د. بنان امراض 10\4\2018
عدد الاوراق ( 6 ) م\3\موصل lec: 5Breast pathology
Normal anatomy and cellular constituents:
The breast is originated from the skin. It resembles a the sweat gland in structure and development, so it is regarded as modified sweat gland.
Each breast consists of 15-25 lobes. Each lobe has a major excretory duct (lactiferous duct) that opens independently at the nipple .
Successive branching of this large ducts eventually leads to the terminal duct lobular unit (TDLU)(the basic structural unit of the breast), which composed of acini, intralobular stroma and buds from intralobular duct.
The lobes of breast are separated by interlobular collagenous stroma and adipose tissue.
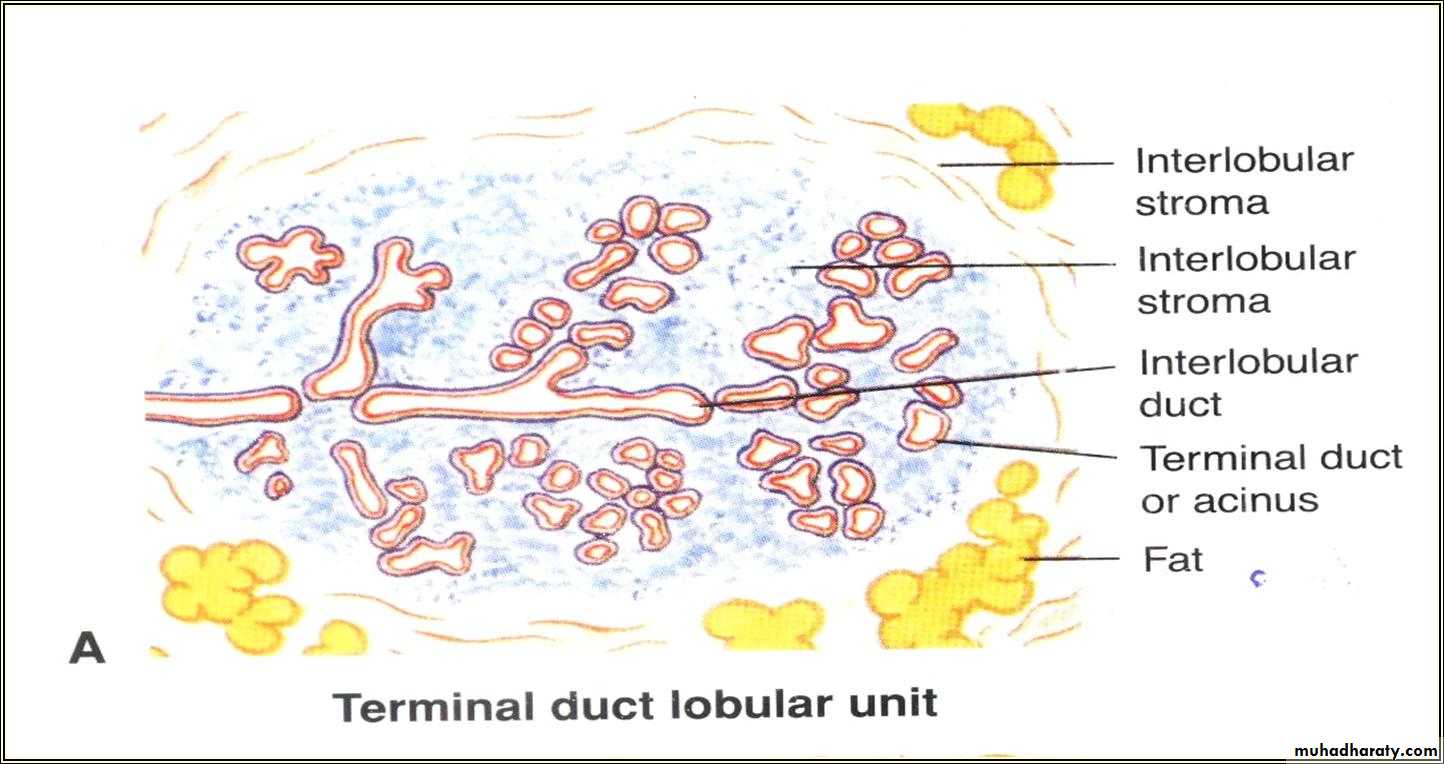

Normal female breast tissue
There is a larger duct to the right and lobules(TDLUs) to the left. A collagenous stroma extends between the structures. A variable amount of adipose tissue can be admixed with these elements.Apart from a keratinizing squamous lining close to the nipple, the ducts and ductules are lined by a two-layered epithelium, an inner layer of cuboidal or columnar cells and an outer discontinuous layer of smaller, contractile myoepithelial cells.
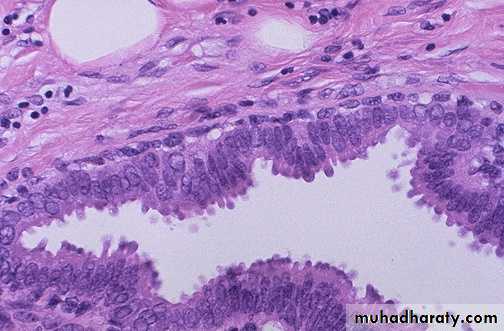
Normal breast duct with double layer
Disorders of DevelopmentPolythelia : Supernumerary nipples (Milkline Remnants (milk-line which extends from the axilla to the groin))
Accessory axillary breast tissue.
Congenital nipple inversion (acquired nipple retraction is of more concern, since it may indicate the presence of an invasive cancer or an inflammatory nipple disease).
Clinical Presentations of Breast Disease
Palpable mass or “lumpiness” (without a discrete mass)Pain (about 10% of breast cancers present with pain)
Nipple discharge
All are nonspecific but must be evaluated because
of the possibility of malignancy.
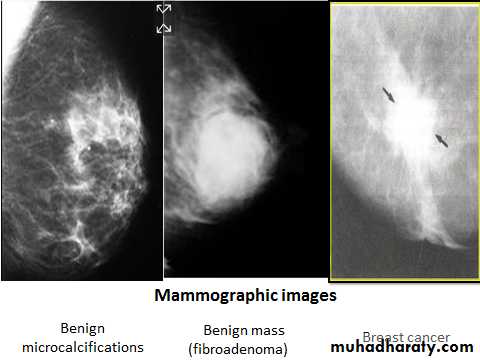
Mammographic Screening:
It was introduced in the 1980s as a means to detect small, non-palpable, asymptomatic breast carcinomas.
Its sensitivity and specificity increase with age.
Recommended to start at age of 40, unless there is patient or strong family history of breast cancer.
Inflammatory lesions of the breast:
Inflammatory diseases of the breast are rare (accounting for <1% of breast symptoms)A. Infective :
1- Acute mastitis (Acute pyogenic mastitis).
2- Chronic nonspecific mastitis.
3- Tuberculous mastitis.
B. Non-infective inflammatory lesions:
1- Mammary duct ectasia .
2- Fat necrosis of the breast .
Acute Mastitis :
It typically occurs during the first month of breastfeeding when the breast is most vulnerable due to cracks and fissures in the nipples. It is caused by a local bacterial infection (Staphylococcus aureus or, less commonly, streptococci ) . If not treated, it leads to multilocular abscess.Pathology
Gross: there may be generalized red, painful swelling of the breast or a localized abscess may form in a single breast lobe. The axillary lymph nodes are frequently swollen & show reactive hyperplasia .
Micro: there is an acute suppurative inflammation and with abscess formation.
Result: it may result in extensive destruction and fibrous scarring if not treated early.
Chronic nonspecific mastitis :
Sometimes, a low-grade bacterial infection will lead to chronic infection without acute exacerbation. Or it results from inadequate treatment of acute pyogenic mastitis.Tuberculous mastitis: :
Its rare , it might be due to :
a. Hematogenous spread of T.B.
b. Lymphatic spread of T.B.
c. Direct spread of T.B. (from lung or pleura).
It leads to tissue destruction with gramuloma formation.
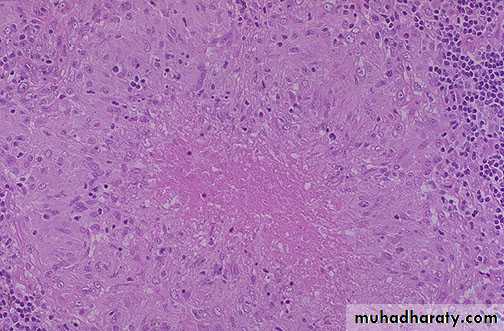
Tuberculous mastitis Granuloma with central necrosis
Duct Ectasia (Periductal or plasma cell mastitis ):This disorder tends to occur in the 5th or 6th decade of life, usually in multiparous women. it presents as a palpable periareolar mass that is often associated with thick, white nipple secretions.
There is progressive dilatation of the large and intermediate ducts, with periductal plasma cell infiltration. These Ectatic dilated ducts are filled with inspissated secretions, when it ruptured, the fatty material goes to the surrounding tissue, initiates a foreign body granuloma.
Subsequent fibrosis produces an irregular mass with skin and nipple retraction, that may mimics the clinical and radiographic appearance of invasive carcinoma.

Duct ectasia : dilatation of large ducts with periductal fibrosis & chronic inflammatory cell infiltrate.
Fat Necrosis
The presentations of fat necrosis are a painless palpable mass, skin thickening or retraction.
It is caused by a trauma to the breast which cause disruption of fat cells and allow the escape of fat globule into the surrounding tissue which cause foreign body giant cell reaction, with foamy cells and later dense fibrous tissue.
Clinically and mammographic examination it may simulate carcinoma due to hard mass production and calcification.
Fat necrosis
Benign Epithelial Lesions
They are classified into three groups, according to the subsequent risk of developing breast cancer:(1) Non-proliferative breast changes.
(2) Proliferative breast disease without atypia
(3) Proliferative breast disease with atypia
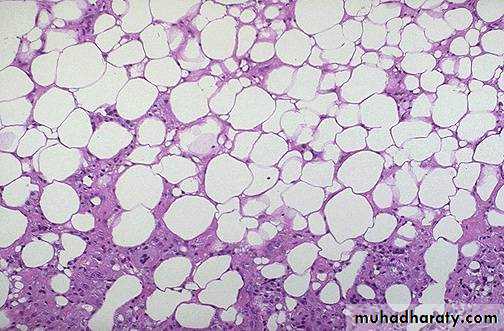
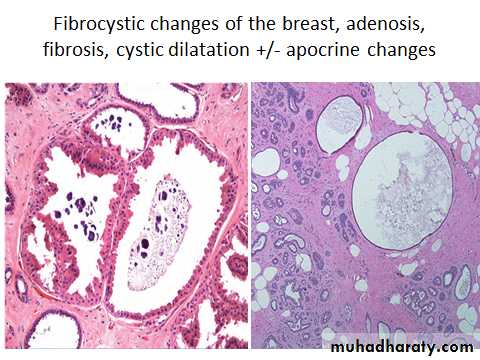
1- Nonproliferative Breast Changes (Fibrocystic Changes)
Fibrocystic changes are the most common breast abnormality seen in premenopausal women, it is widely assumed that it is caused by the influence of hormones on the female breast throughout reproductive life. An association of fibrocystic change with menstrual irregularities has been noted and its incidence is relatively higher in nulliparous women.There are three principal morphologic changes:
Fibrosis
Adenosis
Cystic change, often with apocrine metaplasia.
Cysts: Small cysts form by the dilation of lobules and in turn may coalesce to form larger cysts. Cysts are lined either by a flattened atrophic epithelium or by metaplastic apocrine cells(cells have abundant granular, eosinophilic cytoplasm and round nuclei basely located and closely resemble the normal apocrine epithelium of sweat glands).
Fibrosis: Cysts frequently rupture, releasing secretory material into the adjacent stroma. The resulting chronic inflammation and fibrosis contribute to the palpable nodularity of the breast.
Adenosis: Adenosis is defined as an increase in the number of acini per lobule.

Fibrocystic changes
single large cyst appear brown to blue
(blue dome cysts)
Fibrocystic disease, apocrine change

2-Proliferative Breast Disease Without Atypia
Lesions characterized by proliferation of epithelial cells, without atypia, are associated with a small increase in the risk of subsequent carcinoma in either breast.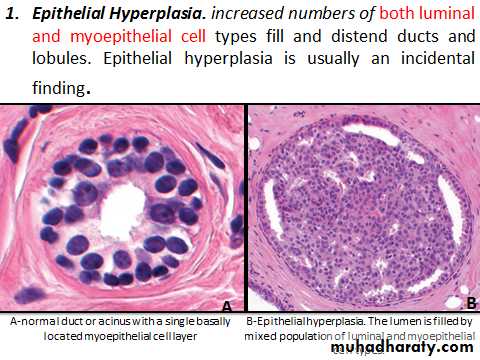

Epithelial hyperplasia
Sclerosing Adenosis. There are an increased in the fibrous stroma and an increased number of acini that are compressed and distorted in the central portion of the lesion.On occasion, stromal fibrosis may completely compress the lumens to create the appearance of solid cords or double strands of cells lying within dense stroma, a histologic pattern that at low power closely mimics invasive carcinoma
Sclerosing adenosis can come to attention as a palpable mass, a radiologic density, or calcifications
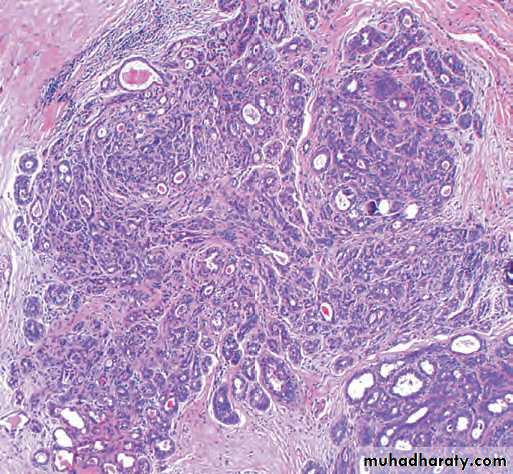
Sclerosing adenosis. There are an increased number of acini which are compressed and distorted by dense stroma. Calcifications are present within some of the lumens.
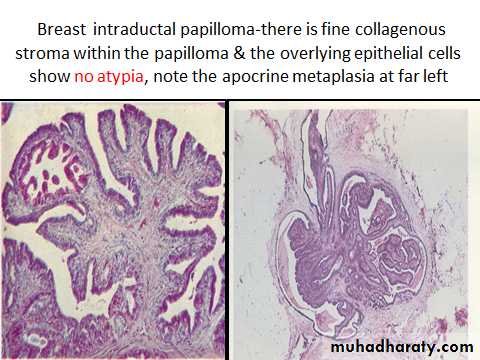
Papilloma: Papillomas grow within a dilated duct are composed of multiple branching fibrovascular cores. Epithelial hyperplasia and apocrine metaplasia are frequently present.
Large duct papillomas: are situated in the lactiferous sinuses of the nipple and are usually solitary. large duct papillomas produce a nipple discharge. Some discharges are bloody.
Small duct papillomas: are commonly multiple (intraductal papillomatoses) and located deeper within the ductal system. Most small duct papillomas come to clinical attention as small palpable masses, or calcifications seen on mammograms. They sometimes become malignant.
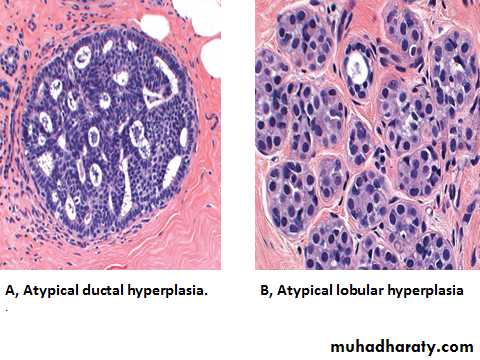
3-Proliferative Breast Disease with Atypia
Atypical hyperplasia is a clonal proliferation having some, but not all, of the histologic features that are required for the diagnosis of carcinoma in situ. It is associated with a moderately increased risk of carcinoma . There are two types:Atypical ductal hyperplasia
Atypical lobular hyperplasia
Clinical Significance of Benign Epithelial Changes
Nonproliferative changes (simple fibrocystic changes) do not increase the risk of cancer.Proliferative disease without atypia is associated with a 1.5- to 2 fold increased risk.
proliferative disease with atypia confers a 4- to 5 fold increased risk of cancer.