EMAIL TWITTER TELEPHONE
MDE
SUBJECT
Blood Transfusion
SUPERVISED BY:
Dr.khalid Naffi
MOSUL MEDICAL COLLEGE
DEPARTMENT OF
MEDICINE
PRESRENTED BY:
SIXTH YEARS MEDICAL STUDENTS -GROUP B-
Abdulrhman Luqman Younis
Mohammad Moyasser Mahmood
Mohammad Salim Sulaimn
Tarik Zyad Hassan
DATE OF PRESNTATION
THURSDAY, FEBRUARY 1, 2018
SUBJECT DISSCUSION
This lecture of hematology talks about blood transfusion from two
views :
1 Blood component therapy
Whole blood, packed RBC, cryo, etc... indication of each one
2 Blood transfusion reaction
Immunological and non-immunological reaction (volume overload
disease transmission and massive transfusion)
2 |
P A G E
Blood components therapy
1. Whole Blood
2. Red Cell Concentrate:
3. Leukocyte - poor RBC:
4. Platelets Conc. ( Random &single doner) :
5. Fresh Frozen Plasma:
6. Cryo – Precipitated Antihaemophilic Factor:
1-Whole Blood
Acute Haemorrhage
Oligaemic Shock
Neonatal Transfusion
Exchange Transfusion
Whole blood should not be used in chronic anaemias, which are better treated with red
cell concentrate, as whole blood may cause cardiac overload
Granulocytes & platelets present in stored whole blood are not functional,
whole blood is also deficient in labile clotting factors
1 unit is expected to increase Hb by 10 g /L in adults.
After transfusion, the increase may be not apparent for 48 – 72 hr while the patient’s blood
volume readjusts to normal
2-Red Cell Concentrate
It is the preparation of choice when the main purpose of blood transfusion is to provide a
means for the transport of oxygen
Red cell concentrate carries the same risk of haemolytic transfusion reaction &
transmission of viral diseases as does whole blood.
The use of red cell concentrate reduces the amount of anticoagulant & electrolyte
transfused
It is more viscose than whole blood & usually takes longer to transfuse.
3-Leukocyte - poor RBC:
These are red cell preparations from which most of the white cells & platelets have been
removed
Several methods are available to produce leucocyte – poor red cell preparations including:
sedimentation, centrifugation, washing & filtration
The volume & composition of the final product depend on the method of preparation. Washed
cells are also free from plasma proteins.
Can be used in the following conditions:
To prevent transfusion reaction in patients with known WBC Abs
To prevent sensitization to WBC Ags in patients requiring multiple transfusions
(thalassaemia, haemolytic anaemias, etc.) or in potential BM transplant candidates
To transfuse patients who are allergic to plasma proteins ( washed cells only)
They carry the same risk of haemolytic transfusion reaction & transmission of viral diseases.
4-Platelets Conc. ( Random Donor (
Each unit of random donor platelets concentrate contain an average of:
5 X 10
10
/ L ( 0.5 X
10
11
/ L ) suspended in about 50 ml of plasma.
It also contains some leucocytes & RBC.
Cross matching is not necessary but ABO compatible platelets should be used, as
platelets express ABO antigens.
Although platelets do not express Rh Ag, Rh compatible platelets should be used
where possible, because all platelet preparations also contain RBC. This particularly
important in Rh negative females of productive age, if it happen ,
the use of Anti – D for prevention of Rh immunization should be considered.
4 |
P A G E
Each unit of platelet concentrate will rise the platelet count of an average adult by 5 – 10 X
10
9
/ L under optimal conditions.
A standard dose of platelets is about 6 units (one unit per 10 kg of body weight)
Massive splenomegaly, high fever, sepsis, DIC & platelets/ HLA Abs can cause less than
expected platelet count increment & survival.
The 1 hr post transfusion platelet count increment is less affected by splenomegaly, high
fever, & DIC than by the presence of platelet or HLA Ab. If the 1 hr increment is less than 50
% of expected, the patient is considered to be refractory & should be screened for HLA Ab &
should be HLA typed.
4-Platelets Conc. (Single Donor):
A standard or a larger dose of platelets can be obtained from a single donor by the use
of cell separator.
It contain 2 – 6 X 10
11
platelets with an average of 3 X 10
11
.
In addition to the indications where random platelet concentrate is used, single donor
platelet concentrates can be HLA matched with the patient.
Each unit is expected to rise platelet count by 30 – 60 X 10
9
/ L
Absolute platelet increment / µl X body surface area (m
2
)/
Number of platelets transfused ( 10
11
)
5-Fresh Frozen Plasma:
Treatment of multiple coagulation factor deficiencies
( massive transfusion, trauma, liver disease, DIC, unidentified deficiency )
Content : 150 – 250 ml plasma containing all coagulation factors except platelets (
400 mg fibrinogen + 1 unit / ml all other factors )
It should be thawed at a temperature of 35 & 37 °C. The thawing process takes about 20
min. FFP should be used soon after thawing, preferably within 2 hr.
FFP must be transfused though a standard blood filter at a rate not exceeding 10 ml /
min.
The dosage of FFP depends on the clinical situation & must be assessed for individual case.
An average dose varies between 5 – 15 ml / kg.
Repeated transfusions, however, would be required for surgical patients until healing has
occurred,
e.g., factor IX has a half life of 18 – 24 hr, requiring daily transfusions.
FFP should not be used for blood volume expansion or protein replacement because safer
products are available; serum albumin, synthetic colloids, and balanced salt solutions, none
of which transmits disease or cause severe allergic reactions.
6-Cryo – Precipitated Antihaemophilic Factor:
Indications:
Factor VIII deficiency
VonWillebrand`s disease
Factor XIII deficiency
Fibrinogen deficiency, dysfibrinogaemia
Content :
VIII = 80 – 150 U
vWF = 40 – 70 % of whole blood level
XIII = 20 – 30 % of whole blood level
I = 150 – 250 mg
FACTOR VIII dosing
Increment desired X body weight/2
The number of bags required = no of units / 80
The dose is given 8 – 12 hourly
Fibrinogen
Increment desired (in mg/ml) X plasma volume
The number of bags required = total dose / 250
Fibrinogen 2.5 g / L = 250 mg / dl = 2.5 mg / ml
e.g. 0.3 g / L, plasma volume 2500 ml, needing surgery?
(1 – 0.3) X 2500 = 1750 mg is needed
1750 / 250 = 7 bags of cryo-ppt are needed
6 |
P A G E
Haemolytic Transfusion Reactions
Immunological HTR
Immediate Intravascular Haemolysis
Usually ABO mix-up
Complement activating Ab
Destruction of transfused RBC
Immediate Extravascular Haemolysis
Attachment of Ab to RBC (usually complement activating IgG )
Rapid destruction of coated RBC in RES
Delayed Haemolysis
Nearly always extravascular
Attachment of rapidly developing IgG Ab to donor RBC
Effects of donor's Ab on recipient's RBC
Nearly always group O plasma with high titered Anti-A &/or Anti-B
Development of positive DAT in the recipient
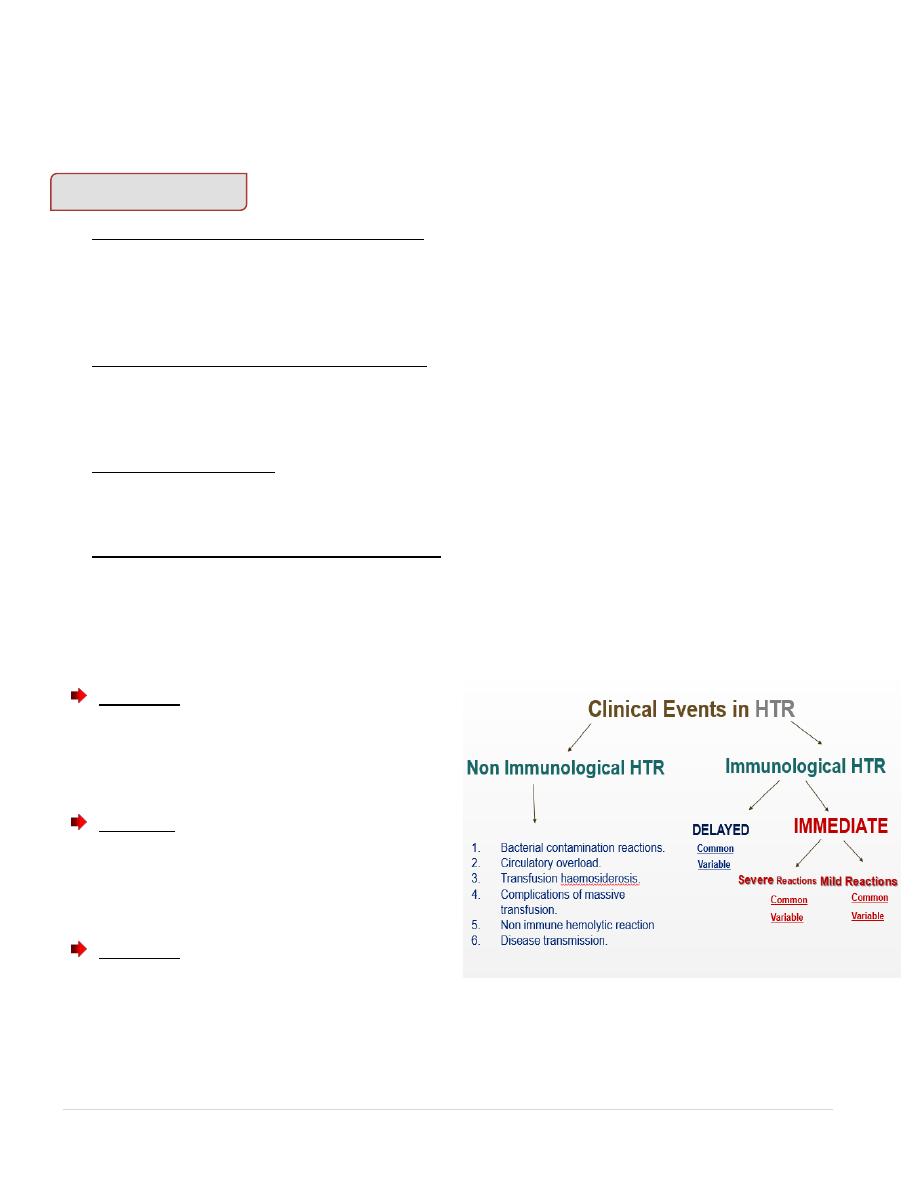
Clinical Events in HTR
Mild Immediate Reactions
Common
Fever
Chills
Tachycardia
Transient blood pressure changes
Variable
Skin flushing
Anxiety
Nausea
Severe Immediate Reactions
Common
Fever with chills
Pronounced blood pressure drop
Chest & /or back pain
Haemoglobinaemia / haemoglobinuria
Variable
Reflex blood pressure elevation
Oliguria
Haemorrhagic diathesis
Delayed Reactions
Common
Otherwise unexplained fever
Positive DAT
Variable
Fall in PCV
Haemoglobinuria
Oliguria
If Transfusion Reaction is suspected
1. Stop the infusion of blood or component. Save the container & the infusion set
2. Check the identifying information on container label & the patient's data
3. Keep the IV line open
4. Draw a posttransfusion blood sample
5. Send the following items to the transfusion service lab
A. Blood container with the infusion set clamped but still attached
B. Clinical notes
C. Posttransfusion blood sample ( EDTA + clotted)
D. Record patient's urine output for the next 6 – 12 hours. Save the first
urine sample voided after reaction is suspected. Send the sample to lab
with notation “ suspected HTR”
8 |
P A G E
Non immunological transfusion reaction
1. Bacterial contamination reactions.
2. Circulatory overload.
3. Transfusion haemosiderosis.
4. Complications of massive transfusion.
5. Non immune hemolytic reaction
6. Disease transmission.
1. Bacterial contamination reaction
Although uncommon,but this type of specific reaction can have a rapid onset and
high mortality in recipients.
The presence of bacteria in transfused blood may lead either to febrile reactions in
the recipient ( due to pyrogens ) or serious manifestations of septic or endotoxic
shock.
Commonly caused by endotoxin produced by bacteria capable of growing in cold
temperatures such as Pseudomonas species, E. coli, Yersinia enterocolitica.
Source of infection.
Infection of stored blood is extremely rare.
Skin contaminants are not infrequently present in freshly donated blood but these
organisms ( predominantly staphylococci ) do not survive storage at 4 º C although they
will grow profusely in platelet concentrates stored at 22 º C.
Healthy donor who are bacteremic at the time of donation. The majority are due to
Yersinia enterocolitica, which grows well in red cell components due to its dependence
on citrate and Iron.
Gram negative, endotoxin – producing contaminants found in dirt, soil and faeces may
rarely grow in the storage condition of blood.
Clinical manifestation
Usually appear rapidly during transfusion or within about 30 minutes after transfusion
with dryness, flushing of skin.
Fever, Hypotension, Chills, Muscle pain, vomiting, Abdominal cramps, Bloody
diarrhoea, Hemoglobinuria, Shock, Renal failure, DIC.

Management.
Rapid recognition is essential
Immediately stop the transfusion.
Therapy of shock, steroids, vassopressors, fluid support, respiratory ventilation and
maintenance of renal function.
Broad spectrum IV antibiotics
The blood component unit and any associated fluids and transfusion equipment should
be sent immediately to blood bank for investigation ie: gram stain and culture.
Blood C & S from the recepient.
Prevention
Strict adherence to policies & procedures regarding blood component collection,
storage, handling,and preparation is essential to reduce the risk.
Visual Inspection of components before release from the transfusion service include
any discolouration, visible clots, or hemolysis.
Ensure the blood components are infused within standard time limits ( 4 hours ).
Blood packs should never be opened for sampling, if any open method of preparation
has been used, the unit should be transfused within 24 hours.
Blood should always be kept in accurately controlled refrigerators (with alarms),
maintained strictly at 2 – 6 º C, the blood should never be removed and taken to the
ward or OT until it is recquired.
2. Circulatory overload
All patient will experience a temporary rise in blood volume and venous pressure
following the transfusion of blood or plasma except for those who are actively
bleeding.
However, young people with normal cardiovascular function will tolerate this
changes provided it is not excessive.
Pregnant women, patient with severe anaemia, elderly with compromised
cardiovascular function will not tolerate the increase in plasma volume and acute
pulmonary oedema may develop.
10 |
P A G E
Clinical manifestation
Frequently due to transfusion of a unit at too fast rate.
Signs of cardiac failure – raised JVP, basal crepitations in both lungs, dry cough,
breathlessness.
Management
Stop the transfusion immediately.
Prop up the patient
Oxygen therapy
Intravenous diuretics should be used appropriately.
If more rapid volume reduction is needed, therapeutic phlebotomy can be used.
Prevention
Packed cell should be used instead of whole blood.
Packed cells should be given slowly over 4 hours.The usual rate of transfusion is about
200 ml per hour. In patient at risk rate of 100 ml per hour or less are appropriate.
Diuretics should be given at the start of the transfusion and only one or two units of
concentrated red cells should be transfused in any 24 hour period.
Blood transfusion should be given during the daytime, Overnight transfusion should be
avoided wherever possible.
3. Transfusion haemosiderosis
A complication of repeated long term blood transfusion.
Most commonly seen in thalassaemic patient.
Each unit of blood has about 200 mg of iron, while the daily excretion rate is about 1
mg.
The body has no way of excreting the excess unless the patient is bleeding.
Assessment of storage iron levels such as ferritin levels should be done.
The use of Iron chelating agent, Desferrioxamine does not completely overcome the Iron
load, but has delayed the onset of problems due to haemosiderosis.
Transfusion of neocytes or young red cells is the other alternative.
However, it is expensive, time consuming, and the result are not as favourable as expected.
4. Complication of massive transfusion
Massive transfusion is defined as the replacement of total blood volume within a 24 hour
period.
This will inevitably lead to :
1) Dilution of platelets.
Blood effectively has no functional platelets after 48 hours storage, after 8 to 10 units of
blood transfusion, thrombocytopenia will usually seen.
Bleeding due to a slightly low platelet is uncommon, therefore routine administration
of platelet after certain amount of blood transfusion is unnecessary.
Regular monitoring of platelet count is more important.
Platelet transfusion may be recquired if platelet count <100 x 10 9 /L with continous
bleeding or surgical intervention.
2) Dilution of coagulation factors.
Stored Whole blood < 14 days has adequate levels of most coagulation factors for
haemostasis.
If stored blood of more than 14 days, or plasma reduced blood or red cells in optimal
additive solution is used,
replacement of coagulation factors with FFP is necessary.
3) Hypothermia
Defined as core body temperature less than 35 c ) is associated with large volumes of cold
fluid transfusion.
This may results in cardiac irregularities in particular VF. Therefore the use of blood warmer
is important.
12 |
P A G E
4) Excess citrate can act on the patient’s plasma free ionized calsium and results in
hypocalcaemia ( transient ).
Citrate toxicity occur with extremely rapid transfusion ( one unit every 5 minute ),
in premature infant having ET with blood stored in citrate for longer than 5 days.
5) Hyperkalemia
Can be caused by intracellular loss of potassium from RBC during storage or infusion
of intracellular potassium depleted RBC blood components such as washed RBC or
frozen washed RBC .
The most important consideration in massive blood transfusion is to replace blood loss
quickly and adequately. Too little blood , too late has more serious consequences than
massive blood transfusion itself.
5.Non immune hemolytic reaction
Mechanical – heat damage from blood warmer, cold, small gauge needle.
Environment – hypotonic or hypertonic solution.
6) Disease transmission.
1. Hepatitis
2. Syphilis
3. Malaria
4. Cytomegalovirus
5. Human immunodeficiency virus
6. Human T cell leukaemia viruses.
Donor selection criteria and subsequent screening of all
donations are designed to prevent disease transmission, but these do not completely
eliminate the hazards.
Hepatitis
Hepatitis A is rarely transmitted by transfusion. Any donor who has been in close
contact with Hepatitis A patient or develops hepatitis A is deffered for 12 months.
Hepatitis B is a frequent sequel to blood transfusion. Currently all blood donations
are tested for HBsAg by very sensitive third generation techniques ( eg; ELISA ), able
to detect at least 0.5 iu of HBsAg per ml of serum.
In HUSM, EIA method is used with 99.9 % sensitivity.
HBsAg positive subjects are permanently excluded from donations.
Hepatitis C
All donated blood are tested for anti – HCV.
Improved screening assays based on multiple recombinant or synthetic antigens
including viral core protein are now available.
Individuals with a history of jaundice may be accepted as donors 1 year after the
illness provided they tested and negative for HBsAg and anti HCV.
Syphilis
The organism is more likely to be transmitted in platelet concentrate due to their
room temperature storage and short shelf life.
Treponema pallidum does not survive well at 4º c and red cell preparation are likely
to be non infective after 4 days refrigeration. Passive transmission of the antibody to
the recepient may cause diagnostic confusion.
Any donations with positive result is discarded, any subjects with positive tests are
permanently deferred, even after effective therapy.
Malaria
Malarial parasites remain viable in blood stored at 4º C and easily transmitted by
blood transfusion.
In some endemic areas, all recipients are treated with antimalarial drugs.
Donors who come from endemic area or have had an attack of malaria can be
accepted, their plasma can be used for fractionation but red cells must be discarded.
14 |
P A G E
In HUSM , BFMP should be tested for certain group of donors ie : army, donors from
endemic area.
Cytomegalovirus
Post transfusion CMV infection is not uncommon.
The infection is characterised by fever spleenomegaly, and atypical lymphoid cells in
the peripheral blood.
Due to its benign course, screening for past infection among donors are not
necessary.
However, there are patient at risk of developing fatal pneumonitis or disseminated
CMV infection : prem baby < 1500g, BM or and other organ transplant recipient,
pregnant women ( risk to fetus ).
For them, anti – CMV free blood & components should be provided.
In UK, incidence of CMV antibodies in adult population is 50 to 60 %.
As an alternative, since CMV is cell associated, leukodepleted blood may be used.
Human immunodeficiency virus
HIV can be transmitted both in cellular and plasma components.
The majority of recipient of blood or blood products who have been infected in the
past were transfused before 1985 with unheated, non pasteurized pooled plasma
products, Factor VIII and IX.
HIV is heat labile, therefore prolonged heat treatment of Factor VIII for heomophiliacs
is effective.
Routine screening of all donated blood started in October 1985 in UK. This in
combination with donor education, and self deferral has reduced the risk of HIV
transmission through contaminated blood. There were 2 documented cases in the UK
since screening program introduced.
With screening programe, HIV transmission still occur through donations given in the
window period of infectivity.
With current antibody screening technique, the estimated window period is about 3
weeks.
PCR for HIV RNA is able to reduce the window period to approximately 1 week.
Human T- cell leukaemia viruses.
HTLV 1 and II are related retroviruses.
HTLV 1 is endemic in the caribbean, parts of Africa and in Japan, 3 – 6 % of the
population are seropositive.
HTLV 1 is associated with tropical spastic paraparesis and adult T cell – leukaemia.
Importance of HTLV II is not clear.

Both HTLV 1 and II are cell associated and not transmitted in plasma.
Currently available test include ELISA and gelatin particle assay, but confirmation of
positive result are difficult due to cross reactivity with other retroviruses.
Investigation of transfusion reactions.
Investigations of transfusion reaction are necessary for :
1. Diagnosis
2. Selection of appropriate therapy
3. Transfusion management
4. Prevention of future transfusion reaction.
Investigations should include correlations of clinical data with laboratory result .
Important clinical data :
1. Diagnosis
2. Medical history of pregnancies, transplant, and previous transfusion.
3. Current medication
4. Clinical signs and symptoms of the reaction.
5. Question related to the transfusion:
Amount of blood transfused to cause the reaction.
How fast , how long ?
The use of blood warmer.
Any filter used ? Other solutions.
Any drugs given at the time of transfusion
Laboratory investigation outline of transfusion reaction.
1. Immediate procedures
•
Clerical checks.
•
Visual inspection of serum and plasma for free hemoglobin ( pre and post transfusion)
•
Direct anti – globulin test. ( post transfusion EDTA sample )
16 |
P A G E
2. As recquired procedures
•
ABO grouping and RH typing, pre and post transfusion
•
Major compatibility testing , pre and post transfusion
•
Antibody screening test , pre and post transfusion
•
Alloantibody identification
•
Antigen typings
•
Free hemoglobin in first voidedurine post transfusion
•
Unconjugated bilirubin 5 – 7 hours post transfusion.
3. Extended procedures
•
Gram stain and bacterial culture of unit
•
Quantitative serum Hemoglobin.
•
Serum Haptoglobin , pre and post transfusion
•
Peripheral blood film.
•
Coagulation and renal output study
•
Urine hemosiderin
Edited by:
Abdulrhman Luqman Younis