د. عماد ادوية 11\4\2018
عدد الاوراق ( 4 ) م\3\موصل lec:9+10New Macrolides
Erythromycin
Clarithromycin
Azithromycin
Roxithromycin
Telithromycin semisynthetic erythromycin derivative ,active against G+ve strain resistant to other Macrolide ( MG, hepatitis, QT prolong)
ERYTHROMYCIN
First isolated from Streptomyces erythreus in 1952Widely employed as an alternative to penicillin
MECHANISM OF ACTION
It is bacteriostatic at low conc & bactericidal at high concBactericidal property depends on the conc, organism concerned and its rate of multiplication
Erythromycin acts by inhibiting bacterial protein synthesis. It combines with 50s ribosome subunits and prevent translocation.
ANTIMICROBIAL SPECTRUM
Spectrum is similar to Pencillin G. Mostly gram +ve and few gram –ve bact.Str. pyogenes , Str. Pneumonia, N. gonorrhoea, Clostridium, C. diphtheriae and Listeria
In addition, Campylobacter, Legionella, Branhamella catarrhalis, G. vaginalis and Mycoplasma (which are not affected by pencillin are also highly susceptible to erythromycin)
Moderately sensitive to, H. influenza, B. pertussis, C. trachomatis, N. meningitidis and Rickettsiae
Ineffective against Enterobacteriaceae, other gram negative bacilli and B. fragilis
Pharmacokinetics
Absorption incomplete but adequate from intestine
Inactivated by gastric HCL, hence given as :
Enteric coated tablets or ester (stearate, ethyl succinate )
Food delays absorption
Not metabolized and actively secreted in bile ( major route of excretion )
Widely distributed into most tissues, except the brain and CSF
Cross the placental barrier
Protein binding – 70- 80 %
Half – life approx. 1.6 hr
Major excretion through liver. Renal excretion is minor
Only 2-5 % is excreted in active form in urine
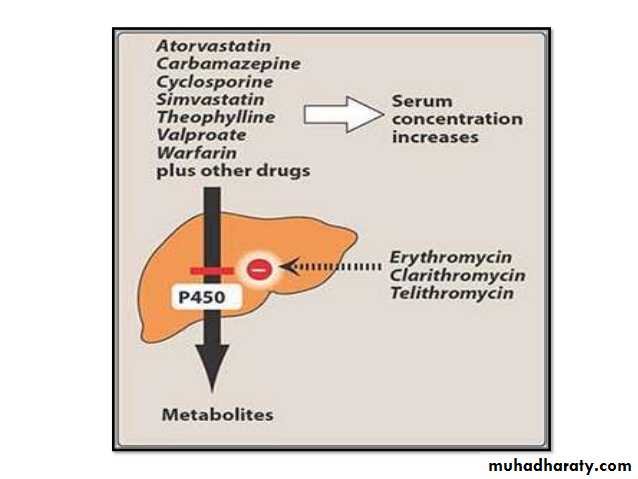
It inhibits hepatic oxidation of many drugs – it rises plasma level of theophylline, carbamazepine, valproate, ergotamine and warfarin
USES
As an alternative to penicillinStreptococcal pharyngitis, tonsillitis, mastoiditis and CAP
Alternative prophylaxis for RF and SABE
Diphtheria
Tetanus as an adjuvant to TT
Syphilis and gonorrhoea
Leptospirosis
As a first choice drug for
Atypical pneumonia caused by Mycoplasma
Whooping cough
Chancroid
6.Adverse response:
GI Effects: nausea, vomiting, abdominal cramps
Liver Toxicity: Cholestatic hepatitis.
3) Cardiotoxic effects
4) Auditory impairment (Ototoxicity)
5)Hypersensitivity reactions
Superinfections
Ototoxicity:Transsient deafness has been associated with erythromycin, especially at high dosages.
Clarithromycin
Pharmacokinetics
Acid stable
Food delays absorption but does’nt alter its extent
Metabolized by the liver to 14- hydroxy clarithro. ( active )
Widely distributed, except brain and CSF
Protein binding 40 – 70 %
Excreted in Urine – unchanged 20 – 40 %
14- H. clarithromycin 10 – 15 %
Biliary
Half- life clarithromycin 3 – 7 hr
14 – H. clarithromycin 5- 9 hr
Advantage over erythromycin
Lower frequency of GI intolerance
Less frequent dosing ( twice daily )
Indications
Pharyngitis / tonsilitis
Otitis, sinusitis
Adjunct in treatment of duodenal ulcer ( H. pylori )
MACROLIDES ( cont. )
Azithromycin
Pharmacokinetics
Rapidly absorbed from GIT
Food delays absorption
Widely distributed ( extensive tissue distribution ), except CSF
Protein binding 51%
Undergo some hepatic metabolism ( inactive )
Biliary route is the major route of elimination
Only 6% is excreted unchanged in the urine
Half- life approx. 3 days
Mainly effective on G- bacteria but less active against G+(s.pneumoniae & s.pyogenes) than erythromycin
Advantage over erythromycin & clarithromycin
Once daily dosing
No inhibition of cytochrome P- 450
Indications
Pharyngitis/ tonsilitis ( s. pyogens ), otitis, sinusitis ( Staph. Aureus & H. influenzae )
Uncomplicated genital chlamydial infections
G+ve aerobic: Clarithromycin>Erythromycin>Azithromycin
G-ve aerobic:Azithromycin > clarithromycin > Erythromycin
Lec:10
Metronidazole and TinidazoleAzoles
This group includes:
1. Metronidazole and tinidazole.
2. Antifungal drugs such as clotrimazole.
Metronidazole(Flagyl)
Metronidazole is a bacteriostatic it is effective in anaerobic microorganisms and some protozoa.It is well absorbed after oral or rectal administration.
Mechanism of action:
In anaerobic bacteria metronidazole is converted into an active form by reduction of its nitro group, this binds to DNA and prevents nucleic acid formatoion.Clinical Uses:
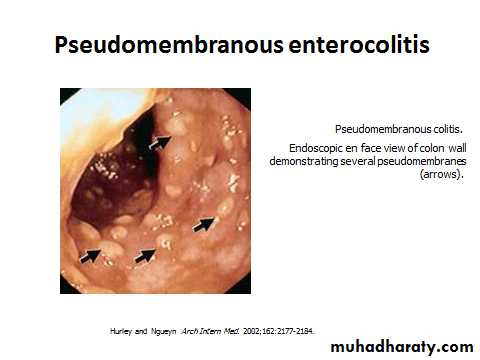
Treatment of sepsis due to anaerobic organisms e.g. Bacteroides species notably : postsurgical infections, intrabdominal infections and septicemia, but also wound and pelvic infection, osteomyelitis and absesses of brain or lung.Pseudomembraneous colitis.
Trichomoniasis.Amoebiasis (Entamoeba histolytica) .
Giardiasis (Giardia lamblia) .
Acute ulcerative gingivitis and dental infections.
Anaerobic vaginosis(Gardnerella vaginalis).
Triple therapy in
Adverse effects:
GIT: nausea, vomitig, diarrhea and unpleasant metallic taste in the mouth.CNS: headache, dizziness , ataxia and seizure,
Rashes, urticaria and angioedema.
Peripheral neuropathy.
Aseptic meningitis
Tinidazole :
It is similar to mertronidazole.Longer half life (13 h).
Same uses.
Same adverse effects.
The longer duration of action of tinidazole may be an advantage e. g. in giardiasis, trichomoniasis and acute ulcerative gingivitis in which tinidazole 2g by mouth in a single dose is effective as a course of metronidazole.