
Growth of cranial vault, cranial base and nasomaxillary complex
Growth of cranial vault, cranial base and nasomaxillary complex

• Development of the calvaria is dependent
upon the presence of the brain. It comprises
the frontal bones, the parietal bones, and the
squamous parts of the temporal and occipital
bones.

Cranial Vault
• The cranial vault is made up of a number of flat bones that
are formed directly by intramembranous bone formation,
without cartilaginous precursors. From the time that
ossification begins at a number of centers that foreshadow
the eventual anatomic bony units, the growth process is
entirely the result of periosteal activity at the surfaces of the
bones. Remodeling and growth occur primarily at the
periosteum-lined contact areas between adjacent skull bones,
the cranial sutures, but periosteal activity also changes both
the inner and outer surfaces of these plate-like bones.
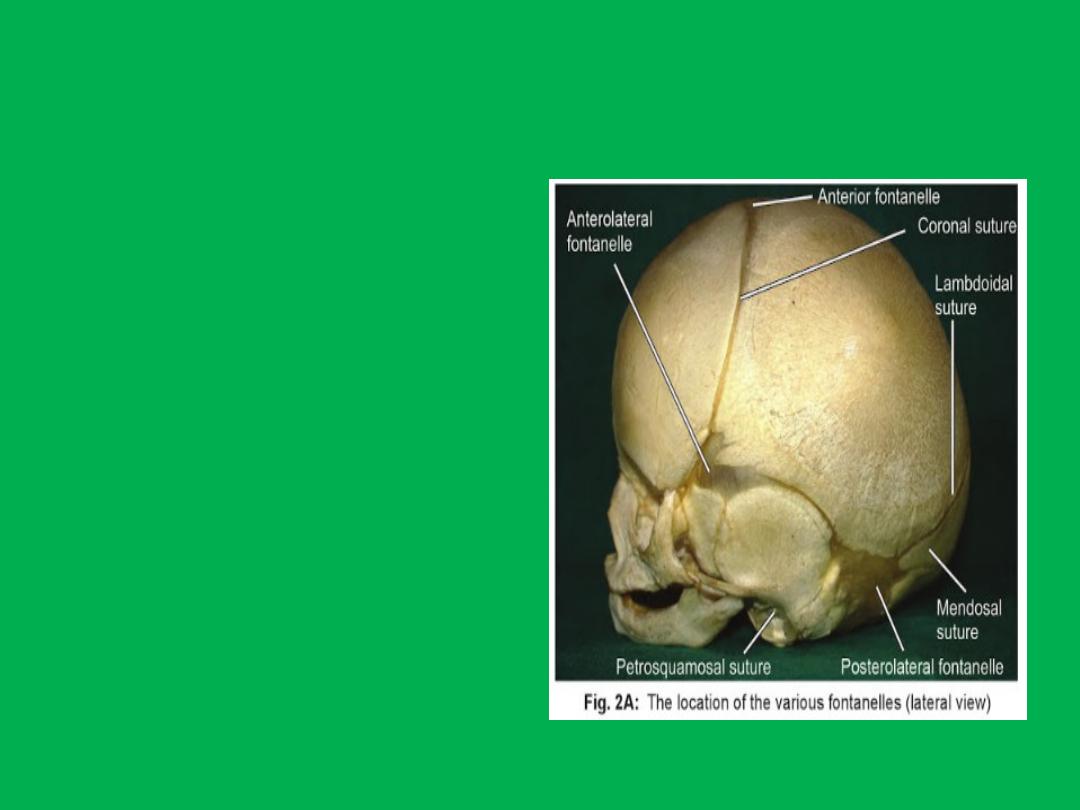
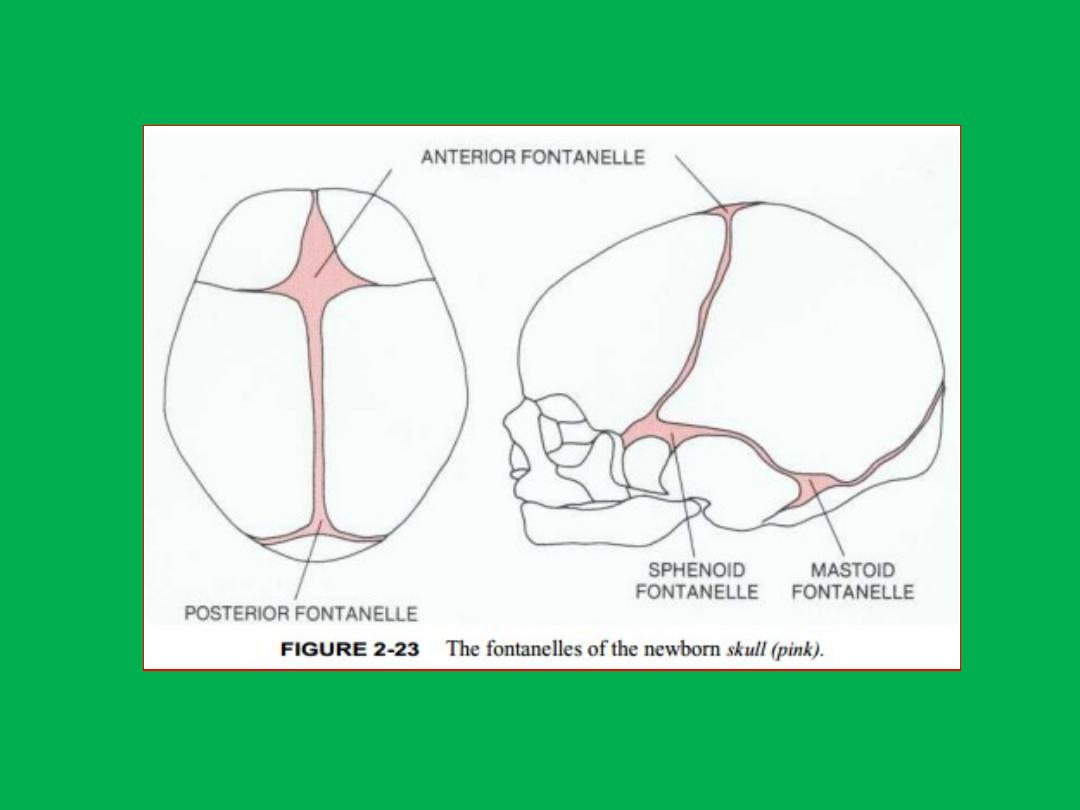
• At birth, the flat bones of
the skull are rather widely
separated by relatively loose
connective tissues. These
open spaces, the
fontanelles, allow a
considerable amount of
deformation of the skull at
birth. This is important in
allowing the relatively large
head to pass through the
birth canal

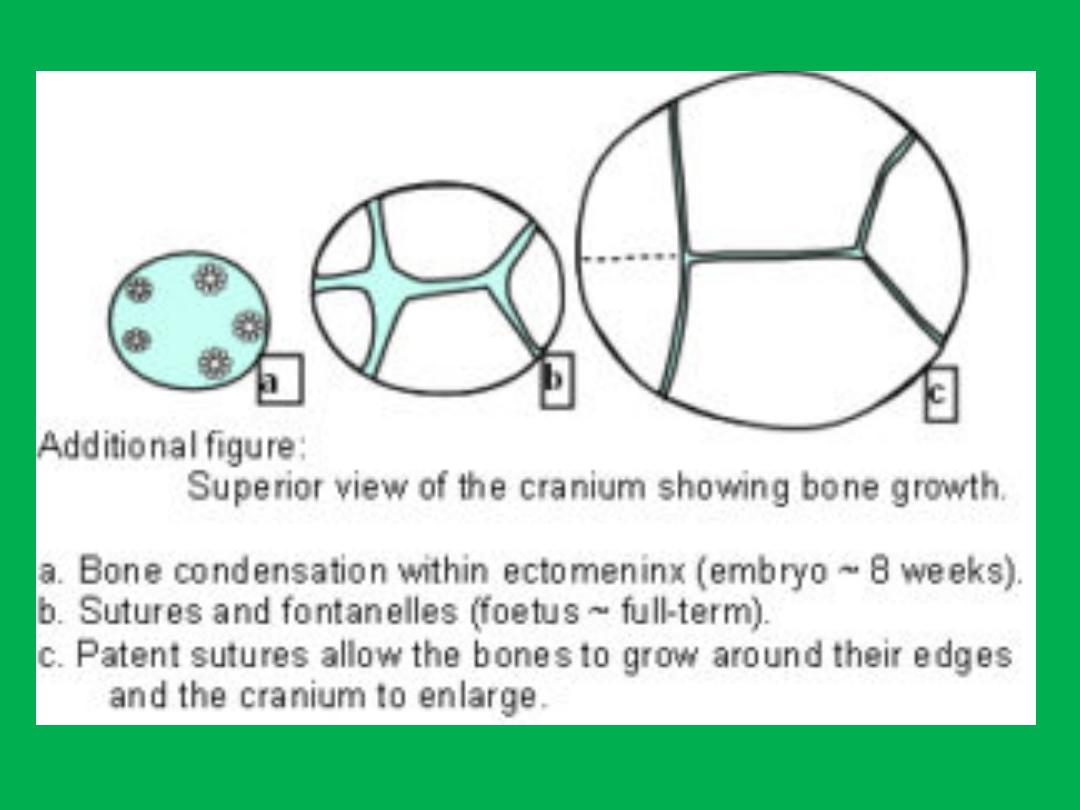
• After birth, apposition of bone along the
edges of the fontanelles eliminates these open
spaces fairly quickly, but the bones remain
separated by a thin periosteum-lined suture
for many years, eventually fusing in adult life.

• Despite their small size, apposition of new bone at
these sutures is the major mechanism for growth of
the cranial vault. Although the majority of growth in
the cranial vault occurs at the sutures, there is a
tendency for bone to be removed from the inner
surface of the cranial vault, while at the same time
new bone is added on the exterior surface. This
remodeling of the inner and outer surfaces allows
for changes in contour during growth.

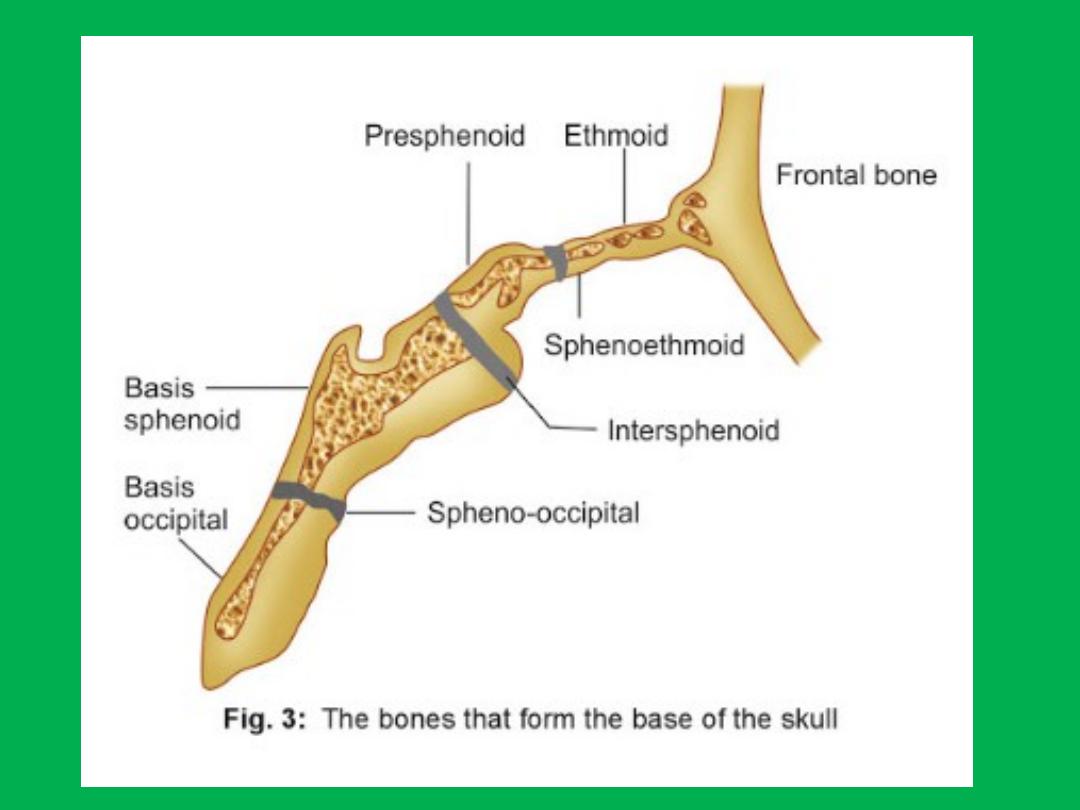
Cranial base
• In contrast to the cranial vault, the bones of
the base of the skull (the cranial base) are
formed initially in cartilage and are later
transformed by endochondral ossification to
bone. This is particularly true of the midline
structures. As one moves laterally, growth at
sutures and surface remodeling become more
important, but the cranial base is essentially a
midline structure.

• Growth of the cranial base is influenced by both neural and
somatic growth patterns, with 50 per cent of postnatal
growth being complete by the age of 3 years. As in the
calvarium, there is both remodelling and sutural infilling as
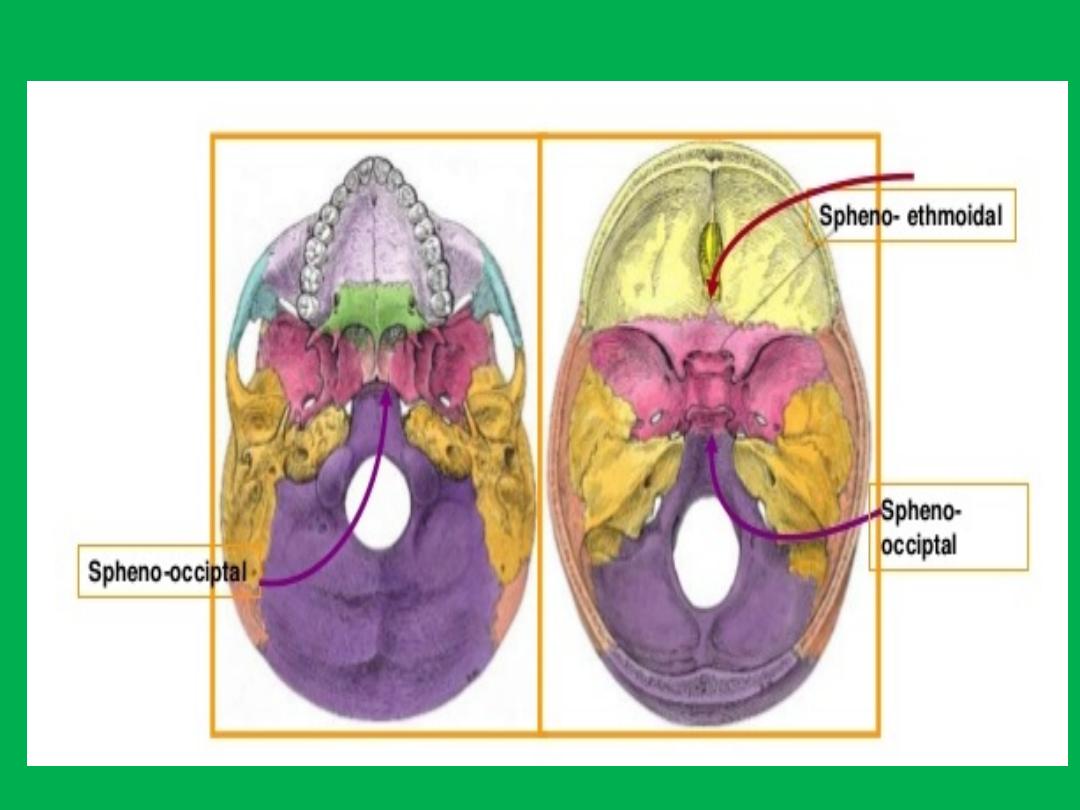
the brain enlarges, but there are also primary cartilaginous
growth sites in this region — the synchondroses.
• Of these, the spheno-occipital synchondrosis is of special
interest as it makes an important contribution to growth of
the cranial base during childhood, continuing to grow until
13–15 years in females and 15–17 years of age in males,
fusing at approximately 20 years.

• Thus the middle cranial fossa follows a somatic
growth pattern and enlarges both by
anteroposterior growth at the spheno-occipital
synchondrosis and by remodelling.
• The anterior cranial fossa follows a neural
growth pattern and enlarges and increases in
anteroposterior length by remodelling, with
resorption intracranially and corresponding
extracranial deposition.

• There is no further growth of the anterior cranial fossa
between the sella turcica and foramen caecum after the
age of 7 years. Therefore, after this age the anterior
cranial base may be used as a stable reference structure
upon which sequential lateral skull radiographs may be
superimposed to analyse changes in facial form due to
growth and orthodontic treatment.
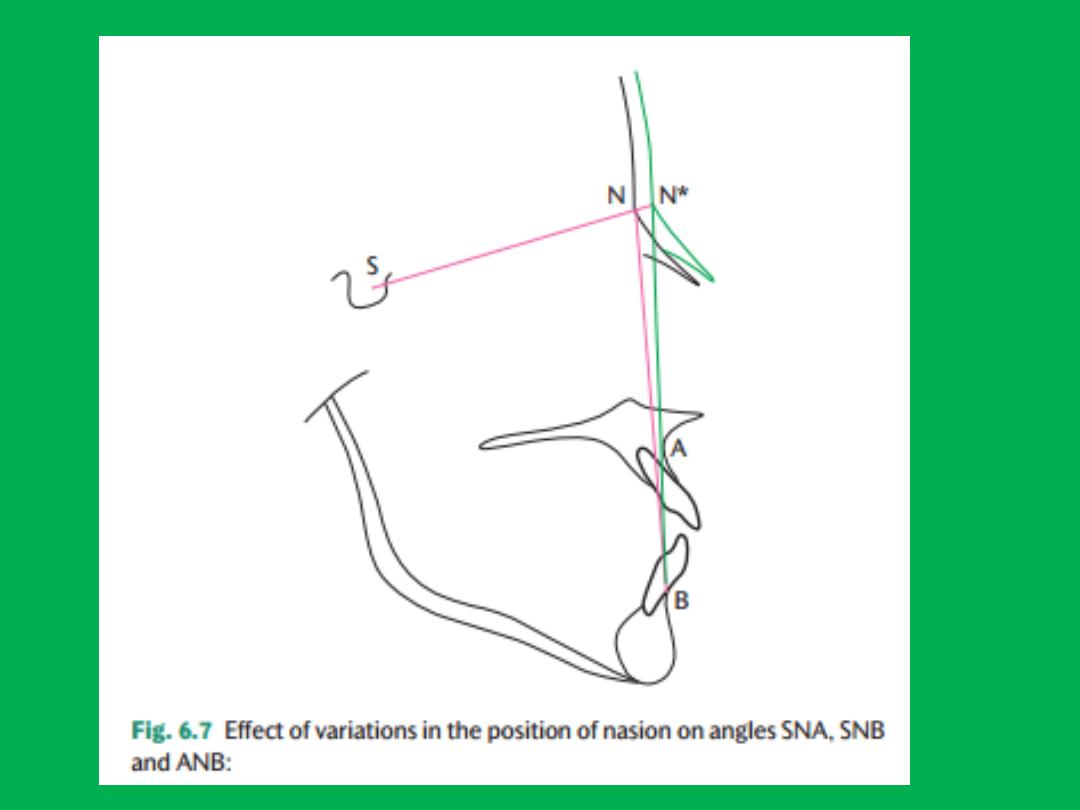
• The Sella-Nasion line is not as accurate because Nasion
can change position due to surface deposition and the
development of the frontal sinuses.

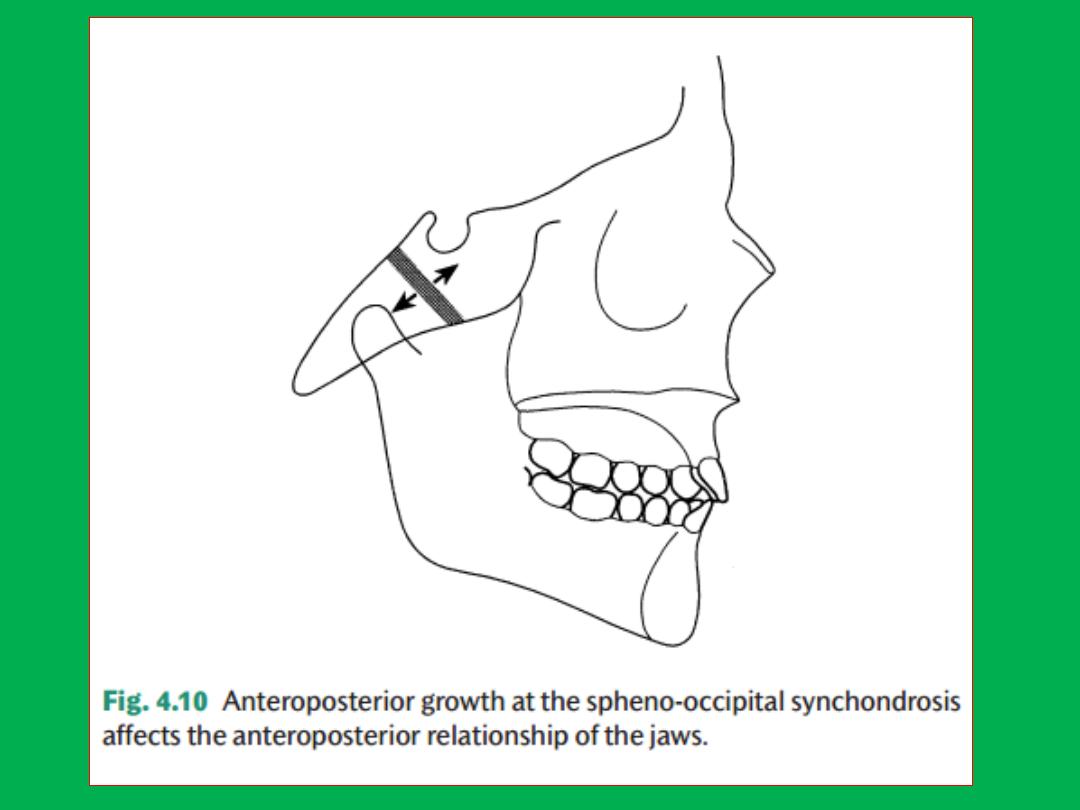
• The spheno-occipital synchondrosis is anterior to the
temporomandibular joints, but posterior to the anterior
cranial fossa, and, therefore, its growth is significant clinically
as it influences the overall facial skeletal pattern ( Fig. 4.10 ).
Growth at the spheno-occipital synchondrosis increases the
length of the cranial base, and since the maxillary complex
lies beneath the anterior cranial fossa while the mandible
articulates with the skull at the temporomandibular joints
which lie beneath the middle cranial fossa, the cranial base
plays an important part in determining how the mandible
and maxilla relate to each other.

• For example, a Class II skeletal facial pattern is
often associated with the presence of a long
cranial base which causes the mandible to be
set back relative to the maxilla.

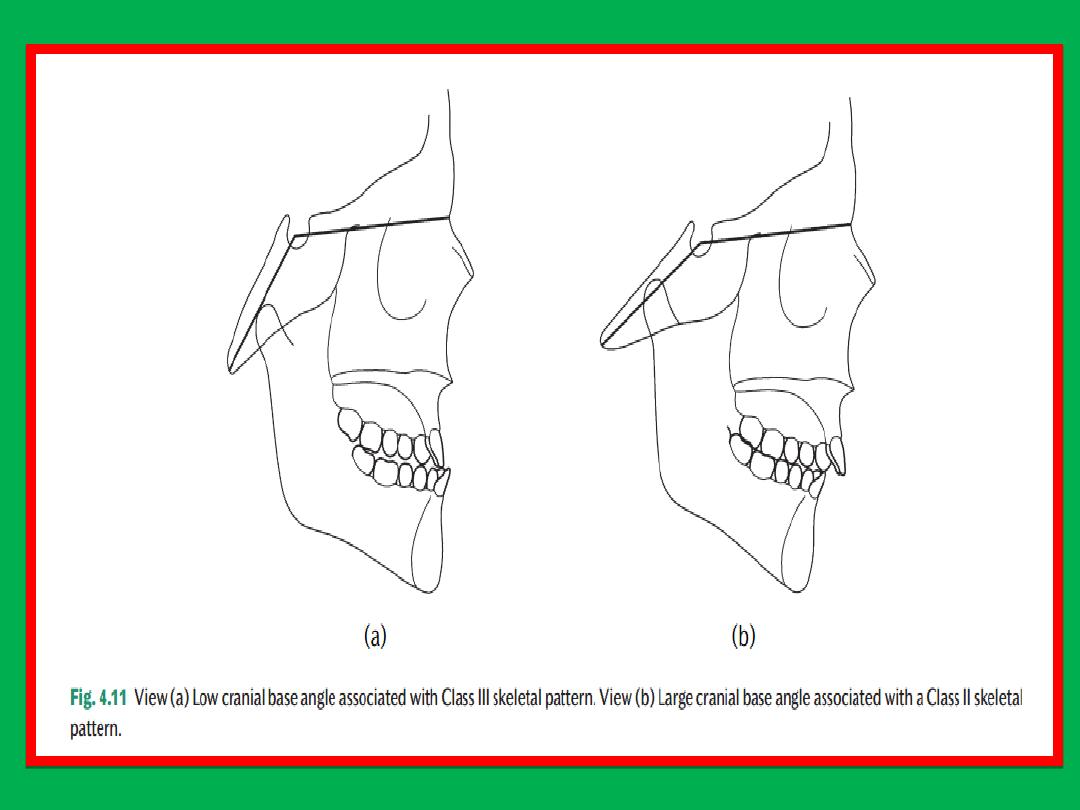
• In the same way, the overall shape of the cranial base
affects the jaw relationship, with a smaller cranial
base angle tending to cause a Class III skeletal pattern,
and a larger cranial base angle being more likely to be
associated with a Class II skeletal pattern ( Fig. 4.11 ).
• The cranial base angle usually remains constant during
the postnatal period, but can increase or decrease due
to surface remodelling and diff erential growth at the
spheno-occipital synchondrosis.

Nasomaxillary complex
• The maxilla derives from the first pharyngeal arch and
ossification of the maxillary complex is
intramembranous, beginning in the 6th week i.u.
• The maxilla is the third bone to ossify after the clavicle
and the mandible.
• The main ossification centres appear bilaterally above
the future deciduous canine close to where the
infraorbital nerve gives off the anterior superior
alveolar nerve. Ossification proceeds in several
directions to produce the various maxillary processes.

• Postnatal growth of the maxilla follows a
growth pattern that is thought to be
intermediate between a neural and a somatic
growth pattern.

• Clinical orthodontic practice is primarily
concerned with the dentition and its supporting
alveolar bone which is part of the maxilla and
premaxilla.
• However, the middle third of the facial skeleton
is a complex structure and also includes, among
others, the palatal, zygomatic, ethmoid, vomer,
and nasal bones. These articulate with each other
and with the anterior cranial base at sutures.

• The maxilla develops postnatally entirely by
intramembranous ossification. Since there is no
cartilage replacement,growth occurs in two ways:
(1) by apposition of bone at the sutures that connect
the maxilla to the cranium and cranialbase.
(2) by surface remodeling. In contrast to the cranial
vault, however, surface changes in the maxilla are
quite dramatic and as important as changes at the
sutures.
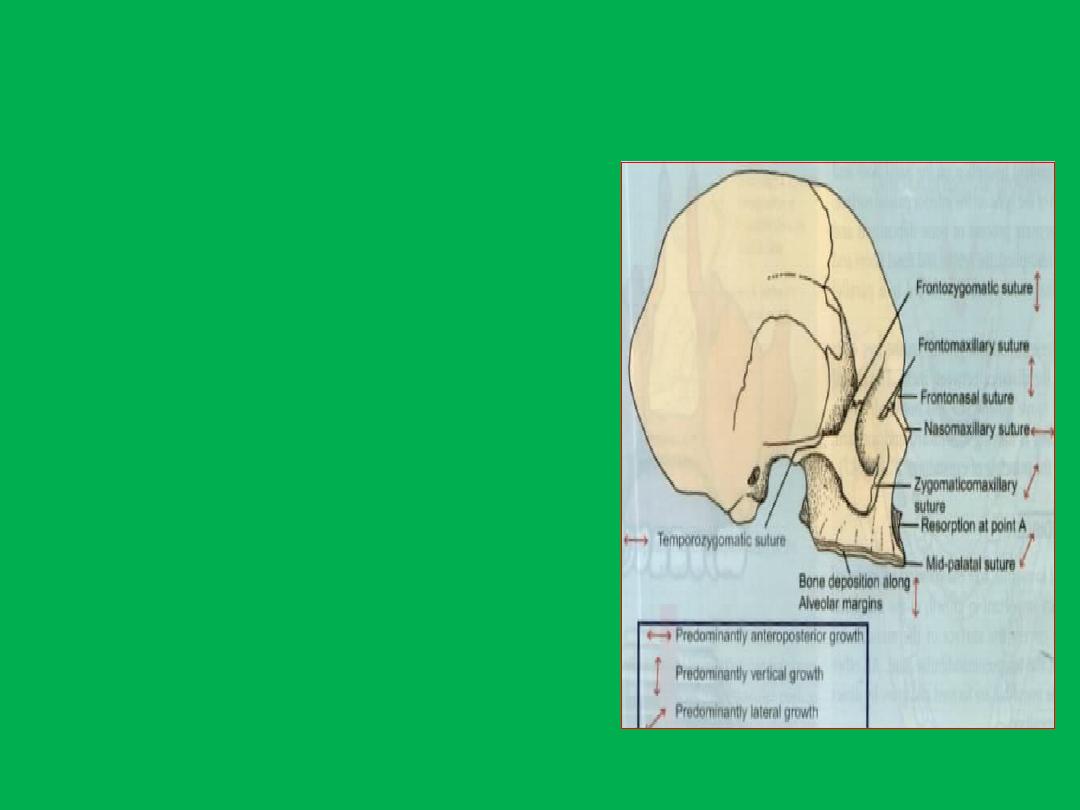
Growth at sutures
• Maxilla is attached to the
cranium by
1- Fronto-nasal suture
2- frontomaxillary,
3- zygomaticomaxillary
4- zygomaticotemporal
5- pterygopalatine suture
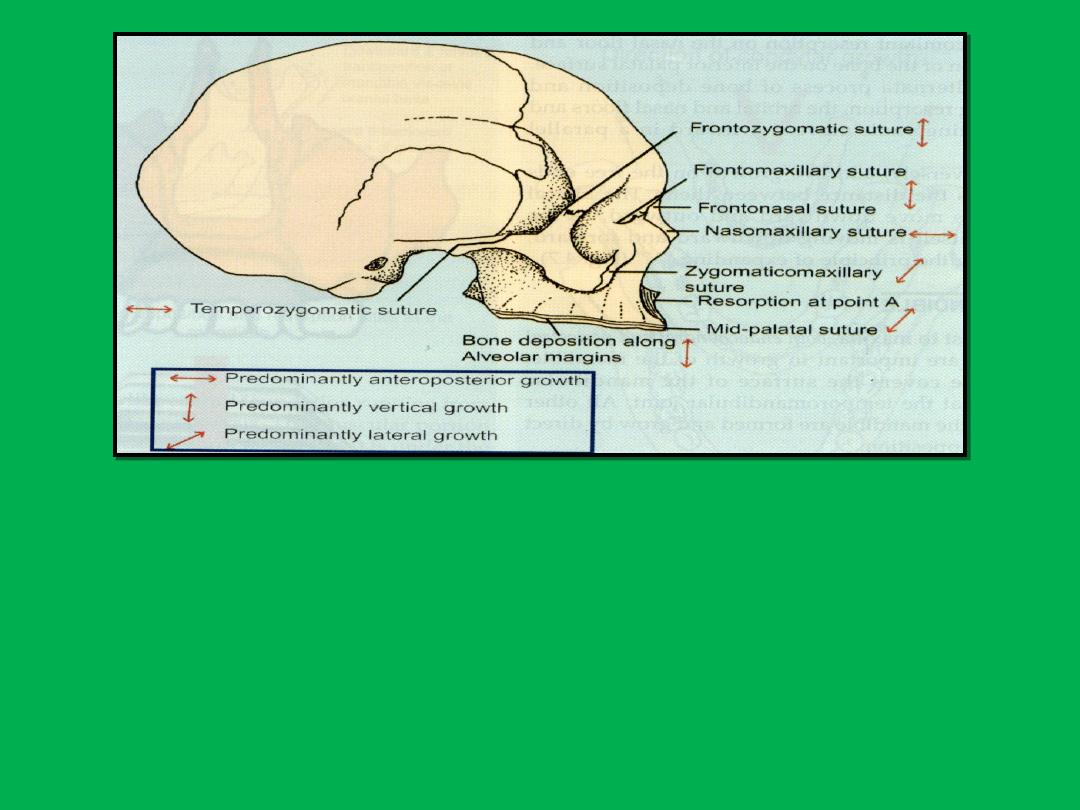
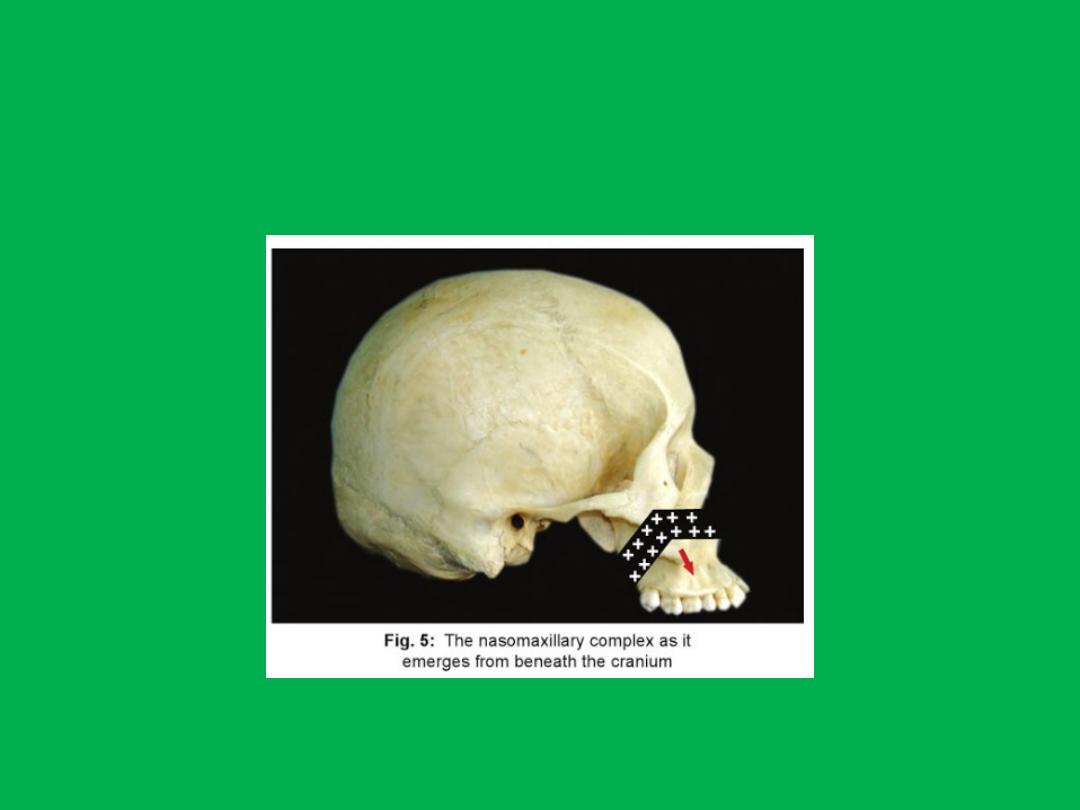
Sutures are oblique and parallel to each other. This allows the
downward and forward repositioning of maxilla as growth occurs at
these sutures. As growth of surrounding soft tissue occurs, the maxilla
is carried downwards and forward. This leads to opening up of space
at the sutural attachments. New bone is formed on either side of the
suture. Thus the overall size of the bones on either side increases.
Hence a tension related bone formation occurs at sutures.

Maxillary tuberosities
• Much of the anteroposterior growth of the
maxilla is in a backward direction at the
tuberosities which also lengthens the dental
arch, allowing the permanent molar teeth to
erupt.
• A forwards displacement of the maxilla gives
room for the depostion of bone at the
tuberosities.
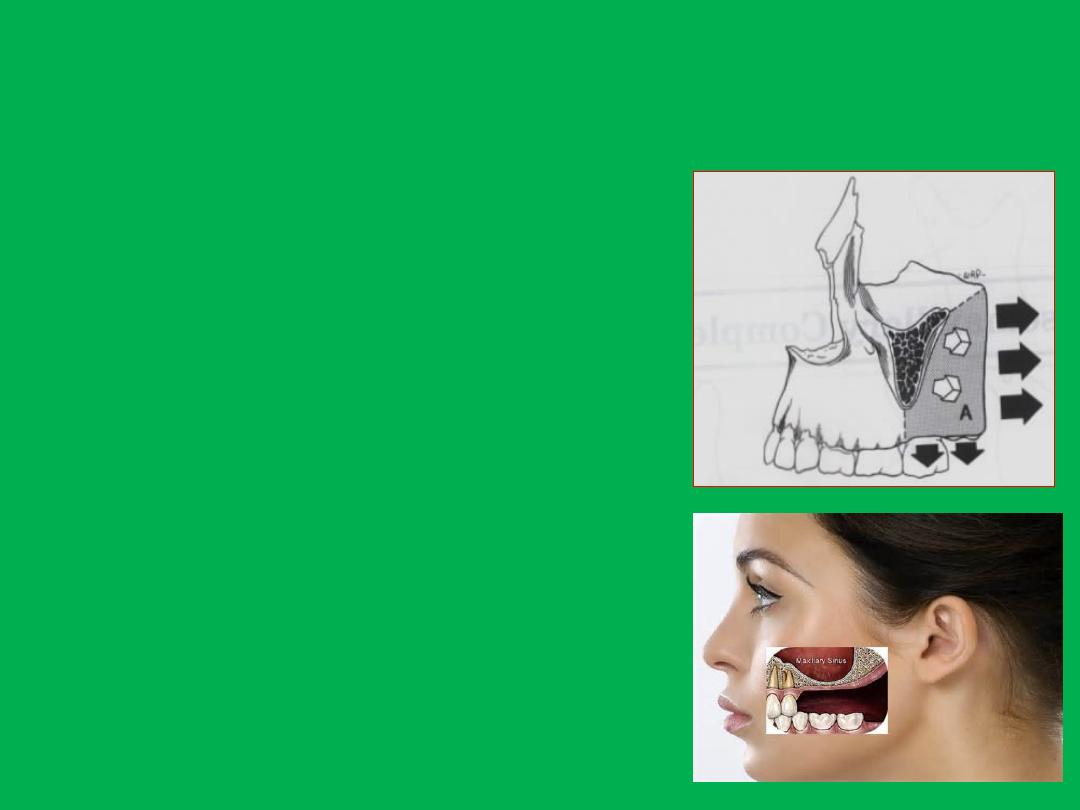
Maxillary tuberosity
• Maxillary arch grows in 3
directions
– Posteriorly deposition on
posterior surface of maxillary
tuberosity
– Laterally- deposition on buccal
surface of tuberosity
– Downward- deposition along
alveolar ridge
• Endosteal surface is resorptive
for growth of maxillary sinus

Zygomatic arch
• The zygomatic bones are also carried
forwards, necessitating infilling at sutures, and
at the same time they enlarge and remodel. In
the upper part of the face, the ethmoids and
nasal bones grow forwards by deposition on
their anterior surfaces
Zygomatic arch
• Resorption at anterior
surface and deposition
at the lateral and
posterior surfaces
• As a result the
zygomatic arches
move posteriorly and
bilaterally outwards

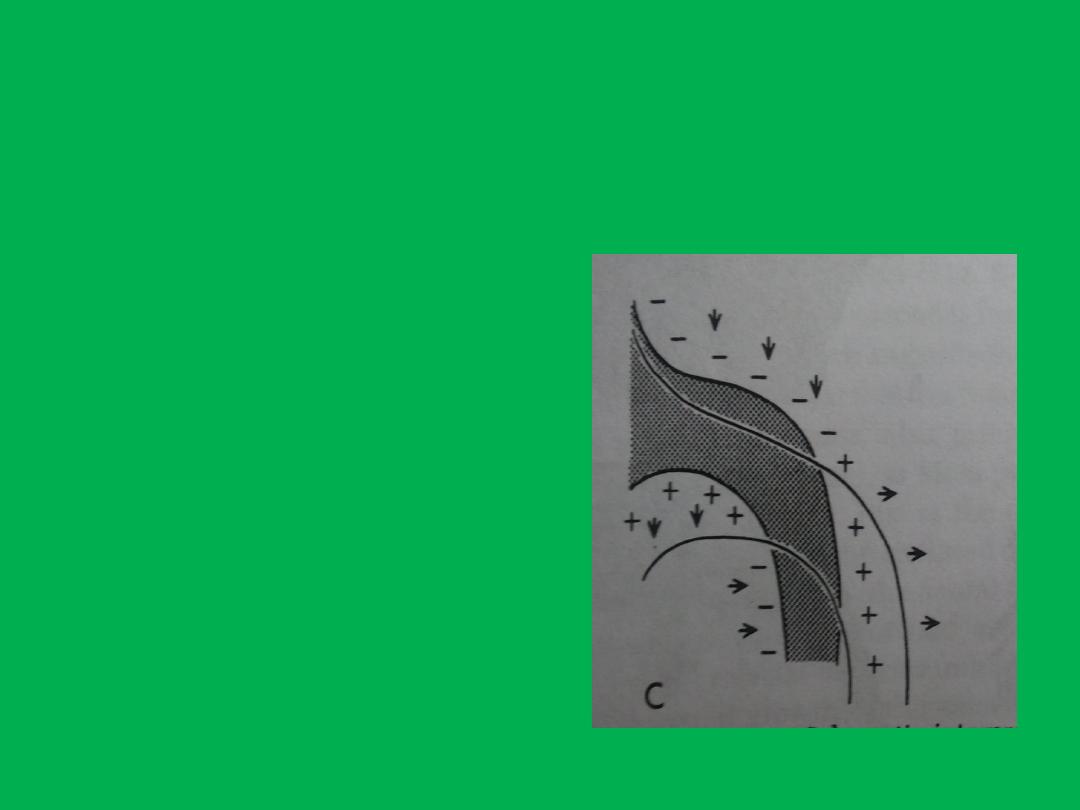
• Downward growth occurs by
1- vertical development of the alveolar process and
eruption of the teeth.
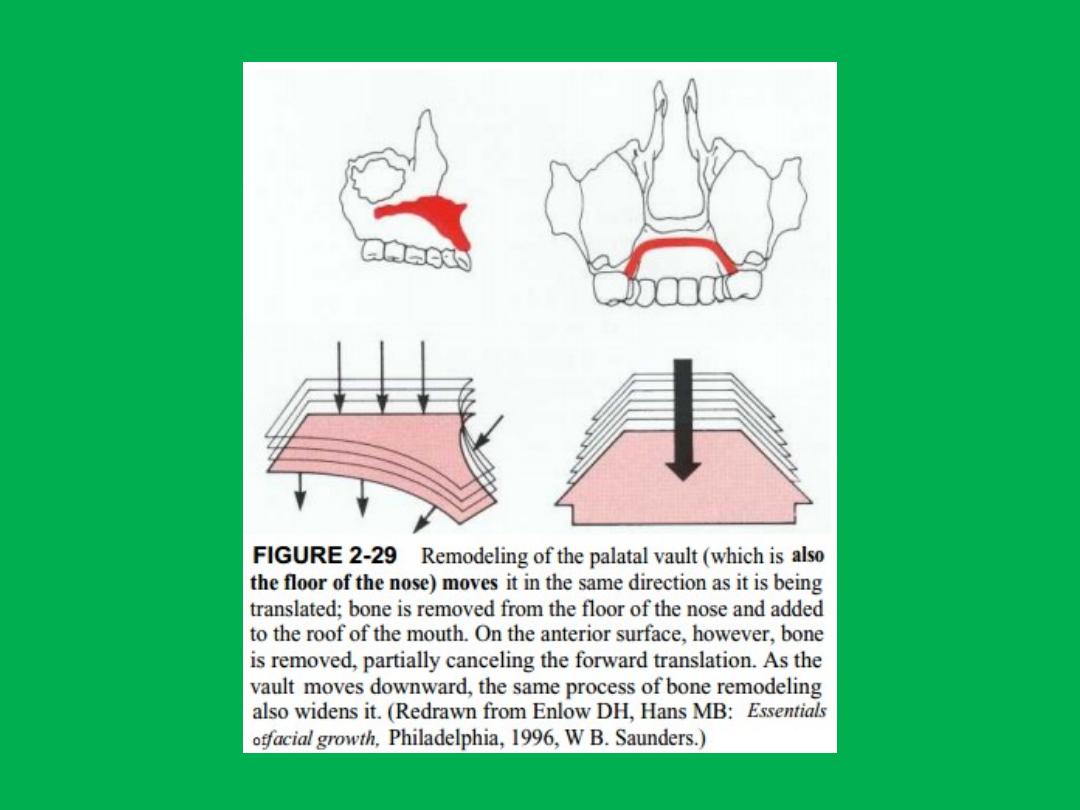
2- also by inferior drift of the hard palate, i.e. the palate
remodels downwards by deposition of bone on its inferior
surface (the palatal vault) and resorption on its superior
surface (the floor of the nose and maxillary sinuses).
3- These changes are also associated with some downward
displacement of the bones as they enlarge, again
necessitating infilling at sutures.
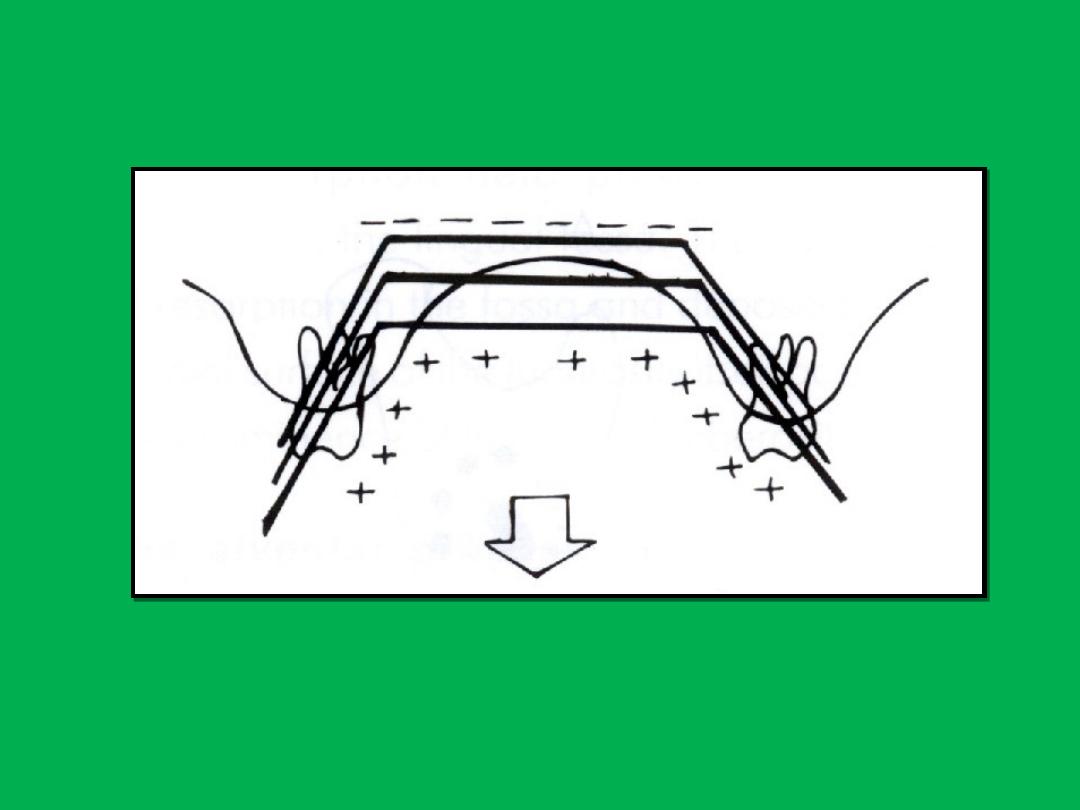

• Lateral growth in the mid-face occurs by
displacement of the two halves of the maxilla,
with deposition of bone at the midline suture.
• Internal remodelling leads to enlargement of
the air sinuses and nasal cavity as the bones of
the mid-face increase in size.

• Despite being translated anteriorly, in fact
much of the anterior surface of the maxilla is
resorptive in order to maintain the concave
contours beneath the pyriform fossa and
zygomatic buttresses.

• Maxillary growth slows to adult levels on
average at about 15 years in girls and rather
later, at about 17 years, in boys.