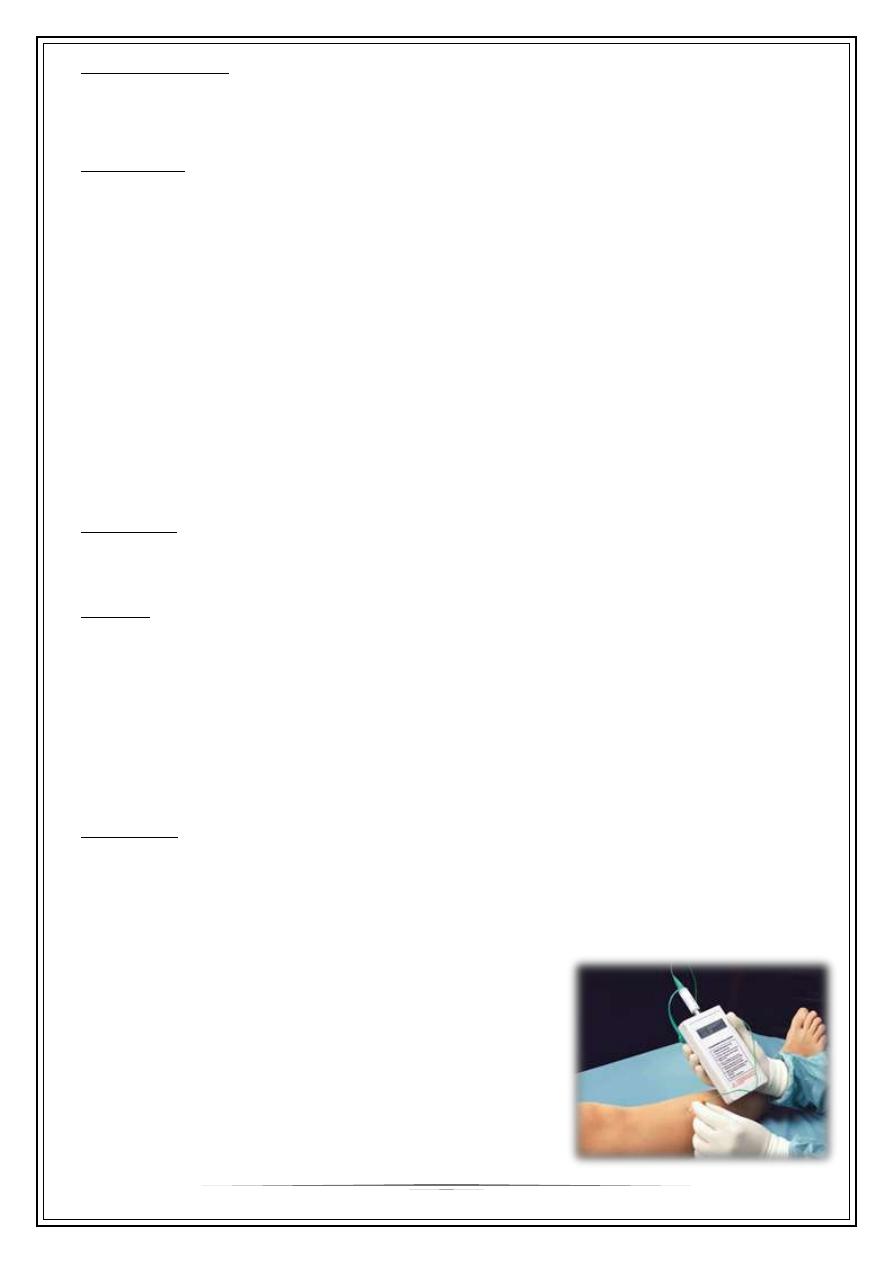
—
Compartment pressures :
> 30 mmHg or within 20 mmHg from the
diastolic BP indicate abnormal compartment
pressure and necessitate faciotomy.

7
Treatment :
—
Leg should be put and the level of the heart
—
Remove cast and Split all dressings down to skin
—
Fasciotomy if continued clinical findings and/or elevated compartment pressure
Thank You,,,